
Abstract
Introduction
Early mobilisation is paramount in the rehabilitation of patients with acquired brain injuries. However, the effectiveness of mobilisation to standing combined with passive leg movement in mitigating orthostatic intolerance remains uncertain. Hence, we investigated whether participants exhibited better tolerance standing in a motorized standing device with passive leg movements, Innowalk Pro, compared to a traditional standing frame.
Methods
17 patients with acquired brain injury (<1 year post-injury) performed two sessions in each standing device on four separate days. Maximum standing time was 30 min, less when symptoms of syncope or volitional exhaustion occurred. Besides total standing time, electromyography of thigh muscles, and changes in mean arterial pressure and heart rate were monitored at rest and during standing.
Results
No significant differences were found in standing time, changes in mean arterial pressure or heart rate between standing in Innowalk Pro and the standing frame. However, participants had significantly more thigh muscle activation (p = 0.006) when standing in Innowalk Pro.
Conclusions
Mobilising participants with a subacute acquired brain injury in a standing frame with motorised passive movements of the lower limbs did, despite higher thigh muscle activation, not lead to better orthostatic tolerance or prolonged standing time compared to a traditional standing frame.
Introduction
Early mobilisation, including movements of the joints and transition into sitting and standing, is an important part of the rehabilitation of patients with severe functional deficits after acquired brain injury in the acute and subacute phases. This approach has been found to improve general physical function including normalizing the orthostatic state,1–6 that is haemodynamic response to postural changes, and to reduce the mechanical ventilator usage, systemic complications and length of hospital stay.7,8
Conventional methodologies employed for mobilising the patients from supine or seated to standing position have historically encompassed beds with tilt function, tilt tables, and standing frames, each offered in various iterations. The process of mobilising patients with acquired brain injuries into a weight-bearing upright stance during early stages of their recovery, presents notable challenges, and sometimes demanding due to prolonged time of immobilising, often due to medical instability and protracted stays in the ICU. 2 Notably, Riberholt et al. (2013) showed that the cardiovascular system in such patients exhibited inadequate adaptions to passive standing regimes. 5 However, patients with an acquired brain injury often suffer from non-neurogenic orthostatic hypotension (OH) (i.e. caused by reduced cardiac output and/or impaired vasoconstriction without a primary autonomic disorder) 9 and/or a neurogenic OH (i.e. inadequate vasomotor sympathetic release of norepinephrine due to autonomic dysfunction). 10 It is challenging to differentiate between OH directly caused by the injury to the autonomic nerves system and OH caused by immobilisation (a prolonged period in supine position).
A static standing frame provides essential support to sustain an individual in an upright, motionless stance, securing the feet, knees, chest, and pelvis without enabling movement of the lower limbs. However, advancements in technology have ushered in a new era of more dynamic assistive devices, exemplified by the Innowalk Pro (Made for Movement, Norway), a robotic end effector device incorporating passive, repetitive leg movements in step-like movements while the patient is an upright position. A systematic review conducted by Glickman et al. revealed that dynamic aids with passively, repetitive leg movement provided greater activity during standing compared to a static standing frame. 11 Correspondently, Luther et al. mobilised nine patients with acquired brain injury and orthostatic dysfunction into a tilt table equipped with motorized mechanisms for passive movements of the lower limbs. 2 Six out of nine patients showed less signs of autonomic dysfunction (orthostatic hypotension, increased sweating, etc.) while standing in this device compared to standing in a tilt table without passive leg movements. 2 These findings suggest that the incorporation of passive leg movement may support orthostatic tolerance while facilitating the transition of these patients to a more upright position. Furthermore, in a single case study by Wesche et al., a patient with acquired brain injury reported a subjective sense of comfort and well-being associated with leg movement while assuming an upright stance. 12
However, the precise mechanisms underpinning the observed enhancement in orthostatic tolerance resultant from passive leg movements remain elusive. There is a lack on studies elucidating the dynamics of heart rate (HR) and blood pressure (BP) regulation during the early mobilization of individuals with acquired brain injury. Additionally, the extent of muscular engagement in the lower extremities during motorized passive leg movements while assuming an upright posture remains uncertain. Electromyography (EMG) represents a valuable tool for estimating muscle activity, quantified in microvolts. The EMG signal arises from the generation of electrical currents facilitated by ion exchange across muscle membranes during muscle activation, detectable via surface electrodes. 13
In healthy people, during normal locomotor activities (e.g., walking, chair climbing), veins physically located within large muscle groups, are alternately compressed and decompressed. 14 This promotes venous return to the heart, influencing both BP and HR control. During mobilisation from supine to vertical position, this mechanism increases BP and HR, and thereby counteracting orthostatic intolerance, that is an abnormal response to being upright causing, dizziness, nausea, and other symptoms that disappear when seated or lying down. 15 Czell et al. showed that passive leg movement during a tilt table test stabilized blood circulation and prevented syncope in healthy adults. 16 One could expect a similar circulatory collapse in patients with neurological diseases or injuries because of the missing venous pump due to paralyzed leg muscles. 9 Our objective was to compare the tolerability of standing in a motorized standing device (Innowalk Pro, Made for Movement, Skien, Norway) versus traditional standing training using a standing frame among patients within the initial year following a brain injury and possessing limited prior experiences with standing mobilization.
