
Abstract
Augmented reality is increasingly used in health care, yet little is known about how AR is being used in physical therapy practice and what clinical outcomes could occur with technology use. In this scoping review, a broad literature review was conducted to gain an understanding of current knowledge of AR use and outcomes in physical therapy practice. A structured literature search of articles published between 2000 to September 2023 that examined the use of AR in a physical therapy context was conducted. Reference lists of articles for full review were searched for additional studies. Data from articles meeting inclusion criteria were extracted and synthesized across studies. 549 articles were identified; 40 articles met criteria for full review. Gait and balance of neurological and older adult populations were most frequently targeted, with more recent studies including orthopedic and other populations. Approximately half were pilot or observational studies and half are experimental. Many studies found within group improvements. Of studies reporting between group differences, AR interventions were more effective in improving function almost half of the time, with 20%, 27% and 28% showing efficacy in disability, balance, and gait outcomes. AR in physical therapy holds promise; however, efficacy outcomes are unclear.
Introduction
Augmented reality (AR), a technology that superimposes a computer-generated image on an image in the real world, allows interactions between virtual images or objects with real world images. AR differs from virtual reality (VR) technologies in that VR imitates the real world by putting people in an imaginary world, whereas AR is designed to supplement the real world. 1 AR is used in advertising to help consumers virtually project imaginary elements into the real world, such as a couch into a room of their home or can be used to measure the length of a wall with a camera. In medicine, AR is being used to enhance surgery and surgical training,2–5 teach anatomy and physiology6,7 and veterinary medicine. 8
AR presents many applications for the discipline of physical therapy. Physical therapists assess, diagnose, and treat movement disorders to optimize functional independence in patient’s daily lives. AR technology can enhance physical therapy practice by improving providers’ abilities to provide feedback to patients while performing activities. For example, markers projected onto a treadmill or floor can cue a patient to step at certain times as they walk. 9 Markers projected on a screen or wall can facilitate movement of weak extremities to reach a desired target while guiding limb segments to follow specified biomechanically efficient pathways. 10 AR applications could allow patients to visualize a weak or painful limb such as a hand with a weak grip due to hemiparesis from a stroke to practice grasping virtual objects. 11
AR could also be used to provide quantitative feedback to patients and clinicians of movement performance during a clinical test. For example, a patient’s biomechanical musculoskeletal system could be superimposed on their own image while they are performing a squat. 12 As the individual squats, valid biomechanical measurements of flexion, rotation, and abduction could be obtained at the trunk, hip, knees, and ankles providing data to develop a rehabilitation treatment plan, practice movement performance, and evaluate outcomes over time. Use of AR could be beneficial to physical therapy both in evaluation as well as movement performance, particularly if the technology can be deployed successfully in a remote telehealth manner.
Digital telehealth is a rapidly growing field, accelerated by the COVID pandemic. The COVID pandemic lockdown and restricted access to healthcare accelerated the need and desire to perform clinical care remotely in people’s homes. 13 As care was increasingly delivered in the home, clinicians recognized the opportunity to use telehealth to allow access to care, provide greater flexibility and convenience to receiving care, and a broader understanding of the contextual home environment of the patient. 14 Collecting objective data (e.g., range of motion, balance) in one’s home was challenging with use of standard telemedicine platforms including Zoom and google hangout.
AR could have several applications in physical therapy, yet little is known about how AR has been used in physical therapy and whether efficacy outcomes are established. In a recent systematic review of 11 studies with meta-analysis of four randomized controlled trials published in 2021, 15 the authors found AR in conjunction with physical therapy treatment targeting balance and function had a small non-significant beneficial effect on balance and a small statistically significant effect on the timed-up-and-go test among adults with stroke16,17 and older adults.18,19 In the study, high heterogeneity was noted with limited generalizability. Given the rapid growth of AR in healthcare and the potential of AR to augment physical therapy care, it would be beneficial to understand historical development of the technology, the areas of focus and applications, current evidence, and future directions of this technology in physical therapy practice. To address these needs, we conducted a scoping review to (1) examine how AR technology is evolving in the field of physical therapy among adults, (2) describe the types of AR technologies that are being evaluated for use in physical therapy applications, and (3) describe the outcomes of physical therapy related AR technology to date. Since the research on the application of AR in physical therapy practice is in its infancy, our aim with this scoping review was to examine broad applications of AR on physical therapy and forecast how applications of the technology are evolving.
