
Abstract
Introduction
Spinal cord injury (SCI) is a complex and debilitating condition that significantly impairs both motor and sensory function, leading to profound challenges in mobility and independence. 1 The National SCI Statistical Center reports approximately 17,000 new cases of SCI annually in the United States, with many individuals facing lifelong consequences. 2 The severity of these injuries varies widely, affecting not only physical capabilities but also psychological well-being and social participation. Despite advancements in medical care and rehabilitation techniques, many individuals with SCI struggle to regain full mobility. 3
Traditional rehabilitation methods often emphasize physical therapy and surgical interventions; however, achieving functional independence remains a significant challenge. 4 Orthotic devices play a crucial role in enhancing the mobility of individuals with SCI. 5 Notable examples include the Prime-Walk, one of the first orthoses introduced in the category of medial linkage orthoses, which, despite its innovative design aiming to align the orthotic joint with the anatomical joint, lacks reciprocating capabilities, limiting its effectiveness in mimicking natural gait patterns. 6 In contrast, the Medial Linkage Reciprocal Gait Orthosis (MLRGO) has been developed with a geared mechanism that allows reciprocating movements between the thighs, promoting more coordinated leg movement and a more natural gait. 7 Efforts have been made in the design to align the joint axis with the anatomical joint axis, although this alignment varies at different positions, indicating a trade-off between functional mobility and anatomical fidelity.
Together, these devices represent significant advancements in assistive technology, thereby improving mobility and functional independence for patients with SCI. 8 Since their inception in the 1990s, orthotic devices have continued to evolve, with various models being introduced to address the limitations of earlier designs. However, many existing models suffer from drawbacks, such as limited range of motion, inadequate stability, and excessive mechanical complexity, which can hinder user acceptance and overall effectiveness. 9
The Advanced MLRGO integrates the principles of orthotics and biomechanics, features reciprocating capabilities, and a medial linkage for the thighs, while emphasizing user-centered design. The precise alignment of the rotational and anatomical axes enhances stability and facilitates natural movement patterns. This optimization improves walking speed, distance, and ease of use, ultimately providing greater comfort and effectiveness for users.
