
Abstract
Keywords
Introduction
Globally, neurological disorders account for 349 million disability-adjusted life years (DALYs), an epidemiological statistic of years lost due to premature death or time in less than complete health. 1 While 500,000 spinal cord injuries occur globally every year, 2 the incidence of stroke is much greater with one occurring every 3 seconds globally. 3 The impairments related to spinal cord injury and stroke, such as muscle weakness and sensory loss, may lead to limitations in activities such as walking, reduced participation in cardiovascular exercise, and increased sedentary time,3,4 all of which may lead to a reduced aerobic capacity and poor cardiovascular fitness.
Aerobic capacity in people with stroke is about half4–6 that of healthy but sedentary individuals of the same age and gender based on peak oxygen uptake, or VO2 peak. VO2 peak values for individuals with stroke (15 mL/kg/min) tend to be below the physical fitness threshold for independence (16-18 mL/kg/min) in activities of daily living.4,5,7 Similar VO2 peak values have been demonstrated in untrained individuals with spinal cord injury, but more so in those with tetraplegia (median = 9 mL/kg/min) than paraplegia (median = 16 mL/kg/min). 8 Consequently, individuals with stroke or spinal cord injury may experience greater levels of fatigue, and subsequent limitations in physical activity.8,9
A consequence of this aerobic deconditioning is an increased likelihood of cardiovascular disease. People with spinal cord injury are approximately three times more likely to develop heart disease as compared with their age-matched healthy counterparts, and are approximately four times more likely to have a stroke, 10 and 60% of people with stroke have cardiac comorbidities like hypertension, coronary artery disease, diabetes mellitus, and obesity. 7 Permanent disability resulting from spinal cord injury or stroke can further lower physical activity levels and exacerbate these modifiable risk factors of cardiovascular disease. Improving physical activity and exercise levels could help reduce the occurrence or prevent cardiovascular and metabolic comorbidities.11–14 Often, however, people with spinal cord injury or stroke do not have the opportunity to participate in recommended moderate-to-vigorous intensity exercise intensity due to barriers like decreased mobility, reduced community access preventing participation in exercise, and limited knowledge, resources and support for physiotherapists to enable safe and adequate cardiovascular training.15–17 Moderate-to-vigorous intensity exercise can be defined as corresponding to greater than 50% heart rate maximum (HR max) and/or a rating of perceived exertion (RPE) of greater than 11 on the Borg Rating Scale of Perceived Exertion. 18
The recent Evidence-based Scientific Exercise Guidelines for Adults with Spinal Cord Injury 19 recommend participation in at least 20 minutes of moderate-to-vigorous intensity aerobic activity twice a week for cardiorespiratory fitness.4–6 Despite these recommendations, only 12% of individuals with spinal cord injury reach the recommended intensity, frequency and duration of physical activity. 20 It is also important to note that 44% of individuals with spinal cord injury report that they are not participating in any physical activity throughout the week. 20
In contrast, the American Heart Association Exercise Guidelines for Stroke 4 recommends 20–60 minutes of moderate-to-vigorous intensity aerobic activity three to 5 days/week. People with stroke do not reach their target heart rate zones for about 95% of the total therapy time during their rehabilitation. 21 Outside of rehabilitation, individuals with stroke spend 41% to 98% of their time being inactive. 7
Assistive rehabilitation technologies, such as robot assisted gait trainers (RAGTs), provide an opportunity to improve access to aerobic exercise for people with spinal cord injury 22 or stroke. 23 The two broadly classified types of RAGTs, exoskeleton RAGT and end-effector RAGT (E-RAGT), differ mainly in the amount of support provided at the hip and knee joints. Both have been shown to increase gait training session times and steps taken per session, while decreasing manual handling by therapists. 24 Exoskeleton RAGTs have either a hip-knee joint or a hip-knee-ankle joint support to help replicate the gait cycle.23,25 E-RAGT, on the other hand, promotes active movement by only having the feet strapped to independent foot plates that move along mapped out paths, providing less control on the hip and knee joints,23,25 which may replicate a physiological gait pattern. 26
It remains unclear whether people with spinal cord injury or stroke can reach and sustain moderate-to-vigorous intensity exercise while using an E-RAGT. RAGTs may increase VO2 consumption levels above resting levels,
27
but it is unknown whether E-RAGTs enable individuals with spinal cord injury or stroke to achieve the recommended moderate-to-vigorous exercise intensity without the added support at the knees and hips of an E-RAGT which may encourage increased cardiorespiratory effort.6,27–29 Furthermore, it is unknown whether the use of E-RAGTs is enjoyable, which is critical to consider when prescribing exercise and enabling exercise adherence.