Methods
A scoping review was conducted using recognized guidelines. 20 Following Peter et al.’s guidelines, 20 the intent of scoping reviews is qualitative in nature and targeted to “assess and understand the extent of the knowledge in an emerging field or to identify, map, report, or discuss the characteristics or concepts in that field.” We approach this study, from this broader qualitative framework.
Search strategy
An experienced librarian was consulted to conduct a structured search of published scientific literature from 2000 to September 2023 was performed in PubMed, Pedro, Cochrane, and CINAHL databases. The keyword strategy used to identify how AR has been incorporated into physical therapy practices included “augmented reality” AND (“physical therapy” OR “rehabilitation” OR “exercise”) AND (“pain” OR “recovery of function” OR “gait” OR “prognosis”). Articles were limited to English language. See appendix for full search strategy in each database. Reference lists of articles selected for full review were searched to identify additional studies. Review articles identified in the search were not included in the data extraction process but reference lists were searched for additional articles to be considered for full text data extraction. (See Appendix 1 for full search strategy)
Criteria for considering studies
Articles were selected for inclusion if (i) the subjects included adults (over age 18) undergoing treatment that could be provided by a physical therapist, (ii) the technology tested was a type of AR, and (iii) if the study was designed to examine an outcome of AR in the context of physical therapy treatment. Articles were excluded if the article only discussed technology developments of AR, if the technology used was solely VR, the study sample was not a population generally treated by physical therapy, or the AR technology would not be used to treat a patient condition seen by physical therapists.
Study selection and data extraction process
Articles identified in the literature search were uploaded to Covidence to organize, review, identify duplicates, and select the articles. Titles and abstracts of all articles in the initial search were reviewed by three trained reviewers (PYH, JS, MW). Two reviewers independently reviewed each study title and abstract to decide which articles would be included for full review. Disagreements were discussed and, if needed, adjudicated by the full study team. Full text articles were reviewed by two independent reviewers for inclusion into the data extraction process. Disagreements were discussed and, if needed, adjudicated by the full study team. A data extraction table was developed to guide extraction of data from full text articles. The following fields were included in the data extraction table: (i) study design, (ii) study sample characteristics, (iii) primary diagnosis and sample size, (iv) AR technology description, (v) intervention vs. assessment, (vi) outcomes, and (vii) general notes. Three trained reviewers independently extracted data. Disagreements were discussed and, if needed, adjudicated by the full study team.
Assessment of the methodological quality
AR applications in general adult populations.

F: female; M: male; CG: control group; EG: experimental group; TUG: timed up and go; ROM: range of motion; LE: lower extremity.
Data analysis
Data were analyzed descriptively and qualitatively. To examine efficacy outcomes, results of primary outcomes from the clinical trials were used. Between group scores were used to establish efficacy; within group scores were deemed not to establish efficacy between groups but treat. Themes were generated across all domains through careful synthesis as well as summary counts. Consensus was used for all elements of synthesis.
Results
549 articles were identified through the search strategy; 40 articles met study criteria for full review. (See Figure 1) 10 articles included general adult samples (four pilot studies,21–24 six experimental studies).12,18,19,25–27 (Table 1); 22 studies included adults with chronic neurological conditions (15 pilot case or observational studies studies;9–11,28–39 7 experimental studies.16,17,40–44) (See Table 2) Four articles were of orthopedic populations, (1 pilot study
45
3 experimental studies).46–48 (Table 3) One study examined clinical outcomes of pulmonary function after knee surgery,
49
one study was among women recovering from breast cancer surgery,
50
one study of older women with sarcopenia,
51
and one patient with burns.