This study aimed to evaluate the performance of the Advanced MLRGO in comparison with existing medial linkage orthoses, specifically, the Prime-Walk and MLRGO models. Through rigorous testing and analysis, we sought to demonstrate the potential of Advanced MLRGO to significantly enhance the mobility and functional independence of individuals with thoracic SCI.
Methods
Study design
This study employed a semi-experimental, single-subject design to evaluate advanced MLRGO in patients with thoracic SCI. The research was conducted in compliance with ethical standards, and informed consent was obtained from all participants.
Participants
Five participants aged 25–45 years with diagnosed thoracic SCI were recruited for the study. The inclusion criteria were: diagnosis of complete or incomplete thoracic SCI, ability to follow instructions and participate in the evaluation process, and absence of significant comorbidities affecting mobility. The exclusion criteria included Presence of orthopedic conditions affecting the lower extremities and history of skin integrity issues related to orthotic use.
Orthosis design and fabrication
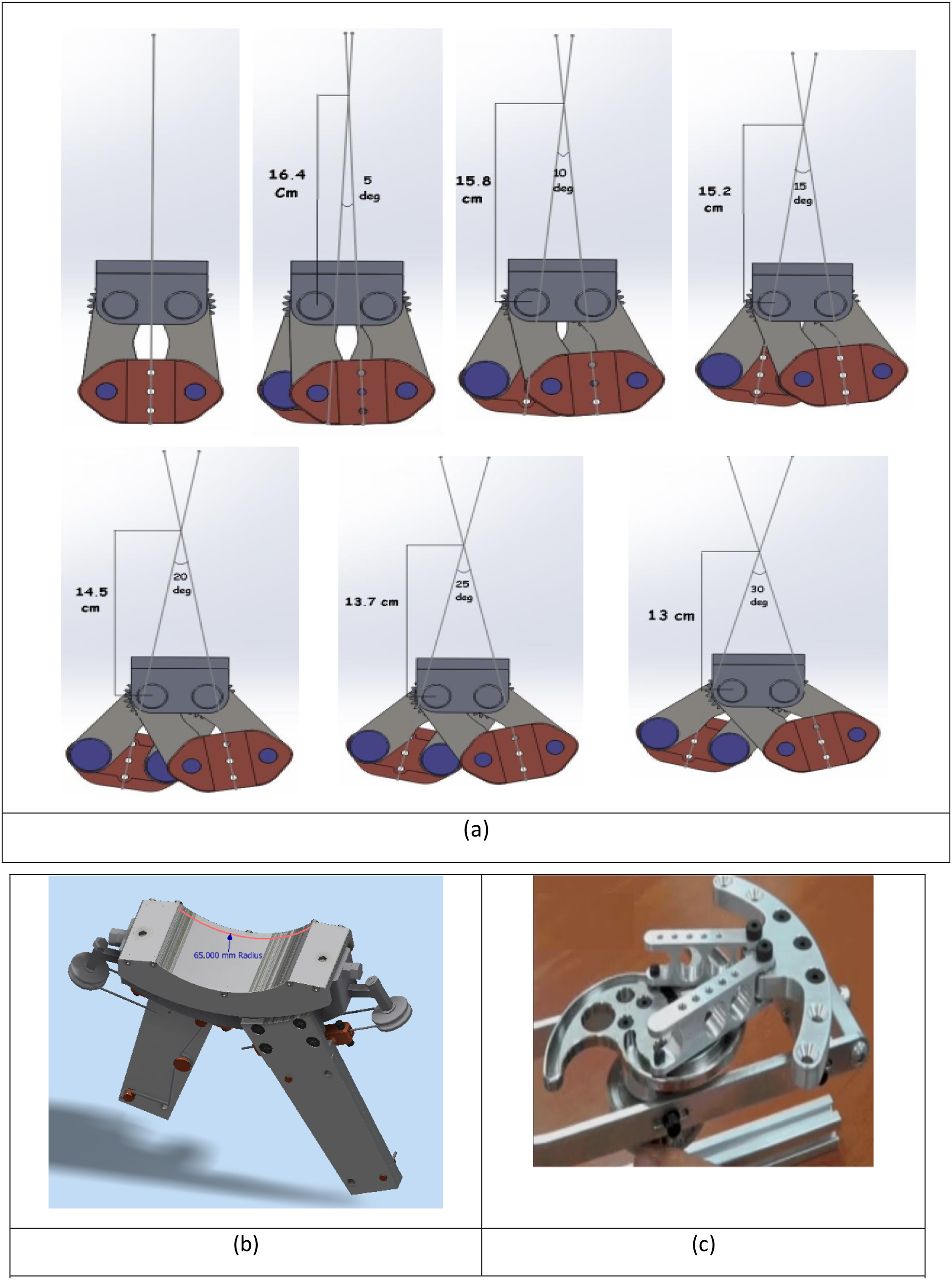
The Advanced MLRGO was designed using Autodesk Inventor Professional and analyzed in COMSOL Multi-physics for static, dynamic, and fatigue assessments. The design process includes the following steps 1. Geometric Optimization: Inspired by existing medial linkage orthoses (e.g. Prime-Walk), the Advanced MLRGO’s dimensions were minimized, particularly its width, which was reduced to 56 mm compared to 60 mm for the MLRGO. 2. Mechanical Structure: The Advanced MLRGO’s hypothetical axis was positioned 65 m from the seating point, aligning closely with the hip axis, in contrast to the MLRGO’s maximum distance of approximately 16.4 cm. 3. Material Selection: The Advanced MLRGO was constructed from aluminum 7075, stainless steel 304, and brass to balance durability and weight. The total weight of the Advanced MLRGO was approximately 1.1 kg, which is significantly below the maximum acceptable limit of 2.5 kg. 4. Reciprocal Mechanism: The Advanced MLRGO integrates three identical conical gears to facilitate reciprocal motion, enhance efficiency, minimize energy loss, and reduce friction and bulkiness (Figure 1). (a) The change in the joint axis location in the MLRGO orthosis as a function of the angle between the two legs, (b) location of the hypothetical axis of the designed orthosis, (c) use of hinged and sliding systems and gears.
