
Abstract
Introduction
A large proportion of a wheelchair user’s body is in contact with their wheelchair. Integrated fan cooling systems fitted to a wheelchair’s backrest aim to alleviate the build-up of heat at the skin-chair interface. The aim of this pilot study was to evaluate the effectiveness of an integrated fan cooling system at cooling the user during daily pushing activity.
Methods
Eight male able-bodied participants completed two conditions, with (FAN) and without (CON) fan cooling, pushing for four 15 min blocks. The fan was turned on (highest setting) at the end of block 1 (FAN), whilst in CON the fan remained off. Skin temperature was measured over the back and chest throughout alongside heart rate and perceptual responses (rating of perceived exertion, thermal sensation, thermal comfort, wetness sensation) at the end of each 15 min block.
Results
Wetness sensation and lower back skin temperature were lower in FAN (both p < 0.02), with the difference in lower back skin temperature between the two conditions being 2.20°C at the end of block 4.
Conclusion
The integrated fan cooling system provided significant cooling to the lower back without affecting any other physiological or perceptual response, besides wetness sensation.
Introduction
There are currently around 1.2 million wheelchair users in the UK. 1 Manual wheelchair users often spend large portions of their day seated in their wheelchair, reported to be on average 9.6 h for individuals with a spinal cord injury. 2 During this period, a large proportion of their body surface area is in contact with the wheelchair. For those wheelchair users who require a large amount of support with a custom fitted seating system, a large skin surface area will be encapsulated; with the majority of the torso, buttocks and upper portion of their legs being in contact with the supporting surface. Heat and moisture will likely increase at the skin surface interface, leading to an increase in skin temperature2,3 because of inadequate air flow around the body. Previous literature has indicated that an increase in skin temperature of 1°C causes a 10% increase in tissue metabolism, 4 increasing the wheelchair user’s susceptibility to health complications, such as pressure ulcers. Hence if a wheelchair user can prevent an increase in their skin temperature whilst seated in their chair, they may reduce their risk of skin injury.
Further complications may occur for manual wheelchair users whose sweating ability is affected because of their disability. For instance, individuals with a spinal cord injury, in particular those with complete lesions, are unable to sweat below their lesion level.5–7 Consequently, the higher their lesion level, the smaller the body surface area from which they can sweat, severely affecting their ability to dissipate heat. Individuals with multiple sclerosis and cerebral palsy may also have a reduced sweating ability8,9 and further implications for other wheelchair users may be caused by their daily medication. In contrast, wheelchair users who can thermoregulate effectively, may experience sweat soaked clothing and discomfort whilst in their wheelchair due to a lack of air flow between the skin and wheelchair interface, reducing their overall evaporative capability and thermal comfort. Varying degrees of functionality and mobility, even within impairment groups, will likely impact both the amount of time individuals spend in their wheelchair and their ability to dissipate heat from the skin surface. Therefore, a range of manual wheelchair users are likely to benefit from cooling methods that assist in dissipating heat from the body whilst in their wheelchairs.
Anecdotally, typical cooling strategies used by wheelchair users during daily activity include the use of handheld fans and cold/wet towel compresses. Given the long periods of time spent in their wheelchairs and the potential for further heat related complications from their disability, these techniques may not be easy to implement. Warm and/or humid environmental conditions will only further exacerbate the issue. Therefore, wheelchair users require a much more accessible means to provide sufficient cooling during prolonged daily activity for both health and quality of life purposes.
An integrated, but discrete cooling system aims to provide cooling for wheelchair users using a fan-based system in the backrest (WheelAir® slingback, WheelAir, Glasgow, UK). The product consists of a canvas backrest that replaces the wheelchair user’s standard backrest and houses an integrated fan cooling system. A fan box is located at the bottom of the backrest and channels direct air up into the backrest, stated to provide cooling to the user’s back. The original version (version 1) enables the user to choose from four fan settings to control the amount of cooling provided. Aside from case study work by the manufacturer, 10 the extent of the cooling provided to the user has not been determined and verified.
The aim of this pilot study was to evaluate the effectiveness of the integrated fan cooling system at cooling the user during daily wheelchair pushing activity. It was hypothesised that the integrated fan cooling system would reduce skin temperature at the lower back, where the user is in contact with the increased air flow due to the fan and improve thermal perceptions (thermal comfort, thermal sensation and wetness sensation). However, it was hypothesised that the cooler skin temperature would only be present at the lower back, due to this area being covered by the integrated fan cooling system and skin temperature would not decrease at the mid back or upper back (scapula).