52
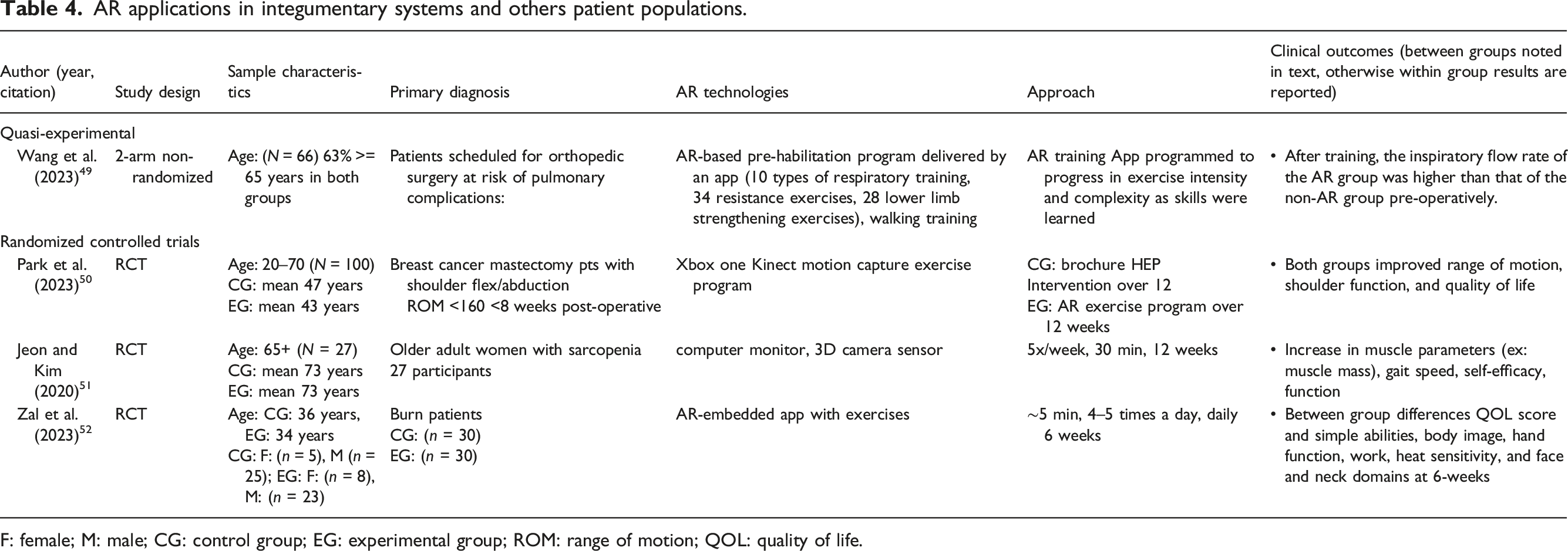
(Table 4) Consort diagram. AR applications in chronic neurologic populations. F: female; M: male; CG: control group; EG: experimental group; TUG: timed up and go; ROM: range of motion; FES: functional electrical stimulation; FMA: Fugl-Meyer assessment. AR applications in orthopedic populations. F: female; M: male; CG: control group; EG: experimental group; ROM: range of motion; WOMAC: western Ontario and McMaster universities arthritis index; EQ5D5L: Euroqual 5-dimensions quality of life; NRS: neuromuscular recovery scale; BBS: berg balance scale; MMT: manual muscle test; DASH: disability of the arm, shoulder and hand; SPADI: shoulder pain and disability index. AR applications in integumentary systems and others patient populations. F: female; M: male; CG: control group; EG: experimental group; ROM: range of motion; QOL: quality of life.


2005 was the first publication of AR in a physical therapy context—a case study of adults with stroke using a head mounted device that facilitated visualizing the patient’s hand over a virtual object (Figure 2).
28
Between 2005 and 2015, 10 studies were published: eight studies of chronic neurological patients9,11,16,17,28–30,40 and two studies of general adult populations.19,21 Between 2016 and 2023, 30 additional articles were published: 14 studies of chronic neurological patients,10,31–39,41–44; eight studies of general adults,12,18,22–27; four studies of orthopedic patients,45–48; one study of pulmonary function among surgical patients,
49
; one study of patients recovering from breast cancer surgery,
50
; one study of older women with sarcopenia,
51
; and one study of patients with burns.
52
Of the 30 studies, 14 were published between 2022–2023.12,23,27,37,39,43–50,52 The four studies of orthopedic populations45–48 were published since 2022 as were the study of patients with burns and breast cancer.50,52 Number of articles published by year.
Summary of clinical outcomes reported in randomized controlled studies: between group differences, within group differences, for no improvement for each outcome examined in the cited study.