Simulation and analysis
Static analysis
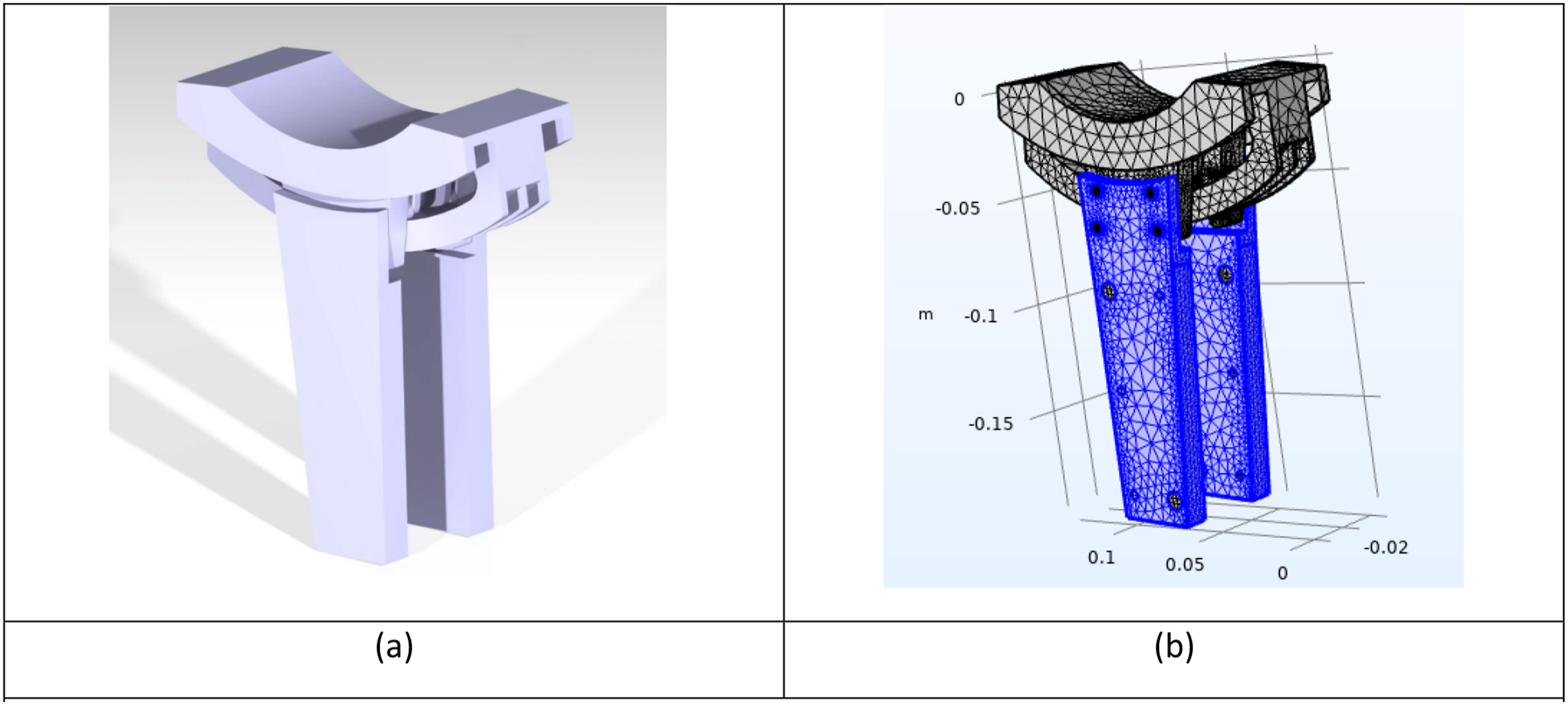
Static simulations were conducted in COMSOL Multi-physics to evaluate the structural integrity of the advanced MLRGO under load. Key aspects: -Force Application: A force of 910 N was applied, corresponding to a safety factor of 1.3, with boundary conditions reflecting the user’s weight and orthotic components. -Meshing: The component was meshed with a focus on areas sensitive to load to ensure accuracy (Figure 2). (a) Orthosis meshing for static and dynamic analysis, (b) simplified form of the model for simulation.
