
Abstract
Assistive technologies for cognition (ATC) can help alleviate some of the impacts of executive dysfunction and support independence. This article presents a scoping review to highlight the research gaps in this area. Search of scientific and gray literature was conducted in clinical and computer science databases, resulting in a selection of 27 papers. Traumatic brain injury and dementia were the disorders for which the most supports were available. Planning and carrying out tasks were the most supported executive function operations. Food preparation was the daily activity for which the most supports were developed. Diverse non-context-aware technologies were used to deliver primarily audio and visual prompts and cues. The performance of most of the technologies was tested among the target population to evaluate acceptability and effectiveness. This review showed that: (1) The goal formulation executive function operation needs to be the focus of more research; (2) the clinical context needs to be described in more be detail; (3) ATC development could benefit from the use of a wider range of user-centered methods, such as observational or ideation methods; (4) more evaluation of user outcomes is needed, such as impact on independence; and (5) a greater diversity of activities of daily living should be supported. Recommendations are presented.
Keywords
Introduction
To live independently at home, an individual must be able to engage both in basic activities of daily living (BADL) and instrumental activities of daily living (IADL). 1 BADL refers to basic personal care tasks related to hygiene and health. Lawton and Brody 1 include activities such as feeding oneself and using the toilet in this category. IADL refers to more complex activities that enable the individual to live independently at home and in the community, for instance using the telephone and preparing food. 1
Studies show that higher-level cognitive functions, such as executive functions (EF), are mobilized2–5 to carry-out IADL, since these activities are complex.4,6 EF are defined “as the capacity to plan and carry out complex goal-directed behavior that is appropriate to the context in which the activity is carried out” (Bottari 6 p. 10). Goal-directed behavior refers to a person’s actions motivated towards attaining a specific goal. 7 In the context of goal-directed daily living activities, it is suggested that EF contribute to four cognitive operations4–6: (1) formulate a goal: linked to motivation, formulating a goal is the ability to have an intention, which can be affected by the environment 3 ; (2) plan: the ability to behave objectively in relation to one’s environment, to think about alternatives, to weigh and make choices, and ultimately to structure this information with a view to actually carrying out the task 3 ; (3) carry out the task: the ability to translate the previous planning into productive activities 3 ; and (4) verify attainment of the initial goal: the ability of the person to monitor their actions and self-correct, 3 and to verify that the task initially planned was carried out. 8
EF are often affected in people with brain damage or neurological conditions, 3 for example, due to hyperactivity disorder (ADHD), traumatic brain injuries (TBI), or neurodegenerative diseases. 9 These conditions are types of mental disorders. 9 A mental disorder is defined as “a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning” (DSM-5 9 p. 20). Executive dysfunctions are associated with difficulties carrying out new activities; initiating new sequences while interrupting ongoing sequences; detecting and correcting errors, modifying a plan, recognizing more favorable goal opportunities, etc.9,10 There is also growing evidence concerning the importance of EF in people’s ability to live independently.6,11,12
Assistive technologies for cognition (ATC) have great potential to support populations with executive dysfunctions. 13 ATC are defined as: “technologies which enable, enhance or extend cognitive function as needed” (O’Neill and Gillespie 14 p. 1). An example of ATC is COACH, which aims to support people with dementia in washing their hands. 15 By means of a camera, COACH monitors the person’s progress. Prompts are provided if the system detects that the person is having difficulty progressing in the task. PEAT is another example of an ATC, an Android application for planning and execution designed to support people with a brain injury. 16 It is able to automatically generate plans and update them in case of unexpected situations. ATC can also support complex everyday activities, for example, the ATC COOK focuses on food preparation. 17 This smart stove is equipped with a tablet that guides the person during recipe completion. In case of a critical situation (e.g., a pan left unattended on a burner), alarms can be triggered, or the stove can be switched off.
There appear to be no specific guidelines to support field research and development of ATC for executive dysfunctions taking into account the specific difficulties related to this cognitive function. Few literature reviews have specifically focused on these cognitive dysfunctions. Existing reviews focus on specific disorders or address EF as part of a larger topic. The scoping review by Desideri et al. 18 aims to identify the categories of ATC which compensate for executive dysfunctions in individuals with autism spectrum disorder and to study the effectiveness of these ATC for this population. Sampled populations of all ages with autism spectrum disorder were considered for this review. 15 studies were selected and these ATC were classified into two categories: context-aware technology and mobile technology. Desidiri et al. 18 suggest that ATC designed to support autism may support specific executive dysfunction difficulties, but that more research is required, such as studying a wider range of EF-related skills. The systematic review by Gillespie et al. 19 aims to covers ATC in terms of the cognitive functions, and EF are one of the cognitive functions considered. Their objectives were to study how the field has changed over time, to explain the relation between ATC and cognitive functions/activity domain/clinical population, and to determine if there was evidence for ATC to support cognitive functions. All populations were considered, including acquired brain injuries (45.1%) and dementia and older people (14.3%). ATC were classified according to ISO categories 24 : alerting, reminding, micro-prompting, storing, and displaying and distracting. However, the main contributions of this review were unrelated to the evidence regarding the use of ATC for EF. The study introduces a first ATC classification related to cognitive functions. It also encourages researchers to use technologies other than prompting and reminding. The state-of-the-art review by Lopresti et al. 20 focuses on interventions that provide compensatory methods and strategies for task performance. One section focuses on ATC for rehabilitation, specifically with regard to executive dysfunction. The authors did not detail their methodology for article selection, nor their target population. However, they take into account both mainstream (technologies for the general population) and rehabilitation technologies. For mainstream technologies they discuss the advantages and disadvantages of using mainstream technologies for people with cognitive impairment. They focus mainly on computer-based devices. While drawing no conclusions from this discussion, the authors do highlight the importance of context-awareness to reduce cognitive load, especially for people who lack initiation and planning skills. Finally, Jamieson and Evans 21 provide a specific review on ATC for executive dysfunction. They focus on technologies that prompt or remind people to carry out a task or which guide them or provide micro-prompt steps for a task. The sample population targeted people with executive dysfunction. The review highlights that design, accessibility, availability, and adaptability of technology for personal use are issues to consider. It suggests that strong clinical trials must be conducted to obtain more evidence. However, the review does not describe their methodology, making it difficult to determine the criteria for selecting articles.
To better determine the research gaps in this area as well as provide recommendations for future research and technology development, we conducted a scoping review to document how ATC for people with executive dysfunctions have been developed and evaluated in the context of goal-directed behaviors.
Objectives
This review addresses the following PICO 22 research question: for people with executive dysfunctions (population), how are ATC developed and evaluated (intervention) in order to improve goal-directed behaviors (outcome)? The “comparison” component of the PICO question is not taken into account here as we do not aim to compare the accuracy of the approaches. 22
To answer this question, sub-research questions (RQ) were defined and related to each PICO component:
Participants
Which populations were most targeted by ATC focusing on executive dysfunctions? (RQ1)
Intervention
What were the characteristics of the ATC? (RQ2) How were these ATC developed? (RQ3) Was the ATC evaluated with participants? (RQ4)
Outcome
What are the goal-directed behaviors targeted by these ATC? (RQ5)
Method
A scoping review was performed following the five stages recommended by Levac et al. 23
The first stage aimed to define the research question. In this study, in line with the previously defined objectives, we aimed to answer the PICO research question and sub-questions detailed in the previous Objectives section.