The main research questions were: (1) How long are patients with major functional outcomes after acquired brain injury able to stand in a standing frame and in the Innowalk Pro, respectively, and what limits the standing time within a time frame of 30 min? (2) Do patients with major functional disabilities after acquired brain injury have an immediate better orthostatic tolerance when using the Innowalk Pro compared to a standing frame? (3) What is the relationship between orthostatic tolerance and muscle activity, measured by EMG, in the lower extremities when using the Innowalk Pro and a standing frame, respectively?
Furthermore, we aimed to investigate the perceived exertion associated with standing in both the Innowalk Pro and the traditional standing frame, as well as the level of satisfaction and any encountered inconveniences among the participants.
Our hypotheses posited that individuals would be capable of sustaining a longer standing duration in the Innowalk Pro in comparison to the static standing frame. Additionally, we hypothesized that participants would exhibit greater lower limb muscle activity and improved orthostatic tolerance while undergoing mobilization in the Innowalk Pro as opposed to the static standing frame.
Methods
Design
Explorative cross-sectional study.
Participants
Persons (18 - 85 years of age) admitted to Sunnaas Rehabilitation Hospital, with a recent (< 1 year) severe acquired brain injury and with few mobilisation experiences in a standing position, were included in the study.
Participants were excluded if they had other significant concurrent medical conditions that might limit their ability to be in an upright position or because of severe cognitive impairments affecting their ability to cooperate. Furthermore, due to constraints associated with the Innowalk Pro, participants with a body weight exceeding 95 kg (kg) and/or a body height surpassing 190 cm (cm) were excluded from participation. Following medical approval from their attending physician, patients were invited to take part in the study. Subsequently, valid informed written consent was obtained for all participants prior to their inclusion. In instances where a participant lacked decision-making capacity, informed consent was obtained from their legal guardian.
Procedures
To characterize the participants’ functional capacity, Functional Independence Measure (FIM) motor score and FIM cognitive score, 17 assessed upon admission, were extracted from the electronic patient records. Prior to enrolment in the study, all participants underwent a head-up tilt test to assess their orthostatic tolerance and ascertain their ability to maintain a passive upright position. 18 Subsequently, each participant engaged in total four standing exercise sessions: two sessions utilizing a standing frame (Delta 2004 Evolution, DLF - Shaw Trust Black, Oldbury, UK) and two sessions utilizing the Innowalk Pro, with the order of sessions randomized. Prior to the head-up tilt test and each standing exercise session, muscle tone in the knee flexors, extensors and ankle plantar flexors was assessed with the Modified Ashworth Scale (MAS), which ranges from 0 to 5. 19 MAS assessment was conducted to determine if muscle activity, as measured by electromyography (EMG) during the standing exercise sessions, correlates with increased muscle tone.