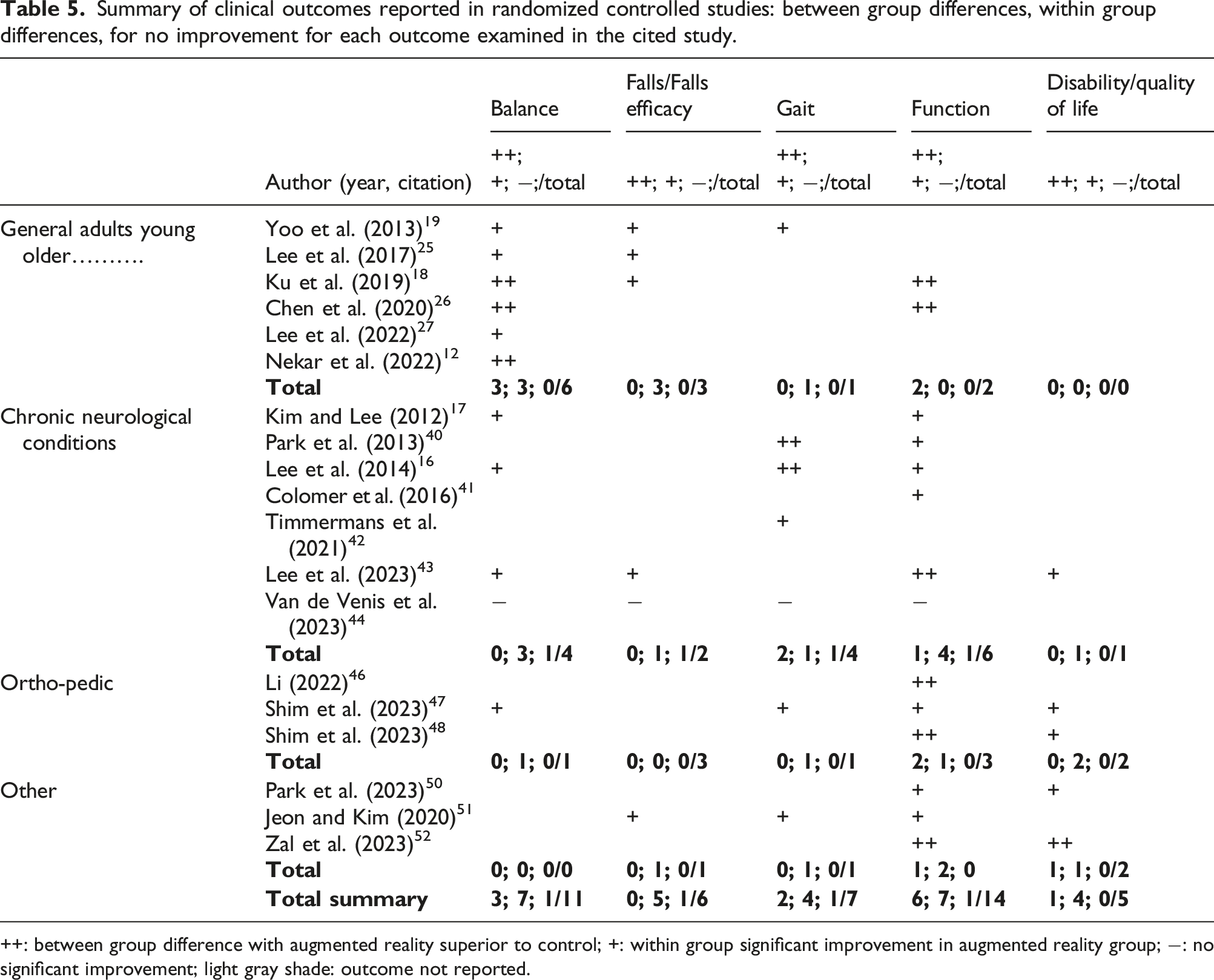
++: between group difference with augmented reality superior to control; +: within group significant improvement in augmented reality group; −: no significant improvement; light gray shade: outcome not reported.
Of the seven experimental studies of chronic neurological adult populations, six studies were of subjects with strokes,16,17,40–43 and one study was of subjects with spastic paresis (n = 1)., 44 (Table 2) AR improved stride length compared to control group in two studies examining gait outcome.16,40 One study showed between group differences in gait velocity.16,40 Within group differences were observed in muscle strength, 17 muscle tone, 17 balance,16,17 fear of falling, 43 gait speed, 42 quality of life, 43 and upper extremity function. 41 (Tables 2 and 5) In one study of people with hereditary spastic paraplegia, people who received C-mill treadmill with AR did not show any improvements in balance, gait or falls. 44 (Tables 2 and 5) Sample sizes ranged from 16 to 68 and were relatively similar between studies that found between group differences and those that did not. Intervention intensity generally ranged from 20 min 3x/week to 60 min 5x/week for four to 8 weeks. Types of AR applications varied across studies. Results of experimental studies were similar to pilot studies.