Concepts and keywords used in the search strategy.

The third stage was article selection. All the following inclusion criteria had to be met: (1) be a book chapter, journal article, or paper published in the proceedings of a conference. Books, PhD theses, opinions, editorials, preprints and reviews were excluded; (2) describe the design of an ATC. It could be a new technology, or an existing technology developed in another context but applied to a population relevant to this review population; and (3) focus on addressing executive dysfunctions. Study selection was conducted independently by GS and HKN. Results were then compared and conflicting interpretation were discussed and resolved between the two authors, without the need to involve a third-party.
In the fourth stage, the variables that would provide relevant data to answer the research questions were determined, then extracted and charted.
ATC target population (RQ1), characteristics of the ATC (RQ2) and ATC development (RQ3).

Legend: ADHD: attention deficit and hyperactivity disorder; ABI: acquired brain injury; AR: augmented reality; ATC: assistive technology for cognition; EF: executive function; HMD: Head-Mounted Display; IR: infra red; MCI: Mild Cognitive Impairment; OT: occupational therapist; RCT: randomized control trial; TBI: traumatic brain injury.
The characteristics of the ATC (RQ2) were addressed by two sub-questions: purpose of the ATC and targeted EF operations. The purpose of the ATC (RQ2.1) was classified following the eight categories of ATC proposed by Cook and Polgar 13 (Table 15-9; definitions extracted from Cook and Polgar 13 p. 389): (1) memory aids (augment or replace the primary memory functions); (2) time management (planning, prioritizing, and executing daily and time-dependent tasks); (3) prompting/cueing (guidance for procedural or navigational sequencing tasks); (4) stimuli control (address attention or perception problems by limiting or manipulating the information presented to the user); (5) language control (assist with writing); (6) alternative input (assist with reading); (7) alternative output (assist with reading and writing); and (8) tracking and identification (safety for users who might not have the cognitive skills required to solve problematic situations). An ATC may belong to one or more of the categories defined by Cook and Polgar. 13 When available, the name of the ATC was reported along with its main objective. The target executive function operations (RQ2.2) were classified according to the definition of Bottari et al. 8 The EF components reported by the studies were first extracted. They were then associated to the classification of executive function operations developed by Bottari et al. 8 (i.e. formulate a goal, planning, carry out the task and verify attainment of the initial goal) and designed to structure the variety of terms used to define EF components, in order to have a common basis from which to examine the executive dysfunctions most supported by ATC. EF components were extracted and then associated with the EF operations involved. Half of the articles were done by AY and the other half by AY and GS.
To determine how the ATC were developed (RQ3), data were extracted following four variables: type of technologies used; design methods used; type of assistance delivered to the user; and context-awareness. The type of technologies used to develop the ATC (RQ3.1) were classified according to the assistive technology categories proposed by the ISO 9999:2022 standard. 24 The definitions of the categories used in this review are summarized in Table 5 in the SM. Data on the methods used to design the ATC (RQ3.2) were extracted from both (1) the section describing the design of the ATC, and (2) the methodology of each selected source. To structure the variety of terms used to design ATC, the terminology proposed by Lallemand and Gronier 25 in the context of user experience was followed. These authors suggest organizing methods according to three stages of product development 25 : (1) Exploration; (2) Ideation; and (3) Generation. The methods are detailed in Table 6 in the SM. This terminology was adopted, as suggested in the literature, to consider user-centered design (UCD) methods when designing ATC.20,26–28 UCD is defined as (Norman 29 p. 188) “a philosophy based on the needs and interests of the user, with an emphasis on making products usable and understandable”. The type of assistance delivered by the ATC (RQ3.3) summarized whether they were audio and/or visual and/or haptic. Details were also provided on how they were delivered in context (e.g., prompts, questions, alarms). The context-awareness variable (RQ3.4) described if the ATC was able to provide assistance/support to the person. To maximize the ATC adoption, authors have suggested that context-awareness capabilities are critical.20,26,27 Indeed, people living with EF impairments may require assistance at any time hence the importance for ATC to understand the context in order to provide assistance at the right time and place. The definition retained for context-awareness is that proposed by Dey 30 : “a system is context-aware if it uses context to provide relevant information and/or services to the user, where relevancy depends on the user’s task” (Dey 30 p. 2).
The following variables were extracted for studies involving human participants (RQ4): the n variable, which corresponded to the number of participants (RQ4.1) involved in the study; the description of the population (RQ4.2) variable, which included, when available, participants’ age, occupation, gender and mental disorder; the evaluation methods (RQ4.3), which described the methodology used in the study, based on the classification proposed by Lallemand and Gronier.
25
See Table 7 in the SM for the list of the most common evaluation methods. The outcomes (RQ4.4) summarized the measures evaluated. Outcomes were extracted from each article (verbatims), and a deductive thematic content analysis
31
was conducted on these verbatims to analyze the results, based on the following coding steps: (1) first cycle coding: codes assigned to each verbatim using a descriptive coding method; and (2) second cycle coding: based on the resulting first cycle codes, pattern coding is performed following the taxonomy proposed by Jutai et al.
32
(Table 1 p. 297, focuses on assistive technologies outcomes) and Nielsen
33
(Figure 1 p.25, focuses on acceptability of technology). We added the “user experience” code from the ISO 9241-210:2019
34
to classify first cycle codes that did not correspond to the taxonomies of Jutai et al.
32
and Nielsen.