Dynamic analysis
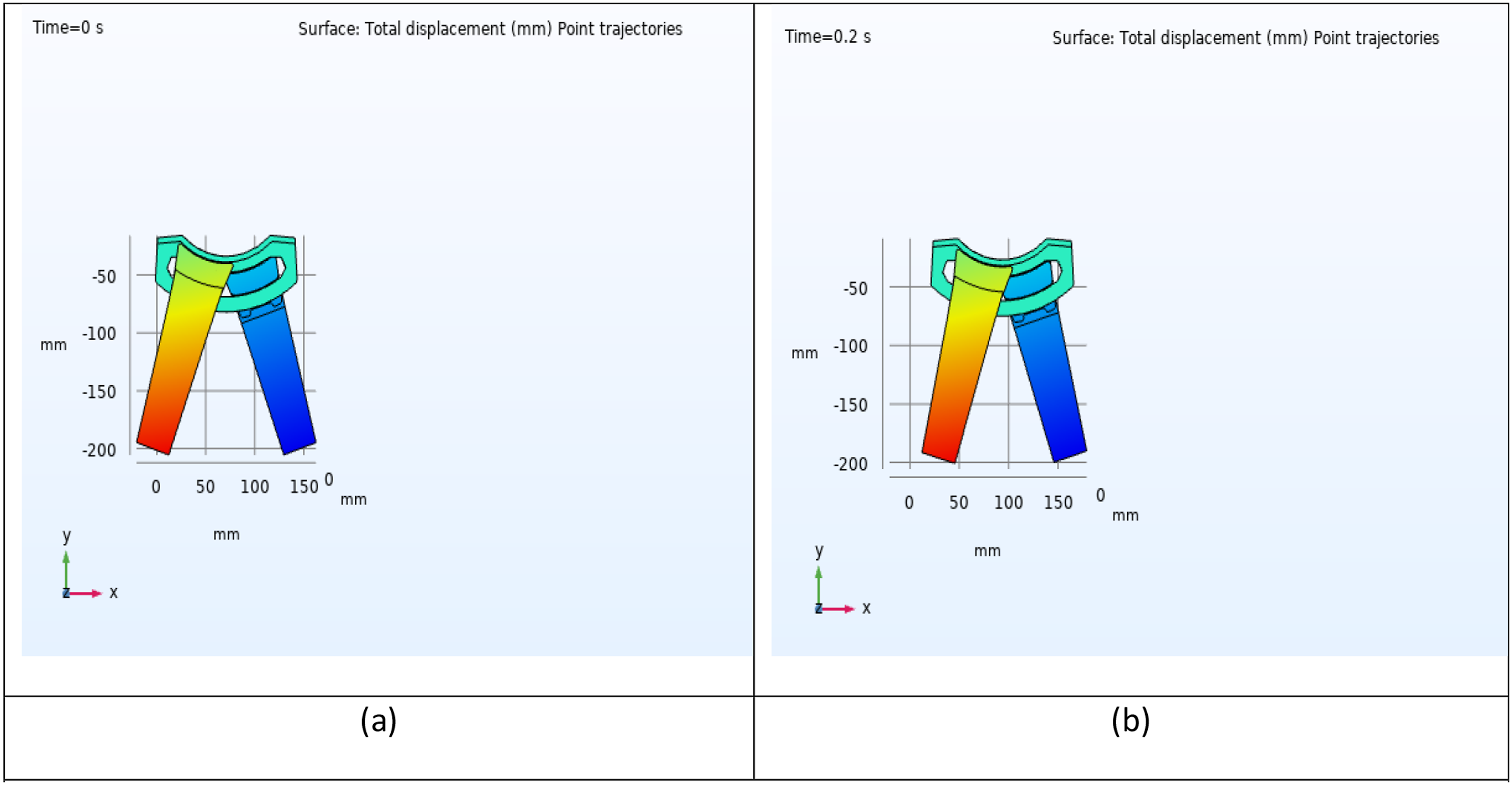
Dynamic simulations used the multi-body dynamics physics module in COMSOL to analyze the interactions between the orthosis and user walking pattern. Key elements included - Parametric Inputs: The proposed design allows for adjustments based on anthropometric data, thereby enabling customization for various user anatomy (Figure 3). (a) Displacement rate at the beginning of the movement cycle (displacement rate in 0.21 s).
Fatigue analysis
Fatigue assessments evaluated the Advanced MLRGO’s durability under cyclic loading conditions. This included: - Torque Application: The torque from the force analysis was applied to critical links, ensuring that component thickness maintained a safety factor of 8 or higher. - Cyclic Loading Conditions: Two loading states were simulated for real-world usage, and stress fatigue models were defined to evaluate the component lifespan (Figure 4). Swing foot force diagram.

Performance evaluation
Performance metrics were evaluated using standardized tests to compare the Advanced MLRGO model with the Prime-Walk and MLRGO models. Evaluations were performed as follows 1. Walking Speed: Assessed using the 6-Meter Walking Test, in which participants walked a distance of 6 meters, and their speed was recorded in meters per second. 2. Travel Distance: Measured using the 2-min walking test, which quantifies the distance covered in meters. 3. Donning/Doffing Times: The durations for participants to don and doff the orthosis were recorded in seconds.
Data analysis
Data were analyzed using SPSS via paired t-tests to compare performance metrics across the three orthotic models, with a significance threshold set at p < 0.05. Descriptive statistics summarize participant demographics and performance outcomes, including means and standard deviations.
