
Abstract
Introduction
Available robot-assisted stroke rehabilitation systems are often limited in their utilization in the home environment, due to several barriers such as high cost, absence of therapists, tedious training tasks, or encumbering interfaces. This paper presents a low-cost robotic rehabilitation and assessment device for restoring wrist function, offering wrist exercises incorporating pronation-supination and flexion-extension movements. Furthermore, the device is designed for the assessment of joint stiffness of the wrist, and range of motion in two degrees of freedom.
Results
The device demonstrates the ability to determine the stiffness of an object with low-cost hardware. Use case scenarios of the device for training and assessment of the wrist are presented, allowing for a range of motion of
Conclusion
The device shows potential to help objectively quantify the stiffness of the wrist movement, which consecutively could be used to represent and quantify the degree of impairment of patients after stroke in a more objective manner. Further clinical study is necessary to examine this.
Introduction
Stroke and other cerebrovascular diseases are one of the major leading causes of death globally (6 million deaths annually) and stroke is the second leading cause of disability within Europe. Therefore, it is of utmost importance to improve rehabilitation techniques and devices in order to better support patients who suffer from sensory-motor deficits caused by stroke. 1
This is especially true as the prevalence of stroke is expected to further increase, as the percentage of the population over 65 years old grows, which is the current trend for most developed countries. Additionally, the long-term disabilities caused by stroke are significantly greater for older patients. The resulting financial burden for the EU27 countries is estimated by the WHO to be €27 billion with an additional sum of €11 billion accounting for informal care. 1 This increasing financial and social burden, in turn, urges the development of affordable rehabilitation solutions that support the rehabilitation effort, not only in a clinical setting but also at home.
Due to the neuroplasticity of the brain repetitive movements of the affected limbs can promote their sensory-motor recovery. Thus, therapists assist exercises and movements to promote recovery of their patients. On average therapy sessions are only possible twice a week, which results in a lack of repetition of the rehabilitation exercises. Robotic rehabilitation devices can assist the patient in carrying out the required exercises; therefore, reducing the physically taxing workload for skilled therapists. As a further consequence the cost of therapy is lowered, while maintaining the high quality of care that is desired. In the case of home rehabilitation this can increase the frequency and duration of therapy and complement the classical therapy approach. The effectiveness of this type of robotic assisted therapy has been proven through multiple studies.2–5
A further benefit of robotic rehabilitation devices is the possibility to employ sensors on the device for monitoring the effectiveness of the rehabilitation effort and other quantities (e.g. duration and frequency of use). Especially in a home rehabilitation setting, this type of data collection gives a physician or therapist a more objective overview. This, in turn, can be used to adapt the current therapy and assess the severity of impairments.
In general, (neuro-) rehabilitation as an interdisciplinary treatment approach for functional health 6 focuses on optimal sensory-motor function, maximal independence and the best possible reintegration in the home and vocational environment of patients with neurological deficits. 7 The concept of evidence-based medicine (EBM) is based on the scientific knowledge from basic and health research as a source for clinical decision-making and optimal care of sick people in the prevailing health system. 8 The clinical-neurological examination, functional assessments and the measurements with high-sophisticated devices to standardize quality of movement are of particular importance. 9
The objective measurement of motor performance is an essential component in the clinical practice and provides important information for identifying neurological disorders and for determining the direction and details of treatment. 10 In this context, objectifying spasticity is not an easy task. Spasticity is clinically most often measured by a stimulus to the muscle tendon (hyperreflexia) or by passive movement of the limb (muscle hypertension). 11 Furthermore, resistance to passive stretch is quantified under laboratory conditions with the help of repeated oscillation or individual ramp movements. 12 The difficulty of the measurement, both in the clinical setting and in the laboratory, is that there is no differentiation of a neuronal cause from a peripheral one, in terms of soft tissue changes. In addition, there is no relation between the phasic stretch reflex (stimulus to the muscular tendon) and the tonic stretch reflex (movement of the extremity). 13
While the (modified) Ashworth scale (MAS) adequately measures muscle resistance, it measures both the neuronal and peripheral contribution to resistance without differentiating it. The Tardieu scale14,15 on the other hand, seems to be able to identify a neuronal component due to different angular velocities, a standardized initial position (condition) and measuring the angle at which the resistance occurs.15,16 Both scales rely on subjective interpretation of the muscle resistance and on the investigator’s clinical experience, as well as, both being physically taxing for the investigator.