33
Terms are defined in Table 8 in the SM. Flowchart of sources screened and included in the review.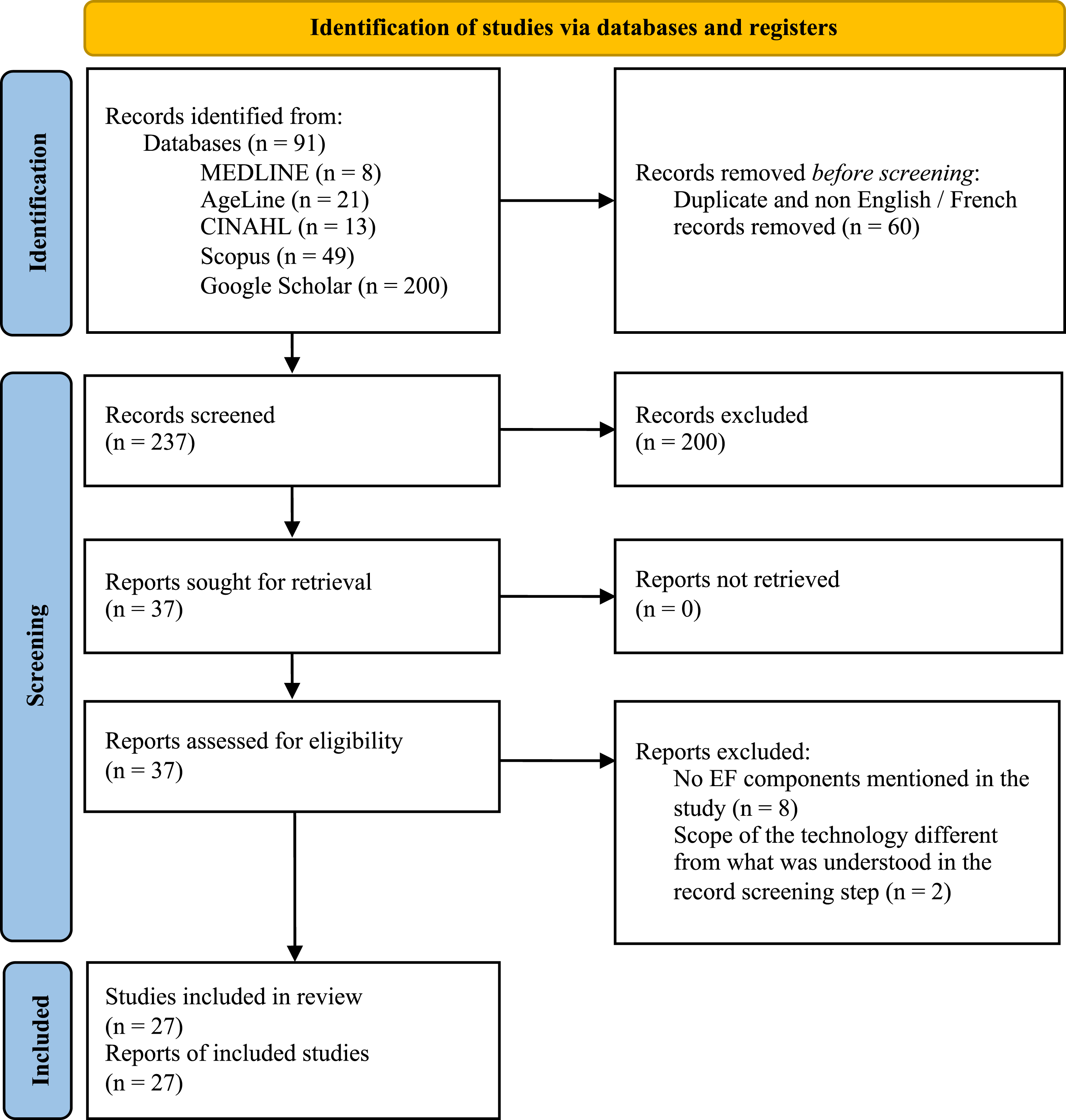
The goal-directed behavior targeted (RQ5) reported the activities supported by the ATC. The classification followed three categories: (1) IADL; (2) BADL; (3) theoretically, any activities. BADL and IADL are the categories defined by Lawton and Brody 1 (presented in the introduction). The third category is added as some ATC are designed to support different usage contexts. An ATC could support several IADL or BADL. An ATC could also support any kind of activity not related to IADL or BADL such as those related to work or school activities.
All data were extracted by GS, excepted for the variables related to EF that were extracted by AY. AY extracted data for two articles, to validate the consistency of the data extraction performed by GS. Verbatims for the deductive thematic content analysis were extracted by GS, and coding was performed by NB and GS.
The fifth stage involved collating, summarizing and reporting the results, in order to determine the characteristics of each ATC. Analyses were based on the number of repeated occurrences for a given variable, and, for specific points of discussion, on conclusions suggested by the articles.
Results
A flow chart of the selected articles is presented in Figure 1. At the second stage, after language filtering and duplicate removal, 237 articles remained for consideration. At the third stage, after screening by title, abstract and type of document, 37 sources met the inclusion criteria for a full-text review. For the fourth stage, a full-text review was conducted on the 37 previously selected articles. During this process 10 articles were excluded for the following reasons: (1) no EF components were explicitly mentioned in the article (n = 8); and (2) the scope of the technology differed from that suggested by the abstract (n = 2). No articles were rejected at the fifth stage. Therefore, a total of 27 sources were included in this review. Among these articles, 23 reported results on a single technology not described by any other selected article, while others were related to the same technological initiatives: TangiPlan35,36 (two articles) and GUIDE37,38 (two articles).
ATC evaluation details (RQ4) with participants and the target goal-directed behaviors (RQ5).

Legend: ADHD: attention deficit and hyperactivity disorder; ABI: acquired brain injury; AR: augmented reality; AT: assistive technology; EF: executive function; HMD: Head-Mounted Display; IR: infra red; NCD: neurocognitive disorder; NDD: neurodevelopmental disorders; OT: occupational therapist; RCT: randomized control trial; TBI: traumatic brain injury.
The population targeted by the ATC (Figure 2 – Table 9 in the SM for details about the references) Traumatic brain injury (TBI) and dementia were the most supported mental disorders by technology. Diagnosis severity was mentioned for seven ATC, six of which targeted people with a mild severity, and one with a major severity. For example, COOK
17
was developed for individuals with major TBI, and is intended to support food preparation, and people with major TBI can easily be distracted. The ATC encourages them to limit the use of distractors, while being context-aware to react in critical situations (e.g., the person leaves a pot unattended on the stove). cARe
39
is a mixed-reality ATC to support food preparation for people with Mild Cognitive Impairment (MCI). It displays instructions for performing the activity at the location where they are to be performed. They indicate that people may need additional motivation. To do this, if the person remains inactive for too long, the system sends an encouraging sentence.