During the standing exercise sessions, both HR and BP were measured by ProBP 3400 Series (Welch Allyn, Skaneateles Falls, New York, United States)- and IntelliVue X3 (Philips, Amsterdam, the Netherlands) monitors and electromyography (Muclelab, Ergotest Innovation AS, Stathelle, Norway) in two thigh muscles (at both sides) were recorded. The head-up tilt test, and all four standing exercise sessions were performed within 14 days, with a minimum of 24 h in between each session. Participants refrained from altering the dose or type of blood pressure medication within the 2 weeks following their enrolment in the study inclusion.
Head-up tilt test
During a head-up tilt test, the participants’ compensatory hemodynamic responses to orthostatic stress are measured. 20 This test is commonly used in clinical practice, but with a variety of protocols, variants and extensions. 21 In our study, participants started this test in supine position on a tilting table (with 0 incline), with straps over their knees, hips and chest, for 5 minutes. Thereafter, the tilting table was raised every fifth minute, to respectively 20°, 40°, 60° and 80°. Throughout the entire protocol, participants’ blood pressure (BP, mmHg) and heart rate (HR, beats/minute) were monitored continuously, with measurements taken every minute. The test was terminated if the participants exhibited any of the following criteria: a heart rate increase exceeding 30 beats per minute, a systolic blood pressure decrease by exceeding 20 mmHg or decrease diastolic blood pressure surpassing 10 mmHg and/or the onset syncope. The head-up tilt test was limited to a maximum of 30 min.
Standing exercise sessions
The standing exercise session were performed at the same time each day. Prior to each standing session, an experienced physiotherapist evaluated the participants’ muscle tone for both knees and ankles in the supine position using the MAS. Subsequently, participants were equipped with a B-cuff on each upper arm, to facilitate rapid measurement of BP and HR.
Preparatory measures for electromyography (EMG) assessments included the removal of hair from the designated skin areas, followed by skin abrasion if needed, and subsequent cleansing with an alcohol wipe. The areas were then air-dried to optimize adherence of the EMG electrodes. 22
Surface EMG dual electrodes (Dymedix Diagnostics, Shoreview, MN, USA), with 2.5 cm separation, were attached along the direction of the muscle fibres on the M. Vastus Medialis (VM) and M. Biceps Femoris (BF) and an additional reference electrode the medial femoral epicondyle (Figure 1). The VM (vastus medialis) sensors were positioned at approximately 4/5 of the distance along the line connecting the spina iliaca anterior superior and the anterior aspect of the knee joint, anterior to the medial collateral ligament. The BF (biceps femoris) sensors were situated at approximately halfway along the line connecting the ischial tuberosity and the epicondyle of the tibia.
22
The surface electrodes were affixed using a double-channel electromyography (EMG) cable connected to a wireless EMG module. The wireless EMG module placed on the thigh muscles, attached with an elastic ribbon.
During the initial 5 minutes of each standing exercise session, participants remained in seated position, with BP, HR and EMG recordings taken every minute during minutes 3-5. In the sixth minute of the protocol, participants were gently elevated to standing position over a span of approximately 20 s. During minutes 6-10 BP, HR and EMG were obtained every 30 s. Thereafter, from minutes 11-35 BP, recordings of HR and EMG were taken at 5 minutes intervals. Throughout the standing exercise sessions, participants were verbally encouraged to maintain the standing position as long as possible, up to a maximum of 30 min which closely reflects typical clinical practice. If participants chose to end the session before the 30 min mark, there were queried the reason for termination.
Standing frame
Participants were initially seated on the bench with their feet on the floor in front of the standing frame (Figure 2). A staff member positioned themselves behind the participant to provide support in maintaining a seated posture. Subsequently, the protocol started. During the session utilizing the standing frame, additional exercises such as passive arm mobilisation, balloon hitting, ball throwing, etc. were incorporated whenever feasible. However, to ensure the integrity of the measurements, no additional exercises were conducted while BP and HR measurements were being taken. Delta 2004 – standing frame.
