
Abstract
Background
The goal of rehabilitation after stroke is to restore safe and sufficient function to hemiplegic patients, and prescription of an ankle-foot orthosis (AFO) to improve speed and functional ambulation is a part of this program.
Objective
This crossover randomized interventional study aimed to evaluate the effect of an anterior ankle-foot orthosis (AAFO) and posterior leaf-spring ankle-foot orthosis (PLS AFO) on speed and functional ambulation in hemiplegic stroke patients.
Method
Clinical assessments were performed on 11 hemiplegic stroke patients by the AAFO, PLS AFO, and wearing shoes. Functional ambulation was measured by the 6-min walking test, Timed Up and Go Test, Time Up and Down Stair Test, and Functional Ambulation Category. Walking speed was measured by the 10-m test.
Results
Both PLS AFO and AAFO significantly improved the performance of TUDS and TUG tests in hemiplegic patients. However, by using PLS AFO, walking distance was significantly greater than walking with shoes. There was no significant effect on the walking speed improvement using PLS AFO or AAFO compared to wearing shoes.
Conclusions
The positive effects of the AAFO and PLS AFO on functional ambulation were significant. By using PLS AFO, hemiplegic patients could walk a longer distance than wearing shoes.
Introduction
Stroke is the second leading cause of mortality and the third most common cause of permanent disability in the world.1,2 The hemiplegic gait pattern, which is a combination of compensatory movements and the deviations of the lower extremity function, is seen with various intensities in patients with stroke. 3 Dorsiflexor weakness and plantarflexor spasticity may cause foot drop in the swing phase of gait and also lack of initial heel contact are characteristics of hemiparetic gait pattern.4-6 Commonly all of these problems can lead to reducing cadence, stride length, and walking speed in post-stroke patients. 7
Recently, correlation of speed with balance, mobility, and quality of life has been investigated in post-stroke patients.8-10 Increasing gait speed, in turn, leads to ambulation improvement of hemiplegic stroke patients, which demonstrates the effectiveness of their rehabilitation programs.8,10 We have to consider that gait speed assessment is not an adequate investigation of the level of functional ambulation in post-stroke patients. In the previous study, it was mentioned that there are no significant differences in gait speed among people who have different functional ambulation scores, and thus further ambulation assessments for determining the ability to do daily tasks and community ambulation like walking up and down stairs are needed. 11
Among a wide variety of passive ankle-foot orthoses (AFOs), the posterior leaf-spring ankle-foot orthosis (PLS AFO) is often used by patients with ankle dorsiflexion muscle weakness without significant mediolateral instability.12,13 PLS AFO improves walking performance 14 and reduces limb asymmetry during a gait 15 through decreasing ankle plantar flexion to neutral position at the initial heel contact and during swing phase, and also by increasing ankle dorsiflexion during the stance phase of gait.14,15 However, the use of an anterior ankle-foot orthosis (AAFO) has had a positive effect on improving gait pattern and walking mobility of post-stroke hemiplegic patients as well, according to previous studies.16-18 The most effective AFO can be selected based on gait speed and functional ambulation category characteristics in the gait of hemiplegic post-stroke patients. 19 The ankle trimline plays a crucial role in determining the stiffness of the AFO which, in turn, provides the different resistance to the dorsi-plantar flexion moments of the ankle. 20 Because of the similarities between the positive effects of the AAFO and PLS AFO on improving walking capacity in hemiplegic patients, 21 the effect of these two types of orthoses on walking performance of post-stroke patients can be compared. Although some studies have evaluated the effects of the AAFO and PLS AFO on static balance and kinematic features of rearfoot motions in hemiplegic post-stroke patients,14,22 there is no clinical evaluation study of the effect of the AAFO and PLS AFO on functional ambulation and walking speed in hemiplegic post-stroke patients. Therefore, the purpose of this study was to conduct this evaluation.
Method
Participants
Participants clinical characteristics.

BMI: body math index, F: female, FAC: Functional Ambulation Category, L: left, M male, MAS: Modified Ashworth Scale, R: right, SD: Standard deviation.
