
Abstract
Introduction
This study aimed to assess women Veterans’ satisfaction with their primary mobility device and the related services they received.
Methods
Women Veterans who received a mobility device in the past 5 years from the Veterans Health Administration (VHA) completed an online survey containing the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST) about their primary mobility device. Scores were analyzed using descriptive statistics while open-ended comments were analyzed using inductive thematic analysis.
Results
571 out of 4078 (14%) invited women completed a sufficient portion (>75%) of the QUEST. They reported high levels of satisfaction with their devices and services received (>4 out of 5 indicating ‘quite’ to ‘very’ satisfied). Despite this finding around 80% of the women left comments related to discontent with their device. Main and sub-themes that were consistent across all devices included equipment issues (mechanical design, lack of features or customizability, poor quality components/material), physical and psychological impacts of the device, usability issues, and unmet service needs (lack of efficiency, lack of quality, issues with service providers and lack of access).
Discussion
Women-centered design and delivery of mobility devices should be prioritized. Opportunities exist for VHA to make improvements within several areas in the service and provision process.
Introduction
There are 1.9 million women Veterans in the United States, and 600,000 of these women are receiving care from the Department of Veterans Affairs (VA). 1 The number of women Veterans living with disabilities is growing at a faster rate than that of men. 2 In 2015, 8% of women Veterans had disabilities, and this is expected to increase to 11% by 2024. 3 Furthermore, the population of women Veterans is projected to increase by 0.3% by 2050 even though the total Veteran population is predicted to decrease by 1.6%. 4
Past studies have shown that women Veterans face barriers while receiving healthcare which is problematic due to their increasing number. For example, one study described how women Veterans’ felt that there is a lack of healthcare providers suited for women-specific health and services. 5 This can lead to significant gaps in addressing women’s health and possible inadequate management of conditions. It is important that women Veterans’ feel they have resources tailored to their unique needs. Furthermore, in a separate study of 3611 women Veterans, 19% had delays getting their healthcare needs met or their needs were left unmet. 6 Notable barriers from this sample’s ability to receive healthcare included affordability, inability to take off work, and transportation issues. 6 These findings highlight critical challenges women Veterans face in healthcare, and a greater focus on improving their care and quality of life is needed. Women Veterans have voiced the need for more information on services available to them and making these services more accessible. 7 They have also recommended increasing outreach and education to increase women Veterans’ entitlement to services provided by the VA. 7
The Veterans Health Administration (VHA) has developed guidelines to try to ensure that women Veterans’ healthcare needs are met and to improve their access to gender-specific care. 8 More recently, VHA has updated the standard requirements for delivering care to women Veterans to further raise the standard of care. 9 VHA offers fertility services, mental health services, and maternity care. 1 Some policies include implementing the roles of Women Veterans’ Health Committee, Women’s Health Medical Director, Women’s Health Patient Aligned Care Team, and Women Veterans’ Project Manager. 9 Furthermore, VHA Directive 1330.01(7) “Health Care Services for Women Veterans” states that Physical Medicine and Rehabilitation services “should be tailored to the needs of women Veterans including ordering and stocking equipment and supplies that are the correct size and fit for women Veterans”. 9
While these guidelines are designed to improve gender-specific healthcare, a limited amount of evidence has explored how well they are working to meet current needs related to mobility devices, a crucial aspect of healthcare delivery for many women Veterans. In Fiscal Year 2021, the VA prescribed 99,100 wheeled mobility devices to Veterans of all genders. Of these, 14,788 were powered wheelchairs, 19,156 were scooters, 22,081 were custom manual wheelchairs, and 53,080 were standard manual wheelchairs. 10 Now, as the number of women Veterans with disabilities is increasing, it is important to ensure they are satisfied with the mobility devices and related services they are receiving.
Studies exploring gender specific experiences with mobility devices outside of the Veteran population have highlighted the need for improvement. A study of 11 women wheelchair users demonstrated challenges that they face with using wheelchairs in daily life, including how they were designed. 11 Some women expressed that their wheelchair was difficult to use and they did not receive their wheelchair through services tailored to women. 11 In another study of women wheelchair users, some women also expressed that their wheelchair restricts their personal autonomy and social participation and caused them to feel uncomfortable. 12 Lastly, a study assessing gender differences in cane use showed that women were less likely than men to use their canes and that physical and social factors may influence these gender differences. 13 These studies indicate potential issues concerning mobility device design not meeting the needs of women and gender-specific disparities in the related services that are provided.
Little is known about the perspectives of women Veterans concerning their experiences with mobility devices. The purpose of the cross-sectional exploratory study was to (1) assess women Veterans’ satisfaction with their primary mobility device and understand concerns related to the device being able to meet their needs and (2) assess their satisfaction with related services (e.g. procurement, repair and servicing, follow-up). Given the wide range of mobility devices used by women Veterans, we further aimed to explore differences in satisfaction between device type categories of canes, walkers, crutches, leg/foot orthoses, manual wheelchairs, power wheelchairs, and scooters.
Methods
Study design
This study is a sub-component of a larger cross-sectional exploratory study that involved a national online survey administered to women Veterans who had received a mobility device in the past 5 years from the VHA. Data collection occurred between May of 2021 to April of 2022. A mixed method approach was employed with the Quebec User Evaluation of Satisfaction with Assistive Technology item scores analyzed using descriptive and inferential statistics and open-ended comment sections analyzed based on pragmatic epistemology theory and inductive thematic analysis. Qualitative study components are reported in accordance with the consolidated criteria for reporting qualitative research (COREQ). 14
Participant selection
Women Veterans were identified using the VA National Corporate Data Warehouse, the VA Spinal Cord Injury National Registry, and the 61 VA medical centers that comprise the Women’s Health Practice-Based Research Network. All identified women Veterans (n = 4078) were mailed an invitation to participate in an anonymous survey to assess their satisfaction and experiences with mobility devices. Participants were told that one respondent would be awarded $100 at random for every 300 responses to the survey. Follow-up reminders were sent to non-responders in an attempt to improve the response rate. This study was approved by the Institutional Review Boards at VA Pittsburgh Healthcare System and the Center of Innovation for Complex Chronic Healthcare Edward Hines, Jr. VA Hospital.