Innowalk pro
The Innowalk Pro (Figure 3) was meticulously adjusted to accommodate the individuals’ height ensuring proper alignment of the seat, backrest, knee, and chest supports. Following the initial measurements obtained in seated position while at rest, the participants were raised to a standing position, and the Innowalk Pro initiated cyclic movements of their legs. Participants capable of voluntarily moving their arms and hands, were encouraged to utilize the handlebars (see Figure 3). Alternatively, for participants unable to actively engage their arms, they were passively placed on a tray affixed to the device. The speed of the passive cyclic leg (and arm) movements was standardized to 30 rates per minute (RPM), although participants had the option to increase this speed actively or have it adjusted by the therapist if it was considered appropriate. Innowalk Pro – motorized standing frame.
Outcome measures
The main outcome measures were time (minutes) participants were able to maintain an upright position during the standing exercise session, muscle activation score, and orthostatic tolerance (changes in BP and HR during the standing exercise sessions).
Additionally, to measure participants’ perceived exertion while standing in both the Innowalk Pro and the standing frame, the Borg Rating of Perceived Exertion (RPE) Scale, ranging from 6 to 20, was employed. 23 This numeric scale, widely utilized in clinical exercise testing, serves as a common tool for assessing perceived exertion. Moreover, Likert scales were utilized to monitor participants’ satisfaction levels with the exercise sessions (Likert; 1-5), and to capture any encountered inconveniences during training (Likert; 1-4). These subjective scales have demonstrated applicability in measuring exertion-related symptoms during steady-state exercise. 24 After the last session, participants were queried regarding their preference for future training modalities, with options including the standing frame, the Innowalk Pro, or expressing no definitive preference. Additionally, any adverse events encountered throughout the study duration were documented.
Data analysis
Heart rate (HR) readings were recorded and the mean arterial pressure (MAP) was computed for each measurement using the formula: MAP = DP + 1/3(SP – DP). ∆ MAP and ∆ HR were calculated as the difference between BP readings taken at rest and the final BP measurement taken during the standing exercise session.
The EMG-signals, which were sampled at a frequency of 1000 Hz, were processed automatically through a built in 20Hz-500 Hz band-pass filter in the Musclelab software (Muclelab, Ergotest Innovation AS, Stathelle, Norway). Using a custom-built VBA-script in Microsoft Excel 2016 (Microsoft, Washington, United States) the signals were checked for noise, rectified and a 50-point moving average of the absolute values of the signals were calculated. Measurements classified as noisy, were excluded from further analysis.
Given the absence of a defined threshold for muscle activity based on electromyography (EMG) signals in existing literature, the authors adopted a novel approach in this study. Muscle activity was defined as three times the average standard deviation (SD) of the resting EMG signal. Subsequently, an average activation value for both the biceps femoris (BF) and vastus medialis (VM) muscles was computed for each day’s measurements during the standing exercise session.
For every session, each of the four muscles was then categorized as either active 1 or not active (0) based on the calculated average activation. These individual muscle scores were aggregated for each day, yielding a scale ranging from 0 to 4, where a score of 0 signifies negligible muscle activity, while a score of four indicates activity detected in all four muscles.
In this study, we considered a MAS score of 0-1 as ‘no increased muscle tone’ and a MAS score of 2-5 as ‘increased muscle tone’.
Statistical analysis
Statistical analyses were performed with SPSS (IBM Corp. Released 2024. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp). Given the limited sample and data skewness, descriptive statistics are presented as median and minimum-maximum (min-max), unless stated otherwise. For all tests, statistical significance was set at an alpha level of 0.05. Demographic, functional characteristics and questions concerning user satisfaction were processed using descriptive statistics.
To compare the participants’ standing time and changes in HR during standing exercise between the Innowalk Pro and standing frame, related-sample Wilcoxon Signed ranked test was conducted. Additionally, paired t-tests were employed to compare the participants’ muscle activity score and changes in mean arterial pressure (MAP) during standing exercise in the Innowalk Pro versus the standing frame.
Results
17 individuals, comprising 11 males and six females, with a median age of 56 years (range: 23-73), were recruited during inpatient rehabilitation at Sunnaas Rehabilitation Hospital through consecutive enrolment spanning a 3 year period (2020–2022).
The participants’ demographics and injury-related characteristics at admission to the hospital.