Ankle-foot Orthoses design
Both AAFO and PLS AFO were fabricated custom-molded for each patient by a certified orthotist (Figure 1). The below-knee casting of the AAFO and PLS AFO was performed while the participant was sitting on a chair with 90° knee flexion and 5–10° ankle dorsiflexion for AAFO or neutral ankle position for PLS AFO casting. Both AAFO and PLS AFO were fabricated by using polypropylene 4 mm thickness. The upper portion trimline of the AAFO was extended from 2/5 cm behind the fibula head to the dorsal surface of the toes without covering malleoli. The foot portion was covered by transverse bars running across of plantar surface of the midfoot to the end of the toes. Likewise, the PLS AFO was trimmed from 2/5 cm behind the fibula head and extended posteriorly to the malleoli. The full-length of the plantar surface of the foot portion was covered to the end of distal phalanges. Three straps were added to the upper part of the tibia, ankle, and metatarsal portions of the PLS AFO. (a) Posterior leaf-spring ankle-foot orthosis (PLS AFO), (b) anterior ankle-foot orthosis (AAFO).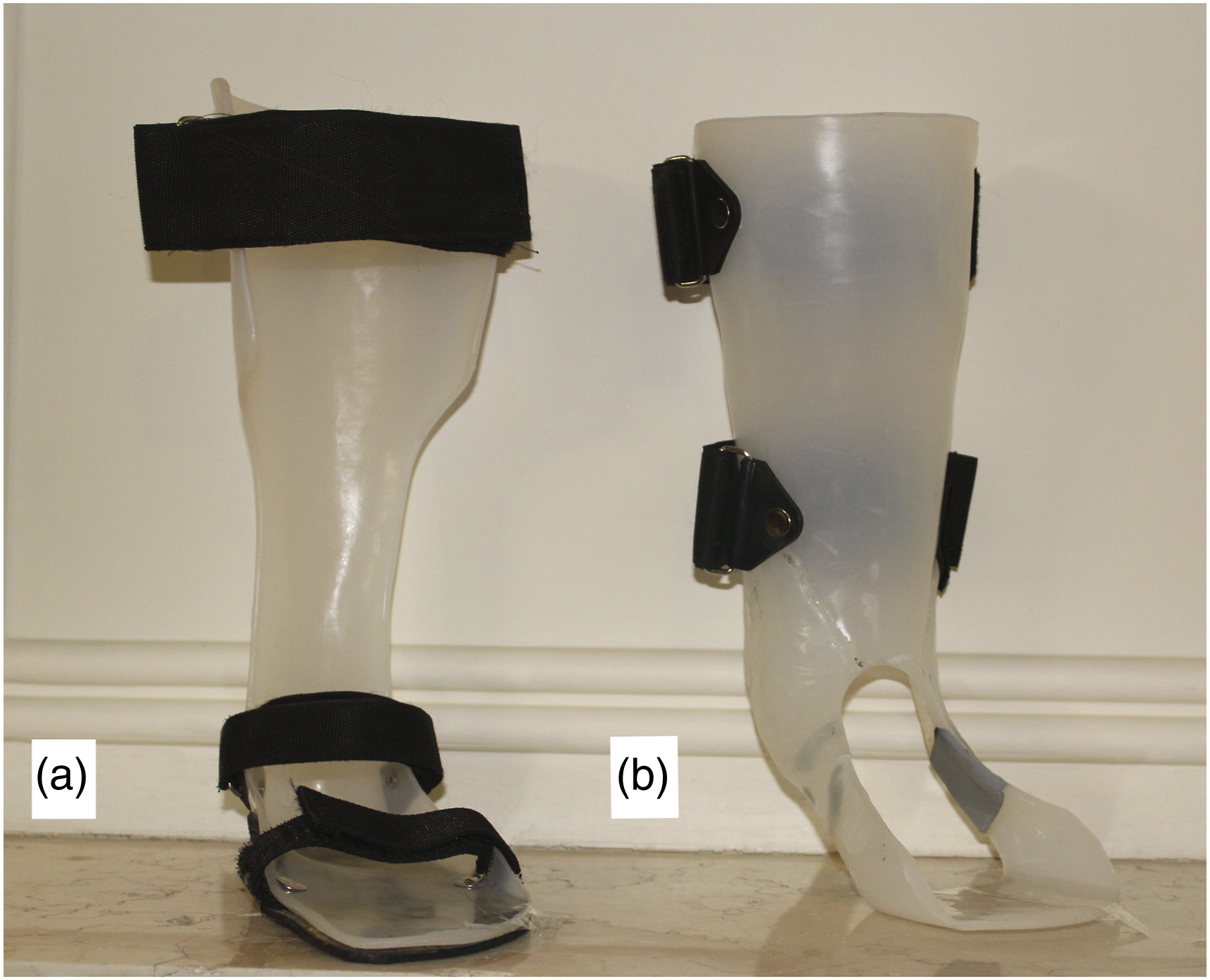
Procedures
All demographic data were collected from post-stroke individuals during the first meeting. Then, subjects participated in three other separate data collection sessions and completed functional evaluation assessments under three conditions: using AAFO, PLS AFO, and wearing regular shoes. During the first session, participants were asked to complete assessments by wearing regular shoes. Subsequently, the second and the third assessment sessions were completed by using AAFO or PLS AFO. The order of distribution of the two types of AFOs has been randomly assigned. Then, the first AFO was used by the participants during daily walking for two weeks before quantitative assessments of speed and functional ambulation. The participants received the next AFO with one week delay because of considering wash-out time. After using the second AFO during daily walking for two weeks before the third assessment session, during the third session, evaluations were completed by the participants using the second AFO.