It is therefore of great scientific and clinical interest to objectively measure spastic changes in muscle tone of neurological patients in order to better assign clinical syndromes, better plan and objectify pharmacological and behavioural interventions, and to better optimize rehabilitation after stroke. Additionally, such research can further facilitate the ability to distinguish between neurological and peripheral contributions to spastic muscle tone. Because of the relevance of a potential assessment for spasticity the presented device focuses on measurements needed to explore the link between spasticity and the mechanical stiffness of the affected limb, through further research, similar to Refs.17–19 Riener et al. showed a significant correlation between measured stiffness and the modified Ashworth scale, in particular for patients with more severe impairments in lower extremity. In this regard, we assume that the assessment of the stiffness is linked to spasticity, also for the upper extremity.
According to the WHO report in 2018 the current situation falls short of a substantial need for rehabilitation. This occurs globally, in some countries 50% of people who require rehabilitative care do not receive it. This is due to several reasons, the majority of which are linked to a lack of funding or a lack of availability of rehabilitation services. This is particularly the case outside of urban areas and is characterized by long waiting times and high expenses for patients. Additionally, a lack of skilled therapists as well as rehabilitation devices is also noted. 20
Embracing the use of low-cost devices especially benefits low-income countries that are lacking in their healthcare systems, and in their availability of the necessary specialized medical personnel. Simultaneously, a low-cost system offers the possibility of being used not only in a clinical setting, but also in a home rehabilitation setting, and thus increasing the frequency and duration of therapy. 21 This requires the device to be easy to use, without requiring assistance of a professional, and have fast setup times. Further, the advantages of the compact, low-cost, and user-friendly devices may increase the use in home rehabilitation. This can play a significant role, especially under the current pandemic situations by facilitating physical rehabilitation exercises at home and reducing infectious exposure.
To provoke the maximum amount of neuroplasticity, and with that potential for a positive rehabilitation effect, different control strategies for the device should be employed. For example methods such as assistance-as-needed through impedance control or an adaptation of control parameters based on patient’s performance. 22 Training in virtual reality environments with adjustable difficulty levels is one further way to implement different levels of assistance depending on the needs of the patient using the rehabilitation device.
State of the art
After the MIT MANUS I was introduced in 1991, many robotic rehabilitation devices have been created. Most of these are solely developed for research purposes, although there are commercially successful devices that are used in a clinical setting.
A majority of these rehabilitation devices for the upper extremity focus on the gross motion. This often overlooks the fine motor skills of the hand and wrist that are necessary for completing activities of daily living (ADL), such as pouring water, eating and writing, independently. Current low-cost rehabilitation devices are typically not actuated and therefore, only compensating the effects of gravity or being used passively by the patient. Although these devices are effective for some patients, they are unable to support patients with severe motor impairments.
Robotic rehabilitation devices focused on the forearm and wrist exercises often provide 2 to 3 DOF, allowing elbow pronation/supination, wrist flexion/extension, and wrist abduction/adduction. However, the characteristics of these robotic rehabilitation devices, such as range of motion (ROM) and maximum torque depend on the mechanical configuration (e.g. capstan drive, slider crank mechanisms, gear drive, etc.), actuator type and its specification.
The ReHapticKnob presented by Metzger et al. 23 is a 2 DOF hand rehabilitation robot which supports a patient’s hand opening movement as well as their pronation-supination (PS) wrist rotation, which are movements that are particularly important for performing ADL. The device offers an impedance control mode with a wide Z-width and an additional force feedback scheme.
Su et al. introduced a lightweight (1.5 kg) and compact 3 DOF exoskeleton rehabilitation robot, supporting the rotation of the wrist by means of sliding crank mechanisms. 24 Another exoskeleton type of 3 DOF wrist exercise device, WREs, employs capstan cable drives. Its wrist interface can be integrated with an upper arm and hand exoskeleton. 25 Compared to other wrist rehabilitation device, ROM is smaller but it generates high maximum continuous torques, especially in the PS joint (over 6 N m). The OpenWrist presented by Pezent et al., 26 is based on a serial kinematic structure that actively supports movements of the wrist in all of its 3 DOF with the necessary torques to provide a rehabilitation effect, even in the case of severe impairments. A gimbal mechanism in combination with capstan drives is utilized for the wrist joint rehabilitation device. 27 The gimbal mechanism enables much greater ROM than other configurations.