Method
Participants
Eight male physically active (≥150 min of physical activity per week) able-bodied participants (25.4 ± 6.8 years, 81.6 ± 5.3 kg) volunteered to participate in this study. To determine whether the integrated fan cooling system provided a sufficient cooling stimulus to even cool the skin of users without a thermoregulatory impairment, able-bodied individuals were recruited for this initial study of the product. This enabled a distinct group to be tested and removed the potential disparity that a mixed group of wheelchair users with varying disabilities and thermoregulatory function might have had.
Participants provided written informed consent, in accordance with the Declaration of Helsinki, and completed a health screening questionnaire prior to participation. All participants completed both conditions, separated by a minimum of 24 h. Conditions were completed in a counter balanced design. Ethics was granted by Nottingham Trent University’s human ethics committee (Application No: 605).
Experimental Procedure
All testing was conducted in a sports hall (24.1 ±1.7°C, 54.1 ± 6.6% relative humidity). Upon arrival to the testing session, participants were weighed and then fitted with a heart rate monitor (HR, Polar M430, Kempele Finland). Eight iButtons (DS1922L-F5, Maxim Integrated Products, Inc, Sunnyvale, CA, USA) were secured to the left and right of the participant’s skin located at the chest, scapula, mid back, and lower back using 3M Medipore tape (Figure 1). Only the lower back iButtons were covered by the WheelAir® slingback. These locations were chosen to provide a representation of the whole of the back, in addition to the chest. Location of the eight iButtons depicted by black circles.
Ambient temperature, humidity, and wet bulb globe temperature (WBGT) (Kestrel 5400, Kestrel, Boothwyn, USA) were recorded at the start of testing and throughout the experiment. These ambient measurements were taken next to the stool where the infrared images were taken. Participants were then asked to sit in a wheelchair throughout the two conditions (Top end Transformer All Sport, Invacare Ltd, Bridgend), except for when the infrared images were taken. Before starting the protocol, participants transferred to a backless stool and infrared thermal images were taken of the backrest, as well as the participant’s chest and back unclothed. Following which, heart rate was taken along with measures of thermal comfort, thermal sensation and wetness sensation. These measures, including the infrared images, were classed as being taken in the rest period. The thermal sensation scale comprised of categories ranging from −10 (“extremely cold”) to +10 (“extremely hot”) in increments of 1. 11 The thermal comfort scale ranged from 1 (“comfortable”) to 4 (“very uncomfortable”) in increments of 1. 12 The wetness sensation scale ranged from 0 (“dry”) to 6 (“dripping wet”) in increments of 1 (modified scale from 13 ).
To standardise the speed at which the participants pushed around the sports hall, participants were asked to push at a rate akin to normal daily activity. Participants were able-bodied and were not used to pushing a wheelchair, therefore, prior to the start of each condition, participants were asked to push the wheelchair around a lap of the sports hall (total distance per lap = 85 m) three times at a rate akin to their normal walking speed (warm-up). Timing gates (Brower TCi-System, Brower Timing Systems, Draper, USA) were used to record the time taken to complete each lap. These three laps enabled the participants to determine a set pace for both conditions. Each lap completed by the participant was recorded in both conditions to ensure consistency throughout a condition and between conditions. If the time to complete a lap deviated from their set pace participants were asked to adjust their push rate accordingly .
A WheelAir® slingback (Figure 2) was fitted to the wheelchair (WheelAir®, Version 1, Staels Design Ltd, Glasgow) for both conditions but was only switched on for the fan condition (FAN). The WheelAir® slingback is a commercially available product designed to replace an existing back support of a wheelchair and aims to improve user comfort by reducing skin temperature by channelling inducted air over the user’s back using a fan box. The version one of the product has four fan settings controlled by a remote attached to the mounted fans. In this study the highest fan setting was used in the FAN condition to investigate the two extremes of no fan (CON) and fan (FAN). The air flow of the highest setting of the slingback, measured by WheelAir®, was measured as 5.60 m/s directly above the fan inlet on the fan box using an anemometer (Testo 405i anemometer, Testo Ltd, Alton, UK). Integrated fan cooling system (WheelAir® slingback) fitted to daily wheelchair.
