
Abstract
Introduction
Task-specific neurorehabilitation is crucial to optimize hand recovery shortly after a stroke, but intensive neurorehabilitation remains limited in resource-constrained healthcare systems. This has led to a growing interest in the use of robotic gloves as an adjunct intervention to intensify hand-specific neurorehabilitation. This study aims to develop and assess the usability of an operating interface supporting such a technology coupled with a virtual environment through a user-centered design approach.
Methods
Fourteen participants with hand hemiparesis following a stroke were invited to don the robotic glove before browsing through the operating interface and its functionalities, and perform two mobility exercises in a virtual environment. Feedback was collected for improving technology usability. Participants completed the System Usability Scale and ABILHAND questionnaires and their recommendations were gathered and prioritized in a Pugh Matrix.
Results
The System Usability Scale (SUS) score for the operating interface was excellent (M = 87.0 SD = 11.6). A total of 74 recommendations to improve the user interface, calibration process, and exercise usability were identified.
Conclusion
The application of a full cycle of user-centred design approach confirms the high level of usability of the system which is perceived by end users as acceptable and useful for intensifying neurorehabilitation.
Keywords
Introduction
Robotic technologies, such as robotic gloves, present an opportunity to practice a task-specific training regime that aligns with the principles of neuroplasticity to help functional recovery after a stroke. 1 Rehabilitation outcomes following a stroke are not only impacted by whether the individual receives task-specific training, but also by the intensity of the rehabilitation. 2 When comparing higher intensity training to normal intensity of conventional rehabilitation interventions (e.g., over 2.5 times the intensity) higher intensity training shows significantly higher activity levels in subacute and chronic stroke.3,4 The intensity of an intervention has two main components: dosage (i.e., number of repetitions), and duration (i.e., time dedicated to exercises). Although the literature seldomly dissociates these two concepts, interventions of shorter duration, and higher dosage have been shown to be more efficient. 5 Despite this evidence, limited resources within the healthcare system (such as limited staff and admission capacity of specialized stroke rehabilitation programs) hinders the ability to increase dosage. 6 As such, there exists a need to offer task-specific rehabilitation training at higher doses, without increasing the demand on the resources. Robotic gloves, in addition to being task-specific, present a promising solution to increase the intensification of sensorimotor rehabilitation by offering additional rehabilitation interventions without or with limited professional rehabilitation assistance.7,8 In order for this solution to be successful, the level of usability of these robotic gloves must be high enough to allow independent use by its end users.
Usability is a broad concept that encompasses effectiveness, efficiency, and satisfaction. The definition of usability specifies that it is context-dependent which includes the task, the user, the temporality, as well as the environment in which the system, product or service is used. 9 In other words, technological developments are ideal when driven not only by efficacy and efficiency, but also by the adequacy between the technology and the nature of its user. 10 Therefore, to optimize the potential acceptability and use of such technologies by stakeholders (e.g., occupational therapists (OTs) and people who sustained a stroke – end user), a user-centered design (UCD) approach is ideal. 11 The current study, and all the phases that preceded, applied a UCD approach to the development of a new operating interface that couples a robotic glove with a virtual environment to optimize sensorimotor hand rehabilitation of people with hemiparesis following a stroke.
The first phase of the development process, now complete, involved documenting the perceptions and expectations of OTs regarding the use of robotic gloves in clinical practice. 8 All OTs consulted favorably the use of robotic gloves as a rehabilitation adjunct that could allow them to increase hand-specific intervention intensity. Important elements and recommendations were identified from this process that helped inform the choice of robotic gloves (Dexmo, DextaRobotics, Shenzhen, China), and exercise inventory in future programs. These considerations included ease of use, cost, movement precision, durability, and safety, as well as some recommendations for the creation of the virtual reality interface. The Dexmo glove is a wireless, lightweight commercialized haptic robotic glove initially created to be coupled with a virtual reality environment. 12 It has the capability to independently mobilize each finger into full flexion and extension with 11 degrees of freedom. In addition, it is worn on the dorsal side of the hand via a single Velcro strap and rubber fingertips for each finger, freeing most of the palm of the hand to optimize sensory feedback when interacting with objects and the environment, and is easy to put on. The glove communicates wirelessly with a computer via a dongle connected in a USB-type C port.
The current study presented here, describes the outcomes of the second phase of the development process, and reports on the development of the operating interface itself. This phase has an overall goal of coupling the Dexmo robotic glove with a virtual environment to optimize hand rehabilitation of people with hemiparesis following a stroke using an iterative approach consistent with UCD.11,13,14 To do so, the objectives of this study were two-fold: (1) assess the usability of the preliminary operating interface (bTrained 1.0), its functionalities, as well as its content in terms of hand exercise inventory and (2) prioritize recommendations, through a detailed and rigorous process which considers various pragmatic aspects and usability criteria to align the development of the final interface with the needs and preferences expressed by potential end users.