Most robotic rehabilitation devices, including the aforementioned, are driven by electro-mechanical actuators. SUE, on the other hand, is a pneumatically driven 2 DOF rehabilitation device. 28 Pneumatic actuators provide high power output, while dimension and weight of the end effector can be substantially decreased by replacing motors and bulky power transmission mechanism with a pneumatic cylinder or tube. But the dimension and weight of the overall system including air compressor, and storage bottle is not compact or light, thus it may become a limiting factor for the home use. Although developed robotic rehabilitation devices offer promising characteristics, they might not be suitable for home and community-based rehabilitation, due to the high cost. We estimate the cost of one of mentioned devices above to be over €1200, based solely on the cost of all mechatronic components of the device mentioned in Ref., 29 although the total cost is likely significantly higher. Additionally, it requires a data acquisition (DAQ) system and a voltage-controlled amplifier for its hardware in the loop setup.
To overcome the cost issues, several low cost rehabilitation devices have been introduced.
Malosio et al. 30 presented an adaptable and affordable 1 DOF rehabilitation device for the upper limb, the LINarm++, a further development of the LINarm. 31 Through its focus on adaptability and modularity it can be configured according to the needs of the patient or usage environment.
The DUALarm presented by Dinon et al. in Ref. 21 is an upper limb rehabilitation device with a focus on its low-cost and accessibility. It is an almost exclusively 3D-printed device and therefore, inexpensive and easy to manufacture. To remain low-cost the DUALarm is unactuated and only offers rudimentary sensor data acquisition.
The use of sensor data to monitor and assess patients is an important benefit of robotic rehabilitation devices, especially for deficits that are not easily quantified, such as spasticity. Assessment is also an important element of rehabilitation in order to examine the training effect of rehabilitation devices, or to offer a suitable therapy according to the patient’s impairments. Objective and automated assessment techniques have been proposed to compensate for the shortcomings of the subjective and high workload requiring conventional assessments. According to the recent upper extremity function assessment survey in 2019, 32 most automated assessments in neurorehabilitation focus on performance of gross or dexterous motor function while automated assessment of spasticity is only scarcely covered.
The surface Electromyographic (sEMG) measurement is one of quantitative spasticity assessment methods that could determine a neuronal component of spasticity due to the presence of muscle activity caused by stretching. Several studies hinted that electromyographic activity is associated with spasticity through significant correlation between MAS and sEMG measurements.33,34
A torque sensor using a metal foil strain gauge measures the torque of the elbow and wrist and these measurements of the resistance torque show significance between different spasticity levels. 35 By using this approach, the torque to overcome the stiffness is determined by taking into account the total torque, torques rotating the device in consideration of the weight of the user’s arm. Heung et al. proposed a joint stiffness estimation approach through pneumatically driven soft actuators to evaluate finger spasticity. According to their study with four stoke patients and four healthy subjects shows that estimated stiffness on both PIP and MCP joints are correlated with MAS and there is an apparent stiffness difference between two participant groups. 36
The NeuroFlexor (Aggero Medtech AB, Sweden) is a commercially available spasticity assessment device for upper extremity. 37 It measures the force required to move a patient’s hand in a purely passive way in 1 DOF. It supports the flexion-extension (FE) and adduction-abduction (AA) (also called ulnar and radial deviation) degrees of freedom, although a change in setup is required when switching from one movement to the other. According to Refs.37–39 the model employed by the NeuroFlexor to determine the level of spasticity sufficiently, especially with patients with moderate to severe impairment. However, the accuracy of the results can vary depending on how well the setup is carried out, which is impractical for a device that should be used without supervision from a professional. The reason for this is due to the employed force measurement that must be compensated for gravity. Therefore, it depends on the position of the center of gravity of the patients arm within the device. The Lokomat® (Hocoma AG, Switzerland) uses force sensors for assessing the spasticity of the lower extremities. Based on the force sensor in the system, the torque required to move a patient’s legs along a predefined trajectory at different movement speeds is measured. The resulting data for leg position and required torque is used to calculate a linearly dependent mechanical stiffness. This method was presented in Refs.,17–19 but has not yet been applied to the upper extremity.