Data collection instrument
The survey was created using Qualtrics and included demographics and the Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0), which evaluates satisfaction with a mobility device and the service provision process. 15 The QUEST is a 12-item validated and reliable scale that assesses the satisfaction concerns on two separate subscales: Device and Service. Each subscale presents unique satisfaction items that respondents were asked to rate based on a Likert scale (1: Not satisfied at all – 5: Very Satisfied). Prior to completing the survey, the following instructions were provided to the respondent: “Next, we would like to evaluate how satisfied you are with your primary mobility device and the related services you experienced. [QUEST version 2.0] For each of the items, rate your satisfaction with your primary mobility device and related services using the following scale from 1 to 5. For any question that you were not ‘very satisfied with’ (your score is less than a 5), please comment in the comments section.” Respondents were then asked to rate their satisfaction on the device on components related to dimensions, weight, adjustability, durability, easy usage, comfort, and effectiveness. Respondents were additionally asked to comment on service-level items relating to service delivery, maintenance, professional, and follow-up services. If respondents rated any satisfaction item a 4 or lower, they were given the opportunity to comment on each item regarding their primary device. This approach was done under the assumption that those who answered a 5 (very satisfied) did not have any concerns. Including a rating of 4 was so we could capture small reasons or concerns as to why they chose not to score a 5. The QUEST also asks respondents to rank their top three most important satisfaction items. The survey also asked women to name the primary device being used: cane, crutch/crutches, walker, leg/foot orthosis, manual wheelchair, power wheelchair or scooter.
Data analysis
Descriptive statistics were determined for the quantitative portion of the survey, as well as the demographical data of the respondent sample using SPSS Version 28. Means, standard deviations, and medians of each satisfaction item were determined. Additionally, an average QUEST score was calculated over all the items and for each subscale (Device and Service) for each primary device. Frequencies and percentages of respondents were used to describe the ranking portion of the QUEST. A one-way ANOVA test was used to assess differences in QUEST items and overall scores by primary device group.
The qualitative data were analyzed using a hybrid approach of inductive thematic analysis and content analysis.16,17 NVivo Version 14 was used to manage the data. The methods of thematic analysis followed the six-step process as described in Braun and Clarke (2006). The data were sorted by primary device type used. After familiarization with the data within each device type, comments were independently assigned initial codes by two researchers (DK, JS). DK and JS are both undergraduate students in biology and kinesiology, respectively. A third researcher (AK) was used to resolve discrepancies in codes and comment assignments. AK holds a PhD in rehabilitation sciences and is an assistive technology professional (ATP). Her expert guidance was used to minimize bias and strengthen trustworthiness. After coding was completed three researchers (AK, JS and RK) conducted the theme searching process by sorting the codes into groups and assigning potential themes. RK holds a background in bioengineering. Authors with varying backgrounds partook in qualitative analysis to reduce bias and bring varying perspectives to the data. The grouping and theming process underwent several iterations of review and refinement before arriving at the final theme names and map. Although thematic analysis is primarily qualitative, frequencies and percentages were reported for each subtheme to promote transparency and provide readers with a sense of the relative prominence of different issues raised by participants. Quantifying the responses helps to contextualize which concerns were most experienced among respondents. This approach is consistent with accepted methods of content analysis that allow for descriptive counts within thematic frameworks. 17
Results
Quantitative results
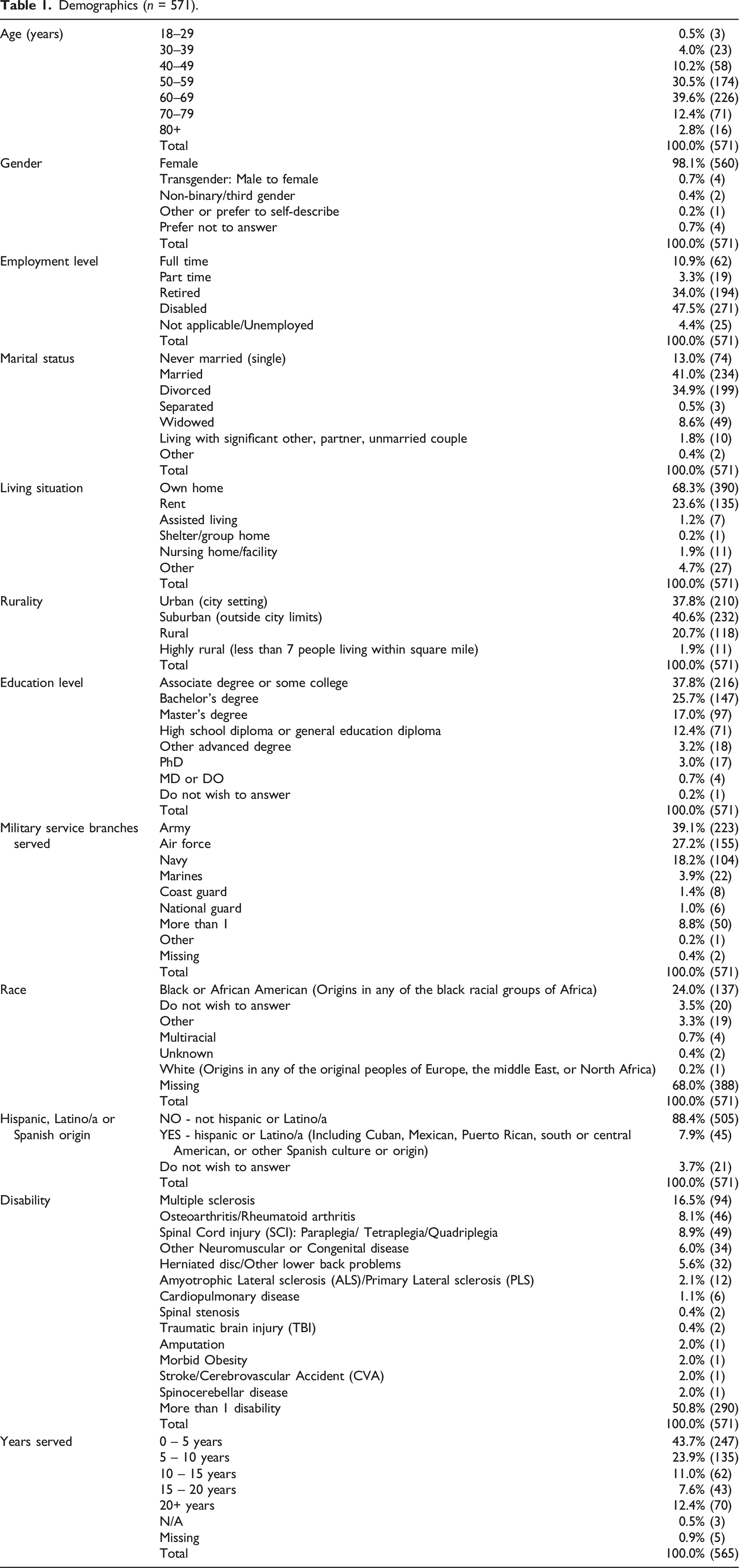
Demographics (n = 571).