Clinical assessments
All assessments were performed in the same environment. The participants performed the 6-min walking test (6-MWT), Timed Up and Go Test (TUG), Time up and Down Stair Test (TUDS) for functional ambulation assessments, and the 10-m walking test (10-mWT) for speed assessment. Each test was repeated three times, and thus the average was calculated for further analysis except the 6-MWT performed once to prevent excessive fatigue of the patients. Patients were allowed to use a cane during the performance, also they were given 1–3 min of rest time between performing each test.
Outcome measures
Walking speed was measured using 10-mWT, which is a basic method of measuring the walking ability of hemiplegic stroke patients. Participants were asked to start walking at their fastest speed 2-m ahead of the start line and stop walking at the 2-m after the 10-m line. 24 TUDS test used to assess free-living physical activity in community-dwelling is measured by the time required for ascending and descending from 12 standard stairs. All participants were allowed to use handrails. 17 The TUG test used to assess functional mobility and balance is measured by the time that is required for participants to stand up from a standard armchair, walk 3 m, return to the chair, and sit down. 17 The 6-MWT used to assess functional community ambulation of participants is the maximum distance traveled at a comfortable walking speed during 6-min walking along a hallway. 25 Functional Ambulation Category (FAC) which is a quick visual measurement to assess independent walking ability was filled. 26
Data analysis
All data were analyzed using descriptive statistics in SPSS version 24.0. The level of significance for all analyses was set at p values < .05. Normality was checked by a Shapiro–Wilk test in all calculations. Gait speed, TUG test, and 6-MWT were calculated using the Paired t-test while the TUDS test and the FAC were calculated using Wilcoxon signed-rank test.
Results
Comparison of application in terms of speed and functional ambulation.

*Significantly different from the mean of the shoe, AAFO, PLS AFO conditions (p < .05).
AAFO: anterior ankle-foot orthosis, FAC: Functional Ambulation Category, 10-Mwt: 10-meters walking test, 6-MWT: 6-minutes walking test, PLS: posterior ankle-foot orthosis, SD: Standard deviation, TUG: Time Up and Go, TUDS: Time Up and Down Stair.
Discussion
This study indicates that both AAFO and PLS AFO improved functional ambulation and mobility by improving the performance of the 6-MWT, TUG test, and 6-MWT compared to shoes in hemiplegic post-stroke patients. However, there is no significant effect on improving walking speed using AFOs compared to wearing shoes.
Walking speed is an independent variable determining the walking ability and community ambulation capacity of the hemiplegic post-stroke patients. Post-stroke hemiplegic patients can walk at a gait speed of approximately 0.4 m/s while the typical walking speed is approximately 1.33 m/s. 11 Although the gait speed of the patients would increase during the post-stroke period, 27 they may encounter limitations in walking and ambulation. 11 The result of this study indicates that there is no significant effect on speed improvement by using the AAFO or the PLS AFO in comparison with wearing shoes. A possible explanation for this result could be that although different types of AFOs are likely effective in improving ankle kinematics during gait,14,15,21 it is mentioned that PLS AFO or AAFO has no significant effect on improving peak knee flexion at initial contact and knee extension during stance phase.21,28 Moreover, a lack of significant effect on the improvement of the hip joint kinematics by AAFO or PLS AFO is reported. 21 Lairamore et al. 29 indicated the ineffectiveness of PLS AFO on improving gait speed due to lack of significant effects on improving the ankle dorsiflexion angle during stance and mid-swing phase of the gait cycle. Lewallen et al. concluded lack of a significant effect of using PLS AFO or articulated AFO on the velocity, which was found in comparison with wearing a shoe only. 16 Thus, the result of this study is consistent with previous results. By contrast, it has been mentioned that both posterior ankle-foot orthosis (PAFO) and AAFO increased gait speed by improving ankle kinematics in the sagittal plane compared to barefoot walking. 21 However, this discrepancy could be due to the differences between the baseline interventions of the studies. Moreover, the small sample size of our study could have affected the result of speed evaluation.