Participants wore the same clothing and were tested at the same time of day for both conditions. Participants were asked to push around a lap of the sports hall (same lap as the warm-up) at the pace set in the warm-up for 15 min. The participants were asked to change direction every 5 min. Lap times were recorded using timing gates. At the end of 15 min (B1, Figure 3), participants were given a 5 min rest period (R1, Figure 3) during which the following measures were taken in the following order; infrared images, HR, rating of perceived exertion (RPE, 6-20 scale), thermal sensation, thermal comfort and wetness sensation. At the end of the 5 min rest period, participants were asked to push for another 15 min (B2) and repeat the measurements taken in the 5 min rest period (R2). Measurements were recorded in the same order each time. Four blocks of 15 min pushing were completed in total. At the end of the fourth block (B4), the final measurements were recorded, and the participant was weighed again. Participants were allowed to drink ad libitum during the rest periods and the volume of fluid was recorded. Summary of testing protocol depicting both the control (CON) and fan (FAN) conditions. Each block of wheelchair pushing (B1-B4) was 15 min, whilst the rest periods were 5 min (R1-R4). B1 = end of block 1, B2 = end of block 2, B3 = end of block 3, B4 = end of block 4, R1 = rest 1, R2 = rest 2, R3 = rest 3, R4 = rest 4, RPE = rating of perceived exertion, TC = thermal comfort, TS = thermal sensation, WS = wetness sensation.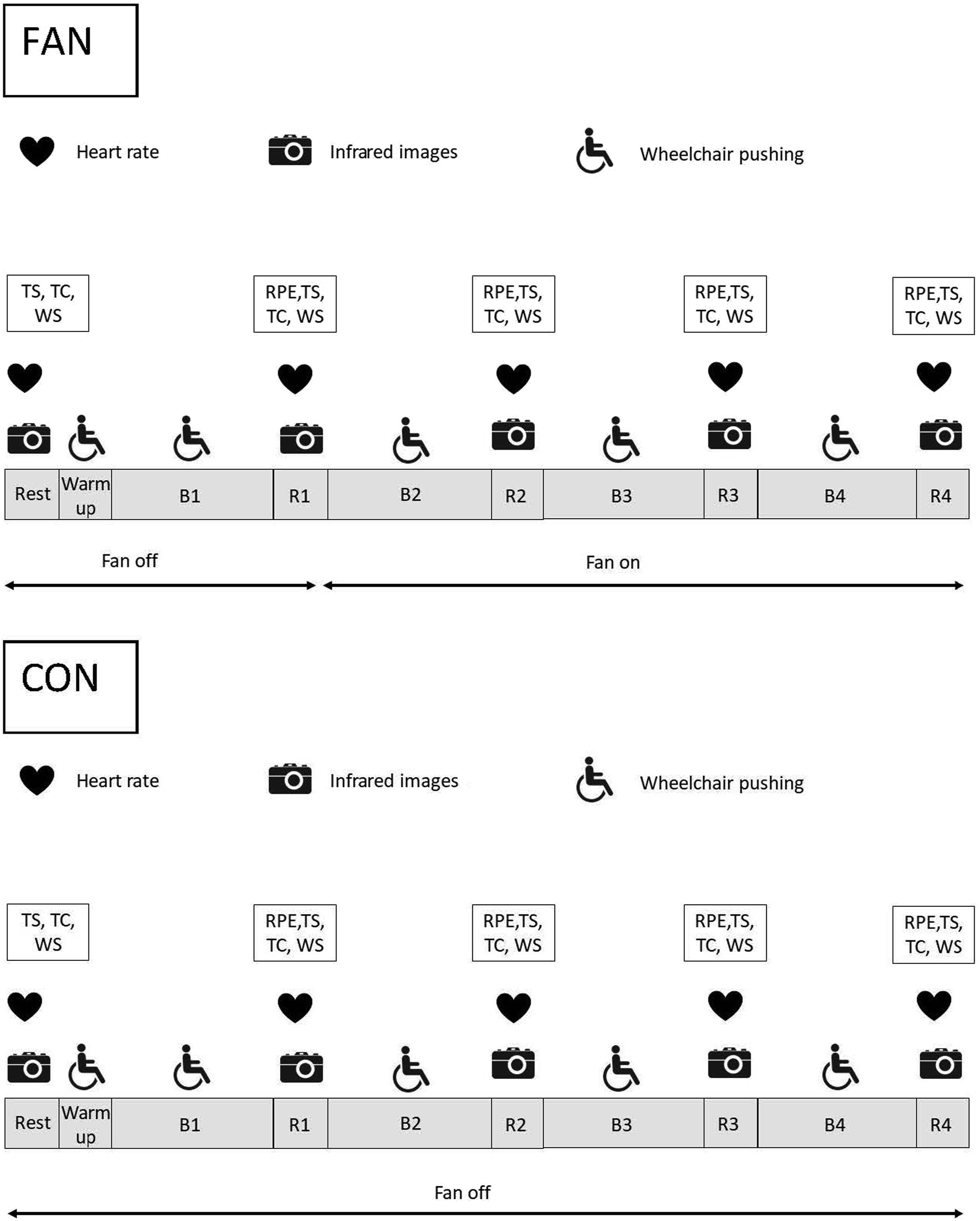
In both conditions the fan was switched off in B1. In the FAN condition, the fan was switched to its highest setting at the start of B2, whilst in CON the fan was not switched on at all. Participants were not informed of the condition they were completing. The fan is low-noise such that the participants could not hear when the fans were switched on. At the start of B2, researchers went around the back of the participant’s wheelchair to either switch on the fan (FAN) or pretend to switch on the fan (CON) such that the participant was unaware which condition they were undertaking. Participants were not informed whether different fan settings were being tested or no fan versus fan.
Infrared images
A FLIR E75 (FLIR Systems Inc. Wilsonville, USA) infrared camera with 17 mm lens was used to capture the infrared images. The camera has a 640 × 480 pixel infrared resolution with a spectral range of 7.5–14 μm. Emissivity was set at 0.95 and the accuracy of the camera is ±2°C. The camera has a very high thermal sensitivity of <40 mK allowing for detection of very small spatial and temporal changes in the temperature of the object in the image. The relative measurements required had sufficient accuracy for the present application, due to the high stability combined with the high sensitivity of the camera. In accordance with guidelines, 14 the camera was switched on prior to measurement to allow for stabilisation.