QUEST scores and differences by device type
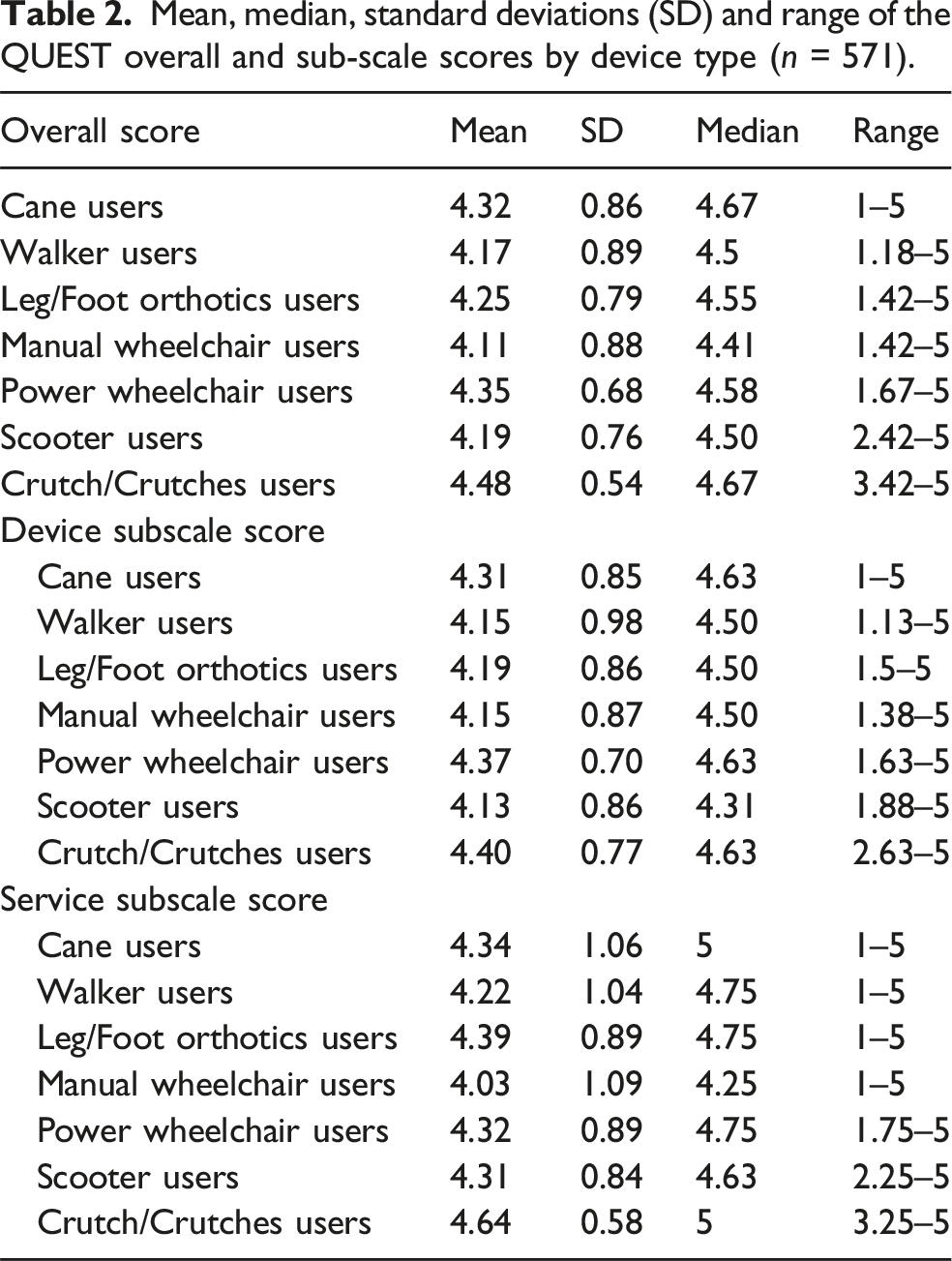
Mean, median, standard deviations (SD) and range of the QUEST overall and sub-scale scores by device type (n = 571).
QUEST Prioritized Satisfaction Factors (n = 563). The QUEST survey consisted of 12 sub questions assessing the level of prioritization with the primary mobility device factors, including dimensions, weight, adjustments, safety, durability, easy to use, comfort, effectiveness, service delivery, repairs/servicing, professional services, and follow-up services. The “Percent (N)” column refers to the number of women that prioritized the factor in their top-three.

Qualitative results
Themes by device type
446 of the 571 respondents (78.1%) who completed the QUEST provided open-ended comments for qualitative analysis. Respondents were included in the qualitative analysis if they commented on one or more satisfaction item. A majority of the comments (96.8% or 1732/1789 total comments) left on the QUEST were related to an element of dissatisfaction with the device or service and were included in the thematic analysis.
Although the thematic analysis was conducted separately within each device type category, four main themes were consistent across all categories: equipment issues, physical and psychological impact of device, unmet service needs, and usability issues (Table 4). The majority of concerns focused on equipment issues (42% of all dissatisfied comments) followed by unmet service needs (28.1%), physical and psychological impact of device (14.7%) and usability issues (14.0%). There were three sub-themes under equipment issues which were also prevalent among all device types: issues with mechanical design, lack of features or customizability, and poor quality components/material. Four sub-themes under the unmet service needs that were present among all device types with the exception of crutch users (possibly due to the small sample size/number of comments) were: lack of efficiency, lack of quality, issues with service providers, and lack of access. A fifth sub-theme under unmet service needs for the scooter group was user barriers to access. The following sections describe the results of the thematic analysis by device.