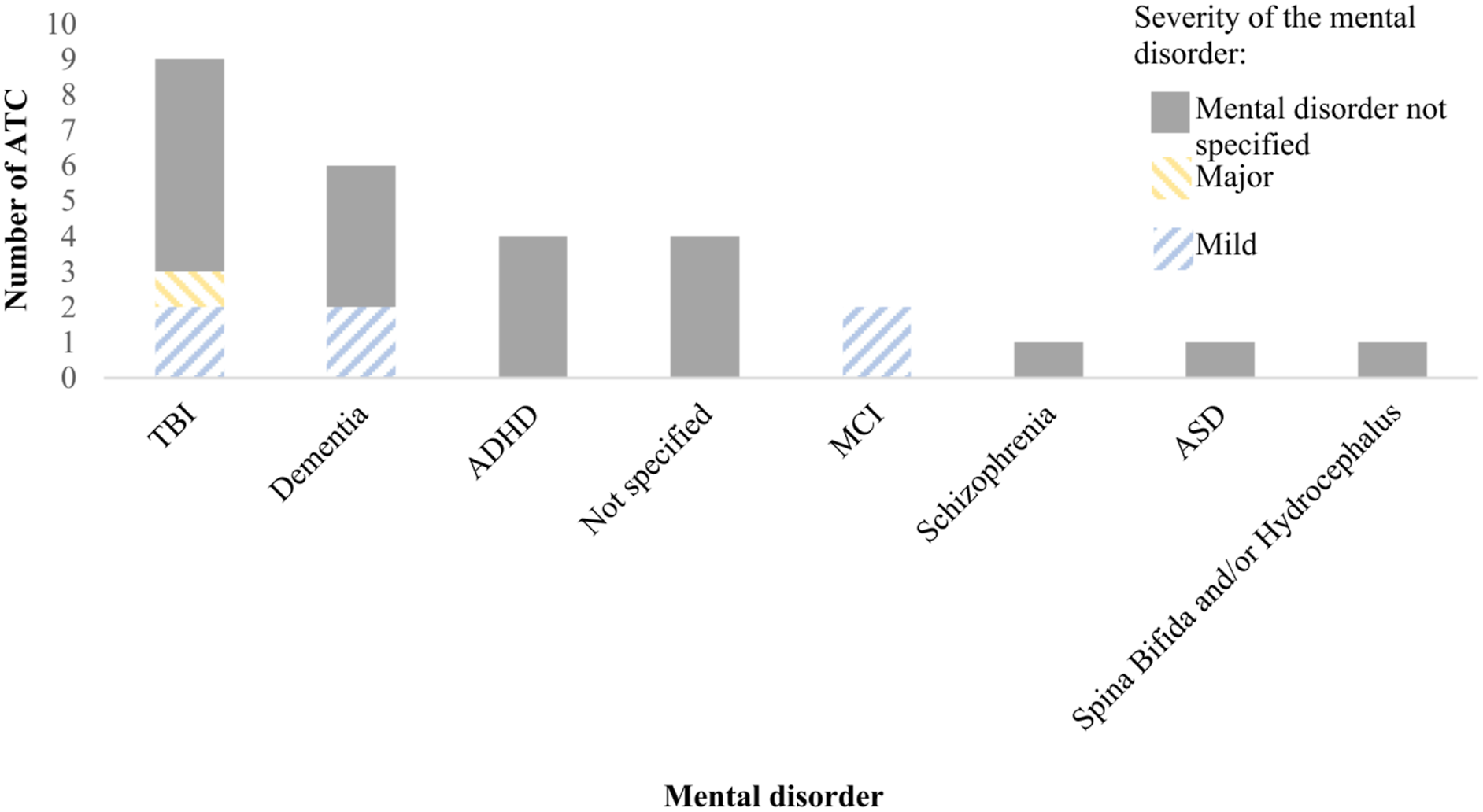
Population targeted by the ATC per mental disorder (RQ1). The colors represent the severity of the mental disorder: gray when not specified; blue for mild severity; orange for major severity.
Characteristics of the ATC
Purpose of the ATC (Figure 3 – Table 10 in the SM) Seven ATC belonged to one category; 13 belonged to two categories; six to three categories; one to four categories. Prompting and cueing, Time management, and Tracking and identification were the most commonly present. Half of the ATC in the Time management category were also in the Prompting and cueing category. For example, TaskTracker
40
is a smartphone application focusing on time management and assistance with task completion. It provides (1) a time-management system as well as a prompting system, using a progress bar to visually represent the time spent and remaining; (2) reminder alarms to get user attention if they are distracted; and (3) a motivational message to encourage them to complete their activities. The version of TangiPlan developed by Zuckerman et al.
36
illustrates the Tracking and identification category in the context of assistance with the user’s morning routine. It provides a tracking system to remind the user to complete tasks before leaving the house.
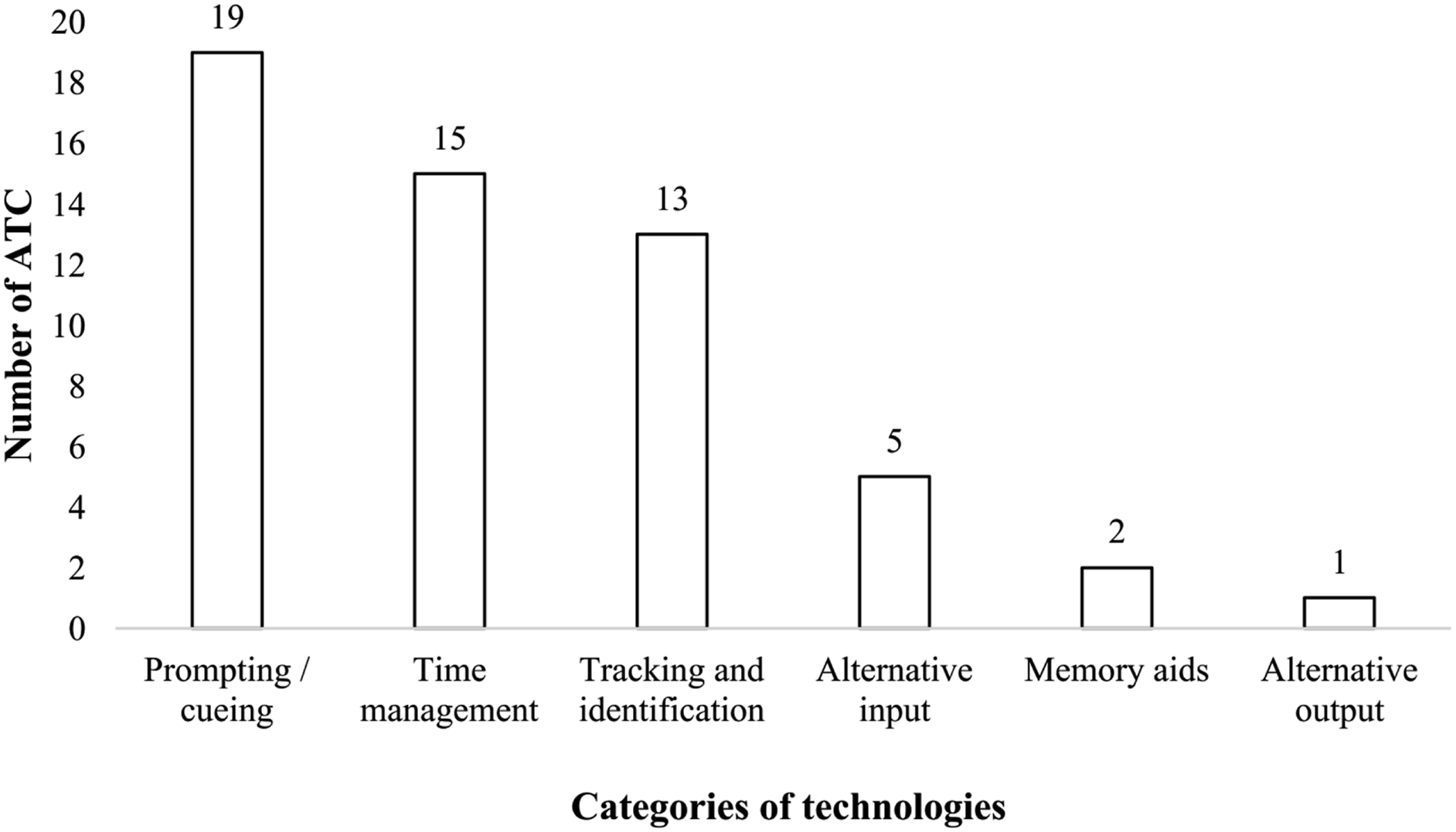
Categories of ATC following the classification of Cook and Polgar 13 . One ATC could be part of several categories (RQ2.1).