Participants transferred to a backless stool for the infrared images to be taken, which was positioned 3 m from the camera. Infrared images of the wheelchair in isolation were also taken 3 m from the camera. The images were taken away from any air conditioning units. Thermograms were always taken in the following order; 1) participant’s chest unclothed, 2) participant’s back unclothed, 3) backrest. Infrared images were taken 5 times during each condition, with three images taken each time. A total of 15 images were taken per condition per participant (30 images per participant for both conditions).
Analysis of infrared images
Extraction of temperature from the images was performed using a Graphical User Interface (GUI) in MATLAB (R2019a, The MathWorks, Natick, Massachusetts, USA). For all images, background colour was removed by converting the images to a greyscale image and applying an intensity threshold which was set by the user and using a two-dimensional median filter (size 5-by-5) to remove any remaining artefacts. The contour of the wheelchair and participant was then derived using an edge detection algorithm based on a Canny 15 filter.
From this contour image, reference points were automatically detected using an iterative algorithm designed specifically for wheelchair-only or wheelchair-and-participant images. For wheelchair-and-participant images, the algorithm first identified top (head), bottom (legs), left (left hand) and right extremities (right hand) of the contour. Location of the shoulder and neck were detected by determining extremes in the slope (derivative) of the contour between the side and top extremities. For wheelchair images, the left top and bottom of the wheelchair were identified as the maximum and minimum pixel row in the left side of the image. A similar algorithm was used to detect the right top and bottom from the right side of the image. Points were plotted on the original image for verification by the user. The user could also manually adapt the location of the reference points via the GUI when required. After this, the image was then aligned with its reference image using a piecewise linear transformation 16 to allow identification of regions of interest according to those manually obtained from the reference image. Regions of interest included the wheelchair for wheelchair-only images and upper torso and lower torso (covered during the condition by the slingback) for the wheelchair-and-participant images. After verification of appropriate alignment of the regions of interest, their temperatures were calculated by taking the mean intensity values and comparing these with the temperature range of the image.
Statistical analysis
Mean and standard deviation (mean ± SD) for the change in chest, scapula, mid back and lower back skin temperature measured using the iButtons and the change in backrest, upper back and lower back skin temperature measured using infrared images, at the end of each block for each condition (CON and FAN). The change in skin temperatures were calculated as the change from the measurements taken at rest.

B1 = end of block 1, B2 = end of block 2, B3 = end of block 3, B4 = end of block 4, CON = control condition, FAN = fan condition. * = significant difference between conditions (p < 0.05).