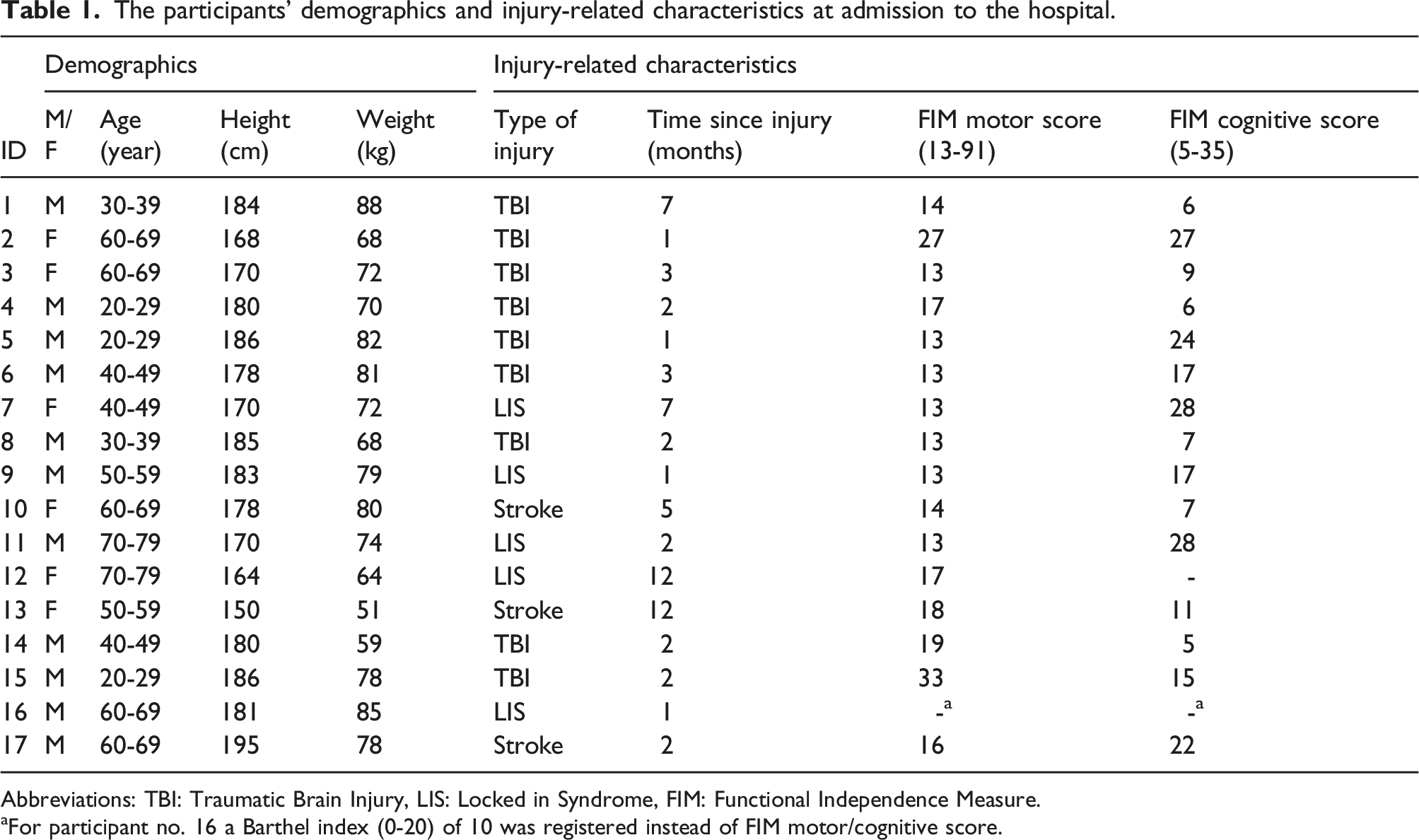
Abbreviations: TBI: Traumatic Brain Injury, LIS: Locked in Syndrome, FIM: Functional Independence Measure.
aFor participant no. 16 a Barthel index (0-20) of 10 was registered instead of FIM motor/cognitive score.
Two participants (no. 10 and 14) performed the head-up tilt test but did not complete any of the standing sessions due to medical complications. Two other participants (no. 7 and 11) performed only one Innowalk Pro session and one standing frame session due to medical complications, which were not related to the standing training. The other 13 participants performed all four training sessions.
