
Abstract
Introduction
Many barriers to physical activity (PA) exist for individuals with spinal cord injury (SCI). Social engagement may improve motivation to perform PA, which in turn may increase PA levels. This pilot study investigates how social engagement facilitated by mobile technology may reduce lack of motivation as a barrier to PA in individuals with SCI and demonstrates design implications for future technologies.
Methods
A user-needs survey was conducted with participants in the community. We recruited 26 participants (16 individuals with SCI and 10 family members or peers). A participatory design process using semi-structured interviews was used to identify themes relating to PA barriers.
Results
One theme related to PA barriers was lack of PA-focused forums to connect with peers. Participants with SCI considered connecting with other individuals with SCI more motivating than connecting with their family members. Another key finding was that participants with SCI did not perceive that personal fitness trackers were targeted towards wheelchair-based activities.
Conclusions
Engagement and communication with peers who have similar functional mobility levels and life experiences can potentially improve motivation for PA; however, PA-motivational platforms are not tailored towards wheelchair-users. Our preliminary findings show that some individuals with SCI are not satisfied with current mobile-technologies for wheelchair-based PA.
Introduction
Spinal cord injury (SCI) is a chronic neurologic condition that affects nearly 300,000 individuals in the United States, with 18,000 new incidences per year. 1 Individuals with SCI have a predisposition to secondary conditions including pressure injuries, urinary tract infections, diabetes, cardiovascular disease, obesity, osteoporosis, and arthritis. 2 Physical activity (PA) has been shown to reduce the risk for secondary conditions in SCI. 3 According to recommendations from a recent study, adults with SCI should engage in at least 20 min of moderate-vigorous intensity aerobic exercise training twice weekly, in addition to three sets of 8–10 repetitions of resistance training to each of the major muscle groups. 4 Most individuals with SCI do not perform the recommended amounts of PA, and individuals with SCI are at higher risk of physical inactivity than the general population. 5 Individuals with SCI are at risk for health complications, and the disproportionate lack of PA compared to the general population exacerbates their health risks further.
Barriers to PA have been explored in previous research. Common barriers to PA for individuals with SCI include lack of accessibility to exercise equipment or facilities due to cost, infrastructure, or transportation; lack of caregiver assistance; pain; fear of injury; lack of energy; lack of motivation; and lack of encouragement, support, or companionship from family and peers.6–9 In addition to the barriers to PA, facilitators to PA have been identified as well. For example, while lack of caregiver assistance, motivation, and access to facilities are barriers, sufficient caregiver assistance, motivation, and accessible facilities are facilitators of PA.8,10
Peer support and peer mentorship foster a sense of community and provide social support for individuals with SCI.11,12 Peer support groups serve an important role on interdisciplinary teams in rehabilitation, offering a valuable source of education and contributing to improvements in PA levels.11,13 A recent review found that person-based support, including peer support, can also provide motivation to facilitate increased PA. 14 Fulfillment of peer support needs in individuals with SCI is also associated with greater participation in outdoor activities. 15 Online support groups allow individuals with SCI to connect with each other and offer reciprocal support with reduced barriers to access. 16 Use of technology to facilitate participation in peer support groups eliminates environmental barriers, such as lack of transportation, and aligns with increasing demands for virtual communication. Receiving virtual support eliminates the concern of accessibility of in-person meetings.
The prospect of using technology-based interventions for wheelchair-based PA is promising. Mobile technologies have been used to track PA and provide feedback regarding activity levels to foster behavioral change in PA patterns.17,18 The Transformative Exercise Framework 19 describes the transformation from rehabilitation exercises in a healthcare setting to PA in the community. The concept of transformative exercise is to support the transition from rehabilitation to wellness in people with disabilities. For individuals with disabilities, wellness includes routines in the community that encourage active living. In a Canadian case study for individuals with stroke, community programs facilitated the transition from hospital-based rehabilitation to community-based rehabilitation by incorporating physiotherapists to navigate patients through the progression. 20 A similar community-based program for individuals with chronic neurological disorders led to improved PA levels by having participants engage in a fitness center program. 21 Building on this framework, we hypothesize that incorporating social engagement into mobile technologies may promote community-based PA in the wellness phase and reduce barriers to PA such as lack of motivation and lack of support from family and peers.