Canes
Equipment Issues: Women who use canes complained about their limited to no ability to adjust or fold them, lack of stability, and poor aesthetics. While some commented on their bulkiness and heaviness others said they were too light. Many women felt that they needed a different kind of device for their disability or would rather use their secondary device because it was easier for them. The canes did not fit them well and it lacked some desirable features that would make it more functional for them. Canes broke easily, had parts that fell out or loosened overtime and were cheaply made. “Canes are slippery on ice and can make falling worse. Also, high winds can blow a cane while walking with it making it more difficult to control.” (Cane) “I have arthritis in my hands and the one size fits all cane and folding walker on a short person is not feasible.” (Cane)
Physical and Psychological Impacts: Women who use canes complained about physical discomfort, indicating that the cane negatively affects their gait, their posture, and is tiring to use. Furthermore, women noted that the cane was creating more medical issues by contributing to causing pain and being unable to prevent, or even causing, falls. Some women also commented that they did not feel safe or secure using their cane, causing anxiety. “I don’t believe it keeps me very safe. I’m often nervous.” (Cane) “I’m now having pain in my right wrist and hand, I believe it's from pressure of the cane.” (Cane)
Usability Issues: Many women who use canes reported that they were difficult to use with pre-existing medical hand or shoulder conditions. One woman noted that their cane is very hard to pick up when dropped. Canes were also noted to be inconvenient in daily use, being difficult to control, difficult to transport, difficult to hold for long periods of time, and difficult to use in varying weather conditions. One woman reported that her cane is difficult to use particularly on wet surfaces. Some women also noted that they require further assistance while using their cane. “They weigh 3 pounds each but that's what helps me use them. Requires weight on shoulders which are worn out.” (Cane) “When I am in a store, they fall, they are a pain to deal with, and if the floor is wet they slip.” (Cane)
Unmet Service Needs: Many women indicated problems with service providers regarding their canes. A woman had problems with the prescription of the cane, indicating that it was provided as a fix for a condition that could have been treated. Other women commented that the service providers were rude, incompetent, or unprofessional, noting that it felt as though staff were uncommitted to providing devices reflecting Veteran lifestyles. Many women also commented on issues accessing maintenance, whether it be regarding lack of education in maintenance options or difficulty with travelling far distances to receive maintenance. One woman commented that her service is limited because only the VA carries the required parts to service her cane. Delivery was a consistent issue for women using canes. Many women commented that the service delivery process was difficult, delayed, or slow, oftentimes having a long appointment fulfilment time or the device being delivered with damaged packaging. Women also complained about the poor quality of their services, stating that they did not receive adequate training, maintenance, follow up, or communication from professionals, and whatever services they did receive were poor. “It takes too long to get the equipment and the Veteran has to stay on top of all necessary equipment!!” (Cane) “Very rude, unprofessional and usually uninformed people who don’t care.” (Cane)
Crutches
Equipment Issues: Women who used crutches complained that they were manufactured for men, were hard to adjust or had no adjustability or ability to collapse. They felt they were ill-fitting and lacked cushioning. Crutch parts do not stay in place after adjusting them and they require frequent replacements. “The crutch does not readily adjust to my height…they are manufactured to fit males.” (Crutches) “The top part that is supposed to wrap around my forearm is too big and does not grip my arm. The metal cuff is also not adjustable, so I can’t make it tighter so that it will grip.” (Crutches)
Physical and Psychological Impacts: Women using crutches indicated that it caused pain and discomfort during use in their underarms or hands. They felt the crutch was inconvenient to use. Some women also reported feeling unsafe while using their crutch, with one woman noting that she has fallen while using the crutch before. “Hand grips are really hard and can be slippery, after hours walking, they leave my hands cramped and sore.” (Crutches) “It makes it uncomfortable, and a few times unsafe because it wasn’t grabbing my arm, and I managed to fall when I let go of the handle.” (Crutches)
Usability issues: Two women commented experiencing usability issues with the crutch. One woman stated that the device is difficult to use for walking long distances, while the other commented that it is difficult to use on public transportation. “They were not made for any long periods of walking or using public transportation.” (Crutches)
Unmet Service Needs: Two women commented on service issues for their crutch. One woman said that there were errors in the prescription of the device with the physician forgetting to place an order for her crutch. Another woman commented that she received no follow up services despite wanting them. “I had to have my pcp place an order twice because it wasn't written exactly as needed the first time.” (Crutches) “There has been no follow-up service.” (Crutches)
Leg/foot orthosis
Equipment Issues: Women using these devices felt they were manufactured for men, either had no adjustability or too many adjustments, and were bulky and heavy. Some felt that they were too light, too rigid or too tight. There were complaints around the device or material being too hot to wear particularly in warmer climates. Sweating and wearing the device over long periods of time cause it to feel heavier. Wearing it can ruin their clothing or cause unwanted odors. Devices lack cushioning and are not customized or personalized to them. The fittings are sometimes incorrect, or the device does not solve the problem they have. Devices wear out and require frequent replacements or adjustments. “Sometimes the Velcro fastening doesn't stick adequately enough to the insole of a shoe/boot, so the lift slips out of position toward the front of the shoe/boot, or out of the side of a sandal. Hard to get old, worn Velcro off to replace with new piece.” (Orthosis) “They send me an orthopedic insert for males versus females. I only received female inserts once. I have very narrow feet.” (Orthosis)
Usability Issues: Women using the leg/foot orthoses commonly reported that their device is difficult to put on or adjust, especially when the user has other pre-existing health conditions, and that they often require assistance from others to put it on. Some also noted the device is awkward to use. “It is not easy to put on. My brace is like a sleeve, so when I have to really move the patella around to adjust it, it creates a lot of pressure.” (Orthosis) “My arthritis makes it difficult to grip, twist, pull, or hold things so installing and adjusting devices is often impossible.” (Orthosis)
Physical and Psychological Impacts: Many women who use a leg/foot orthoses reported that their device is restrictive, inconvenient, and limits movement. There were complaints that the device does not feel secure, is tiring to use, and requires extra effort, with many women complaining that the device is causing more issues than what it is solving. Users mention strain, pain, discomfort, allergic reactions, and pressure on the body. One woman also noted that her dependence on her brace negatively affected her psychological well-being. “I have a deformed small toe and the brace pushes that toe to the top of the shoe where it is painful.” (Orthosis) “It’s humiliating and demeaning. It diminishes my sense of independence and self-pride.” (Orthosis)
Unmet Service Needs: Many women using leg/foot orthoses commented on dissatisfaction with their service relating to prescription, delivery, and follow up maintenance. Women commented that when prescribed their device, there was a clear lack of education on other options for treatment or on what maintenance/ repair options exist. They felt alienated by services and encountered rude and unprofessional staff, with one woman commenting how her physician lacks knowledge of her condition and another woman feeling like she needs to fight for her needs. One woman commented that she feels there are a lack of better options available for Veterans. Many women also experienced major delays in delivery of their device accompanied by poor communication from those delivering the device. Maintenance of the device also prevailed as a major issue, with many women commenting on the lack of access to maintenance options due to far distances. Some women commented there were no options for maintenance available, and that they desired those services. Maintenance on the device also was said to be poor quality, with their device adjustments not staying in place or requiring frequent follow up maintenance. “I think there are devices out there that are more comfortable but cost more and we are not offered them.” (Orthosis) “Protocols are not so much face to face friendly.” (Orthosis)