Difference in lower back skin temperature between control and fan conditions. The difference in lower back skin temperature was calculated by subtracting the absolute lower back skin temperature measured in FAN from the lower back skin temperature measured in CON. The black dots represent the individual data points. B = refers to block number of protocol. * = significantly different to rest, # = significantly different to end of block 1.
All data were analysed using the Statistical Package for Social Sciences (version 19, SPSS Chicago, IL) and presented as mean ± SD. Distribution and normality of data were assessed using the Shapiro–Wilk test. Main effects (condition and time) were accepted as statistically significant when p ≤ 0.05. In addition to the main effects of condition and time, to ensure standardisation between conditions, comparisons are made between conditions at rest and at the end of block one before the fan was turned on in FAN. Hence, all outcome variables should have been the same between rest and the end of block 1. Unless specified, all measurements were analysed using a repeated measures (condition x time) analysis of variance (ANOVA). Where significance was obtained for time, post-hoc pairwise comparisons with a Bonferroni correction were used. Where assumptions of normality were not met, specifically for the analysis of thermal comfort and wetness sensation, Wilcoxon signed ranks test (non-parametric) were used. A paired samples t-test was used to determine differences in fluid balance between the conditions. Effect sizes were estimated using Cohen 17 ’s d, where 0.2 represented a small effect size, 0.5 a medium effect size and 0.8 a large effect size . Effect sizes were used to determine the magnitude of the effect between conditions for lower back skin temperature measured using the iButtons and infrared images.
Results
Lap time
Participants maintained the same average lap time between conditions (67.23 ± 2.44 s and 67.26 ± 2.17 for CON and FAN, respectively, p = 0.96) and over time (p = 0.08). There was no condition order effect for lap time (p > 0.66).
Environmental conditions
Ambient temperature (24.9 ± 2.0°C vs 23.4 ± 1.8°C for CON and FAN, respectively, p = 0.06) and relative humidity (52.7 ± 5.8% vs 55.4 ± 9.1% for CON and FAN, respectively, p = 0.36) were similar between conditions. Ambient temperature significantly increased (23.5 ± 1.9°C at rest and 24.6 ± 2.2°C at B4, p < 0.001) and relative humidity significantly decreased (56.4 ± 8.5% at rest and 52.4 ± 7.4% at B4, p < 0.001) over time.
Fluid balance
Total body mass loss was not significantly different between conditions (0.69 ± 0.41 kg and 0.52 ± 0.38 kg for CON and FAN, respectively, p = 0.38). Participants drank a minimal amount of fluid for both conditions (0.05 ± 0.08 mL and 0.05 ± 0.09 mL for CON and FAN, respectively, p = 0.98).
Heart rate
Mean and standard deviation (mean ± SD) for heart rate and perceptual responses at rest (except for rating of perceived exertion) and the end of each block for each condition.