The Modified Ashworth Scale (0-5) for knee flexors, knee extensors and plantar flexors was measured before each training session. Despite a substantial proportion missing data (32%), results showed that four out of 14 participants with available scores day 1-4, had an increased muscle tone (MAS ≥2) in one or more of the measured muscles (bilateral), before the exercise sessions. 5.1 % of the MAS measurements had a score of 2, distributed on four participants. Two of these four participants had measurements of MAS 3, totalling 2.5 % of all measurements. The remaining scores in these participants indicated no increased muscle tone. No increased muscle tone (MAS 0 or 1) was found in twelve (of 14) participants on day one, eleven (of 13) on day two and eight (of 11) on day three and four.
Participants’ standing time, muscle activity score and changes in heart rate and mean arterial pressure during standing exercise in Innowalk Pro and standing frame.

Abbreviations: min: minutes, b/min: beats per minute, mmHg: millimetre of mercury, MAP: mean arterial pressure, HR: heart rate, MA score: muscle activity score. The muscle activity score (0-4) represents the number of thigh muscles showing EMG activity above resting values.
We found no significance difference between the Innowalk Pro and the standing frame in median standing time (respectively 275–30 minutes vs 26.514–30 minutes, p = 0.80), median ∆HR (respectively 16 (0-49) beats/min vs 196–28 beats/min, p = 0.293) or mean ∆MAP (respectively 3.1 (SD: ±15.2) mmHg versus −2.8 (SD: ±7.4) mmHg, p = 0.203). However, the mean muscle activity score during training sessions with Innowalk Pro (1.60, SD: ±0.67) was significantly higher (p = 0.006) compared to the standing frame (0.97, SD: ±0.58). Chi-square tests of independence showed no significant association between muscle activity score at test day 1 and 2 for the Innowalk Pro (p = 0.87) nor the standing frame (p = 0.93), showing a high day-to-day variation in muscle activity score in both standing devices. Moreover, we found no significant association between the participants’ muscle tone (MAS) prior to the exercise sessions and their muscle activity score during the standing exercise sessions.
Test performance
Number of sessions completed/terminated and reasons for termination of single sessions for each of the standing devices.

aThree participants reported pain in the knee, leg or the whole lower extremities.
bTest personnel terminated the session due to large fall in systolic blood pressure (>20mmHg).
Perceived exertion
Eight out of 17 patients expressed their perceived exertion (Borg scale, 6-20) after the first session with a median score of 11 (min-max 7-20), 7 after the second with a median score of 14 (min-max 11-20), and five patients after the third and four session respectively median scores of 11 (min-max 6-15) and 13 (min-max 9-13). Many participants (43 out of 68 possible answers) were not capable of answering these questions due to exertion/tiredness or lack of ability to communicate.
Satisfaction, disadvantages
Due to either cognitive impairments and/or tiredness, rather few participants were able to score the Likert scales. Satisfaction with the training sessions scored on a Likert scale from 1 to 5, (1 = very dissatisfied, 5 = very satisfied), was represented by 26 of 68 possible scores. 17 were satisfied (score 4), four were very satisfied (score 5), while five were neutral (score 3).
Disadvantages from the training sessions scored on a Likert scale from 1 to 4, (1 = major disadvantages, 4 = no disadvantages) were also represented by 26 of 68 possible scores. Participants answered 19 times either no disadvantages [12] or negligible disadvantages [7]. The remaining seven participants experienced minor disadvantages [6] or major disadvantages [1]. Visual inspection of these Likert scales revealed that experienced satisfaction was rather similar for the two devices.
Only six out of 15 participants were able to answer which standing device they would prefer to continue with in the further course. Three participants preferred Innowalk Pro, while three had no definite preferences.
Discussion
This investigation involved individuals with subacute acquired brain injury who underwent mobilization using the Innowalk Pro and a standing frame, while various physiological parameters were monitored. Our findings revealed no significant difference in standing duration between the Innowalk Pro and the standing frame. Additionally, participants exhibited no notable differences in mean arterial pressure (MAP) and heart rate when assuming a standing posture in either of these devices. Nevertheless, participants demonstrated markedly greater activation of thigh muscles while standing in the Innowalk Pro compared to the standing frame. Furthermore, despite several standing sessions being terminated prior to the intended 30-min duration, participants expressed satisfaction with the standing exercises conducted in both devices.