Walkers
Equipment Issues: Women using walkers feel they are manufactured for men and have limited to no adjustability, are hard to adjust and that the adjustments require tools or are difficult to reach. Walkers had limited to no collapsibility and are difficult to stow. Women feel their walkers are bulky, too big or too heavy and awkward to use. They lack cushioning and lumbar support (on devices with a seating option). The designs make maneuvering them difficult. There were complaints around warped frames and ineffective wheel material and frame material getting too hot to touch when using it in warm weather. Some women felt that the device did not solve their problem and would prefer to use to a different device. The device did not fit them well and lacked desired features and customization. The device broke easily requiring frequent replacements. Adjustments or parts loosened over time or functioned inconsistently. “The rollator is very huge bulky and unable to fit in between doorways easily… if it was small for a female would be easy to maneuver but it's heavy and big and bulky.”(Walker) “The ease of adjustments [is] very hard and take manpower to move… being a woman it's hard to do especially if something breaks on a transport chair or the rollator.” (Walker)
Usability issues: Many women commented that their walker is difficult to use with their pre-existing medical conditions (shoulder conditions, problems with dexterity, cognitive issues), while others commented that it restricted their movement and is difficult to operate when fatigued. They also reported that the walker limited their mobility, was difficult to operate on stairs, in public places, and for long distances. Women also commented that their walker was difficult to lift and transport. Lastly, many comments were made about the walker limiting their independence and activities of daily living, causing them to seek further assistance from individuals or other devices. “Plastic knobs to adjust height are hard for someone with grasping issues to hold onto. The knobs loosen constantly making the handles wobble.” (Walker) “I am still extremely limited in what I can do.” (Walker)
Physical and Psychological Impacts: Walker users reported experiencing physical and mental issues due to use of their device. Physical issues included discomfort, pain, poor posture, and fatigue. Some complained that the device caused additional medical problems. Women reported that they felt discouraged from being forced to received care in a male-centered healthcare system, and that they felt stuck using their walker but just needed to accept it. One woman commented that the mechanical issues of the walker leave women embarrassed and humiliated. Others reported that the walker makes them feel unstable and requires focus to use. “Too heavy and awkward to pick up and put in/get it out of the minivan. I have had to have recent surgery on both my shoulders. But also very tippy when in use and I am off balance-- tips to the side if I apply too much weight.” (Walker) “[My walker] hurts my upper arms and shoulders because I have to sort of lean over to use it, I would rather it not affect my posture.” (Walker)
Unmet Service Needs: Women who used walkers commented on poor experiences with prescription, delivery, and maintenance of their device. Some women had issues with their healthcare provider, stating that their physician ordered the incorrect device, or that the VA authorized an unsafe rollator. Other women described an unprofessional experience with VA services. With the prescription of their device, many women commented they were not given proper training or information on how to access available maintenance options. Delivery was another common issue, with long delivery times or far pick-up distances sometimes exacerbated by COVID-19. Two major issues with maintenance included a general lack of maintenance options through the VA or poor-quality maintenance received from the VA. Some women commented that the VA did not provide any repair options, requiring the women to pay for device repairs out of pocket elsewhere. Other women commented that the maintenance they did receive from the VA was insufficient. One woman stated that she desired a female mechanic who understands women’s needs. “Need more mechanics, maybe a real female one. She would know about the issues.” (Walker) The equipment was delivered to the house with no feedback on how to fix any issues.” (Walker)
Manual wheelchairs
Equipment Issues: Women using manual wheelchairs felt their device was not built for women or that they were manufactured for men. It is hard to adjust or has no adjustability. The wheelchair does not collapse or is difficult to collapse and doesn’t store easily. It can be difficult to assemble. The device is too big, too heavy or too bulky. It’s not compatible with their home, their lift system, or other assistive technology. The devices lack lumbar support or brakes. It makes unwanted noises and there are loose and missing parts. Some women felt their wheelchair did not work well for them or that it was not ideal for their specific disability. The device was not fitted to them well and lacked customization. The devices lacked durability, were cheaply made and required frequent replacements or maintenance. Women using power assist add-ons complained of low or poor battery life. “Made for a 400lb male and won’t go through doors.” (Manual wheelchair) “The bearings on my caster wheels need monthly maintenance.” (Manual wheelchair) “Wheelchairs I’ve had are not built for females and the choices are limited to what vendors the VA has to [choose] from.” (Manual wheelchair) “I also lean to my right a lot due to my core muscles are weak because of MS. I also lean to the right and I need a cushion that leans a bit away from my right. Or a cushion that undulate so my buttocks won’t get sores or a standing wheelchair.” (Manual wheelchair)
Usability issues: Several women who predominantly use manual wheelchairs reported issues with the usability of their device. Issues arose with integrating the device into their daily routine, with many women commenting that the device was difficult to use, hindered independence, or was difficult to use for long periods of time. The device also negatively impacted daily activities, including transportation, reaching for objects, maneuvering in different directions, and navigating on real world terrain, with many women reporting the need for further assistance outside of their device. Some women noted that their wheelchair was difficult to use with other medical equipment as well. “It does not give me the independence I need in a mobility device. I'm reliant on my husband, or another person, for help to get me where I need to go.” (Manual wheelchair) “It’s difficult for me to use for any extended period of time.” (Manual wheelchair) “Because I have a bad right arm, it is difficult to maneuver.” (Manual wheelchair)
Physical and Psychological Impacts: Women that use manual wheelchairs reported feeling restricted in their social interactions due to the dimensions of their wheelchairs, with one woman noting that she felt discouraged from being shorter than everyone else. Users also noticed transportation barriers that caused physical harm, stating that transportation workers lack knowledge about wheelchair transport safety. Many women felt their wheelchair caused pain and discomfort while using and during transfers. They felt the wheelchair was unsafe or unstable, and that some devices lack clear caution labels. “I’d like to be a little 'taller' in it. If it was somehow still stable, but just a few inches taller I could do more and deal less with people talking over my head to each other.” (Manual wheelchair) “The leg causes me pain at times and many times there is nothing that can be done because of the way that it is designed.” (Manual wheelchair) “It feels like I'm going to tip over sometimes when outside on the crappy sidewalks of San Diego, CA. I try to look ahead and avoid certain areas but its not always a choice.” (Manual wheelchair)