Which executive function are targeted by the ATC? (Figure 4 - Tables 11 and 12 in the SM) An ATC could target several EF operations. Planning and carrying out the task were the most supported EF operations by technology (by respectively 25 and 20 ATC out of 27). The ATC presented by Kwan et al.
41
use a smartphone to support wayfinding. Using the smartphone’s GPS application, the ATC supports planning by helping to develop a sequence of steps to get to the destination. GUIDE37,38 illustrates the EF operation of carrying out the task, as it supports the user in completing a task (i.e. prosthetic limb donning) by providing verbal promptings if the user encounters difficulties in making progress in completing their task or has questions.

Number of ATC targeting each executive function operation. One ATC could be part of several categories (RQ2.2).
How were these ATC developed?
Which types of technologies are used by these ATC? (Figure 5 - Tables 13 and 14 in the SM) For clarity, only the major ISO 9999:2022 categories are presented in the figure. An ATC could fall into several categories. Assistive products for managing time, memory, and planning (88.8% of the ATC) and Computers and terminals (85.2% of the ATC) were the most used types of technologies. The category “computers and terminals” includes heterogeneous technologies: computers, ambient technologies, wearable computers, tablets, and smartphones. The HeyJoy Octopus
42
illustrates the category Assistive products for managing time, memory, and planning. It uses a smartwatch to teach the user the concept of time and routine. Computers and terminals could take different forms and could be central to the ATC or just one component of it. For example, Hirsch and Wild
43
use a smartphone to support planning, carrying out the task and verifying attainment of the goal through several applications. Archipel
44
uses a touch screen to display varied information as part of a smart home ATC to support food preparation.
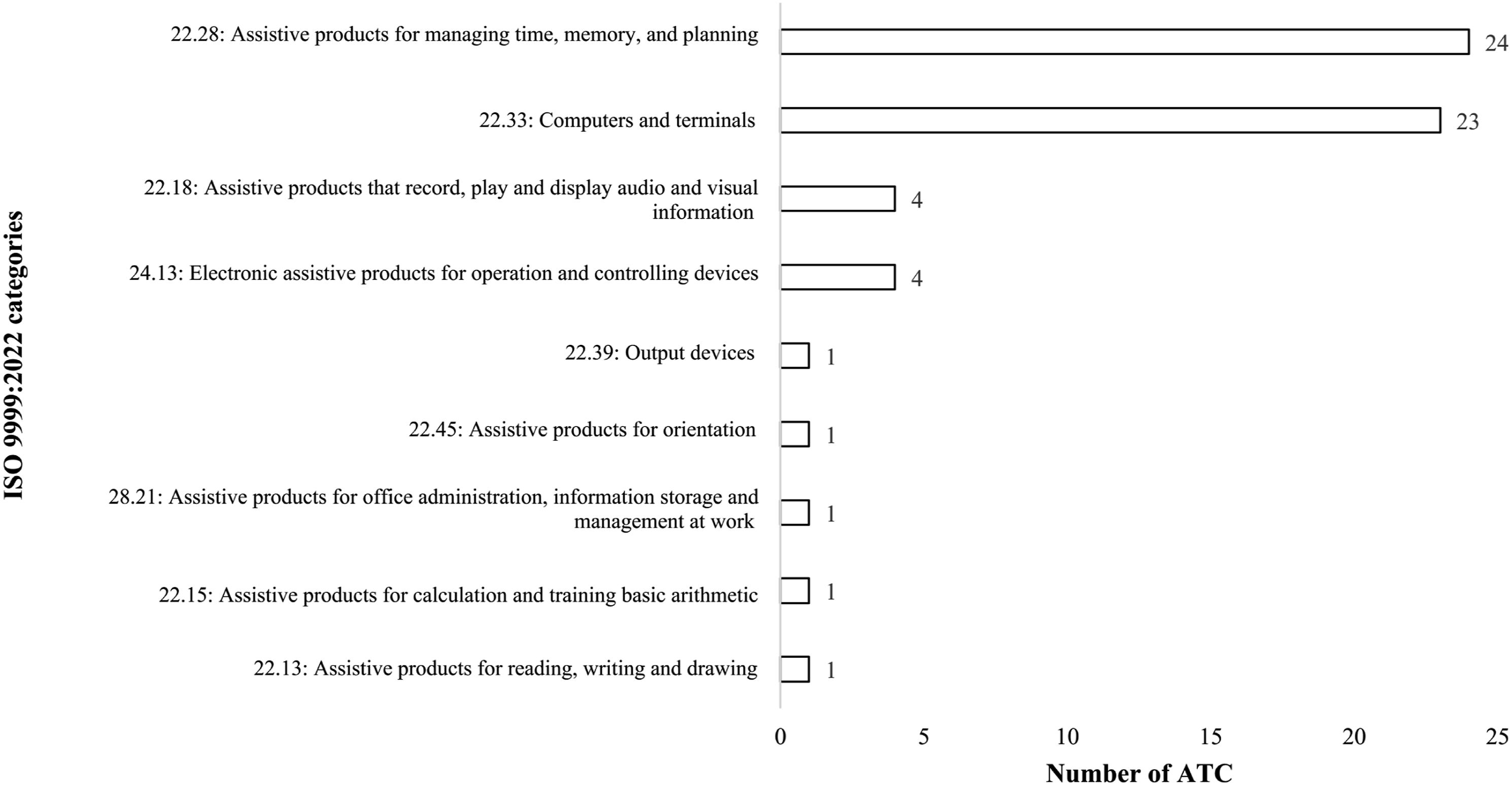
Type of technologies used by ATC according to the ISO 9999:2022 classification 24 . One ATC could be part of several categories (RQ3.1).
Which design methods were used? (Figure 6 - Table 15 in the SM) An ATC could use several design methods. Exploration was used in developing 21 ATC, ideation for one and generation for 25. A combination of exploration, generation and evaluation was used for 16 ATC. The most commonly used methods were: (1) prototyping (generation step); (2) drawing on previous literature (exploration step); and (3) interviews (exploration step). For example, Lapointe et al.
45
primarily used findings in the literature to develop guidelines for maximizing prompt effectiveness. A prototyping phase was also conducted to develop a version that could be evaluated during use by participants. During the development of the Cueing Kitchen ATC,
46
an observation phase was conducted to identify salient features of the participant’s kitchen environment, preferences and emotions during cooking activities. Additionally, interviews were conducted before and after the observations. The first interview aimed to understand the role of cooking in the participant’s life, their rehabilitation process etc. The second interview aimed to collect cooking related anecdotes, accidents, appliances used, etc. From this information, a brainstorming session was held to identify possible technological solutions to unmet user needs. The solutions identified were then implemented in a smart kitchen environment.