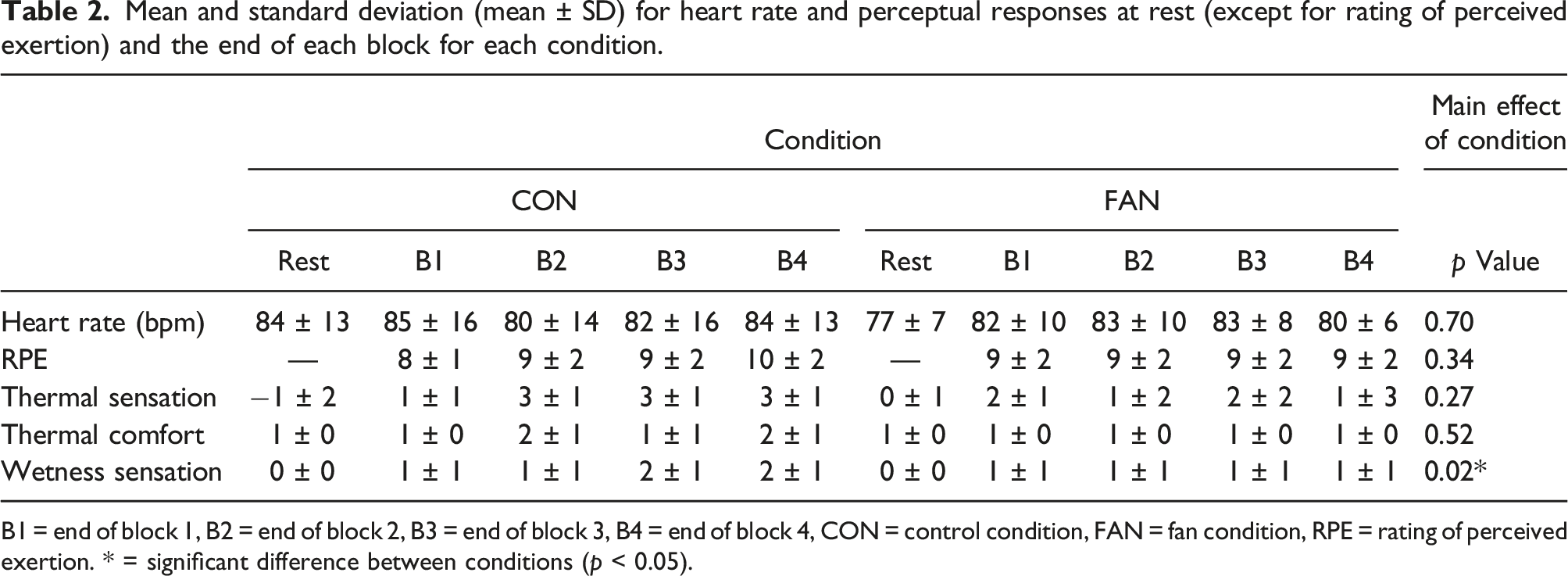
B1 = end of block 1, B2 = end of block 2, B3 = end of block 3, B4 = end of block 4, CON = control condition, FAN = fan condition, RPE = rating of perceived exertion. * = significant difference between conditions (p < 0.05).
Skin temperatures
Table 1 shows the change in chest, scapula, mid back and lower back skin temperatures measured using the iButtons at the end of each block for each condition. All skin temperatures were not significantly different at rest (all p > 0.14) or at the end of B1 (all p > 0.07) between conditions. Only the change in lower back skin temperature was significantly different between conditions being significantly smaller in FAN than CON (p = 0.01, d = 1.47, Table 1). There was no order effect for lower back skin temperature (p > 0.30). The difference between the two conditions at rest and at the end of each block for lower back skin temperature is shown in Figure 4.
Infrared images
Table 1 shows the change in backrest, upper and lower back skin temperatures measured using the infrared images at the end of each block for each condition. The temperature of the backrest was similar between conditions at rest (27.63 ± 2.17 and 28.38 ± 1.71°C for CON and FAN, p = 0.49) and at the end of B1 (31.81 ± 0.49 and 31.73 ± 0.69°C for CON and FAN, respectively, p = 0.71). There was a main effect for condition for change in temperature of the backrest, being smaller in FAN than CON (p < 0.001, Table 1).
Upper back skin temperature was similar at rest (32.90 ± 0.59°C and 32.87 ± 0.25°C for CON and FAN, respectively, p = 0.86) and at the end of B1 (32.89 ± 0.57°C and 32.58 ± 0.27°C for CON and FAN, respectively, p = 0.07) between conditions. Lower back skin temperature was similar at rest (31.74 ± 0.61°C and 31.21 ± 0.57°C for CON and FAN, respectively, p = 0.06) and at the end of B1 (32.67 ± 0.53°C and 32.56 ± 0.49°C for CON and FAN, respectively, p = 0.72) between conditions. There was a main effect of condition with the change in lower back skin temperature being smaller in FAN than in CON (p = 0.009, d = 1.39, Table 1). Figure 5 shows infrared images from one trial, depicting the change in temperature of the backrest during both CON and FAN. Figure 6 shows infrared images from one trial, depicting the change in temperature of a participant’s unclothed back during both CON and FAN. Infrared images of the backrest during the control (CON) and fan (FAN) condition at the five time points. The images were taken during one participant’s trial. B1 = end of block 1, B2 = end of block 2, B3 = end of block 3, B4 = end of block 4. The temperature scale for the images is shown at the right of the images (20–35°C). Infrared images of a participant’s back unclothed during the control (CON) and fan (FAN) condition at the five time points. The images were taken during one participant’s trial. B1 = end of block 1, B2 = end of block 2, B3 = end of block 3, B4 = end of block 4. The temperature scale for the images is shown at the right of the images (20–35°C).

