
Abstract
Introduction
The purpose of this study was to compare the impact of three types of orthoses (knee orthosis, ankle foot orthosis (AFO), and foot orthosis) on knee alignment, pain, function, and quality of life in individuals with medial knee osteoarthritis (MKOA).
Method
Thirty patients took part in this study and were randomly assigned to three groups (n = 10 in each group) based on the type of intervention. Knee function was assessed using the knee injury and osteoarthritis outcome score (KOOS) questionnaire, and knee alignment was evaluated by measuring angles using the images of bony prominence (AMI) method.
Results
After using knee orthosis and AFO, all subscales of KOOS showed significant improvement (p < .05). However, there was no significant difference in the results after using foot orthosis (p > .05).
Conclusion
The findings indicate that knee orthosis or AFO for 6 weeks can improve clinical outcomes for individuals with MKOA. This suggests that clinicians can consider using knee orthosis and AFO among the available treatment options to improve clinical outcomes.
Introduction
Knee osteoarthritis (KOA) is a chronic and debilitating joint disease that is one of the most prevalent inflammatory joint conditions. It leads to pain, loss of function, reduced quality of life, and physical disability, especially in middle-aged people.1–4 KOA significantly impacts daily activities by causing deformities and pain. 4 Disease-related changes, such as joint space reduction and degeneration, are often observed in the medial compartment of the knee, accompanied by genu varum. 5 The medial compartment is affected 5 to 10 times more than the lateral compartment due to the more significant mechanical pressure applied during walking. 6 Furthermore, narrowing the medial joint space contributes to the progression of varus deformity, exacerbating joint space reduction. Thus, knee alignment emerges as an independent risk factor for the progression of the KOA. 7 For these reasons, assessing lower limb alignment is crucial for understanding and predicting the progression of KOA. 8
A conservative treatment for individuals suffering from medial knee osteoarthritis (MKOA) is the use of unloader knee orthosis and lateral wedge insole.9,10 Properly fitted unloading knee orthosis can significantly alleviate patient pain.11–13 According to the study by Ornetti, these orthoses have 76% effectiveness in reducing pain and enhancing stability. 14 This effectiveness is attributed to their ability to apply direct or indirect forces, which is essential for managing pain and instability, particularly in cases of genu varum. 15 However, despite the widespread prescription of knee orthoses, the debate surrounding their therapeutic efficacy persists. While many studies highlight the success of knee orthoses in alleviating clinical symptoms of individuals with MKOA,13,16,17 there is limited evidence supporting the long-term effectiveness of these devices.
Foot orthoses offer a simple and potentially convenient means of indirectly reducing knee adduction moment. 18 Lateral wedge insoles may alter the mechanical axis of the lower limb, thereby reducing forces on the medial compartment of the knee joint. However, such insoles may increase step width, inadvertently directing ground reaction force inward. 19 Despite the positive effects of lateral wedge insoles in alleviating pressure on the affected knee compartment, research has not consistently demonstrated a significant reduction in pain compared to standard insoles.18,20,21 One study reported that the maximum load reduction on the medial compartment of the knee using a lateral wedge insole was only 5% to 6%, which may be insufficient to significantly alleviate knee pain. 22
The ankle foot orthosis (AFO) is a device that indirectly reduces the adductor moment force on the inner part of the knee by stabilizing the ankle and foot joints. This minimizes tibial torsion, which in turn reduces the adductor moment on the knee. 23 The AFO is designed to counteract the varus moment at the knee and create a valgus moment. 24 It features a rigid sole connected to a vertical axis, which generates a valgus force on the lower limb during the stance phase, shifting the ground reaction force laterally and reducing the lever arm on the knee.
Recent studies indicate that the AFO may achieve a more significant reduction in the knee adductor moment compared to lateral wedge insoles. However, research on AFO remains limited.21,24 A review of five systematic reviews reveals that many studies have evaluated the outcomes of knee orthoses, foot orthoses, and AFOs in individuals with MKOA.25–29 Most of them compared the effects of one type of orthosis against another. However, the comparative impact of AFO, foot, and knee orthoses on the clinical outcomes of individuals with MKOA remains unclear. A study assessed the immediate effects of AFO, knee orthosis, and shoes on the knee adduction moment in 52 individuals with MKOA, finding that AFO and foot orthosis were more effective in reducing the knee adduction moment than knee orthosis.