Results
The study evaluated the performance of the Advanced MLRGO through two sub-studies: the first comparing the Prime-Walk orthosis with the standard MLRGO, and the second comparing the MLRGO with the advanced MLRGO.
Sub-study 1: Prime walk versus MLRGO
Walking speed and distance
Participants using the MLRGO method achieved a statistically significant increase in walking speed compared with the Prime-Walk method, with a mean walking speed of 0.045 m/s for the MLRGO method versus 0.036 m/s for the Prime-Walk (p = 0.03). In terms of distance traveled during the 6-min walking test, participants covered an average of 11.07 m with the MLRGO compared to 9.25 m with the Prime-Walk, reflecting a 19.64% increase in distance (p = 0.04).
Donning and doffing times are as follows
The MLRGO system exhibited an 8.5% reduction in average donning time compared to the Prime-Walk system, with mean times of 202.34 s versus 219.53 s, though this was not statistically significant (p = 0.059). Doffing times were similar between the two devices, showing no significant differences (MLRGO: 124.52 s; Prime-Walk: 123.53 s, p = 0.17).
Sub-study 2: MLRGO versus advanced MLRGO
Walking speed and distance
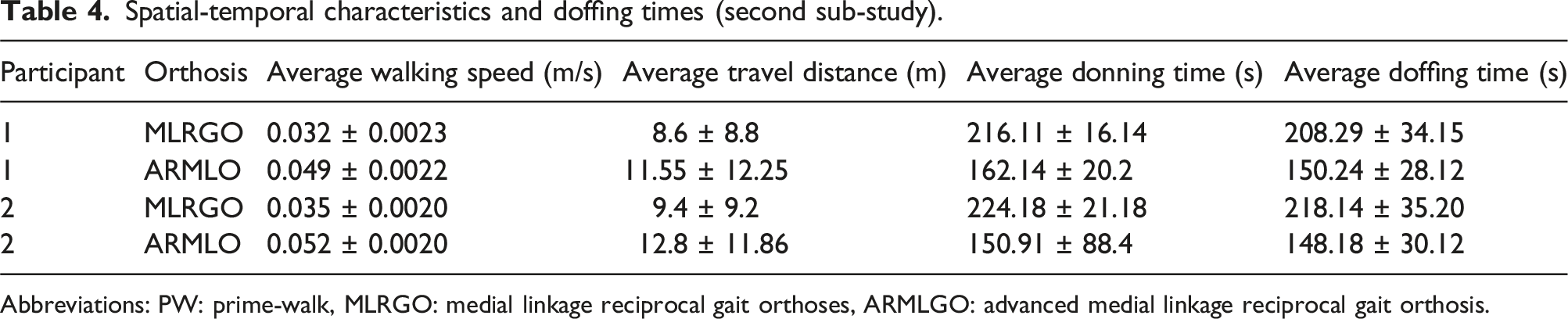
The advanced MLRGO method showed a substantial improvement in walking speed compared to the standard MLRGO method, with participants achieving an average speed of 0.0505 m/s for the advanced MLRGO method versus 0.0335 m/s for the MLRGO method, indicating a 50.7% increase (p = 0.033). The distance traveled also significantly improved, with participants covering an average of 12.18 m using the advanced MLRGO compared to 9.00 m using the MLRGO, resulting in a 35.28% increase in distance (p = 0.026).
Donning and doffing times
The advanced MLRGO demonstrated a significant reduction in the donning time compared to the standard MLRGO, with a mean donning time of 156.52 s for the advanced MLRGO and 220.145 s for the MLRGO, reflecting a 28.9% improvement (p = 0.048). However, the doffing times for the advanced MLRGO method increased by 30.02% compared to the MLRGO method, although this change was not statistically significant (advanced MLRGO: 149.21 s; MLRGO: 213.215 s, p = 0.064).