Unmet Service Needs: Women who use manual wheelchairs reported many issues with their service providers. Some women stated that the staff were rude, unprofessional, inconsistent, or unresponsive, with one woman stating she felt discriminated against in the VA system. Some women felt as though they needed to fight to get a device, and one woman stated her provider refused repairs. There was also a general inconvenience to women regarding receiving their device. Delivery times were long or inconsistent and pick-up distances were far. Other issues arose with maintenance with many being unaware of maintenance or follow-up options. Those who utilized maintenance services commented they were forced to follow up on service delivery or that their concerns were not addressed. Many women commented that their maintenance services were poor and required repeated follow-up requests, with one woman stating that maintenance fails to address repair concerns. “I don’t know if things have changed but women Veterans were treated like second class citizens.” (Manual Wheelchair) “Some of the people who work at the VA do not realize that they are here for us instead of the other way around. It took the mobility specialist three months to actually order my first chair after taking measurements.” (Manual wheelchair) “I really hate asking the VA to help with my chair. It takes too long. It’s just easier to go to a local shop to have anything fixed on my chair. I don’t live by a SCI Center, I feel the people at my VA have no clue to how important it is for me to have my chair. They think I can walk and get around without, and I can’t!” (Manual wheelchair)
Power wheelchairs
Equipment Issues: Women using power wheelchairs felt they were manufactured for men or not designed for the female anatomy. They had limited to no adjustability or in some cases had too many adjustments. Adjustments were hard to reach or required technicians to do them. Devices were bulky, too big or too heavy, and difficult to fit through doorways. The weight of the device limits transportation options and produces strain on their lift device. The device could roll on its own or would shut down randomly. The devices were not waterproof. The design of the charging systems made them difficult to use. Devices lacked lumbar support or sufficient cushioning and drove too slowly. They were ill-fitted, lacked customization and desirable features. Devices were cheaply made with loose or easily breakable parts and had a poor battery life. They required frequent adjustments or replacements. “It shuts down in the middle of the street […]; shut down once in middle of major intersection. I got stuck in a closet once because the sensor wouldn't let the seat lower after I raised it.” (Powerchair) “Positioning is critical. I have a particular problem with the seat being in contact with my lady parts all day. A seat specifically designed for a woman’s anatomy would be very helpful.” (Power wheelchair) “Can’t use it on my lift on my van. I have to use my older chair which is lighter” (Power wheelchair)
Usability issues: Many women who used power wheelchairs noted that it was difficult to use with their pre-existing medical conditions. Some stated that the device was difficult to adjust due to medical limitations, while others noted that it was difficult to operate due to vision impairments. Many women reported that their power wheelchair was inconvenient in their daily lives, noting that it was difficult to transport, not usable in public areas, and sitting in the wheelchair made it difficult to reach their surroundings. Travel on airplanes was also mentioned as a limitation. Several women commented that their power wheelchair was difficult to navigate on uneven terrain and difficult to use in varying weather conditions. Finally, some women stated that their device required them to seek further assistance, and that they were forced to use an alternative device. “I’m unable to use my wheelchair outside of my home because the weight is so heavy that I do not have a vehicle to transport it and the portable hoist needed to assist me.” (Power wheelchair) “Not effective since I can't use in in yard, on soft outdoor surfaces or take with me and use in everyday life outside my home since I have no means of transportation for it and the portable hoist is required.” (Power wheelchair) “As long as I always have someone with me, it can be made effective. I can’t use it effectively by myself.” (Power wheelchair)
Physical and Psychological Impacts: Women power wheelchair users reported that they felt limited in their independence, lifestyle, and participation in activities of daily living due to their wheelchair. The wheelchair also limited movement about the home due to poor home accessibility. Many women reported pain and discomfort with the use of their device as it relates to posture, with some noting that the wheelchair contributes to additional medical issues, including fatigue. They noted that their device feels unsafe and unstable. “Head rest not wide enough to allow for the tilted angle of my head in its most comfortable state of rest, current position places pain on nerves in head, neck and shoulders because it keeps my head at an unnatural angle (which is not perfectly in line with the rest of my body due to injuries).” (Power wheelchair) “It feels like I’m always leaning forward, it irritates my forearms and breaks out my behind and the back of legs.” (Power wheelchair) “I would like to have something that allowed me to go everywhere without having to change chairs.” (Power wheelchair)
Unmet Service Needs: Many women prescribed a power wheelchair commented on poor experiences with their healthcare providers, stating that they felt silenced by the VA, were dismissed for being a female Veteran, experienced rude interactions with staff, and were constantly forced to fight for their needs. One woman mentioned that there were inconsistent order submissions for her wheelchair. Several women had issues with delivery or procurement of their power wheelchair, describing that the process was difficult and slow. One woman purchased every part individually to avoid the service delivery. Most women who use power wheelchairs complained about problems with follow up services, indicating a lack of options, slow options, or poor-quality services. Some women stated that follow up options are not available to them at all. Those who had maintenance options said that the repair services were unresponsive, poor quality, and required frequent follow-up. One woman stated that her technician lacked knowledge on how to perform the required maintenance. “The VA treats me like an idiot and doesn't listen to anything I tell them.” (Power wheelchair) “The company that had been servicing my chair was absolutely terrible. They made mistakes and were generally incompetent.” (Power wheelchair) “Updating programming is usually impossible and understanding some of the quirks about the chairs never gets passed along to the new user because of the rushed processes.” (Power wheelchair) “Because women Veterans are put on the low priority lists, being told ‘well you can contact you congressman if you do not like it’. Or they tell those of us who are 100% service connected, use your own insurance, knowing that we do not get reimbursed for out-of-pocket expenses.” (Power wheelchair)
Scooters
Equipment Issues: Women using scooters felt they were not adapted to females, manufactured for males and their assembly was not compatible with their strength. They are hard to adjust or have no adjustability. Adjustments are difficult to reach. The devices are too bulky, too big, too heavy, too long, and too wide. They have low clearance (underneath) and can damage flooring. They are awkward to use and cause unwanted noise. They are ill-fitted and lack desirable features including seatbelts and a cushion. They can’t be brought onto planes, and they lack brakes. Scooters are cheaply made and break easily. They have missing parts or parts that require frequent replacements. “The 4 wheel scooter issued by the VA are large and heavy. Seems as they are intended for permanent use large men.” (Scooter) “I received a scooter thru the VA and though the weight is ok, the scooter came in pieces. Women are not as strong as [men] and with having MS our strength isn't that great. It would be great to have the folding scooter available instead of the scooter has to be put together. The folding scooter is somewhat lightweight and it doesn't require women to put together pieces of a scooter that is heavy. I wish I had one, especially when travelling. It takes about 10 mins to put together with help and longer without help.” (Scooter) “Large, cumbersome, translates into very heavy. I do have a lift, but have had issues in getting it on that, sometimes, because of the space needed to maneuver it onto the lift.” (Scooter)
Usability issues: Many women who use scooters complained that their device was inconvenient in their daily activities. Some women commented that it was difficult to transfer in and out of their scooter. They also reported that their scooter was difficult to use for long distances or long periods of time. Many women reported issues with day-to-day travel using their device, stating their scooter was difficult to: navigate in public places, use in real world conditions, load into their vehicle, maneuver, transport, adjust, and use on uneven terrain. Some women also complained that their device was difficult to understand. “I cant handle more than 1/2 hour sitting in the scooter.” (Scooter) “Hard to navigate stores, medical centers etc.” (Scooter) “I live out in the country. The school is a 3 wheeled scooter. Is extremely unstable on bumpy terrain. I haven't been on my lawn since I've gotten a scooter.” (Scooter)