The long-term effects of these orthoses on clinical and biomechanical parameters have not been thoroughly evaluated yet. Therefore, there is a need for a study to investigate and compare the performance of foot and knee orthoses, as well as AFO, regarding pain, function, quality of life, and biomechanical alignment of the knee in individuals with MKOA. By examining the knee alignment, we can better understand how variations in alignment affect quality of life, function, and pain. We hypothesized that wearing a knee orthosis, due to its direct biomechanical impact on the knee, and an AFO, by enhancing ankle and foot stability, can serve as alternative treatments to improve clinical outcomes for individuals with MKOA.
Materials and method
Participants
This was an experimental clinical trial. Our university’s Ethics Review Board approved the study (IR.USWR.REC.1400.166). It was conducted from May 2021 to May 2023 and registered in the Iranian Registry of Clinical Trials in May 2022 (IRCT20221017056212N1). The population in this test comprised individuals diagnosed with MKOA by an orthopedic surgeon who met the study’s inclusion criteria.
The participants were selected from among people with 2nd and 3rd-degree knee joint osteoarthritis who had been referred to our city’s clinics and rehabilitation centers. They were referred to our study after a physician confirmed their osteoarthritis degree (Kellgren-Lawrence index 2 and 3) and completed the consent form. The participants were randomly selected according to the inclusion and exclusion criteria.
The criteria for inclusion in the study were: (1) being between 40 and 75 years old, (2) having grade 2 or 3 osteoarthritis in the medial compartment of the knee based on the Kellgren-Lawrence scale. The exclusion criteria were varicose veins, conditions affecting walking, neurological diseases, torn knee ligaments (meniscus tear), recent knee injuries, other diseases, rheumatoid arthritis in the lower limbs, inability to wear shoes for less than 8 hours a day, leg ulcers, neuropathy, joint infection, diabetes, and use of walking aids.
Interventions
Foot orthosis
Prefabricated insoles (Savad Teb Darman Tehran Iran) were given to the patients based on their foot size. According to the studies, the insole covers the entire length of the sole and has arch support and a 6 mm lateral wedge. In our study, a prefabricated insole with a 6-degree lateral wedge made of cork material similar to Thermocork with a density of 60 durometers was placed in the patient’s comfortable walking shoes. 20
Three-point pressure knee orthosis
This orthosis was designed for patients with osteoarthritis of the medial compartment of the knee. It works by reducing the load on the medial compartment through the use of three pressure points created by stretching straps. This reduces the pressure on the medial side of the knee by decreasing the length of the lever arm and the reaction force of the ground and subsequently reduces the internal moment on the knee joint. The orthosis used in this study includes a medial bar, cross straps to apply external force, two thigh shells, a leg made of polypropylene, and a dynamic joint connecting them. The orthosis covers two-thirds of the femur at the top and the tibia at the bottom. To create a knee orthosis, we need to know the circumference at the level of the calf muscles, the circumference of the knee joint, and 17 cm above the knee. The knee orthosis is custom-made for each patient based on their size.
Ankle foot orthosis
The AFO was custom-made for each individual, and a lateral wedge was placed under the plantar surface to create a valgus moment. According to Schmalz, 21 a 7 mm wedge was placed under the foot to increase the adductor pressure. Each participant’s foot was cast, and the necessary modifications were applied. Then, after making the required corrections, the mold was ready for draping. The sheet used in this orthosis was made of 4 mm Polypropylene and was drawn on a mold of each person’s foot. A lateral aluminum bar was placed to create a valgus force of 4 degrees of adduction shows orthoses used in this study. 23 All participants used sports shoes made by DC Company in two sizes, 38 and 39 EU.