In their study, Czell et al. 16 showed that individuals without known health conditions who experienced syncope or near-syncope during a conventional head-up tilt test were able to stabilize their blood pressure (BP) during a subsequent head-up tilt test. This test was conducted on a tilt table equipped with passive movements facilitated by a motorized stepper, effectively preventing syncope. These findings contrasts with the outcomes of our study, which might be explained by an inadequate vasomotor sympathetic release of norepinephrine due to autonomic dysfunction in the participants with TBI. 10 Another contributing factor might be the disparity in mobilization techniques; our study involved transitioning participants from a seated to a standing position, as opposed to the supine-to-standing mobilization employed by Czell et al. Moreover, in our study participants were encouraged to be physical active during their sessions in Innowalk Pro as well as in the standing frame, while the lower limbs of the healthy participants in the study of Czell et al. were moved passively. EMG measurements during the standing sessions with passive leg movement confirmed that participants had no muscle activation in Czell’s study versus significant muscle activation (mean muscle activity score of 1.6 on a scale from 0 to 4) in our study.
The significantly higher muscle activation score during standing in the Innowalk Pro, was not accompanied by a higher increase in mean HR, which can be expected as a response to a higher oxygen demand in active muscle tissue. However, an increase in HR can also occur as a response to a fall in MAP, that is to maintain orthostatic tolerance. 18 On average, the participants in our study had an increase in MAP of 3.1 (±15.2) mmHg while standing in the Innowalk Pro, versus a minor decrease in MAP of −2.8 (±7.4) mmHg while standing frame. Although no statistically significant difference (p = 0.203) in ∆MAP was found between the two standing devices, a difference of 5.9 mmHg might have influenced the participants’ HR response to some extent.
The participants’ muscle activity score (0-4) during the standing exercise and their muscle tone (MAS) before the exercise sessions were not associated. This indicates that the higher muscle activation score measured during the Innowalk pro, seems to be voluntary muscle activity rather than uncontrolled increased muscle tone caused by disrupted signals from the brain.
Unlike the results in a study by Luther et al, 2 our study did not find prolonged standing time or less cases of syncope during mobilisation with leg movement. However, since Luther et al 2 did not measure any physiological parameters such as HR, BP and muscle activity during head-up tilt testing, it is challenging to compare these two studies in further detail.
The most common reason for determination was tiredness. Interestingly, like blood pressure drop and dizziness, this could also be a symptom of orthostatic hypotension (Table 3). The results show that the participants had rather similar reasons for termination between the two standing devices. This in in contrast to Luther et al. who found 2 that six out of nine patients had less signs of autonomic dysfunction (orthostatic hypotension, increased sweating, etc.) while standing in standing device with passive leg movements, compared to without.
Riberholt at al. showed, as in our study, no difference in the number of adverse events, serious adverse events, or adverse reactions between head-up mobilisation with stepping versus standard care in patients with severe traumatic injury. 25
Methodological limitations
The data collection in this study was performed during the COVID-19 pandemic, which contributed to a lower sample size and longer recruitment period than expected. The pandemic also entailed isolation restrictions which has caused some dropouts and missing data.
This extensive age span (20-75 years) of the participants in our study, covers a diverse range of musculoskeletal systems, introducing notable variations among participants. Several physiological variables such as muscle strength, blood pressure and heart rate are highly age-dependent and might therefore have affected the statistical significance of these study results. 26
Our study included participants diagnosed with various forms of acquired brain injury, such as locked-in syndrome (LIS), traumatic brain injury (TBI), and stroke, thereby introducing heterogeneity into the sample. Moreover, due to increased risk of intracranial pressure and other medical complications during subacute inpatient rehabilitation, the time from admission to enrolment varied. The heterogeneity in our study population and the large variation in time-to-inclusion might partly explain the large individual differences in standing time, muscle activity score, and in ∆HR and ∆MAP during the standing exercise sessions.