Measurement of muscle tone has been a scientific goal for decades. 40 However, due to the complex nature of spasticity, its comprehensive quantification has been impossible to date. Adequate treatment of spastic patients is important, but the assessment of the training efficacy remains challenging. The previously mentioned rehabilitation devices for upper extremity mainly focus on motor training and do not take into account the function of spasticity assessment. A high performance rehabilitation device can measure joint stiffness by using a torque sensor, but the high price of such a torque sensor consisting of strain gauges is a limiting factor for home rehabilitation. As shown by the discussed devices, and summarized in Table 1, there is a severe lack of low-cost rehabilitation devices that are designed for therapy of the distal upper extremity, particularly for the wrist. Similar is true for any assessment functionality, particularly with regards to spasticity.
Characteristics of similar rehabilitation devices; assistance types: A - active, p - passive; prices are estimated based on used components; range of motion (ROM); assessment capabilities (ASMT): Y - yes, N - no.

To overcome the aforementioned limitations of home rehabilitation settings, we present a low-cost rehabilitation device for assessment as well as therapy of wrist/forearm functionality. Unlike other low cost rehabilitation devices compromising between costs and performances, the proposed device targets to support high performance (high torque output, great ROM, high resolution sensing) and a low-cost and easy to use home rehabilitation system. In general therapy and assessment are carried out sequentially and individually during a rehabilitation process. As Jang et al. showed intervention of the hand and wrist stretching by their proposed device enhances not only spasticity but also motor function. 42 We propose a device that can support both 2 DOF motor training (including similar wrist stretching as Jang et al. presented) of the wrist and forearm simultaneously and assessment of joint stiffness. In this context, it is possible to adjust the speed or range of motion adaptively according to a patient’s joint stiffness, with higher resolution than the conventional assessment methods (Ashworth Scale, MAS, or Tardieu scale).11,43,44 This may be another scientific brick in understanding these manifold correlations of abnormal muscle tone. To examine our ultimate hypothesis, this article presents a therapy and assessment device and addresses a feasibility test to validate the joint stiffness based on the current measurement of the motors as an initial step.
System design
The proposed wrist rehabilitation device employs a serial kinematic chain with two rotatory joints that align with the movement axes of the PS and FE joints of the human arm and wrist as shown in Figure 1.

Serial kinematic chain of the device consisting of a rotational axis each for PS and FE which have an angular offset of 90° to each other.
This configuration simplifies the degrees of freedom of the wrist by not incorporating the adduction-abduction DOF of the wrist, as it is not used extensively in ADL and exhibits the lowest range of motion (ROM) of the three DOF of the wrist. This also simplifies the employed controller, independent of its type or structure. This results in the possibility to use a low-cost microcontroller for the entire control scheme, as well as for data acquisition. This reduction in system complexity, in turn, leads to a decrease in overall system size and cost.
The novel stiffness assessment functionality of the proposed device is based on the measurement of the torsional stiffness of the affected upper limb. A similar approach has been presented in Refs.17–19 which has so far only been applied to the lower extremity. This is done by moving a patient’s wrist through a chosen trajectory at different velocities. The torque required for this movement is measured and used in combination with the position data to determine a linear stiffness value for a given movement velocity. Additional measurement capabilities are also available, e.g. for determining the active and passive ROM or the time necessary to complete a rehabilitation exercise.
Mechanical design
A rendered CAD model of the wrist rehabilitation device is illustrated in Figure 2, also depicting the two movement axes. The device features a mechanically limited ROM of

Rendered CAD model of the developed rehabilitation device. Colors do not represent the real device; functional units share the same color.
The mechanical construction of the device uses laser cut acrylic sheets and extruded aluminium profiles for its main structural components. Each joint of the serial kinematic chain features a capstan transmission which are the main components of the design. They are color-coded in Figure 2, with orange and yellow for PS and FE, respectively.
Both revolute joints use the same type of sealed radial groove ball bearing (DIN 625 608), to allow for smooth rotation. This type of bearing also allows for moderate axial loading, which is necessary for the FE DOF and, to a lesser extent for the PS DOF. Additionally, these bearings are relatively inexpensively, as they are also the standard used in sporting equipment like skateboards.
As illustrated in Figure 3 the arc design of the PS joint requires a curvilinear slide to allow rotation around its central axis. This is the case, because the patient’s forearm has to lie coaxially within this arc. Therefore, a custom bearing assembly, which can be manufactured with the previously mentioned processes, has been developed. It features three bearings that ride on the two concentric surfaces of the PS arc.