Physical and Psychological Impacts: Some scooter users reported that their scooter caused discomfort or pain, primarily related to posture. Other women reported that the device made them feel unsafe, unstable, and stressed while using it. “I have to lean forward; hurts my posture.” (Scooter) “The adjustment knob for the steering handle is unsafe.” (Scooter) “It is also jarring on the slightest bump.” (Scooter)
Unmet Service Needs: Most women who commented on unmet service needs for their scooter discussed an overall lack of quality in education, delivery, and maintenance. Some women indicated they received no training for use of their scooter, with one woman indicating that she did not want a scooter and was prescribed one anyway. Delivery was poor, oftentimes delayed, slow, or inconsistent. One woman commented that delivery was not offered for her. Maintenance also remained a major issue, with miscommunication from service providers and inconvenient maintenance options. Some women commented that the maintenance received was incomplete or that they were denied VA coverage. Many women commented that they did not receive any maintenance or follow-up. Scooter users also had some user barriers to access, including no time for service repairs or that the required maintenance was out of their price range. One woman commented that she felt she was at fault for not communicating her concerns early on, and now feels stuck with her scooter. “I have a lift for this one, and no instructions were provided regarding loading the scooter on the lift.” (Scooter) “I had a 12+ year old scooter that needed to be replaced. It took over a year (16 months?) for my scooter to actually be replaced from the date it was requested by my doctor.” (Scooter) “I had three broken appointments by vendor. He made promises not kept.” (Scooter)
Gender specific concerns
Women Veterans were concerned with the mechanical design of their device and how it failed to reflect the female user’s body, abilities, and needs. They complained that the device was too heavy and using it was not compatible with the strength of a woman. Further, women Veterans complained that the device was ill-fitted, and the dimensions reflected the body of a male user. Scooter and manual and power wheelchair users felt as if their device was just simply not built or adapted for the use of women or their anatomy. Respondents utilizing a cane expressed dissatisfaction with the aesthetics of their device. I have a particular problem with the seat being in contact with my lady parts all day. A seat specifically designed for a woman’s anatomy would be very helpful.” (Power Wheelchair) Because women veterans are put on the low priority lists, being told well you contact your congressman if you do not like it.” (Power Wheelchair) Seems as if they are intended for permanent use by large men.” (Cane)
Discussion
This national study aimed to assess the satisfaction of women Veterans regarding their mobility device and the services that accompany it. The mixed model methods allowed both quantitative and qualitative analysis of satisfaction of these women Veterans. This approach permitted the identification of specific issues related to mobility devices and service; ones that would have been overlooked if only the QUEST scores were considered. The QUEST average and median scores did not communicate any distinct dissatisfaction amongst items or across device types. However, qualitative data uncovered numerous concerns and feelings of discontent with their device and related services. This finding presents an opportunity to evaluate the utility of the QUEST measure and its ability to gather important or relevant information in the context of device satisfaction and related problems. Indeed, a recent study noted a ceiling effect in the quantitative items of the QUEST that also skewed towards the higher end of the response scale similar to our study. 19 This calls into question the ability of the measure to fully tease out issues that may be problematic but are broadly considered to be manageable or acceptable within the context of device satisfaction. Future studies should be aware of the potential limitation in relying on the quantitative items on the QUEST to solely assess device satisfaction.
Average overall and sub-domain QUEST scores were high demonstrating that women across all device types have quite to very high levels of satisfaction for their device and the services they obtained through the VA healthcare system. Our findings are consistent with other studies involving both men and women that have found high levels of satisfaction with the QUEST across similar device type groups.20–24 While we could find no studies that involved only women, a few previous studies have assessed gender differences in QUEST scores. In a study comparing men and women leg orthosis users (n = 49; 47% women), QUEST scores were high and similar across both gender groups, with both groups similarly rating safety, effectiveness, and ease of use being most important factors to their satisfaction. 22 A study on rollator (walker) users (n = 89, 66% women) found women who used rollators were less satisfied with them than men who used the same device. 20 A German study with manual and power wheelchair users (n = 110; 55% women) found that male power wheelchair users indicated lower levels of satisfaction than female power wheelchair users for all items of the QUEST which they attributed in part to the men being ‘more critical’ of their device. 25 Without QUEST data present from a population of Veteran men, it is uncertain if our women Veterans vary in satisfaction from them; however, given the large number of comments of discontent that were left, women Veterans in our study seemed to score the QUEST less critically in comparison to their expression through their comments.
QUEST scores were similar across all device types with the exception of leg/foot orthoses users reporting lower levels of satisfaction in the dimension item score compared to power wheelchair users. Women left comments that they were rarely given women sizes and forced to utilize devices that only came in male sizing, commenting they were too heavy, too bulky, and ill-fitted for their body. The comments suggest that women who use orthoses desire a higher level of customization than what is currently being offered through the VA. Previous studies have shown that Veterans are more likely to feel satisfied with their device when it is customized to them and fits their unique needs.26,27 While similar complaints around dimensions were noted by the power wheelchair users (too bulky, too large, etc.) this may have had a lesser impact on their overall functional mobility compared to the orthotic users. 28 The lower dimension satisfaction scores among women orthotic users puts an emphasis on the importance of implementing a user centered design and fit of these devices to women rather than the prescription of “off the shelf” braces.
Women Veterans prioritized the comfort, ease of use, and safety of their device over all other factors when ranking the features most important to them. This finding is the same as that reported among a mixed group of women and men walker and manual and power wheelchair users (n = 209; 65% women). 23 Factors related to services in our study were ranked least important despite many comments indicating service-related concerns in the qualitative analysis. These rankings are supported by the relative overall numbers of comments left wherein each device type had a much higher proportion of comments regarding equipment issues compared to service issues. These findings indicate women Veterans prioritize device satisfaction over service delivery (procedures, length of time), professional services, follow-up services, and repair or maintenance services.
The qualitative portion of the survey prompted participants to comment on specific features of their device and service. As a result, some of the themes directly align with the comments and questions asked. However, the thematic analysis also uncovered themes that were not directly linked to questions asked. For example, none of the questions asked specifically about the physical and psychological impact the device had on participants, but many comments related to this aspect. Many of the themes extracted in this study align with other studies that have investigated service related problems in healthcare and thus are issues that are not all unique to the VA. 29
The qualitative findings present unique gender-specific concerns faced by women Veterans utilizing mobility devices. Many mechanical and service-related comments suggested that women were unhappy with how their device suited their strength and anatomy. These concerns reassert the need for gender-specific design changes and for devices to be better customized to meet women’s specific abilities, their lifestyle, and their needs.