Methodology
Research design, approach, and framework
A mixed-method design integrating a UCD approach based on key constructs of the Unified Theory of Acceptance and Use of Technology (UTAUT2) was used. The UCD approach recommends three main principles: (1) focusing on users and tasks throughout every step of the design process; (2) empirically measuring the usability of technology by end users; and (3) following/applying an iterative design process. 13 The UTAUT2 framework includes seven main constructs which all influence behavioral intention to use technology and/or technology use.15,16 These constructs include performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, price value and habits. Excluding price value and habits, these constructs guided data collection and analysis. The research team did not include price value as construct in the design because the cost of using this kind of technology in Quebec is not typically covered by end user. Habits was also excluded, as the proposed study was not performed over a period long enough to assess habits. The project was approved by the CRIR Research Ethics Committee (CRIR-1410-0419/multi).
Participant recruitment
A total of 14 participants were recruited from a database of persons who had experienced a stroke and who had or were attending rehabilitation in centers or hospitals offering structured neurorehabilitation programs in the province of Quebec. To be included in the present study, potential participants needed to have functional impairments to the left hand following the stroke and be able to communicate and understand French or English. Individuals who were unable to give informed consent or with impaired expressive communication skills or cognitive impairments that affected their ability to carry on a fluent conversation were excluded.
A person independent of the research team first contacted eligible candidates from the database to explore their interest in participating in the study. When an eligible candidate expressed interest in participating, a member of the research team was notified. This same member then contacted this person by telephone to offer detailed information about the study and schedule their participation. Information about the specific objectives of the participation and an electronic copy of the consent form were emailed to them.
Among the 14 participants recruited, two were approached to join our research team as patient-partners to advise the research team on usability at each stage of the design process, in line with the first principle of the UCD approach.
Data collection
As per the third principle of the UCD approach, data collection was conducted in two blocks with an equal number of distinct participants (N = 7) per block, and 2 months separating each block. After giving informed consent, each participant engaged in a face-to-face 90-to-120-min consultation conducted by a graduate student in Rehabilitation Sciences or a research intern. Participants sociodemographic was first obtained. Then each participant was invited to don the robotic glove and browse through the interface, its functionalities and perform two prototype exercises, complete three questionnaires and finally participate in an interview about their experience as end users (details below).
After the first block of seven participants, a preliminary data analysis was conducted to formulate recommendations for the continuous improvement process of the user interface, calibration process and exercise inventory for improved usability before launching the next block of data collection.
The consultation was structured as follows:
Sociodemographic (5–10 min)
Participants answered questions regarding their clinical profile (e.g., gender, age, stroke onset, dominance, most affected hand, experience with- and example of technology-based rehabilitation intervention received during rehabilitation, rehabilitation status).
ABILHAND (10–20 min)
A 23-question self-reported questionnaire assessing the perceived ability to perform daily bimanual tasks. The ABILHAND has high reliability and validity in the chronic stroke population.17–19
The Dexmo glove and operating interface and exercises in a virtual environment (software prototype bTrained 1.0) (60–90 min)
After an explanation and a demonstration, participants were invited to put on the glove by themselves with minimal verbal assistance. This task was timed without their knowledge so as not to bias their performance. The goal was to simulate a realistic rehabilitation situation for usability purposes. Thereafter, the operating interface and its functionalities, including the calibration process and two exercises were presented to the participants for them to assess the usability and the user-experience (Figure 1). The btrained 1.0 software – The home page of the prototype virtual interface software bTrained 1.0 is accessed via an icon on the computer screen. (a) At the top right, the user selects their name (username) and which hand they want to train (right or left). The calibration is automatically associated with the chosen username and only needs to be performed once. Two types of calibration are offered: pose calibration and manual joint calibration. (b) The pose calibration requires the user to recreate different hand poses shown on the images and record this position by pressing the “record” tab. (c) Manual joint calibration requires the user to position their hand in any position they want and manually adjust the position of each joint of each finger in all spatial planes (XYZ). (d) Once the calibration is done, the icon “mobility”, available on the home page, can be explored to further access to mobility exercises. The bTrained 1.0 prototype includes two mobility exercises. (e) A stationary ball grasping exercise (opening and closing the hand) with moderate glove assistance throughout the movement and (f) A rhythm pinching exercise where the user must synchronize the flexion and extension of the index finger to an auditory feedback (a beep) without any assistance from the glove.