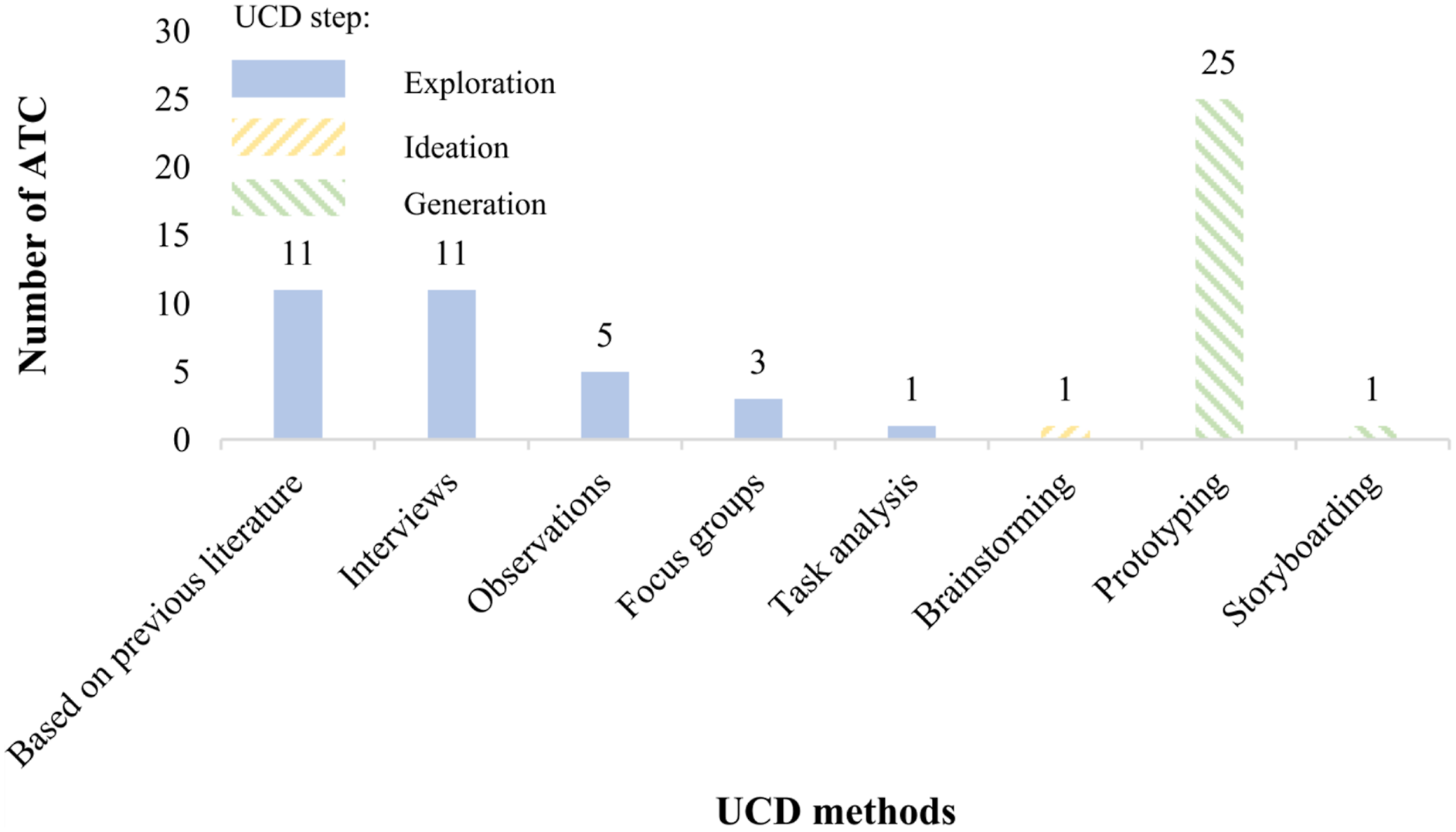
UCD methods based on the classification of Lallemand and Gronier 25 . One ATC could use several UCD methods (RQ3.2). Methods belonging to the exploration step are colored in blue, yellow for the ideation step, and green for the generation step.
Which types of assistance are delivered by the ATC? (Figure 7 - Table 16 in the SM)
The most frequently used types of assistance modality were visual and audio. Twelve ATC used both verbal and visual assistance. For example, one of the requirements identified by Gómez et al. 47 in the development of their ATC was that the interface adapt to the user, i.e. people with TBI, which can be done using different modalities. For instance, their ATC displays text that can also be read aloud. They also provide a picture of the activity to be carried out, accompanied by text. Park et al. 48 rather developed a conversational agent (i.e. audio interactions). Their design focuses on audio, since their target population was children, and, given the democratization of smart speakers, children are familiar with conversational agents.

Number of ATC per type of assistance. One ATC could deliver several types of assistance (RQ3.3).
Are they context-aware?
The majority of the ATC were not context-aware (n = 17; 62.9%). When used, the reasons for having context-awareness vary from one ATC to another. For example, Pollack et al. 49 used context-awareness to adapt reminders to be provided to the user in case of a disparity between expectations of the user and their actual behaviors. The Ambient Kitchen ATC 50 uses context-awareness for activity recognition, based on data from various sensors placed in the user’s environment. COOK 17 uses context-awareness for various purposes, including to detect critical situations.
Was the ATC evaluated with participants? If yes:
w many participants took part in the evaluation? Depending on the study, the evaluation process involved between one and 170 participants, with an average of 22.94 and a median of 6.5. Eight evaluations were conducted in a controlled environment, nine in the participant’s own and two in both. For example, with SAMI, Groussard and al.
51
conducted a study with seven participants in their own environment to evaluate the benefits of mobile services. Cole and Dehdashti
52
detailed various case-studies to illustrate the benefits of customized ATC for people with TBI.
What were the characteristics of the participants? Eighteen systems were evaluated with the target population. Of these systems, four were also evaluated with healthy individuals. For example, Seelye et al.
53
conducted a study comparing three groups: one with multiple-MCI (29 participants), one with a single-MCI (18 participants), and one with healthy older adults (47 participants), each in a controlled environment, to compare perceptions of different types of prompting technologies. Similarly, Etten et al.
54
conducted a study with 170 participants to compare the preferences for different types of prompts: 116 participants were healthy older adults and 54 had medical conditions (MCI, Parkinson etc.).
Which methods were used for the evaluation? (Figure 8 - Table 17 in SM) An ATC could use several evaluation methods. UX diary and user tests were used most frequently. Seven ATC used two or more methods. For example, Navarro et al.,
55
conducted a UX diary study with two dyads (the person with dementia and their caregiver) in the participant’s environment to assess their ATC in the context of taking medication (“responsibility for own medication” IADL). The study was conducted over a period of 16 weeks with regular visits to the participant and caregiver. Questionnaires are also used to evaluate several criteria: apathy, depression, caregiver burden and self-efficacy. To evaluate Mobus, Sablier et al.
56
conducted a six-week UX diary study with nine participants, which took place in the participant’s own environment. A custom questionnaire, completed by the participant after the evaluation, was used to assess their opinion of the system.

Number of ATC using each evaluation method. An ATC could use several evaluation methods (RQ4.3).