All functional tests including the TUDS, TUG, and 6-MWT tests are the main clinical assessments, which predict free-living physical activity and community ambulation of hemiplegic post-stroke patients. Stair negotiation is a routine locomotor task that requires more physical and motor tasks than level walking. 30 In this study, the results of the TUDS and TUG tests indicated that the completion time of the TUDS and TUG tests significantly decreased by 14%, 19%, and 11%, 11%, respectively, by using AAFO and PLS AFO compared to wearing shoes. Ankle dorsiflexor strength, the percentage of single-limb support phase on the paretic side, 31 and also ankle dorsiflexion angle during stance and swing phase of the gait cycle are variables that are the most associated with TUDS test performance.32,33 It has been investigated that both AAFO and PAFO significantly improved static and dynamic balance by decreasing center of pressure sway (COP) and increasing weight-bearing capability of the affected side in comparison with a shoe or the barefoot condition. 22 Thus, both AAFO and PLS AFO could be effective in improving dynamic tasks that require mediolateral weight shifting on the paretic limb. Chen et al. 17 reported that by using AAFO the performance of the TUDS and TUG tests significantly improved. Moreover, AFOs significantly decreased the test completion time of the TUG test which showed mobility improvement in hemiplegic patients compared to the patients without AFO. 23 However, Zollo et al. announced that PLS AFO was not significantly effective in improving the TUG test performance of patients compared to no AFO condition. However, it has been mentioned that presumably, the short-term use of the orthoses led to differences in the result of the study compared to other studies. 15 In addition to this, the majority of participants of the study had a greater passive ankle range of motion in comparison with the participants of our study, which could result in the contradiction between the studies.
Walking endurance is measured by the 6-MWT which is the strongest predictor of community walking activity in individuals. A 6-MWT distance ≥ 205 m discriminated between home and community ambulatories, whereas a 6-MWT distance ≥ 288 m discriminated between limited and unlimited community ambulatories.34,35 The result obtained from the 6-MWT indicated that the PLS AFO significantly increased the ability of walking distance during 6-MWT in patients compared to shoes, but the differences between the positive effects of the AAFO and PLS AFO on improving the 6-MWT performance of patients were not significant. Since excessive foot inversion which caused mediolateral instability or poorer postural control36,37 is seen in the hemiplegic gait pattern, 38 the PLS AFO by its posterior reinforcement and full-length foot portion could be more effective in increasing mediolateral weight shifting effectively through keeping the COP with the foot axis 11 and enhancing rear-foot dorsiflexion during a whole gait cycle, 17 which may result in enhancing the ability to walk long distance and community activity. Our result was similar to the previous studies that indicated the effect of posterior AFO on walking distance improvement during 6-MWT.39,40 In this study, the positive effect of the AAFO on improving 6-MWT performance was not significant compared with shoes. However, it is reported that the improvement of walking distance in post-stroke patients was significantly greater by AAFO compared to no orthotics intervention. 18 This contrast could be explained by the differences between baseline interventions in comparison with other studies.
There is a strong relationship between speed, cadence, step, and stride length, 41 and also a risk of falling to the functional ambulation in hemiplegic post-stroke patients. 42 Although it is reported that using hinged AFO or PAFO significantly improved the functional mobility in the hemiplegic patients,43,44 even post-stroke patients with FAC score of 5 could not achieve walking ability similar to that of older adults. 45 According to the result of the study, using the PLS AFO improved FAC score just in one participant. Therefore, the effect of the AAFO or PLS AFO on the FAC score improvement was not significantly greater than shoes in hemiplegic patients. Similar to the finding, De Wit et al. reported that AFO had no significant effect on improving FAC in stroke patients 24 while Tyson et al. reported a significant effect of using AFOs on the improvement of FAC who were at the duration of the acute phase of post-stroke. 44
Study limitations
In this study, participants could have used a cane, which might have affected the homogeneity of participants.
By considering that all assessments were performed in three separate sessions, changing the psychological and physical conditions of patients could have influenced the results obtained.
Conclusion
In conclusion, using AAFO or PLS AFO contributed to improving functional ambulation and mobility in post-stroke patients with hemiplegia. Using PLS AFO provided a greater capability to increase walking distance in hemiplegic stroke patients compared to wearing shoes. The AAFO and PLS AFO did not significantly affect gait speed improvement in hemiplegic patients with stroke.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.