Interview with UTAUT2 constructs
At each stage of the bTrained 1.0 platform presentation and assessment by participants (e.g., donning the glove, navigating the interface, the calibration process, etc.), closed and open-ended questions covering UTAUT2 constructs (performance expectancy, effort expectancy, facilitating condition and hedonic motivation) were asked.15,16 Some questions also addressed elements that the participants felt could be improved both regarding the interface and the exercises.
System usability scale (10 min)
At the end of the interview, participants completed a standardized questionnaire on the usability of the technology (SUS) to empirically measure the usability of technological intervention by users (second principle of the UCD approach). The SUS is a 5-point Likert scale questionnaire incorporating 10 alternative positive and negative questions with total scores ranging from 0 to 100 to assess subjective system usability.20,21 It is worth noting that the scores for individual items are not meaningful on their own and that the total score represents a composite measure of usability. Scores of over 50, 70 and 85 are respectively considered as “ok”, “good” and “excellent”.22,23 The original English version of this questionnaire was supplemented with an in-house French translation under each question.
Data analysis and statistics
Quantitative data
Sociodemographic data for all 14 participants, the ABILHAND score, timed tasks and SUS score are presented using descriptive statistics. The ABILHAND raw scores were submitted for an online analysis (http://rssandbox.iescagilly.be/abilhand-rasch-analysis-chronic-stroke.html). Items score out of 23, patient scores, measures and standard errors (logit and percent of logits for both) were extracted. The results of the timed task of putting on the glove were also analyzed using descriptive statistics. From the SUS raw score, a corrected score for every question and an overall corrected score were calculated. 24 Descriptive statistics were computed for corrected overall SUS score.
Other relevant quantitative information collected during interviews were analyzed through descriptive statistics. These included: (1) number of recommendations collected in each block of interviews, (2) number of different types of exercises and level of difficulty of exercises per type to maintain users’ engagement and motivation, and (3) estimated frequency and duration of expected use. All statistics were conducted with R studio Version 1.3.1093.
Qualitative data
The anonymized text transcription of all recorded interviews was performed and imported into QSR International’s NVivo 12 qualitative data analysis software 25 for thematic analysis. A first coding frame based on the closed and open-ended questions was created. This coding frame was supplemented following an inductive process, by the emergence of any new recommendations to improve the user experience (both regarding the Dexmo and bTrained 1.0), and this, from one interview to another. The transcripts were coded according to the key areas of the UTAUT2 and the occurrences where the interviewees mentioned various recommendations. In both blocks of interviews, data saturation was achieved after the sixth interview. To confirm data saturation, a seventh interview was conducted to assure the lack of new information.
After the first block of interviews, all recommendations were merged into a Microsoft Excel spreadsheet. To prioritize recommendations preceding the next block of interviews, a Pugh matrix was developed. Pugh matrices allow for the logical and rigorous comparison and prioritization of different recommendations based on chosen predefined criteria.26,27 The five-step Pugh Process described below was followed:
Step 1 — Identify and define criteria to be considered to prioritize recommendations and assign weights to these criteria. Specific constructs of the UTAUT2 were used as criteria in the matrix (performance expectancy, effort expectancy, facilitating condition and hedonic motivation), the popularity (frequency) of the recommendation, and the time and resources needed to implement the recommendation. Other UTAUT2 constructs such as social influence, price value and habit were excluded as they were not applicable in this context. To assign weights to UTAUT2 criteria, the results from the direct effect of the structural model, which predicts consumers behavioral intentions and use of technology, were used. 16 The weights for the popularity, time and resources criteria were determined arbitrarily by the expertise of the clinical research team and the engineer team. From one iteration to another, the weight of the time and resources criterion was modified to account for the differences in time frames to implement the recommendations (2 versus 6-months).
Steps 2 and 3 — Use a baseline to compare new recommendations. Compare each recommendation against the baseline for all criteria. In this study, the baseline was the prototype, as it was presented during the consultation. To assess the pairwise score of each recommendation with the baseline, a 5-level Likert scale (2, 1, 0, −1, −2) was used for all criteria except time and resources (0, −1, −2, −3 for the first block and 0, −0.5, −1, −1.5, −2, −2.5, −3 for the second block) for the same reasons as mentioned above. A score of 0 was given to a recommendation of having no more, no less impact on the criteria compared to the baseline prototype.
Steps 4 and 5 — Calculate total score for each recommendation considering all criteria and their weights. Check your ranking and use judgment in interpreting it. In the context of this study, the execution of one recommendation sometimes facilitates the execution of another, which led to prioritizing a recommendation that would not have been best rated initially.