Discussion
The present research has provided sufficient evidence on the efficacy of Advanced MLRGO, a new medial linkage orthosis, in enhancing the mobility and functional independence of patients with thoracic SCI. Comparative analyses led to the identification of certain significant improvements over already existing orthoses-like Prime-Walk and the standard MLRGO in terms of walking speed and traveled distance, as well as the efficiency of donning and doffing. Results of the first sub-study revealed that participants using the Prime-Walk and MLRGO orthoses exhibited a 19.64% increase in distance covered during the 6-min walking tests with MLRGO. These differences can be explained by specific design features inherent in these devices, namely that the MLRGO allows for reciprocal movements, which are not provided in the Prime-Walk device. Orthotics with reciprocal mechanisms are more closely approximating the normal gait cycle, thereby allowing a more effective walking pattern, which could account for the higher efficacy of MLRGO. 7 Within the second sub-study, the Advanced MLRGO showed an astonishing 35% increase in the distance traveled compared to the standard MLRGO. This represents not only improved mobility but also a reflection of how design changes in Advanced MLRGO can optimize its kinetic and kinematic parameters. These parameters are important because they determine the degree to which the orthosis positively engages the user’s biomechanics while ambulating. Improved joint alignment and energy transfer mechanics may significantly improve these features, enabling users to achieve more productive walking. This is further reinforced by the analysis of the participants’ walking speeds, which showed a 25% increase with the MLRGO compared to the Prime-Walk and an impressive 50.7% enhancement with the Advanced MLRGO over the standard model. Such a large increase in walking speed points to a significant result because higher walking speeds are consistently associated with superior functional cardiovascular health, superior overall functional independence, and quality of life for individuals with spinal cord injury. In addition, higher walking speeds often equate to less fatigue and energy expended, which could provide a longer period of mobility and enable participation in activities. 10 Another important set of metrics is functional independence donning and doffing times. The MLRGO demonstrated an 8.5% reduction in the average time to use the device compared to the Prime-Walk. The Advanced MLRGO model improved on this metric even further, demonstrating an average 29% reduction in the donning time relative to the standard MLRGO. The most important finding is that the obtained results improve the efficiency of orthoses and highlight the usability of assistive devices. Efficient use of don and doffing is elemental to users, whereas ill-fitted equipment discourages proper use, thus obviating the potential benefits of the orthosis. Doffing time with the Advanced MLRGO method shows a 30% increase, which is a negative characteristic because it is not statistically significant compared to the MLRGO. Longer follow-up durations and possibly more adaptation time might help reduce the doffing time of advanced MLRGO.
The commitment of the Advanced MLRGO to biomechanical and orthopedic principles ensures its adoption for the provision of maximum possible support and stability of the lower limbs, which are important factors in patients with SCI. 11 In light of this, a possible reduction in the risk of falls and related injuries is of great importance considering the heightened vulnerability of this population. Stability during ambulation not only gives users better confidence but may also affect their tendency to participate in physical activities because of its impact on quality of life in general. 12 However, some limitations of this study have to be considered. A small sample size restricts generalization and calls for further exploration of inter-individual variations in response to advanced MLRGO. Individual data analyses may reveal subtle patterns and demographic influences that add more detail to the effect of the orthosis. Long-term adaptations to the use of the orthosis were not measured in this study, although the initial results are encouraging. Further research using longitudinal designs when considering long-term efficacy, user satisfaction, and physiological changes is needed to place the Advanced MLRGO into clinical practice. Additionally, there was limited investigation in the current study of psychological factors or personal preferences that might contribute to an individual’s acceptance and adoption of the advanced orthosis. The incorporation of subjective analyses may enrich future studies and further fine-tune orthosis designs. Finally, future work on updates to the Advanced MLRGO should consider present innovations in assistive technology, including but not limited to the incorporation of smart systems, such as motion sensors, adaptive gait control, and energy recovery mechanisms. Features of this type may significantly improve the functional level and degree of autonomy enabled, pushing the envelope on devices intended to assist the mobility of users far beyond simple aids to enable active adaptations to the user’s environment and biomechanical needs.
Conclusion
Stress analysis results and displacement amounts at three angles: 0, 18, and 20°.

Clinical characteristics of participants.

Spatial-temporal characteristics of walking, donning and doffing times, and energy consumption (first sub-study).

Abbreviations: PW: prime-walk, MLRGO: medial linkage reciprocal gait orthoses, ARMLGO: advanced medial linkage reciprocal gait orthosis.
Spatial-temporal characteristics and doffing times (second sub-study).
Abbreviations: PW: prime-walk, MLRGO: medial linkage reciprocal gait orthoses, ARMLGO: advanced medial linkage reciprocal gait orthosis.
Examining the impact of using orthoses on parameters.

Abbreviations: PW: prime-walk, MLRGO: medial linkage reciprocal gait orthoses, ARMLGO: advanced medial linkage reciprocal gait orthosis.
Asterisks indicate levels of significance: *p < 0.05.
Footnotes
Acknowledgements
We thank Mr Cadkhodaei for his advice and comments on the fabrication of this orthosis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.