There were numerous concerns about poor gender-specific experiences with the services offered by the VA. Power wheelchair users communicated feeling dismissed by service providers in clinical settings for being a female Veteran. One woman expressed that she felt at the bottom of the priority list when in need of professional services. Walker users found it difficult to receive care from VA providers in a male-centered system, a finding consistent with recent studies reporting that women Veterans often encounter gender bias and limited availability of women-specific services. 30 Finding service that is not adapted for men is difficult and women feel stuck with the options they are given for receiving these services. When women Veterans who use walkers pursue VA’s services, they receive services from male maintenance providers who they feel know little about the needs and lifestyles of women Veterans, aligning with broader findings of a lack of female providers and women-specific care within VA systems. 31 Further, manual wheelchair users expressed feeling discriminated against in VA healthcare settings for being women, which in turn, prevent them from utilizing these services. These concerns demonstrate the pervasive gender bias that remains prevalent in clinical settings. Despite advancements in assistive technology and the care that accompanies them, some women continue to leave clinical settings feeling out of options, ignored, and dismissed. 32 These concerns provide a foundation for the improvement and development of the services and providers, reflecting modernized and comprehensive care for women regarding assistive technology.
In addition to the several gender-specific concerns that were noted, it is possible that there are numerous issues that are not directly women specific but are less likely to be communicated by male Veterans or non-Veterans utilizing these mobility devices. While not specific to women, the likelihood of a user communicating concerns about the appearance of their device is potentially more prevalent in the female population. While discontent with the weight of their device or it being cumbersome and bulky does not directly reflect a gender-specific issue, devices that are not consistent with the bodies, the lifestyle, or the strength of female users may give rise to more concerns about these factors among women compared to men. Future work should focus on conducting semi-structured interviews with women Veterans to further understand the strengths and weaknesses of their mobility assistive technology and related services. Further, the research can include subtypes of mobility devices (such as subgroups of manual and power wheelchair users) for a more thorough analysis. For example, for some durable medical equipment (DME) such as a custom rigid frame manual wheelchair, specialty or expert credentials are required to assess and prescribe the device based on individualized needs and the service aspect of procurement is very different than for some other types of manual wheelchairs. For off-the-shelf items, such as a cane or walker, there may be very little detailed assessment or interaction with providers involved to understand nuanced needs of users, especially if the provider only provides a routine script that is not individualized. Further studies on these factors will allow for more detail on satisfaction (or dissatisfaction) with device and service-related factors.
Limitations
The open-ended feedback from the respondents does not always reflect the manner at which these women quantitatively rated the satisfaction items. Some respondents who communicated dire concerns about the functionality of their device, simultaneously rated the same corresponding satisfaction items high on the Likert scale. The reasons for this are unclear but it’s possible that the questions were not specific enough to rate poorly, and the open-ended platform allowed them to express more personalized issues they were having with their devices. Furthermore, response bias is inherent with the QUEST as comments can only be left by participants selecting a score less than 5 (very satisfied). This results in most comments to be negative and expressing sources of dissatisfaction, limiting comments capturing aspects of the device that work well. There is also the potential for selection bias in participants as those who feel less satisfied with their device may be more likely to participate and respond. Improvements in response rates for future efforts could be done by providing larger renumeration for participation in the study or more frequent follow-up reminder emails.
By including only women from the VA, the design limits how applicable these results are to non-Veteran women. In addition, the low response rate reduces the generalizability of the results to all women Veterans who received a mobility device through the VA. Data on race is largely missing from the dataset and thus it’s unclear if the results and sample are fully representative of the race distribution present in the women Veteran population. Further, there is no demographic data available for participants who did not respond to the survey, so it remains unclear if a certain demographic of women were less likely to respond. During the inductive coding process, despite instructions, many women commented on devices other than the ones they stated as their primary device. An effort was made to identify which device category the comment belonged to and to move that comment to the corresponding device category for analysis. Finally, men were excluded from this study, so no data were collected on male Veterans’ experiences with mobility devices. Therefore, any comparisons made between women and men mobility device users are based on external literature and not on internal study findings. This exclusion limits the ability to directly assess gender differences within the current sample.
Conclusion
Despite many women scoring high levels of satisfaction with devices and services received on the QUEST, thematic analysis of the open-ended comments revealed many problems with their device and the related services. Across all devices there were concerns related to the mechanical design being manufactured for men, the device not being adjustable or adjustable enough, and that they were bulky and heavy. They lacked customization to the user and desirable features; they had numerous usability issues particularly when trying to use the devices in various environments outside of the home and in wet and warmer climates. Device users suffer consequences in the form of pain, discomfort, or strain related to device use. The concerns expressed about mechanical design and physical/psychological impact emphasize that devices are not manufactured with gender specific end-user feedback in mind. The prevalence of significant service concerns in all device type groups emphasize the crucial call for reforming clinical services with regards to improving provider training and customer relations, timeliness of services and improved access to maintenance, repair and follow-up services.
Supplemental Material
Supplemental Material - Assessing women veterans’ satisfaction with mobility devices
Supplemental Material for Assessing women veterans’ satisfaction with mobility devices by Diya Kad, Jessica Stanley, Rutuja Kulkarni, Kelsey Berryman, Pooja Solanki, Frances M. Weaver, Brad E. Dicianno, and Alicia M. Koontz in Journal of Rehabilitation and Assistive Technologies Engineering
Footnotes
Acknowledgements
The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Ethical considerations
This study was approved by the Edward Hines, Jr VA Hospital Institutional Review Board (IRB), approval number 1574439, approval date: 8/20/2020 and the VA Pittsburgh HealthCare System, Human Subjects Subcommittee, approval number 1617402, approval date: 11/16/2020.
Consent to participate
Eligible women Veterans were mailed a letter and an information sheet describing the study and providing a link to the on-line Qualtrics survey. The letter and information sheet described the purpose of the study, why the individual was identified to receive a letter, and that all information provided will be anonymous as we will not be able to connect their responses to their identities. Further, it explained that participation is voluntary and if they choose not to participate that it will not affect their health care in any way. Completion of the survey signified the respondent’s consent to the one-time survey. Also, we had waiver of HIPAA to send information sheets to eligible women Veterans based on the VA Cooperate Data Warehouse list of persons who received mobility devices/equipment. Further, we had waiver of HIPAA and waiver of written informed consent for completion of the survey.
Author Contributions
Conceptualization: FW, BD, AK; Data curation: KB; Formal analysis: KB, DK, JS, RK, AK; Funding acquisition: FW, BD, AK; Investigation: FW, PS, BD, AK; Methodology: FW, BD, AK; Project administration: FW, BD, PS; Resources: FW, BD; Supervision: FW, BD, AK; Validation: AK; Visualization: DK, JS, RK; Writing -original draft: DK, JS, RK, AK; Writing – review & editing: KB, PS, FW, BD, DK, RK
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a SPiRE Award Number RX003452-01A1 from the United States (U.S.) Department of Veterans Affairs Rehabilitation Research and Development Service and a VA RR&D Service Research Career Scientist Award Project #1K6RX005030-01.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data can be made available upon request from the corresponding author (AK) and with an approved Data Use Agreement through the VA.
Supplemental Material
Supplemental material for this article is available online