Step 6 — Make a decision and justify the reasons behind those decisions. To help clarify the results, we used a color system to categorize the different recommendations under three priority levels based on their rank: green (score of 0.7 and over), orange (score of over 0.5 and less than 0.7), and yellow (score of over 0.3 and less than 0.5) (Figure 2). Recommendations with a score lower than 0.3 were discarded as their relevance was deemed to be of limited priority in the present study or did not require further discussion with patient-partners. An excerpt from the first Pugh Matrix which shows each of the targeted criteria, their assigned weights as well as the final scores with the ranking.
Results
Participant’s sociodemographic results
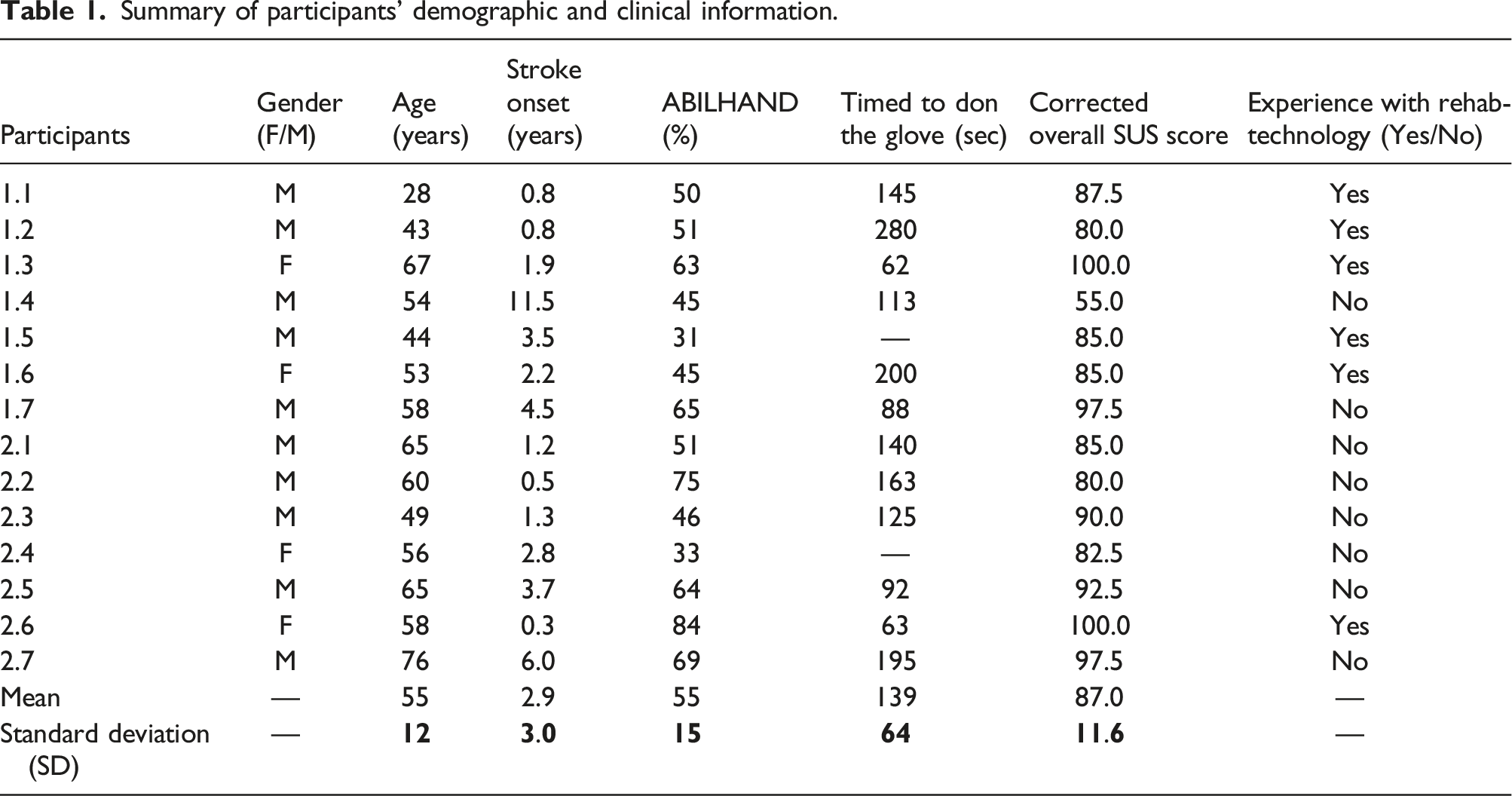
Summary of participants’ demographic and clinical information.
Specific objective 1: general usability of the current prototype
The general usability of the prototype throughout the two blocks of consultations was addressed during the interviews by addressing five of the seven constructs that influence intention to use and use behavior of technology from UTAUT2. These five constructs included: (1) performance expectancy, (2) effort expectancy, (3) social influence, (4) facilitating conditions and (5) hedonic motivation. Participants were also invited to share their solutions/recommendations to improve usability. Below is an overview of the combined findings from both blocks of consultations, that may impact participants’ user experience with this technology.