Perceptual responses
Mean ± SD for perceptual responses at rest (except for RPE) and the end of each block for each condition are shown in Table 2. Thermal sensation and thermal comfort were not different at rest between conditions (p > 0.05). Rating of perceived exertion, thermal sensation, thermal comfort and wetness sensation were not different at the end of B1 (p > 0.05). Rating of perceived exertion and thermal comfort did not significantly change over time (p > 0.05), whilst thermal sensation did significantly increase over time (p < 0.01). For perceptual responses, only wetness sensation was significantly different between conditions, being lower in FAN compared to CON (p = 0.02).
Discussion
The current pilot study aimed to determine the effectiveness of an integrated fan cooling system (WheelAir® slingback) during simulated daily pushing in able-bodied participants. Despite the participants being able to thermoregulate effectively, having the fan on its highest setting resulted in a lower back temperature difference of 2.20°C compared to no fan (iButton data). By the end of the fourth block in the FAN condition, lower back skin temperature had returned to resting levels after having the fan turned on for 45 out of the 60 min of total pushing time. Previous research has shown that a 1°C increase in skin temperature causes a 10% increase in tissue metabolism, 4 increasing the user’s susceptibility to skin injury. The reduction in skin temperature observed at the lower back in the FAN condition highlights that the integrated fan cooling system could help reduce the risk of skin injury at this localised region of the back.
To ensure the only differences between conditions was the use of the fan during the second to fourth blocks of pushing, all other measurements (ambient conditions, lap time, fluid balance, heart rate, RPE) needed to remain the same, which was observed in this study. The skin temperature measurements of the chest, scapula and mid back measured by either the iButtons or infrared camera were not significantly different between conditions, signifying that the integrated fan cooling system only provided cooling to the localised skin region directly exposed to the fan. Hence, results showed that the only temperature differences between conditions were lower back skin temperature and the temperature of the backrest itself, measured using both the iButtons and the infrared camera. Participants did not perceive to be any cooler or more comfortable in FAN, yet wetness sensation was lower in FAN compared to CON. Therefore, despite cooling being provided at a local level, participants did feel overall their skin was ‘drier’ using the integrated fan cooling.
The present study did not directly compare the extent of the cooling provided by the integrated fan cooling system in comparison to other cooling strategies anecdotally used by wheelchair users during daily activity, such as water sprays or wet towels. However, meta-analysis data has shown that cooling methods applied to individuals with a spinal cord injury utilised pre and during exercise have a large effect on mean skin temperature (Hedges’ g = 1.11). Cooling techniques included in the meta-analysis consisted of ice/cooling vests, hand, neck and head cooling, ice slurries and water sprays. 18 In the current study the integrated fan cooling system had a large effect (p = 0.01, d = 1.47 and p = 0.009, d = 1.39 from the iButton and infrared image data, respectively) on lower back skin temperature during activity aimed to represent daily pushing activity. This shows that even during low activity levels, the integrated fan cooling system does provide a comparable cooling effect on skin temperature, albeit locally, compared to current cooling techniques used during exercise. 18 Of note, the participants used in the meta-analysis and current study are different, limiting the direct comparison of these data sets. Despite this, the present data indicates that the integrated fan cooling system does provide a significant change to lower back skin temperature, which also impacts user wetness sensation.
From a practical perspective, the potential disadvantage of existing cooling techniques, despite the low cost, is the need to be able to refill or refresh the spray or towels frequently to continue to provide an adequate cooling stimulus, which may not always be possible or easy to navigate for some wheelchair users. Despite the need to re-charge the integrated fan cooling system, with a recommended battery life of 6–20 h depending on usage by the manufacturer, recharging the battery would be less frequent than the need to refresh towels or spray bottles. Therefore any product that is integrated into the wheelchair enables the user to be in charge of their cooling needs as and when they are required. Future developments in wheelchair design should attempt to accommodate not only the wheelchair user’s needs in relation to comfort, weight, durability and manoeuvrability but also consider the thermal requirements of the users and possible cooling integration with the user’s wheelchair.
As this was the first research study to test the integrated fan cooling system during daily pushing, able-bodied individuals were recruited to participate to determine whether there were any distinct and clear differences between using the highest fan setting of the slingback fan and not having the fan on at all. The participants were novice wheelchair users, hence the consistency and efficiency of their pushing between conditions may have been considerably lower than wheelchair users. 19 Despite this, participants were able to maintain the same speed between conditions, with similar lap times between both conditions and no effect of condition order. Therefore, given the slow speed and short period of pushing time (15 min), the able-bodied participants were able to regulate their pushing activity between conditions.