30
Therefore, the aim of this study was to determine: 1. What is the proportion of individuals with spinal cord injury or stroke that can achieve and maintain the moderate-to-vigorous intensity exercise recommendations in accordance with the Evidence-based Scientific Exercise Guidelines for Adults with Spinal Cord Injury,
19
or American Heart Association Exercise Guidelines for Stroke,
4
respectively, with the assistance of an E-RAGT? 2. How enjoyable is an exercise session with the assistance of an E-RAGT?
Methods
Study design and settings
An observational study assessing the same intervention in two different populations was conducted at Advance Rehab Centre, Sydney, NSW, Australia. The study was approved by the Macquarie University Human Research Ethics Committee (HREC reference number: 52021582832245) and is reported according to the STROBE statement for observational studies. All participants provided informed consent prior to participation. Briefly, participants included in the study underwent a session on the E-RAGT as part of their usual rehabilitation which also included some time with overground walking. The goal of the session on the E-RAGT was to improve walking and cardiovascular fitness.
Participants
People with stroke or with spinal cord injury were screened for eligibility between February and May 2022. Participants were included in the study if they completed at least four sessions on the E-RAGT to ensure familiarity with the device and be able to communicate in English. Due to the size restrictions on the E-RAGT, participants were excluded if they weighed less than 15 kg or more than 180 kg, and their height was less than 100 cm or more than 200 cm. To ensure safety when using the E-RAGT, participants were also excluded if they had highly pronounced vascular disease of the lower limbs, osseous instability (non-consolidated fractures, unstable spinal column, pseudoarthrosis), high grade ataxia, open body sites or skin lesions which meet the device, inability to follow instructions (communication impairments, cognitive impairments and history of behavioral impairments), severely restricted range of motion of the lower extremity (fixed joint contractures, joint arthrodesis), osteopenia or osteoporosis or had acute pain symptoms. Finally, participants with spinal cord injury were excluded if they had a complete injury at or above T4, which would prevent participants from safely mobilizing in the E-RAGT due to complete loss of motor control of the trunk and lower limbs.
Baseline characteristics
Demographic characteristics were recorded from electronic record system of the clinic and participants were required to complete questionnaires before participating. These included the Physical Activity Scale for Individuals with Disabilities (PASIPD) which measures self-reported levels of activity in the previous 7 days, 31 Falls Efficacy Scale-International (FES-I) which measures concern about falling in various tasks in the home and in the community 32 and the European Quality Of Life Scale (EuroQol) which measures quality of life.33,34
Intervention
Each participant was required to complete one monitored session on an E-RAGT (LEXO, Tyromotion, GmbH, Austria). Once transferred onto the E-RAGT, participants were given one to 2 minutes to get accustomed to the movement and ensure they were set up comfortably. The exercise session involved guiding the participant onto the E-RAGT, where their feet were strapped onto the bilateral foot plates while the E-RAGT was static. Participants were secured with a harness at the height of their pelvis. The harness was used to modify the amount of body weight support, which was individualized for each participant. The E-RAGT has a passive mode, in which walking parameters are pre-set, or the E-RAGT could be autonomously driven via an active mode. In the passive mode, the speed cadence, step width and length could be manually set. In both modes, participants were encouraged to work with the machine to improve walking biomechanics as advised by the physiotherapist (e.g., focusing on foot clearance). It was up to the participants and physiotherapist which mode was selected. A screen was used by participants as visual feedback about spatiotemporal features of walking (e.g., walking in a scene, shifting weight, heel strike). The amount of time participants spent on the E-RAGT was decided jointly by the participant and the physiotherapist.
Prior to the intervention, participants were fitted with a heart rate monitor on the unaffected (if applicable) forearm (Polar OH1, Polar Electro, Kempele, Finland) which has previously been validated for use in moderate-to-vigorous intensity exercise.35,36 It was attached to the Polar Flow App which connected to an iPad via Bluetooth (Apple, Cupertino, CA, USA) and allowed remote monitoring of heart rate every minute.