Data collection
Function and pain
The function of the patients was assessed using the Knee Injury and Osteoarthritis Outcome Score (KOOS) questionnaire at two different times: before using the orthosis and 6 weeks after using the orthosis. The KOOS questionnaire is a patient-centered 42-item survey that covers five main areas: pain (9 items), other disease-related symptoms (7 items), daily life activities (17 items), sports and recreation activities (5 items), and quality of life related to knee problems (4 questions). The questionnaire uses a 5-point Likert scale for answers. The scoring for each part is calculated according to specific formulas and the provided answers. The scores range from 0 to 100, where 0 indicates the worst situation, and 100 indicates the best situation. 30
Knee alignment
The knee alignment of the patients was examined clinically in the two stages before and 6 weeks after using the orthosis. Angle measurement using images of bony prominence (AMI) method was used to check knee alignment clinically.
8
The AMI technique is a method of assessing the alignment of the lower limbs, whose validity and reliability were examined and evaluated in 2018.
8
This method was introduced by Ohnishi et al. to measure the angle between the femur and tibia in the frontal plane by placing markers on bony ridges without the need for radiography. The AMI method has three steps: (1) using markers in lower limb landmarks (Figure 1), (2) taking a photo of the lower limb, and (3) measuring the alignment of the knee joint on the image of the lower limb using processing software.
8
Marking in AMI method. 1. Greater trochanter, 2. Lateral femur condyle, 3. Fibular head, 4. Lateral Malleolus, 5. Center of Patella.
Randomization
An orthotist blinded to the study treatment and procedures’ details did the randomization. It was done simply by adding a specific identification number for each participant. The statistical package for social sciences (SPSS) software version 26 randomly assigned participants to groups. The recruited participants were added in three equal groups of 10 participants each. Sequentially numbered, opaque, sealed assignment envelopes concealed the allocation. Each envelope contained a piece of paper with the group’s name for allocation. An independent orthotist performed the envelope opening process in front of the participants; each envelope was marked after being opened so as not to be used again.
Sample size calculation
Using G*power software, the sample size was calculated based on a priori analysis with a desired power of 99%, partial eta square of 0.5, and significance level of 0.05. A total of 26 cases were needed. To consider a potential dropout rate of 15%, we finally included 30 participants (10 participants in each group).
Procedure
Thirty people with osteoarthritis of the medial compartment of the knee were included in the study if they met the inclusion criteria and after a physician’s approval. Before the test, the participants were taught how to use the orthotic device according to the group to which they were randomly assigned. At first, the questionnaire was provided to patients without orthosis. The knee alignment of people was also assessed using (AMI) method. 8 One person completed all the steps to ensure consistency in the accuracy and quality of the tests. After that, the patients received the interventions. The participants were unaware that the orthoses were not given randomly. Each patient’s registered code contained all their information, and only the therapist had access to this information. After 6 weeks, the patients were asked to complete the provided questionnaire. The therapist examined the knee alignment with AMI method. To confirm that the patients used the orthosis, the first author sent them a text message every week (five times from Saturday to Thursday) asking about their usage frequency. The conditions were carried out in two stages: first without orthosis, then 6 weeks after using the orthosis. Each group was compared with itself in different stages and with three other groups.
Data analysis
We used SPSS version 26 to analyze the data. In this study, the Kruskal-Wallis test was used to check the existence of significant differences between participants at the beginning of the study. After the Wilcoxon test, there was a difference between the participants before and after the intervention. Ultimately, the test Quade nonparametric analysis of covariance (ANCOVA) was used to check and compare the changes in pairs and between the groups before and after the intervention. They were compared in pairs with the Mann-Whitney U test for multiple comparisons. All analyses were performed at a 95% confidence level. p value less than 0.05 was considered significant.
Results
Comparing knee alignment index changes between groups.

aWilcoxon Signed Ranks Test.
bQuade Nonparametric ANCOVA.