Performance expectancy
All participants (N = 14) thought that this technology would or would have benefited them during their rehabilitation. It was considered as a great rehabilitation adjunct to improve mobility and strength, as the users felt that the gloves could intensify the dosage of specific hand movements performed per day. Moreover, one participant found that using the glove helped reduce their fatigue compared to performing similar exercises without it, allowing it to be used for a longer period (P13). The glove was also seen as a relevant alternative for people with very little motor control in their hands. This was due to the ability of the glove to allow the individual to be more autonomous in their rehabilitation by providing a way to open and close the hand without the help of a therapist: “To become more independent. Because [my therapist] was the one moving my fingers. I couldn't open my hand alone with my left hand, he had to move my fingers so with [this technology] I wouldn't need help!” (free translation P6)
Effort expectancy
Effort expectancy, defined as the ease of use of the technology, was discussed with the participants for each of the stage of use (donning the glove, calibration, navigation, exercises’ instructions, and exercises’ parameters). With the addition and help of some facilitating conditions (see Facilitating Conditions), as well as the execution of certain recommendations such as the creation of an automatic countdown timer during calibration, and/or the help of a family member, when necessary, all participants (N = 14) could imagine using this technology independently at every stage of use without direct help from a therapist. This was true even for participants who reported having very little experience with everyday technologies such as computers and smartphones: “Well, for me, there’s nothing difficult [in using this technology]. However, I’d have more difficulties in using the computer since I'm not used to computers. But [my life partner] could help me if needed.” (free translation P8)
For the calibration, the manual joint calibration method was certainly more difficult and less intuitive for nearly all participants (N = 13), although participants all recognized its relevance for accuracy.
Social influence
All participants (N = 14) agreed that their caregivers, family members, friends and perhaps even their therapist would like or would have liked to see them access and use such technology in rehabilitation.
Facilitating conditions
The participants believed that the research team could improve and better support the independent use of this technology by the users. Most participants agreed that it would be necessary to have a training session similar to the one offered during the consultation. A detailed user guide would also be appreciated by the end users.
Moreover, a minimal therapeutic supervision session with a qualified therapist would be expected by the participants. This support could take the form of a telerehabilitation session once a week or via a dual patient-therapist interface. This dual interface would allow the therapist to access the performance of the user and to pre-select the exercises they wished the individual to perform according to their clinical judgement.
Although the rubber fingertips of the robotic glove were easy to put on, they occasionally slipped off while performing the exercises and caused user dissatisfaction. In addition, the choice of fingertip sizes was not exhaustive, which limited the comfort for some. Longer fingertips with a greater selection of sizes would be helpful. As for facilitating navigation and increased intuitiveness, a touch screen would be preferred by all participants: “It would be nice to have a touch screen for people accustomed to tablets and smartphones!” (free translation P1)
Some participants with little motor control of the hand and forearm mentioned that access to stabilization aids for the hand or forearm would help when putting on the glove.
Hedonic motivation
When asked what increased their motivation and engagement to use this technology, seven participants said that just seeing their hand move and/or having access to that technology at home would be appreciated: “To have it at home would be enough to increase my motivation in using it” (free translation P14)
To maintain long-term motivation to use this technology, different recommendations related to the addition of encouragement and performance indicators (e.g. point system, score, different levels of difficulty), as well as adding realism and playfulness (e.g., gamification) through the exercises were mentioned by participants.
Specific objective 2: prioritization of recommendations to improve the prototype
First interview block
A Pugh matrix was conceptualized from the first block of interviews, listing all 74 recommendations collected from the participants and grouped into seven major categories: creation of user personalized account (13 recommendations), sequence of gaming (3), user learning framework (7), glove (11), user physical support (4), basic interface (6) and games (30). Of these 74 recommendations, six were not retained because they were impossible to implement based on the model of the glove used. Two additional recommendations were deferred to the subsequent Pugh matrix for a later stage of development: the creation of a user’s guide and the classification of exercises by level of difficulty. It is expected that they will evolve further as the development process continues based on future recommendations.
Of the 66 remaining recommendations, six achieved scores above 0.7 (i.e., high priority) and were implemented prior to the second block of interviews. The highest priority score was for the development of a new process to create custom user accounts to incorporate user-specific options such as hand appearance, injured hand choice, and language choice.