Perceived exertion was recorded separately for dyspnea and lower limb fatigue at rest and every minute while exercising using the Borg Rating Scale of Perceived Exertion.37,38 Following the completion of the session, participants were required to rate their overall fatigue throughout the session as well as their overall enjoyment of the session.
Primary outcome
The primary outcome was the proportion of participants that reached and maintained moderate-to-vigorous intensity exercise in accordance with guidelines for each condition.
Based on a position statement on physical activity and exercise intensity terminology,
39
participants were considered to have reached moderate-to-vigorous intensity exercise if they reached any of the following threshold for at least 1 minute: - Based on dyspnea: moderate intensity exercise was rated between 11 and 13 and vigorous intensity 14–16 or higher on the Borg Rating Scale of Perceived Exertion. - Based on lower limb fatigue, using the same method as for dyspnea. - Based on heart rate: moderate intensity was defined as 55%–69% of HRmax while vigorous intensity was 70%–89% or higher of HRmax.
For both conditions, HRmax was calculated using the formula 206.9 – 0.67 × age which was adjusted for participants on beta blockers (164 – 0.7 × age). 6 Bouts of rest were excluded from the analysis.
People with spinal cord injury were considered to have reached the Evidence-based Scientific Exercise Guidelines for Adults with Spinal Cord Injury 19 if they reached at least 20 min of moderate-to-vigorous intensity exercise during the session.40–43
People with stroke were considered to have reached the American Heart Association exercise guidelines for stroke if they also reached at least 20 minutes of moderate-to-vigorous intensity exercise during the exercise session.4,18
Secondary outcome
At the end of the session, participants were requested to rate their overall fatigue (Borg Rating Scale of Perceived Exertion) and their level of enjoyment on a five-point Likert Scale (from one-not at all enjoyable to five-extremely enjoyable).