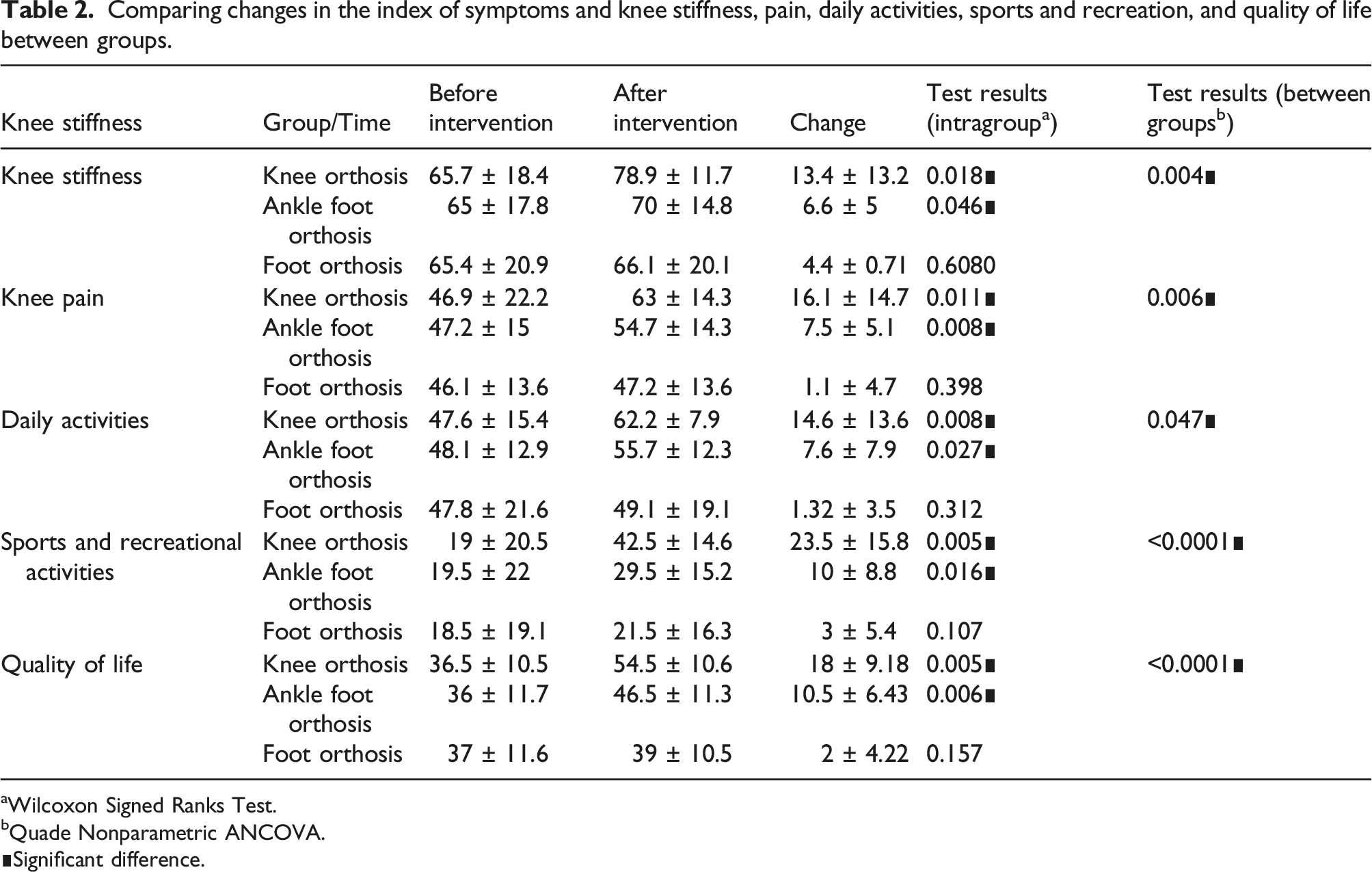
Comparing changes in the index of symptoms and knee stiffness, pain, daily activities, sports and recreation, and quality of life between groups.
aWilcoxon Signed Ranks Test.
bQuade Nonparametric ANCOVA.
Before the intervention, there were no significant differences in knee stiffness and symptom scores between the three groups (p = .998). However, after the intervention, the Wilcoxon test showed a significant improvement in knee stiffness and symptoms for both the knee orthosis and AFO groups. Furthermore, when comparing the changes in stiffness and symptoms between the groups, there was a significant difference (p = .004). Additionally, a significant difference was found between the knee orthosis and AFO groups (p = .01) as well as between the knee orthosis and foot orthosis groups (p = .001).