The maximal standing time was set to 30 min, as this time frame is close to clinical practice. However, several participants were able to stand longer than 30 min indicating a ceiling effect in the outcome measure ‘standing time’. On the other hand, we only included patients that passed the head-up-tilt test, 18 and thereby excluding patients with severe autonomic dysfunctions. Our results are therefore only applicable to patients with acquired brain injury with mild symptoms of orthostatic intolerance.
In this study the muscle activity score is based on muscle activity (i.e. EMG values) in the biceps femoris and vastus medialis muscles. However, the effect of muscle activation in other lower extremity muscles on orthostatic tolerance should not be neglected. As the participants knees were immobilised in the standing frame, most muscle activation would be expected in the calf muscles (not in the thigh muscles). This could explain why participants in this study showed a significant higher thigh muscle activity score in the Innowalk Pro. As hips and knees are immobilised in the standing frame, the Innowalk Pro has more potential to facilitate larger muscle groups around the knee and hip during standing exercise sessions.
We found large day-to-day differences in ∆HR, ∆MAP and muscle activity score, for both standing exercise modes. Kalra et al 9 stated that the severity of symptoms of orthostatic hypotension often varies day-to-day or throughout the day and can be affected by ambient temperature, physical exertion, and food and fluid intake. These factors, and cognitive fatigue, have not been controlled for which could explain the day-to-day variations in our study. And, since both neural and local peripheral factors contribute to the control of skeletal muscle blood flow, 27 several other factors that might play an important role in the interaction between sympathetically-mediated vasoconstriction and the effect of local vasodilatory factors, have not been taken into account.
Patients with acquired brain injury often have cognitive impairments and become fatigued quickly. The low cognitive FIM scores in several of the participants in our sample might explain why some participants were unable to answer questions on how they experienced the standing sessions. Consequently, due to the limited number of answers in our study we could not detect any possible indifferences how participants experienced (i.e. Borg scale, satisfaction and disadvantages) training in the standing frame versus Innowalk Pro. Only six participants answered which training form they would prefer to continue with in a future perspective.
Clinical implications
Mobilising to upright position has become a central component of the rehabilitation of patients with acquired brain injury in the acute, subacute and chronic phases.11,28 The current study confirms that mobilising patients is feasible, and most of them tolerated this type of standing exercise for 30 min. Our study results indicate no differences in orthostatic tolerance between standing with or without passive motorized leg movements, which is of clinic importance for those working with this patient group. Standing exercise in the Innowalk Pro entailed more thigh muscle activation and may indicate that this cyclic movement can be positive for standing/walking function in the long term. Moreover, early mobilisation combined with voluntary muscle activity can potentially affect other rehabilitation outcomes, as physical exercise regimes seem to improve brain plasticity and neurocognitive performance in persons after acquired brain injury.29,30
Conclusions
Mobilising participants with an acquired brain injury in the Innowalk Pro did, despite a higher thigh muscle activation, not lead to prolonged standing time compared to a traditional standing frame. The participants had similar changes in MAP and HR when standing in the standing frame and Innowalk Pro. Thus, motorised passive movements of the lower limb in upright position, did not increase orthostatic tolerance in the participants of this study.
Footnotes
Author contributions
MFW was responsible for designing the research protocol, data analysis, testing of the patients and writing the manuscript. EIB contributed to the protocol, data analysis, testing of the participants and gave feedback on the manuscript. EH contributed to the protocol, data analysis and writing the manuscript. APW contributed to the protocol, testing of the participants, and writing the manuscript.
VJ contributed to the protocol and gave feedback on the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Research funding from a third part (Made for Movement) causes competing interests. However, the funder only had a minor role for in the conceptualization of the study. The authors hereby declare that data collection, data analysis and preparation of the manuscript, have been performed without any involvement of the funder.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Made for Movement, Norway.
Ethical approval
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research. The study was approved by the Regional Committee for Medical and Health Research Ethics (Ref: 106287) and the Norwegian Centre for Research Data (Ref: 669181). The study is registered in ClinincalTrials.gov (NCT04452019).
Data Availability Statement
Additional data are available from the corresponding author on reasonable request.