Statistical analysis
Demographic characteristics, description of the session on the E-RAGT and participants’ level of enjoyment were reported as median (IQR). The duration of bouts of exercise at different levels of intensity was also reported as individual participant data. The proportion of participants who reached and maintained moderate-to-vigorous intensity exercise were reported as a count (%). Statistical analysis was performed using Prism 8 software (GraphPad, San Diego, CA, USA).
Results/findings
Participants
25 participants were screened for eligibility and five people with spinal cord injury and ten people with stroke agreed to participate (Figure 1). Their baseline demographic characteristics are shown in Table 1. Briefly, four were women (26%) and their median age was 59 (IQR 46 to 66) years. The mean time since disease onset was 12.4 (SD 9.0) years for spinal cord injury, and 4.2 years (SD 2.8) years for stroke. Ten participants (67%) were able to walk and 11 (73%) experienced at least one fall in the previous twelve months. All participants with spinal cord injury had incomplete injuries. Participant flow chart. Demographic characteristics of the participants. PASIPD = physical activity scale for individuals with disabilities, EuroQol = European quality of life scale, FES-I = fall efficacy scale – international. Data are shown as median (IQR) or count (%). aData are not mutually exclusive as some participants used more than one type of walking aid. bData were available for eight out of ten participants with stroke. cIndex values were based on the United Kingdom value set.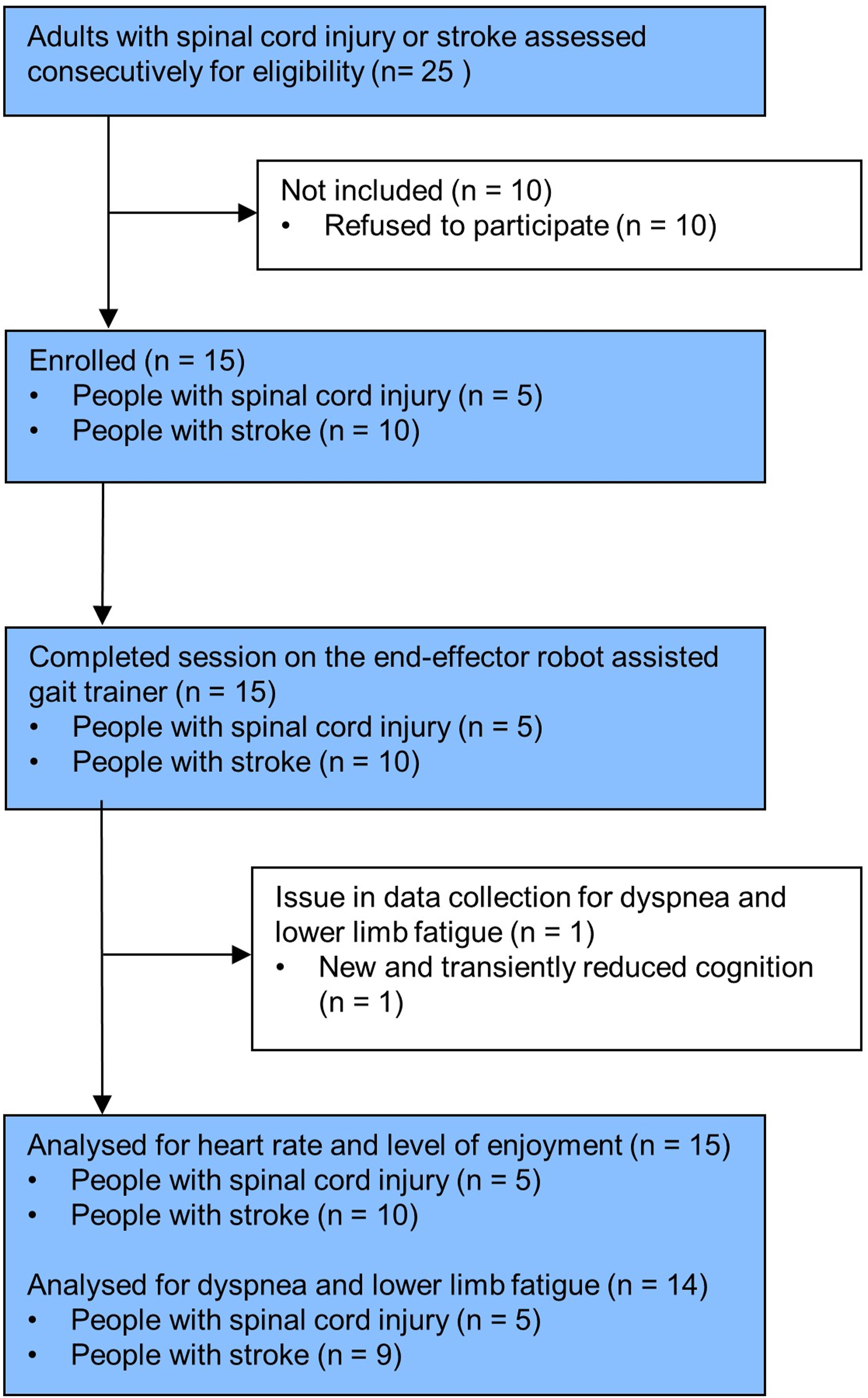

Exercise session on the end-effector RAGT
Description of the exercise session on the end-effector robot assisted gait trainer.

Data are shown as median (IQR) or count (%).
aThis percentage refers to the overall time that the person shifted their weight to the left or right when using the gait trainer.