Numerous other improvements had been made ahead of the second block of consultations. For instance, the calibration process was integrated as a step in this new customized user account creation process. Also, in the first block of consultations, during calibration process, not all participants were able to imitate the requested hand positions with their affected hand. Some participants had to use their non-affected hand to assist, making it impossible to simultaneously use the cursor to record the position. To free the user’s unaffected hand from the cursor and aid in the execution of the requested calibration positions in the second block of consultations, an automatic countdown timer with delay and an automatic save button were added. In the game instructions, videos demonstrating the movement to be performed were also integrated.
Additionally, alternative parameters to modulate the difficulty of the ball grasping exercises were also incorporated before the second block of consultations. For example, difficulty could be adjusted by modifying the size of the ball, the number of repetitions and the level of assistance by the glove during flexion and extension movements. As for the rhythmic exercises of index finger flexion, an editable parameter of the rhythmic frequency was included. For both mobility exercises, two different levels of difficulty were developed with the option to modulate them using the parameters named above. This addition made it possible for participants to gradually adopt a hybrid mode of managing the levels of exercise difficulty. Indeed, one of the recurring recommendations from participants was to develop a hybrid mode of managing the exercise levels of difficulty. It was suggested that when participants click an icon to start an exercise program, a pre-established order of exercise difficulties would appear, alongside the option of manually modifying the parameters to adjust the difficulty of the exercises (Figure 3). Navigation through the improved btrained 1.0 software interface. In green are the new features added from the first Pugh Matrix.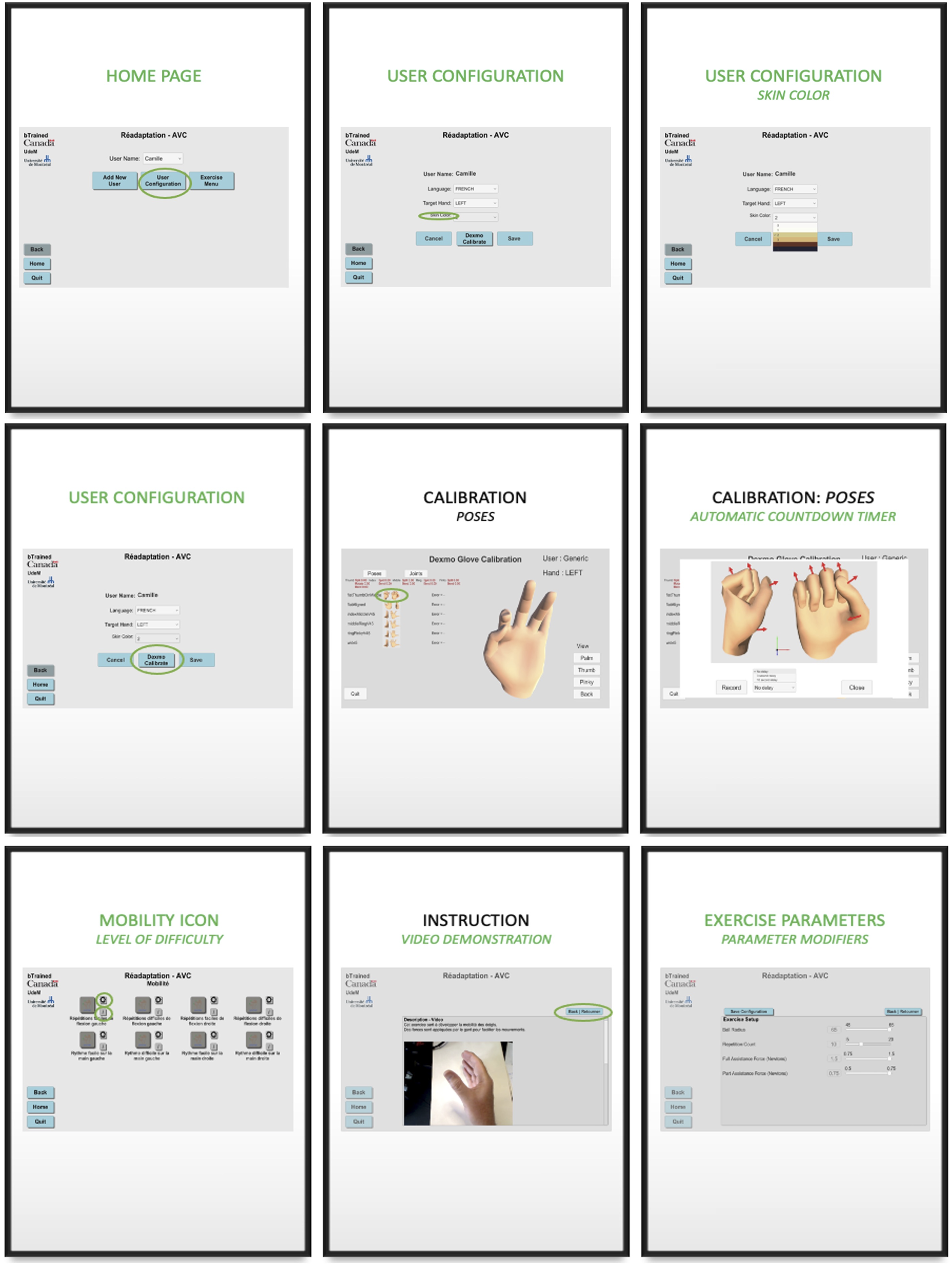
Other recommendations that required more resources and time were noted for future development but were not addressed in preparation for the second block of consultations. Such recommendations included adding other fingers to the exercises and the addition of a visual cue to coordinate the movement.