What were the main outcomes of the evaluation? (Figure 9 - Table 18 in the SM) Several outcomes were documented by the studies selected. The most recurrent outcomes were acceptability (55.6% of the ATC) and effectiveness (37% of the ATC). For example, in the context of exploring assistive technologies to college students with TBI, Brown and Wollersheim
57
measured usability based on accuracy and rule violation (students had to comply with some rules) and self-evaluation of success (how well they executed tasks). In the context of assistive technology to support productivity at work among people with TBI, Hartmann,
58
evaluated effectiveness through the impact on productivity at work (activities and participation).

Main outcomes used by studies. An ATC could cover several codes (RQ4.4).
What are the goal-directed behaviors targeted by these ATC? (Figure 10 - Table 19 in the SM; Figure 11 - Table 20 in the SM) Ten ATC could theoretically support any activity, i.e. they have been developed from technical choices with respect to impairments without targeting a particular activity. One example would be using a watch to stimulate goal-directed behavior in children with neurodevelopmental disorders.
42
The most supported IADL was food preparation (five ATC), where carry out the task and planning are the most supported EF operations Some of the other IADL were supported by only one ATC each. A single ATC supported BADL, i.e. dressing. Of the five ATC supporting food preparation, four use a similar approach, referred to as pervasive computing (Archipel,
44
COOK,
17
Smart Cueing Kitchen,
46
Ambient Kitchen
50
), and one uses mixed reality (cARe
39
). Archipel, COOK and Smart Cueing Kitchen all report targeted behaviors related to safety in order to generate a safety response by the equipment, for instance, automatically switching off the stove and/or oven in case of critical situations.17,44–46

IADL and BADL supported by the ATC. An ATC could support several IADL or BADL (RQ5). IADL are highlighted in blue, BADL in orange, and those that can be of any category (BADL / IADL / others) are in white.

Number of ATC supporting each activity, per executive function operation (RQ5).
Discussion
The purpose of this scoping review was to provide an overview of studies on ATC that were developed and evaluated to compensate for difficulties related to executive dysfunction in order to support goal-directed behaviors. To the best of our knowledge, this review is the first to explore the domain of executive dysfunctions ATC in such detail.
EF have a strong impact on a person’s ability to continue to live at home and in the community independently.2–5 A first encouraging highlight of this review is the observation that specific ATCs are developed and studied for various disorders.
Focusing on the research questions, the following points emerged from the results: Most of the articles mentioned the target mental disorder. TBI and dementia were the most supported mental disorders. Most of the ATC aimed to provide guidance for procedural or navigational sequential tasks (via prompting/cueing); carrying out the task and planning were the most supported EF operations, whereas formulating a goal was seldom supported. Eighty-eight percent (88.8%) of the ATC supported time management, memory and planning and 85.2% used computers and terminals (tablets, smartphones etc.) to deliver the assistance. It is encouraging to see that the selected ATC cover a wide of technologies. Most studies used generation (prototyping) and exploration (previous literature, interviews etc.) design methods. The majority of the ATC (62.9%) were not context-aware. Seventy percent (70%) of the ATC have been evaluated and the majority of the evaluations were conducted in the participant’s environment. Eighty percent (80 %) of the evaluations were conducted with the target population; Acceptability was measured for 55.6% of the ATC, and effectiveness for 37%. When specified, 45 % of the ATC aimed to support IADL/BADL. Food preparation was the most supported IADL/BADL.
From these highlights, we propose the following research guidelines:
Identify the target population and the severity of the mental disorder (RQ1)
Only a few articles mentioned the severity of the mental disorder. The literature suggests that the requirements can differ according to the severity of impairment.3,4 Hence, it could be suggested to better define the target population to identify their needs in greater detail. This could help increase the ATC adoption, as unmet user needs are one of the most cited reasons for technology abandonment27. The high rate of ATC abandonment is a known problem. 27
Focus on the “formulate a goal” EF operation (RQ2)
Only six ATC focused on goal formulation. In the context of cognitive aging and on the continuum towards dementia, Bier et al. 61 suggest that goal formulation, along with planning, can be the most difficult EF operations. Similarly, in the context of TBI, Lezak 62 indicates that people with TBI have a reduced capacity for defining goals. Regarding ADHD, Denckla 63 suggested they have difficulties with goal initiation. Goal formulation is important, because it is linked to the ability to satisfy a need or to solve a problem. 8 Our recommendation here is to focus more on goal formulation in future studies.
Use observational methods to design ATC (RQ3)
It is worth noting that most ATC were developed based on data collected from interviews or focus groups, and only a few ATC were designed by collecting data from observations (Figure 6). Although observational methods are known to be time-consuming and difficult to implement, especially with populations facing EF-related challenged, 26 they remain an important approach for collecting data without the risk of individual interpretation bias, as well as for obtaining non-verbal information.25,64 Our recommendation is thus to encourage the use of observational methods.
Use ideation methods to design ATC (RQ3)
Regarding the development methods of ATC, only one study used an ideational method, 46 whereas such an approach can bring added value. For example, Mensah et al. suggest, in a study to identify children’s needs, that the persona ideation method can facilitate collaboration and help people identify with the target population. 65 Other articles using persona and targeting diverse populations (Parkinson, aphasia, dementia and TBI) came to the same conclusions.66–71 Our recommendation is to use more ideational methods in the development of ATC.
Use a full UCD process to design ATC (RQ3)
Twenty-three articles used design methods from at least two of the four UCD steps. The literature suggests following a UCD approach to design ATC targeting people with mental disorders20,26,27,72,73 and it is encouraging to see most articles selected for this review at least partially following such a design approach. Among the articles, Hartmann 58 argues that without such an approach, it would not have been possible to identify deficits. Brown and Wollersheim 57 conclude that their results emphasized the need for a person-centred approach to treatment, due to the variability in performance accuracy and system preferences.
Although UCD is advised as a design approach for ATC, some other approaches exist. For instance, three of the selected articles specify the use of a participatory design approach.46,50,51 Mahajan and Ding 46 adopted a participatory approach based on reasoning that the involvement of end-users enhances the design quality of the solution and acceptance of the solution by the user. According to Groussard et al., 51 participatory design allows participants to express their needs and feelings, and to evaluate the proposed solutions. The fact that only a few articles use this approach may be because it seems to be more complex to set up than UCD that does not necessarily involve the active participation of end users. 27 Some design approaches are developed specifically for people with (cognitive) disabilities. For instance, Mihailidis et al., 28 and completed by Boger et al. 27 introduce the principle of zero-effort technologies (ZET), which aim to guide the development of assistive technologies for such populations. Newell et al. 74 introduce the concept of user sensitive inclusive design, to address the specific needs of these populations. Lindsay et al. 75 propose a design approach for people with mild to moderate dementia. None of these approaches are used in the selected contributions. Our recommendation here is to fully implement UCD or an alternative approach to design, develop and evaluate ATCs.