Among the three recent experimental studies of orthopedic populations, (see Tables 3 and 5) one study showed an AR knee surgical recovery program had significantly higher improvements in pain and function compared to a traditional knee surgical recovery program among people recovering from knee surgery. 46 Similarly, among people recovering from rotator cuff repair, an intervention using AR with a Kinect and 3-dimensional camera compared to a conventional written home exercise program resulted in improved clinical shoulder outcomes. 48 On the other hand, there were no between group differences in clinical outcomes among patients recovering from total knee replacement surgery, however, the AR group did have within group difference in knee replacement clinical outcomes. 47 Sample sized ranged from 40 to 115. Two studies used the UNICARE AR system, an AR platform integrated into Xbox One Kinect with 3-dimensional camera sensor serial plug-and-play device that translates scene geometry into depth information to track the movements of 25 joints with mixed results.47,48 Duration of intervention ranged from 6 to 12 weeks.
A randomized control trial of 70 patients recovering from burns reported significant between group differences in quality of life, function, body image, Hand function, work, heat sensitivity, and face and neck domains at 6-weeks. 52 (See Table 4) Increased muscle performance was noted in an AR based exercise program among 27 older adults with Sarcopenia when exercising for 30 min 5 days/week for 12 weeks. 51 (Table 4) On the other hand, within group differences were found with an AR exercise based 12 weeks program among breast cancer surgery patients. 50
AR was utilized for a therapeutic context in all but one study. Borresen et al. 45 examined the ability of AR to accurately assess shoulder range of motion and strength remotely. Gait, balance, and function were targeted most frequently (Table 5).46–48,50 One study examined the use of an AR platform to improve pulmonary function among people undergoing surgery at risk of pulmonary complications and found the AR intervention superior to conventional care. 49
In summary, of published studies to date approximately half are pilot or observational studies and half are experimental studies. (Figure 3) Of the experimental studies, the clinical outcomes of balance, gait, function, or disability/quality of life were reported 43 times, with AR improving outcomes similar or superior to conventional approaches in 93% (n = 40/43). (Table 5) AR interventions were more effective in improving function almost half of the time (n = 6/14, 47%) with 20%, 27% and 28% showing efficacy in disability, balance, and gait outcomes. No study found between group differences with AR in improving falls or falls efficacy. Improvements in balance, falls, gait, function, and disability were noted in 64% (n = 7/11), 83% (n = 5/6), 57% (n = 4/7), 50% (n = 7/14) and 80% (n = 4/5) respectively. AR did not improve clinical outcomes among people with hereditary spastic paraplegia.
44
Number of studies of neurological, general adults, orthopedic, and integumentary and other conditions (observational study designs in gradient color; experimental study designs in solid color).
Discussion
The literature evaluating the use of AR in physical therapy applications is in its infancy but growing rapidly. This scoping review shows there is promise in AR technologies to improve clinical outcomes; however, it is unclear if AR is superior to conventional treatments. Outcome assessments are short-term and little is known about how AR could augment conventional rehabilitation in the home setting. Most of the research to date examines use of AR among chronic neurological and older adult populations, with recent advances in orthopedic and cancer surgery rehabilitation and burn rehabilitation. About half of the studies are experimental and half are pilot or observational studies.
The types of AR interventions were highly variable making it difficult to compare outcomes across studies. In our study, balance, gait, and function outcomes were shown to have the best evidence supporting AR interventions. Disability outcomes were rarely studied and outcomes assessed were highly variable across studies. As the field grows, it is imperative to establish the clinical effects across important patient clinical outcomes such as function, disability, participation, and quality of life. 53
Our results are similar to Gil et al., 15 : and we concur that generalization of findings is limited due to the small number of studies, small sample sizes, and large heterogeneity in study methodology. Our study differs from Gil et al. 15 as the nature or our scoping review was to examine the broad context of AR applications in physical therapy, rather than determine the efficacy of AR which was the focus of Gil et al.’s 15 investigation that included a meta-analysis of four studies. We aimed for a broader analysis to characterize overall use of AR in PT in today’s clinical practice in order to capture applications of AR in a broader context.