For wheelchair users that are unable to perceive an increase in back skin temperature, for example individuals with a spinal cord injury, using the integrated fan cooling system may help to prevent a build-up of heat at the skin-surface-chair interface, which could prevent an increase in skin temperature2,3 and potentially secondary complications. However, the integrated fan cooling system is yet to be independently tested using wheelchair users, either with or without a thermoregulatory impairment, so this result is currently speculative.
Limitations
Participants were asked to push at a speed akin to normal daily activity to try to ensure that the chosen speed was reflective of typical daily pushing activity. On average this related to a speed of 1.27 m/s regardless of the testing condition. These self-selected speeds by the participants in the current study are likely to be faster than the speeds typically used by wheelchair users during daily activity. Previous literature has reported an average daily pushing speed of 0.47 m/s (1.7 km/h) for individuals with tetraplegia and paraplegia 20 and typical daily bouts of wheelchair pushing being 0.23–0.83 m/s for individuals with a range of disabilities, but mainly users with a spinal cord injury. Faster bouts, stated as being greater than 1 m/s and similar to the speeds selected in the present study, being more common in younger users (∼36 years old). 21 Nevertheless due to the large disparity between wheelchair users of different functionality, daily pushing speed is likely to vary quite considerably between users. The 85 m lap to push around is not wholly representative of the pushing activity encountered daily by wheelchair users, due to the lack of change in terrain, environmental conditions, or obstacles to overcome. A wheelchair skills test 22 does exist to determine wheelchair user’s skill deficiencies, encompassing daily life activities such as going up and down curbs and stairs. However, the authors believe that a set lap distance and recorded time for each block was easier to replicate for the two conditions, especially for the able-bodied participant group, to determine whether the integrated fan cooling system cooled the skin of the user.
The generalisability of the findings of the study may be affected by the recruitment of an able-bodied participant group instead of a wheelchair user group. As this study was undertaken as an initial pilot study to investigate the effectiveness of the integrated fan cooling system, to reduce the potential disparity between wheelchair users with differing disabilities and physiological function, able-bodied participants were recruited. As mentioned above, wheelchair users are likely to push at slower speeds than those used in the present study and hence produce less heat. The difference in lower back skin temperature between conditions in the current study was highly variable (Figure 4), especially at the end of block three and four. This could be due to differences in clothing between participants and the contact between the participant’s back and backrest because of position and posture in the wheelchair. For wheelchair users, the disability of the wheelchair user, in addition to the speed of pushing, clothing and contact between the back and backrest will likely also impact the temperature of the back, but by how much is unknown. For example, for those with a thermoregulatory impairment, a smaller thermal gradient may be apparent between the backrest and back skin temperature, compared to able-bodied individuals. Therefore, cooling using the integrated fan system may have a greater impact on back skin temperature. Though this requires further investigation.
Conclusion
Using the highest fan setting of the integrated fan cooling system (WheelAir® slingback), wetness sensation was lower and lower back skin temperature was reduced by 2.20°C (iButton data) during daily pushing activity compared to not using the fan. Having the fan turned on for 45 out of the 60 min of total pushing time reduced lower back skin temperature to resting levels. The skin temperature measurements of the chest, scapula and mid back and all other measurements (ambient conditions, lap time, fluid balance, heart rate, RPE, thermal sensation and thermal comfort) were not significantly different between conditions. This signifies that the integrated fan cooling system only provided cooling to the localised skin region directly exposed to the fan and did not affect any other physiological responses. Despite the recruitment of able-bodied and novice wheelchair users for this study, future research should independently test using wheelchair users, both with and without a thermoregulatory impairment to determine whether a similar response is apparent to those observed in this study.
Footnotes
Acknowledgements
The authors would like to acknowledge the undergraduate students, Jacob Day and Kate Hopwood, that assisted in collecting the data for this study and the participants for volunteering for this study. Nottingham Trent University provided a financial contribution (Trent Institute for Learning and Teaching) to support these students financially whilst collecting the data for this study. Gratitude is given to WheelAir® for loaning the WheelAir® slingback to be tested in this study.
Author contributions
KG contributed to the study conception and design, data collection and analysis. FV contributed to analysis of the data. The first draft of the manuscript was written by KG and FV. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
KG.