Second interview block
A second Pugh matrix was created listing all 45 recommendations, including two recommendations carried over from the first Pugh matrix and intended for a later stage of development (user guide and exercise-level display), as well as one previous recommendation (the development of new parameters for the rhythm exercise). The recommendation to develop new parameters for the rhythm exercise was further refined and broken down into five separate recommendations since each parameter requirements differ in terms of time and resources, bringing the list of recommendations to a total of 49. These were again grouped into the seven major categories previously created after the first block of interviews: creation of user personalized account (10 recommendations), sequence of gaming (1), user learning framework (3), glove (3), user physical support (2), basic interface (5) and games (25). One recommendation (move real objects) was not retained because it did not fit with the objective of the glove and exercise program. Of the 48 remaining recommendations, only eight differed from the first block of interviews. Four of these recommendations were associated specifically with the updated version of the bTrained 1.0 software following block one’s recommendations (e.g., have a greater delay selection for the automatic countdown timer, choice between opaque or translucent hand appearance, adding videos of other views in the game instructions, and more intuitive visualization of parameter modifier).
When combining the matrices of the first and second blocks together and withdrawing recommendations already implemented following the first block, a final Pugh matrix of 74 remaining recommendations was obtained. While all recommendations are considered implementable within the next year, the previously used prioritization scoring system was reapplied, allowing for an enriched decision-making process for prioritizing recommendations.
Lastly, additional relevant quantitative information was collected as part of the development process. Participants reported that an average of over six types of exercises and over four levels of difficulty per type of exercises would be sufficient to maintain their engagement and motivation. Also, with the addition of this amount of exercise type and level, participants envisioned themselves using the glove at an average frequency of 5-to-6 days a week during a 60-min period.
Discussion
The main purpose of this study was to report on an iterative development approach consistent with UCD which could provide guidance for future research and robotic-assisted technologies in rehabilitation of people with hemiparesis following a stroke. Development processes ought to be initiated with the aim of meeting specific needs which often emerge from the end users. Usability evaluation as a central component of the development process must occur at every phase of development through an iterative design as specified by the UCD approach. Indeed, there must be a cycle of design in which user testing is followed by redesign and repeated as often as necessary. 13 The current study illustrates one full cycle of development, with additional cycles to be added in future research to support the continuous improvement process.
Usability challenges encountered in the current development of rehabilitation technologies
Schulz et al. (2015) proposed an explanatory model of development and evaluation process of technology which distinguishes evaluation and measurement strategies used in the early or later stage of development. The early-stage evaluations focus on effectiveness, efficiency, ease of use, acceptability, user satisfaction, safety, aesthetics, and other parameters, through observation and simulations of the use of technology, scenario tests, interviews, and focus-groups. Later-stage evaluations focus on targeting adoption, performance in real tasks, impact on quality of life, and impact on caregivers through clinical trials. 30 The literature notes that the evaluation of the usability of rehabilitation technologies even in the early-stage is mostly associated with a study whose main objective is to evaluate the efficacy of treatment.28,30,31 Thus, most outcome measures essentially target the treatment and are based on the evaluation of its effect (“intervention-related outcome measures”). 32 Outcome measures related specifically to usability are primarily aimed at assessing the accuracy, sensitivity, and reliability of technology, as well as the feasibility and patient satisfaction with the treatment.31,33 One study that explored the main usability assessment tools for telerehabilitation and virtual reality showed that SUS was the most widely used questionnaire (N = 12), compared to User Satisfaction Evaluation Questionnaire (USEQ) (N = 2) and the Gameplay Experience Questionnaire (GEQ) (N = 2) which were both created specifically for this purpose. 34 Therefore, even when the use of general tools complies with the first principle of the UCD approach, it does not always match adequately with the specific context in which the technology is used. 35
It is possible that some questionnaire items may not apply to the targeted technology, while other items may have greater contextual relevance, hence the importance of developing evaluation tools specific to the technology being developed and its context of use. 36 However, the creation of evaluation tools can be a tedious and expensive process, which can discourage many, and which may explain the abundance of general usability evaluation tools. Thus, these general tools require to be combined with other means of evaluation. This explains why Schulz et al. (2015) suggest usability evaluations following a qualitative methodology, similar to the one presented here, as a simple solution specific to the evaluated technology and its context of use that adequately complements general tools. However, the literature documents little on the process of information collected by these qualitative methods, such as prioritization of needs and recommendations by users.