Primary outcome
Spinal cord injury
Based on dyspnea, five out of five participants reached moderate-to-vigorous intensity exercise for a median duration of 20 (IQR 7 to 23) minutes and three participants (60%) were able to maintain this intensity for at least 20 minutes (Figure 2(A)). Individual participant data for time spent exercising at different exercise intensity thresholds based on Borg rating scale of perceived exertion for people with spinal cord injury according to (A) dyspnea and (B) lower limb fatigue and for people with stroke according to (C) dyspnea and (D) lower limb fatigue.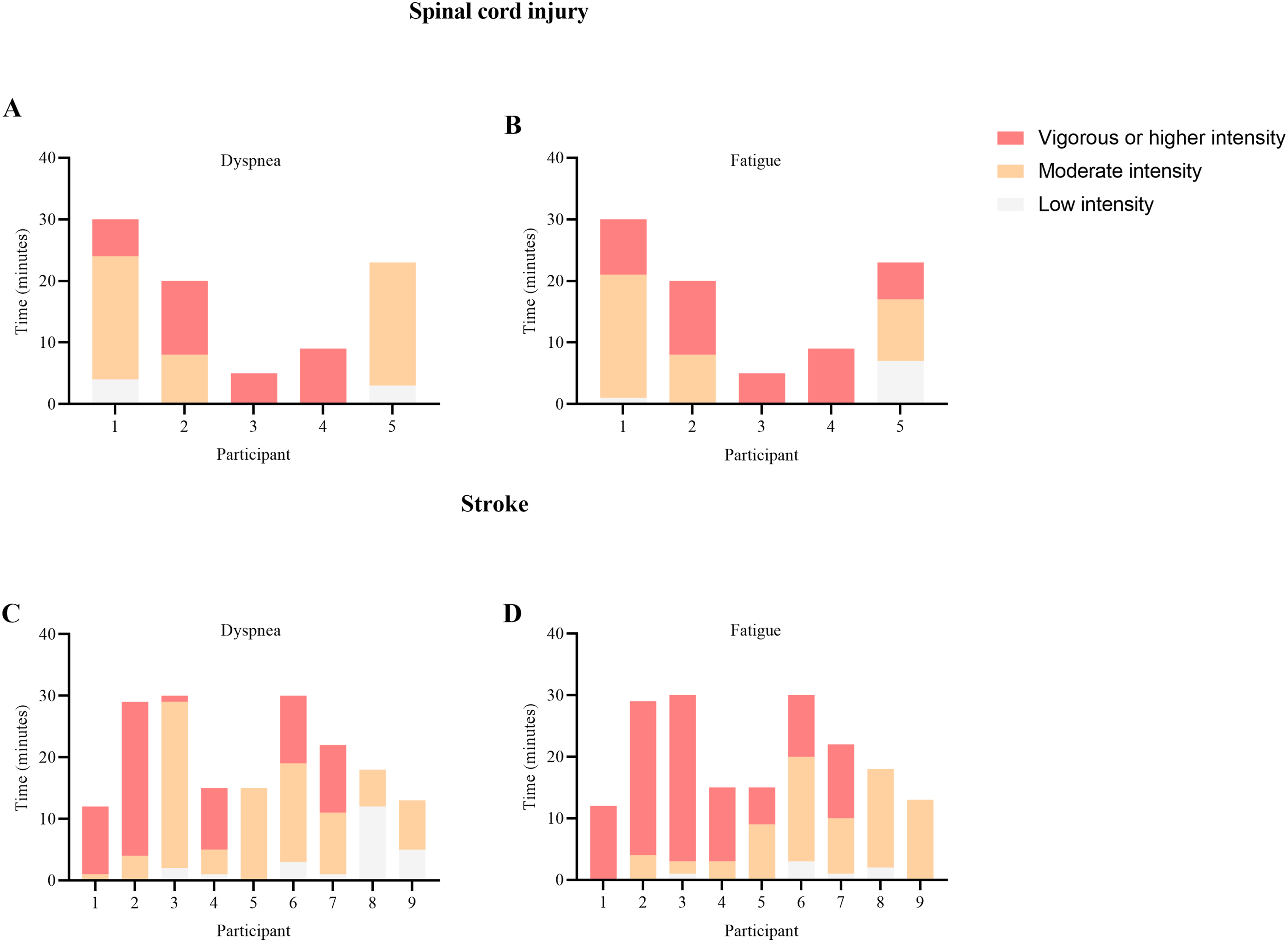
Based on lower limb fatigue, 100% of the participant also reached moderate-to-vigorous intensity exercise for a median duration of 16 (IQR 7 to 25) minutes. Two participants (40%) were able to maintain this intensity for at least 20 minutes (Figure 2(B)). Moreover, these two participants were also able to maintain moderate-to-vigorous intensity exercise for at least 20 minutes based on dyspnea level.
Finally, based on heart rate, each participant also reached moderate-to-vigorous intensity exercise for a median duration of 20 (IQR 4 to 26) minutes. Three participants (60%) were able to maintain this intensity at least 20 minutes (Figure 3(A)). Among them, three participants and two participants were also able to maintain moderate-to-vigorous intensity exercise for at least 20 minutes based on dyspnea and lower limb fatigue levels, respectively. Individual participant data for heart rate during exercise for (A) people with spinal cord injury and (B) people with stroke.
Altogether, 100% of the participants reached moderate-to-vigorous intensity exercise and three (60%) were able to maintain this intensity for at least 20 minutes. The median aggregated exercise duration at moderate-to-vigorous intensity based on at least one of the thresholds was 20 (IQR 7 to 26) minutes.