A health outcomes intervention that leveraged social media by using a smartwatch that tracked PA levels and a Facebook group to deliver health education tips increased intrinsic motivation, feelings of social support, and PA levels in college students. 22 Another study identified that real-time feedback and social support networking were effective strategies for PA modification in older adults. 23 To our knowledge, use of technology-assisted social engagement to address barriers of PA has not been explored in individuals with SCI. We conducted this research to identify barriers to PA for individuals with SCI in the community that may be addressed through a technology-based intervention that provides timely social support during PA. Furthermore, this research assessed user needs to inform development of an application that alleviates barriers to PA through social connection. The objectives of this pilot research was to investigate how social engagement impacts motivation for PA in individuals with SCI, and to explore if motivation and social support could be improved through social engagement. This research also informs the development of potential features for technology-based interventions that contribute to improvements in wheelchair-based PA levels.
Methods
Participants
Participant demographic information. All values are reported as n (%) or mean (SD).
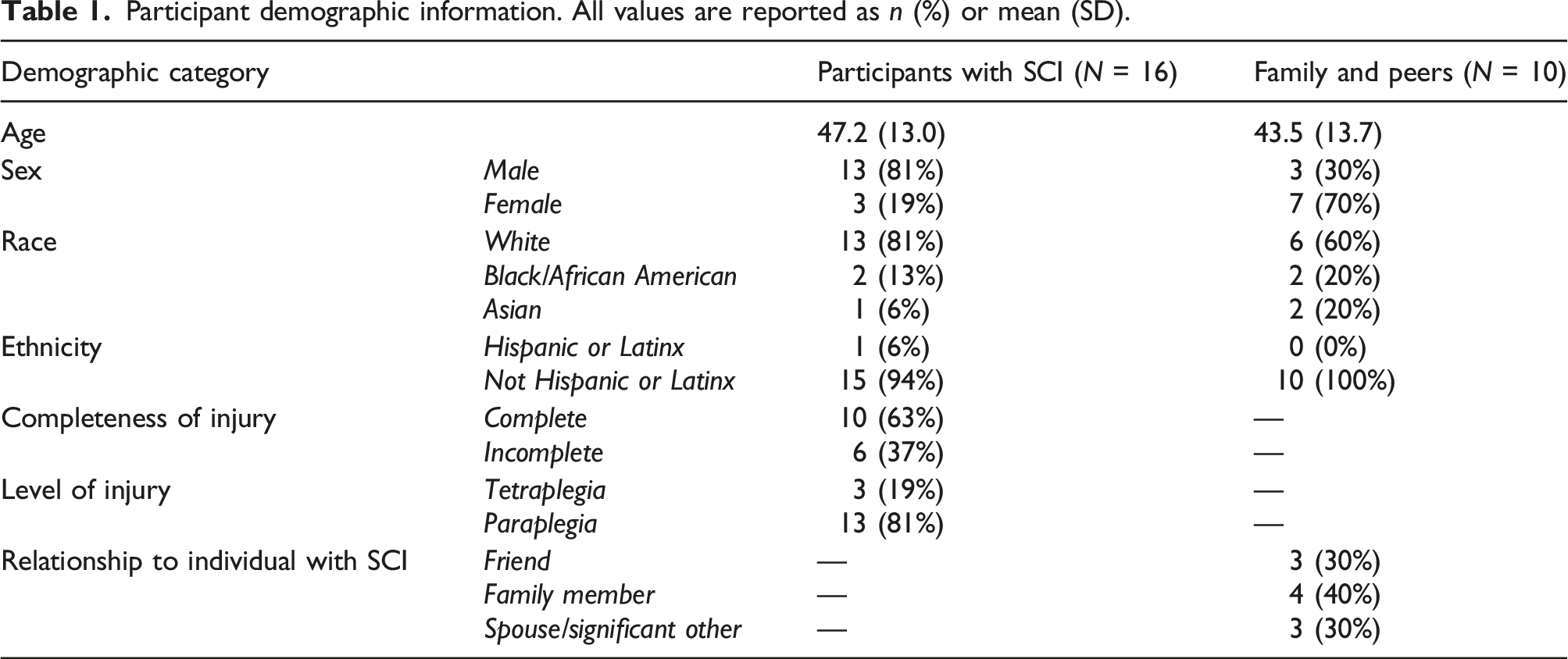
Participants were recruited as dyads; each participant invited a family member or peer to participate. Some participants were recruited individually if they did not have family or a peer to join them in this study. Family and peers were included to provide perspective on how caregiver support can influence PA and to understand the perspective of the individual’s support network. Eligibility for individuals with SCI was determined by the following criteria: 18–75 years of age, had a history of traumatic or non-traumatic SCI, used a manual wheelchair as primary means of mobility (>80% of time), interested in increasing PA, and could use smartphone and smartwatch independently. Participants with SCI were excluded if they had health conditions that make PA medically contraindicated, had a history of traumatic brain injury, or were currently pregnant. Family and peers of individuals with SCI were recruited in conjunction with participants with SCI when possible. Family and peers were eligible to participate if they were at least 18 years old, able to use a smartphone and smartwatch independently, and their PA was not medically restricted. All participants provided informed consent and were compensated $20 per session for their time. This study was approved by Temple University’s IRB (protocol 27,645).