Where engineering meets rehabilitation
In the field of technology development and engineering, several prioritization techniques are widely used for the creation of software, such as Numerical Assignment, Planning Game and the Hundred Dollar Method. 37 However, these methods mainly consider the technical aspects of the technology development, often ignoring the clinical aspects, despite being essential considerations for the development process of a technological rehabilitation intervention. Other methods, such as the TRIAGE method, 38 predominantly take into account the clinical aspects, but ignore technical aspects, which may have undesirable consequences. In the current study, the Pugh matrix was chosen to consider each of these aspects and have the flexibility to weight each one as needed. This matrix is similar to the Planning Game technique, but with the ability to integrate clinical criteria. In the present study, this clinically-integrated matrix emerged from the UTAUT2 framework, and proved an ideal matrix to list, classify and prioritize recommendations. To the knowledge of the authors, this study is the first to use this method in a rehabilitation context.
Usability of the current prototype and prioritization of recommendations
The sub-objectives of this study were to: (1) assess the usability of the current prototype of a hand exercise program with the Dexmo in a virtual reality interface by people who have sustained a stroke, and (2) prioritize recommendations to optimize the prototype to better meet the needs of those people and allow them to perform the intervention on their own.
Overall, the Dexmo glove and the interface developed for its use were well appreciated by all participants who also reported a high intention to use it independently as a means to intensify sensorimotor hand rehabilitation. Quantitative and qualitative results revealed that such technology has good to excellent levels of usability from the perspective of a heterogeneous sample of individuals with hand hemiparesis following a stroke according to the ABILHAND score, and who had varying levels of experience with rehabilitation technologies. The majority of participants (12/14) were able to don and doff the robotic glove independently in less than 5 min after receiving only a few verbal cues. The time requirement aligns perfectly with the expectations of OTs who recommend that no more than 10 min should be dedicated to this step to maximize therapy time. 8
In addition, the evolution of the different Pugh matrices indicates that the number of recommendations was reduced by 18 during the second block in comparison to the first block, but remained similarly distributed across the seven major categories. Several hypotheses could explain this observation. Changes implemented prior to the second block may have made the user experience more enjoyable, thus reducing the propensity to express other recommendations. Alternatively, it may be that the second group presented a higher level of baseline performance, thereby facilitating the use of the Dexmo and its interface, and reducing the number of recommendations. The data from the Pugh matrices also indicates that the execution of the recommendations prior to the second block leads to the emergence of new recommendations related to these changes. This phenomenon highlights the importance of continuously involving end users at all stages of technological development. Adopting a patient-as-partner approach embodies the ideal of making the end user a bona fide team member early in the research project and aligns with currently emerging research practices.
Conclusion
This study reported the iterative development process of an interface to couple the Dexmo robotic glove with a virtual environment to optimize hand rehabilitation of people with hemiparesis following a stroke. The prototype had a high level of usability by its end users, although several recommendations were made to further improve its usability in future iterations. These recommendations align with the intention of using the technology with or without limited professional rehabilitation assistance. The execution of these recommendations and the continuation of iteration cycles with participation from patient-partners will be of great relevance in preparing for future feasibility and efficacy studies. The acceptability of technology, largely influenced by its usability, is a key determinant for rehabilitation intensification which, in the end, is the ultimate goal.
Footnotes
Acknowledgements
The authors acknowledge the Clinical research coordinators of the stroke programs at the IURDPM and Villa Medica Rehabilitation Centers, respectively Perrine Ferré and Frédéric Messier. The authors thank Manouchka T. Louis Jean and Jasmine Lemire for assistance with data collection and analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by the Initiative for the Development of New Technologies and Innovative Practices in Rehabilitation (INSPIRE) and AGE-WELL NCE Inc., a member of the Networks of Centres of Excellence program. CP holds a scholarship from INSPIRE, AGE-WELL NCE Inc., the School of Rehabilitation (Bourse de Mérite de la Faculté de médecine de l’Université de Montréal) and from the Canadian Institutes of Health Research (CIHR; # 477076), and DG hold senior research salary award from the Fonds de la recherche du Québec – Santé (FRQS; #268982) and co-chairs the INSPIRE funded by the LRH Foundation.