Stroke
From the session data, perceived exertion for one participant was eliminated due to new and transiently reduced cognition impacting ability to respond but their heart rate data was included in the analysis.
Based on dyspnea, nine out of nine participants (100%) reached moderate-to-vigorous intensity exercise for a median duration of 15 (IQR 10 to 28) minutes and four participants (44%) were able to maintain this intensity for at least 20 minutes (Figure 2(C)).
\Based on lower limb fatigue, nine out of nine participants also reached moderate-to-vigorous intensity exercise for a median duration of 16 (IQR 14 to 28) minutes with four participants (44%) able to maintain this intensity for at least 20 minutes (Figure 2(D)). Among these four participants, all were also able to maintain moderate-to-vigorous intensity exercise for at least 20 minutes based on dyspnea level.
Finally, based on heart rate, eight out of 10 participants (80%) participant reached moderate-to-vigorous intensity exercise for a median duration of 12 (IQR 6 to 23) minutes with three participants (30%) able to maintain this intensity for at least 20 minutes (Figure 3(B)). These three participants were also identified as able to maintain moderate-to-vigorous exercise intensity for at least 20 minutes based on either dyspnea and lower limb fatigue levels.
Altogether, nine participants (90%) were able to reach moderate-to-vigorous intensity exercise and four were able to maintain this intensity for at least 20 minutes. The median aggregated exercise duration at moderate-to-high intensity based on at least one of the thresholds was 16 (IQR 13 to 27) minutes, which corresponded to 100% (IQR 99 to 100) of the total exercise duration for a given participant.
Secondary outcome
At the end of the session, people with spinal cord injury and stroke rated their overall fatigue at a median score of 16 (IQR 14 to 16) and 15 (IQR 13 to 15) on the Borg Rating Scale of Perceived Exertion, respectively.
Finally, participants rated the session as enjoyable with a median score of 4 (IQR 3.5 to 5) and 4 (IQR 3 to 4) for people with spinal cord injury and stroke, respectively, which corresponded to “very enjoyable”.
Discussion
This pilot study showed that individuals with spinal cord injury or stroke can achieve moderate-to-vigorous exercise intensity according to disease-specific exercise guidelines when walking on a E-RAGT, but some individuals may have difficulty maintaining this intensity for at least 20 minutes. Most participants found training on a E-RAGT very enjoyable, highlighting the potential for E-RAGT to increase participation and adherence to cardiorespiratory training.
Our findings are comparable to other studies exploring how robotic assisted gait training may enable patients to reach moderate-to-vigorous exercise intensity using other types of gait trainers. Prideaux et al. 5 found that all 10 participants with subacute stroke were able to achieve and maintain moderate-to-vigorous intensity exercise on an exoskeleton RAGT. It is likely that all the participants in the study by Prideaux et al. 5 had higher levels of cardiovascular fitness given that the average time since stroke was 32 days, whereas the median time since stroke was 4.2 years in our study. In relation to spinal cord injury, Hoekstra et al. 44 showed that only two out of 10 participants reached moderate intensity exercise according to metabolic equivalents (METs) in their study. This proportion is lower compared to our study, which may reflect differences in measures of exercise intensity. Because gas exchange analyzers are not readily available in neurological rehabilitation clinics, our study was designed pragmatically when assessing exercise intensity by using heart rate and perceived exertion. Future research may need to replicate our methodology using METs as the measure of exercise intensity in individuals with spinal cord injury.
Though most participants were able to achieve moderate-to-vigorous exercise intensity, less than half of them were able to maintain this intensity long enough to reach the recommendations for people with neurological conditions. It is possible that they were not able to maintain this training intensity because they were generally untrained, had low mobility and had low levels of self-reported physical activity, probably due to the chronic nature of their conditions, with the minimum time since disease onset being 2.3 years (Table 1). Additionally, we assessed participants on their fifth session on the E-RAGT. It is possible that a larger number of sessions of cardiovascular fitness training would have allowed more participants to reach and maintain the recommended exercise threshold. Further research is required to determine whether a targeted cardiovascular training program on the E-RAGT can improve fitness and maintenance of moderate-to-vigorous exercise intensity compared to other types of exercise.