Guidelines for assistance modalities (RQ3)
In the selected articles, there was a prevalence of visual assistance provided to the user by the technology (Figure 7). Among researchers who explain the choice to use audio and/or visual assistance, there seems no clear consensus on the best modality. According to O’Neill and Gillespie, 37 using audio cueing is preferable as it entails less cognitive load, and does not require users to switch focus between tasks for the user. Park et al., 48 who developed a solution for children with ADHD, favor voice interaction to relay information, based on the fact that too much screen time is associated with a 10 % increased risk of future ADHD symptoms. Wolf et al., 39 who developed a mixed-reality ATC targeting people with dementia, only use visual assistance. They argue that findings in the literature suggest that visual cues offer better localization precision and speed than audio cues. Furthermore, their own evaluations suggest that audio cues cannot be localized reliably by the person and have a higher error rate. They also did not consider haptic feedback, as previous literature suggested that this increases cognitive load.
For a target population of people with mild Alzheimer’s disease, Lapointe et al. 45 proposed adapting prompts to the person’s particular deficit (agnosia, memory etc.). They focus on visual and audio prompts, as they suggest that other types (such as smell or touch) are seldom used when performing (I)ADL. Their evaluation suggest that the prompt should target a different sense than the one used to perform the task, to limit attentional disengagement and cognitive load. They argue that more research is needed to define which prompts are the most effective, although they suggest that people with Alzheimer’s disease do not respond optimally to verbal prompts. The literature on ATC suggests that the combination of pictures/words and auditory cues can improve performance.19,20 Furthermore, Etten et al. 54 note from their evaluation that prompt preference is not related to executive EF. Further investigation to determine which types of prompts are suitable according to the type of mental disorder and technology used for the ATC is recommended.
Develop context-awareness ATC (RQ3)
Sixty-three percent of the ATC included in this review were not context-aware. Lopresti et al. 20 suggest that ATC be context sensitive, so that the user does not have to manually inform the ATC of each step they have completed over the course of the entire activity. Lopresti et al. 20 argue that requiring the user to enter each step completed increases the user’s cognitive load, which can in turn increase their frustration and agitation. Boger et al. 27 also mention the importance of context-awareness in ZET design, in order to ensure adaptability of the ATC and to reduce the perceived effort on the part of the ATC user. Our recommendation is thus to encourage the development of context-aware ATC.
Take cognitive load into account in the design and evaluation of ATC (RQ3/RQ4)
The cognitive load induced by ATC was considered in the development of only three ATC37–39 and evaluated in one of them. 39 In our recommendation “Develop context-awareness ATC”, we highlighted the importance of cognitive load.20,27 In the context of a review of ATC for older adults, Rashidi and Mihailidis 76 also suggest that the risk of cognitive overload may be a design issue in ATC. When the use of technologies requires increased user effort, the device may not be readily adopted, or may even be abandoned. 27 Reducing cognitive load is also one of the core principles of ZET, which aims to help design “technologies that require little or no effort to use them” (Boger et al. 27 p. x). Our recommendation here is to encourage researchers to (1) design ATC that require low efforts, for instance by following the ZET principles 27 ; and (2) evaluate the cognitive load, for instance with the NASA-TLX questionnaire. 77 However, some recent articles seem to take this factor into account, such as Jamieson et al. 78 who evaluated task load in the context of the development of a reminder application for people with TBI.
Evaluate outcomes centered on the user (RQ4)
The single-most outcome evaluated by researchers to date is the degree of acceptance of ATCs, followed by effectiveness and user experience. Rashidi and Mihailidis 76 suggest that both acceptance and user experience are considered important when designing ATC.
The domains identified in the taxonomy of Jutai et al., 32 focusing on assistive technologies outcomes, were not often used. This taxonomy is based on the CATOR framework, which aims to “delimit the outcome domains that are important for each key stage of the process that extends from the user’s procurement of an ATD [Assistive Technology Device] through to long-term use or disuse” (Jutai et al. 32 p. 296). It is important to take these aspects into account during the design and evaluation of an ATC, to maximize its long-term use, which is a known issue27,72. We recommend encouraging more consistent evaluation of the outcome of the user. It is encouraging that recent studies seem to point in this direction, such as that by Van Dam et al. 79 who evaluated a social robot whose task was to remind the user to engage in various activities. The team evaluated the impact of their ATC on user independence over a three-month period. Similarly, Ertas-Spantgar et al. 80 evaluated the impact of an ATC on user independence over 6 weeks.
Design ATC that support a wider range of IADL (RQ5)
ATC for food preparation represented the majority of those for which the support of a specific IADL/BADL was mentioned. However, individuals may have difficulties with other IADL, for which assistance is often provided by a (professional) caregiver.81–83 For example, “house cleaning and home assistance” is an activity for which older adults with cognitive decline often require assistance, 84 and yet, to our knowledge, this has not been studied in the field of ATC. Our recommendation is to encourage the development of ATC to support IADL other than food preparation. Recent studies seem to be showing interest in diversifying ATC application to other types of activities, such as Van Dam et al. 79 who evaluated their ATC for various activities such as engaging in household tasks, taking medication or being ready in time for an appointment.
Conclusion
EF have an important impact on the ability to live independently. ATC have the potential to support people with EF impairments in accomplishing activities essential for their independence. This scoping review aimed to provide an exhaustive review of how ATC to support EF impairment are developed and evaluated in the context of goal-directed behaviors in order to identify the research gaps in this area. Analysis of 27 selected articles led to recommendations to guide future research and development of ATC to support EF impairments, focusing on EF operations, design and target activities. The selected articles covered a wide range of mental disorders and technologies and most of them conducted evaluations with the target population.
This review identified some strengths in the current literature, but also has a unique contribution to the field of assistive technologies for cognition by highlighting a number of elements that need to be addressed in the future from a user-centered design perspective. Future research should better identify the target population and the severity of the target mental disorder, while focusing on providing assistance to goal formulation and supporting a wider range of instrumental activities of daily living. Observation and ideation methods could be used more often as part of a complete user-centered design methodology. Evaluations could prioritize user-centered outcomes. There could also be a focus on defining what type of prompts are most appropriate for different types of mental disorders and technologies. Additionally, technologies should have more contextual features while requiring low cognitive load to ensure adaptability and reduce the perceived effort of the ATC.
In sum, this paper was the first to investigate the domain of assistive technologies for cognition designed to support executive dysfunction, identifying research gaps in this area and proposing recommendations for future research and technology development.
Supplemental Material
Supplemental Material - Assistive technologies designed to support executive function impairments while promoting independence: A scoping review
Supplemental Material for Assistive technologies designed to support executive function impairments while promoting independence: A scoping review by Guillaume Spalla, Amel Yaddaden, Hubert Kenfack Ngankam, Charles Gouin-Vallerand and Nathalie Bier in Journal of Rehabilitation and Assistive Technologies Engineering.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de recherche du Québec – Nature et Technologie (FRQNT) – INTER Strategic Cluster and by the Natural Sciences and Engineering Research Council of Canada (NSERC); a salary support award from the Fonds de Recherche du Québec – Santé (NB); a CRIUGM/Age-Well EPIC-AT grant (GS).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.