There was no significant difference in the knee pain score before the intervention between the three groups (p = .853). After the intervention, there was a significant after using knee orthosis and AFO. Finally, there was a significant difference in pain after the intervention between the three groups (p = .006). The comparison of the two primary groups also indicated a statistical difference between the knee orthosis and ankle and AFO group (p = .036) and the knee orthosis and FOs (p = .002).
There was no significant difference in the score of daily activities before the intervention between the three groups (p = .999). After the intervention, the Wilcoxon test indicated a significant after using knee orthosis and AFO. Finally, there was a significant difference in the daily activities after the intervention between the three groups (p = .047). A comparison of the two primary groups also showed a significant difference between the knee orthosis and AFO groups (p = .015).
No significant difference was found in knee exercise and recreation scores before the intervention between the three groups (p = .968). After the intervention, there was a significant difference after using knee orthosis and AFO. Ultimately, there was a significant difference in sports and recreational activities after the intervention between the three groups (p < .0001). The results of comparing the two primary groups showed a significant difference between knee orthosis and AFO (p = .009), knee and foot orthoses (p = .0001), and AFO and foot orthosis (p = .023).
Lastly, there was no significant difference in quality of life score before the intervention between the three groups (p = .957). After the intervention, the results of comparing the two primary groups indicated a significant difference between the knee orthosis and AFO group (p = .041), the knee and foot orthoses group (p = .0001), and AFO with foot orthoses (Table 2; p = .007).
Discussion
This study compared the effect of three types of orthoses on knee pain, function, quality of life, and knee joint alignment in people with MKOA. Our results show that all three orthoses improve function, reduce pain, and improve quality of life compared to not wearing an orthosis. Regarding a between-group comparison, the effect of knee orthosis and AFO on parameters of interest was significantly higher than that of foot orthosis condition.
Most people with MKOA typically experience pain while walking. Furthermore, the functional capabilities of people with KOA are severely limited.2,3 According to Baldwin et al., the pain experienced by normative individuals between 50–59 years old is 96.8 (via KOOS). In our study, the pain levels in the three groups were about 46 to 47 (via KOOS) before intervention. The study outcomes demonstrated a significant improvement in pain and function post-intervention, registering at 63 (via KOOS) for the knee orthosis group and 54 (via KOOS) for the AFO group. Therefore, the pain level was approximated to the normal level. 31
In a study by Peterson et al, both knee orthosis and AFO effectively diminished pain and enhanced quality of life in comparison to the control group without orthotic intervention. 32 In contrast to our study findings, which revealed a notable distinction between the AFO and knee orthosis groups, Peterson’s study did not report any significant variance between the AFO and knee orthosis groups. This may be due to the extended treatment duration in Peterson’s study for comparing orthotic effects, whereas our study assessed participants after 6 weeks. A study by Mahmoodi et al confirmed that the length of the treatment duration plays a pivotal role in the efficacy of orthotic interventions. 25
Our study showed a significant reduction in pain parameters during 6 weeks of using knee orthosis. These results align with the studies that investigated the effect of knee orthosis on people with MKOA, in which knee orthosis significantly reduced pain compared to the control group.12,33–36 As mentioned, the function of individuals after 6 weeks of treatment showed significant improvement. These results align with the study by Madara et al, which evaluated the use of knee orthoses on function in people with MKOA. Although their study reported improved performance after using the knee orthosis compared to the control group, this improvement was insignificant. 35
The recent results highlight that the use of knee orthosis and AFO significantly reduced pain and improved performance and quality of life compared to foot orthosis. Our findings align with two other studies comparing knee orthosis and insoles for people with MKOA. These studies demonstrated that longer treatment duration enhances the effectiveness of knee orthosis in improving performance, exceeding the benefits of insoles.37,38 However, our findings contradict those of Jones et al. (2013), who found no significant differences in the clinical outcomes of people with MKOA after 2 weeks of using knee and foot orthoses. The disparities might be due to the treatment duration in the two studies. As mentioned in a literature review by Mahmoudi et al., the length of the treatment period is a crucial factor in determining the effectiveness of orthoses in individuals with MKOA. 38 This supports previous observations by Schowarzet et al, who suggested that the use of AFO compared to a foot orthosis is more effective in improving knee pain. 39