Most investigations of AR to date are in the controlled experimental or clinical setting and conducted over short time periods. In our study, there were no investigations of use of AR as a supplement to conventional treatment to support additional practice of evidence-based treatment in the home setting, yet this is a critical need. Using technologies to facilitate home based treatment in conjunction with clinical care could enable greater practice of therapeutic skills and movement and perhaps integration of therapeutic strategies into daily activities and improved long-term outcomes. 54 In this context, AR technology could bridge the clinic to the home. 54
One mechanism by which AR may effectively augment physical therapy is by providing meaningful feedback to patients and therapists to motivate and guide treatment which can promote improved performance and motor recovery.12,18,26,43 Meaningful feedback is recognized as important for motor recovery, correct performance of exercises for strength training, and behavior change. 12 AR can provide this type of meaningful feedback and could be used in a remote digital telehealth application thereby providing the clinician with a better understanding of movement in the home and community setting. AR technologies could also be motivating and foster adherence and increase effort at specific tasks.24,55 Newer applications of digital technologies support applications of AR with mixed digital programing such as virtual reality, perhaps even in a gaming context to promote interest and engagement of therapeutic activities in the home setting. Adherence of evidence-based rehabilitation for people with chronic conditions is critical for clinical outcomes, yet the majority of people with chronic conditions do not engage in recommended programs. AR could be a tool to support adherence to recommended activities and could provide objective information for providers and possibly provide incentives for health plans. 56
Our finding that the type of AR technology was highly varied between studies concurs with others. 15 High heterogeneity will limit the generalizability of findings, and it may be helpful to have a classification system to define technology types. Different approaches may result in different outcomes, and for physical therapy, it may be meaningful to develop an AR classification system that aligns with clinical and therapeutic needs that can then link to physical therapy outcomes. 55
Only one study in our review examined the use of AR to conduct a clinical exam in a virtual setting: a small pilot study that examined reliability and validity over one time point. 45 The ability to quantify biomechanical movement virtually could guide clinical decision making and could have major implications on the measurement of clinical outcomes remotely. Use of AR in this domain is promising but assessments must be valid and reliable. Much research is needed in this area.
Digital health applications are anticipated to increase substantially over the next decade. The use of AR in physical therapy practice is in its infancy and research is limited. With the explosion of technology development and potential to augment physical therapy, it would be fruitful to align research inquiries with the field of implementation science. 54 Implementation science, as applied to healthcare, is the field of study that examines how novel approaches are adopted and implemented by consumers (e.g., healthcare providers, patients, and insurance regulators). Usability of systems is paramount and perspectives of end-users of technology provide valuable direction as to how the technology should be used. Integrating clinicians and patients in technology development is essential. AR is a technology that could be incorporated within existing treatment paradigms and principles of implementation science can help guide the understanding of barriers and facilitators to adoption while simultaneously evaluating efficacy.
As technology is developed for implementation, researchers and clinicians must consider and optimize accessibility. Technologies need to be accessible across clinics and user groups as well as accessible across function and cognitive abilities. Additionally, to assure equitable access costs of technologies need to be considered across user groups.
To our knowledge, this is the first study examining the evolving context of the use of AR in physical therapy related applications. Understanding the breadth of AR applications can help researchers advance the field of study. However, our study has a few limitations. First, while we employed a rigorous search and screening process, we may have missed articles with our scoping review methodology and broad exploration of our topic. Second, our study may have some biases as study quality and meta-analytic approaches were not used to determine study results. Third, definitions of AR in articles were not always clear and as such we may have missed articles. Forth, given the AR field in physical therapy is in its infancy and is under a great deal of development, studies that did not find within or between group differences may not be published leading to potential publication bias.
In conclusion, AR is rapidly evolving in the field of physical therapy and will likely continue as digital technologies are growing at an unprecedented rate. Many clinical questions need to be answered, and to do so rigorous methodological study designs of important patient and health service clinical outcomes must be employed. First, AR technologies, particularly those that are used to quantify movement parameters need to be validated with gold standard approaches. Second, efficacy and pragmatic studies are needed to identify which clinical populations benefit from AR approaches, what dosing is needed for clinical outcomes, and whether outcomes are short- or long-term. An important opportunity for AR is to promote adherence to evidence-based interventions. Studies should carefully study long-term adherence and long-term outcomes as physical therapy interventions tend to be relatively short-term as adherence drops after care is terminated. Further, as technologies are adopted for practice, research efforts should identify implementation strategies and outcomes.
AR holds promise in physical therapy. Without a doubt, the next decade will see an explosion of AR, likely integrated with other digital technologies, incorporated into clinical and community treatment approaches. Perhaps the most appealing application of AR is to augment clinical-based physical therapy with guided practice of exercises and movement with feedback to the patient and clinician for self-monitoring in the community; yet little is known as to whether and how AR could support clinical practice in this manner.
Footnotes
Acknowledgements
We would like to thank Marjorie Wickenden in the support of reviewing article abstracts for inclusion in full text review, extraction of data in full text review, and for data synthesis in early drafts of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by NIH grant 2R44AG072991-02.