Despite the difficulty with maintaining moderate-to-vigorous intensity exercise observed in participants in this study, low intensity physical exercise training in untrained individuals may be sufficient to improve cardiovascular fitness. 44 This is reassuring for the participants in our study, who generally had low cardiovascular fitness as demonstrated by their self-reported physical activity levels. Additionally, exercising on the E-RAGT may still be able to improve some other outcomes, including muscle strength, functional capacity, and quality of life. Further research is required to determine the added cost-effectiveness of E-RAGTs compared to other approaches to improving cardiovascular fitness in people with stroke 45 or spinal cord injury, 12 particularly as RAGTs are not yet widely available globally.
Strengths and limitations
This was the first study to look at whether people with spinal cord injury or stroke can achieve and maintain moderate-to-vigorous exercise intensity with the help of an E-RAGT. We used subjective and objective measures of exercise intensity that are readily available in neurological rehabilitation clinics and found that fitness training using E-RAGTs may be feasible in this population.
A limitation of this study includes potential over-estimating exercise intensity and duration by aggregating all three criteria. Interestingly, the agreement between the methods used to determine exercise intensity was strong for people with spinal cord injury. Indeed, all participants reached thresholds for moderate-to-vigorous exercise intensity with each measure, and the same participants were also identified as having maintained this intensity for at least 20 minutes with each measure, except one participant who maintained at least 20 minutes based on dyspnea and heart rate but only 16 minutes based on lower limb fatigue. The agreement between perceived dyspnea and lower limb fatigue measures was also strong in identifying people with stroke who reached and maintained moderate-to-vigorous intensity exercise as prespecified thresholds consistently identified the same participants who reached and maintained 20 minutes of moderate-to-vigorous exercise intensity. Agreement between these measures and that of heat rate was, however, weaker. Prespecified threshold based on heart rate identified less participants who reached moderate-to-vigorous exercise intensity and did not identify one participant who was able to maintain at least 20 minutes of moderate-to-vigorous intensity exercise using thresholds from other measures. The use of beta-blockers did not seem to result in less agreement in measures in the one participant. Therefore, our results highlight the importance of the use of multiple measures of exercise intensity rather than a single measure in research and clinically in this population with potentially heart rate modulating treatments or autonomic disorders. Additionally, discrepancies in measures of exercise intensity in different neurological populations suggest the need for disease-specific measures for exercise intensity.
Another limitation is this study is the small sample size. In this context, inferential statistics were deemed inappropriate which may limit the generalizability of the findings. Generalizability was further limited as eligibility criteria was restricted to those with minimal co-comorbidities. Further studies should explore whether E-RAGT may be offered to people irrespective of co-morbidities, as E-RAGT may provide a safer option for people with more serious co-morbidities to engage and benefit from cardiovascular fitness training.
Implications on physiotherapy practice
Individuals with spinal cord injury or stroke who use an end-effector robot assisted gait trainer can reach moderate-to-vigorous exercise intensity, but not all individuals are able to maintain this intensity of exercise for the disease-specific recommendations of 20 minutes. Nevertheless, given that most people with spinal cord injury or stroke are untrained, the use of robot assisted gait trainers in improving cardiovascular fitness may be feasible, safe, and enjoyable. Moreover, targeting cardiovascular fitness by using accessible technology such as end-effectors may enable a feasible and safe method to improve DALYs in this population. Future research should explore the effectiveness of a targeted training program using an E-RAGT to improve cardiovascular fitness and reduce cardiometabolic risk factors in people with spinal cord injury or stroke.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tristan BONNEVIE declares receiving grants from Fisher and Paykel Healthcare, unrelated to this study. Tristan BONNEVIE declares personal fee from Asten Santé and other from KerNel Biomedical, both unrelated to this study. All other authors do not declare any conflict of interests related to this study. Melissa MCCONAGHY is the Director of Advance Rehab Centre, where the robotic assisted gait trainer (i.e., LEXO®) is being used as part of therapy with clients. MCCONAGHY was not involved in the screening of potential participants, recruitment, or data analysis of this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Dr. Emre Ilhan.
Author contributions
All authors has made substantial contributions to conception and design, or acquisition of data, or analysis and interpretation of data. All authors has drafted the submitted article or revised it critically for important intellectual content. All authors has provided final approval of the version to be published. All authors has agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.