Another finding is that foot orthosis does not significantly improve people’s quality of life. The obtained results are consistent with the studies of Jones et al and Lewinson et al.40–42 They also reported that insoles were ineffective in reducing knee pain. Although the amount of pain reduction in the foot orthosis group with a lateral wedge was reported in some studies, this amount of pain reduction was also reported in the control group with neutral insoles.43,44
These findings suggest knee orthosis is more effective in reducing pain than the other two. Similar to ours, Arazpour et al and Igbal et al found that the use of knee orthosis compared to foot orthosis significantly reduces pain.37,38
Since the increased knee alignment is directly related to increased pressure on the medial compartment of the knee, the knee alignment is considered an independent risk factor for osteoarthritis progression. 8 Therefore, we decided to examine the knee alignment before and after 6 weeks of using orthoses. The knee alignment in all three orthoses was improved, but insignificantly. Although the AMI test reported a small and non-significant angular change, it seems reasonable that the angular reduction leads to decreased loads transmitted through the knee joint in the medial plane. It has been reported that a significant decrease of the lever arm in the frontal plane may only be achieved in the combined state of using a knee orthosis and foot orthosis with a lateral wedge. 45 In a study, Sol et al. compared knee orthosis and AFO on knee alignment in the people with MKOA. The use of AFO in their study did not cause a significant change in the alignment of the knee like ours. Still, in contrast to our study, the knee orthosis group reported a substantial change in the knee alignment. 46 In the study by Sol et al., unlike ours, only the immediate findings were reported. Perhaps this difference in the knee orthosis can be explained in this way.
Limitations
While our findings offer valuable data for further research in this area, there are some limitations to consider. A limitation was the six-week treatment period. Six weeks might have been insufficient for testing the overall clinical effectiveness of the orthoses. However, our follow-up was similar to several studies investigating orthoses’ effects,47–50 generally between one to 6 weeks of familiarization.36,51–55 It should be noted that KOOS is a valid, reliable, and responsive self-administered instrument that can be used for short-term and long-term follow-up of several types of knee injury, including osteoarthritis. 56
Future studies should examine outcomes of individuals with MKOA over a longer duration and investigate any potential relationship between knee alignment and quality of life. Additionally, neither the therapist nor the participants were blinded to the treatment group. However, participants were unaware of the other groups. In studies evaluating orthoses, it is challenging to ensure blinding for individuals and therapists. 57
More work is needed to determine and evaluate function using performance-based tests; in this study, we assessed function using the subscale value of the KOOS. Future clinical studies may benefit from the methods used in this study, which combine baseline performance and functional testing. Another limitation is the absence of a control group. However, as Stetter mentioned, 58 building a real control or placebo group is known to be a problem in such investigations because any intervention can cause effects, for example, by altering proprioception. 59 Including orthopedic aids, subjective factors like pain perception can also be affected by placebo effects. 60 Examining and comparing three orthoses from a biomechanical point of view and their impact on biomechanical findings is still questionable. The investigation and comparison of the effect of three orthoses on clinical findings in the long term is evaluated in etiological studies. Finally, our findings should be evaluated clinically and biomechanically in larger MKOA populations.
Conclusion
The study found that using a knee orthosis or AFO for 6 weeks can improve the clinical outcomes of individuals with MKOA. When comparing the two, the study suggests that knee orthosis was more effective than AFO in improving the patient’s quality of life, knee pain, and function. The findings suggest that clinicians could use knee orthoses and AFOs as effective interventions for improving patients’ clinical outcomes. Additionally, future studies could assess the long-term effects of knee orthosis, AFO, and foot orthosis on clinical and biomechanical outcomes in individuals with MKOA.
Footnotes
Acknowledgements
The authors thank Dr. Taher Babayee and Muhammed Hussein Mousavinasab for helping to edit this text.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Iranian Research Center on Aging, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.