Procedures
This study was conducted as proof-of-concept for development of a technology-based physical activity intervention for individuals with SCI in the community setting. The National Institute on Disability, Independent Living, and Rehabilitation Research Framework for Development describes that the proof-of-concept stage verifies if a product concept is feasible by testing components to resolve any potential technical challenges. 24 The next stage of development is proof-of-product, in which a fully integrated prototype of the product is created to test with participants, and the final stage, proof-of-adoption, evaluates the benefit of the product. 24 For this study, a participatory design process was used, which entailed conducting semi-structured interviews to assess the individual and interpersonal needs and challenges of individuals with SCI. These interviews explored and identified themes relating to barriers for PA, which have been incorporated into the iterative development of a prototype smartphone and smartwatch application to be tested in the proof-of-product stage. This mobile-health technology is intended to engage individuals with SCI and their support networks to improve PA levels.
Five virtual interview sessions were conducted remotely using Zoom video conferencing software. The first session to obtain consent and demographic information lasted about 30 min, and the subsequent four sessions lasted 60–90 min each. Content and interview questions for each session were developed in conjunction with an SCI consumer advocate on our research team. In the second and third sessions, interview questions were focused on individual PA routines and preferences, individual and interpersonal motivators and barriers to PA, social support for performing PA, and communication habits with family members and peers. Based on interview responses, investigators identified key features that could be incorporated into a technology-based intervention to support social engagement and communication. These features were explored in the fourth and fifth sessions; they included scheduled messaging with context-aware triggers that facilitate delivery of encouraging feedback at appropriate times, integrated templates for communication about PA and suggestions for conversation related to PA, and various methods to share PA achievements with others (Figure 1). Mock screenshot of a smartphone application conceptualizing a feature to share physical activity with others. Left side demonstrates the notification that the user sees. Right side demonstrates a message that appears on peer’s phone if the user shares their notification.
Analysis
A total of 102 interview sessions representing approximately 46 h of content were conducted. Audio recordings were transcribed using Zoom software and manually reviewed and edited for accuracy. Personal identifiers were removed from transcripts, and participants were assigned a participant identification number (i.e., S01 or P01, with S indicating a participant with SCI and P indicating a family member or peer). Two researchers independently coded transcripts using Quirkos software (version 2.4.1), labeling and categorizing quotations. Using thematic analysis, 25 themes were generated, reviewed, and defined to develop a codebook by consensus.
Results
Participant comments on established barriers to physical activity.

Participant comments on the lack of physical activity-focused forums to connect with peers.

Participant comments on applications tailored to wheelchair-based activities.

PA-focused forums
Participants with SCI, as well as their family and peers, agreed that a platform for individuals with SCI to connect with peers with SCI would be beneficial. One participant rationalized the need for easily accessible forums because wheelchair users strive to be independent. More than half (10 out of 16) of our participants with SCI considered connecting with other individuals with SCI motivational; however, a key finding was that five participants perceived connecting with peers to be more motivating than connecting with their family. Communicating with other wheelchair users unlocks a new understanding for individuals with SCI. Three participants with SCI indicated they would be less receptive to communication promoting PA from their family members who are caregivers than to communication from family members who are not caregivers, friends, or peers. The nature of relationships affects how communication is interpreted. It was also conveyed that there are limited opportunities for individuals who use wheelchairs to perform PA together, and it is difficult for able-bodied individuals to relate to the barriers to PA faced by individuals with SCI.
Fitness tracking tailored to wheelchair-based activities
Four participants with SCI expressed that they did not perceive that personal fitness tracking devices and applications were targeted towards wheelchair-based activities, even if wheelchair-based activity options were available. Participants expressed dissatisfaction with wheelchair-based options, stating that they are inconvenient to use in other fitness applications. Motivation can be increased by designing technologies specifically for wheelchair users, rather than having wheelchair-based activities as an option in technologies designed for ambulatory users. Another participant conveyed interest in differentiating between levels of functional mobility when using wheelchair-based PA technology. Interest in competing with other wheelchair-users was a prevalent theme that was mentioned by six participants with SCI, and they felt that the notion of competing with other individuals in wheelchairs was motivational. A platform tailored to wheelchair-based activities would also be motivating because of the connection to others.
Discussion
Many barriers to PA exist for individuals with SCI, including lack of motivation and support from family and peers.6–9 Along with these common barriers, three additional technological barriers were presented in our work: lack of tailored, PA-focused forums to connect with peers, and lack of personal fitness tracking devices available on the market, and applications tailored to wheelchair-based activities. Activity sensors designed to detect walking are not accurate for wheelchair-users, and although some devices that detect wheelchair-based PA have recently become commercially available, they have not been validated in community settings.
26
Both barriers may be mediated through a socially engaging mobile technology for wheelchair-based activities. Using technology to promote higher PA levels can bridge the gap between rehabilitation and participation in community-based PA. Improvements in motivation achieved through socially engaging mobile technology can be sustained after transitioning from rehabilitative exercise to community-based PA for wellness.
19
The interpreted connection between these themes, social engagement, and motivation is depicted in Figure 2. Interpreted connections between emergent themes related to barriers to physical activity.
An important aspect of social connection is the relationship between the individuals who are socially interacting. Relationship dynamics affect comfort of communication related to PA. Individuals with SCI may prefer to share experiences about PA with other peers who are wheelchair-users, rather than family or friends who they feel may not be able to relate to them. Therefore, the effectiveness of motivational communication may vary depending on the nature of a relationship and how communication is interpreted, particularly in relationships between caregivers and care receivers. Sometimes, caregivers and care receivers perceive the functional abilities of the care receiver differently, which may lead to a power dynamic.
In a qualitative study utilizing seven dyads of individuals with SCI and their caregivers, emotional support from caregivers was a facilitator to self-management, and caregiver burnout was a barrier to self-management. 27 The presence or absence of support from caregivers can generate either facilitators or barriers to self-management. Likewise, the presence and absence of peer support can generate facilitators or barriers for PA. 10 In our findings, we also discovered that, more generally, a lack of barriers can be a motivator for some individuals. Cost of equipment and accessibility of facilities were recognized barriers for participants with SCI, however the opportunity to borrow or rent sports equipment or having arrangements to participate in outdoor activities motivates the performance of PA. The simple absence of barriers may be a facilitator in circumstances when performing PA that requires advanced planning and commitment.
Gorgey 7 found that clinicians failing to provide appropriate exercise routine based on spared muscle function is a barrier to PA for individuals with SCI. Several of the participants in this study reported levels of PA that exceed recommended minimums for individuals with SCI. Individuals with SCI who are physically active have likely adapted patterns for PA. 4 Some patterns of PA may reflect preferences or personal interests, such as emphasis on stretching or adaptive sports, whereas other patterns may have developed as a result of intact muscles and level of physical function. PA that is personalized and reliably structured to minimize barriers in conjunction with consistent support of individual needs is valuable in maintaining long-term engagement in PA and lifestyle changes. Wheelchair sports facilitate connecting with team members, but for wheelchair users who are not interested in team sports, a mobile application could serve as a substitute platform to connect with each other.
In summary, our findings have determined that PA-focused communication with peers within a wheelchair-based PA application may increase motivation for individuals with SCI to participate in PA. These findings could inform the development of technology-based interventions by promoting features that combine a platform for peers with similar goals to connect, with an interface that is specifically designed to collect wheelchair-based PA.
Limitations and future implications
This study has several limitations. Due to the COVID-19 pandemic, our recruitment efforts were limited to virtual strategies. Retention of participants through all five sessions was also a limitation of this study, as two participants completed only four sessions, six participants completed only two sessions, and two participants completed only the first session. We suspect the virtual nature of this study and technological challenges may have impacted interest and attrition. Nine participants with SCI did not have a family or peer available to participate, so we adapted our procedures and recruited participants with SCI separately from participants who are family members, friends, or peers to individuals with SCI.
The challenges we observed where some individuals with SCI were unable to find a family member or friend willing to participate may be indicative of lack of social support. Over 43% of individuals with SCI are single 1 year after injury, 1 and divorce rates are higher for individuals with SCI. 28 The addition of social support should be considered in development of technology-based interventions to increase PA levels in individuals with SCI.
Conclusions
Relationship dynamics between individuals with SCI and their peers impacts the efficacy of communication as a strategy for mitigating barriers. Social engagement and communication with peers who have similar functional mobility levels and life experiences can potentially improve motivation for PA in individuals with SCI. However, there is a lack of PA platforms tailored towards wheelchair-users.
Footnotes
Author’s note
Portions of this work have been presented at the 2022 American Congress of Rehabilitation Medicine Annual Conference, the 2022 International Spinal Cord Society Annual Scientific Meeting, and the 2022 Conference on Computer-Supported Cooperative Work and Social Computing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Disability, Independent Living, and Rehabilitation Research.