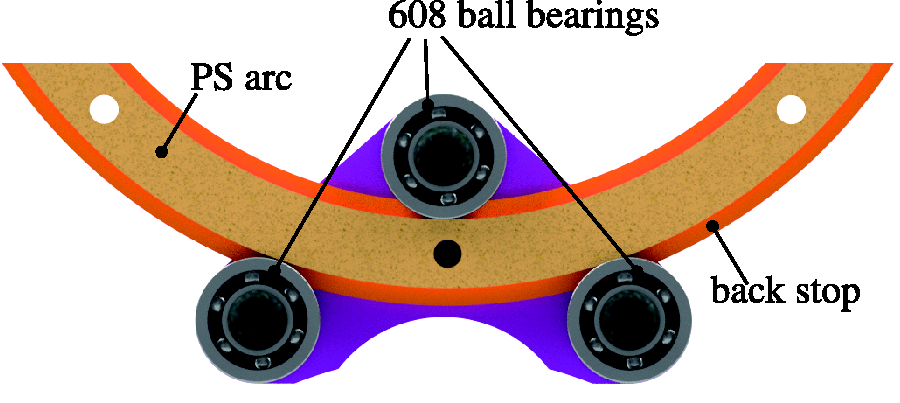
Low-cost bearing assembly as replacement for curvilinear slides; top bearing can be displaced downwards to create a preload.
To take up any axial thrust the PS arc features a back stop that rides on the planar faces of the bearings. The PS arc assembly is laser cut, solely requiring a constant thickness between its concentric surfaces. This absolute dimension is not overly critical as the top bearing can be displaced downwards to create a preload and through that remove any unnecessary play. This ensures that no additional manufacturing steps have to be taken to create an adequate bearing surface.
The basic usage of the device is demonstrated in Figure 4. The patient positions their forearm on the main housing and on the elbow support of the device (colored green and red respectively in Figure 2). This ensures that the natural human movement axes are coaxial with the actuated axes of the device. This position then allows the patient to grab the end effector handle.

Side view of the presented device; hand is positioned for using the rehabilitation device.
Actuation
Each joint is actuated by a brushed DC motor (RS775SM-6027-97, Wintech Precision Industrial Ltd.) through an H-bridge motor driver, and features an incremental rotary encoder (HEDM-5500#B14, Broadcom Inc.) for position and velocity feedback.
Detailed characteristics of the two joints are given in Table 2, all values are indicated with respect to the output side of the transmission of each revolute joint.
Joint characteristics; Note that transmission refers to the transmission ratio depending on the radii of the capstan; torque refers to maximum continuous joint torque; Error indicates to the maximum encoder error factoring in the transmission ratio.

For durations of less than 10 s higher torques of twice the stated continuous torques are possible before reaching the over current protection of the used motor driver. Furthermore, the torques are limited by the transmission capability of the capstan drive.
The specified joint torques from Table 2 are chosen as a design goal based on data presented by Pezent 29 and summarized in Table 3. This data describes the average continuous torque capabilities of six similar rehabilitation devices that were deemed successful, as well as the continuous torques necessary for completing ADL. This demonstrates a large difference between the requirements of ADL and the capabilities of typical rehabilitation devices.
Maximum continuous torques needed for ADL and average max. Continuous torque capabilities (mean μ and standard deviation σ) of six similar rehabilitation devices. 31

It is necessary to provide such high torques to move a patient’s wrist when increased muscle tone occurs from spasticity. To achieve this each joint employs a capstan transmission with a high transmission ratio
Lu et al.
47
describe the transmission capability in terms of the pretension in the cable Fp, the radius of the output arc ro, the coefficient of friction μ and the wrapping angle α

In the case of the presented device with a desired transmission capability
The cable has to be tensioned correctly, which can be done with a pair of adjustment screws at the fixation points on each capstan arc. On the initial assembly it is critical to have proper tension, which requires a way of measuring it. This is done by plucking the cable similar to a guitar string and measuring the frequency of vibration. This can in turn be used to calculate the tension based on the free-swinging wire length l and mass per unit length ml.


For the desired pretension of
Sensors
As the presented wrist rehabilitation device provides a novel assessment and measurement capability it is not only equipped with the rotary encoders, but also with two hall effect current sensors (LTS 15-NP, LEM Holding SA) which measure the motor current I for each joint during operation. The quadrature rotary encoders offer 4096 increments per revolution, when evaluated in full quadrature mode.
As the armature voltage of each motor is a pulse-width-modulation (PWM) signal with a frequency greater than 20 kHz, there are fast transitions dI/dt in the motor current that have to be considered in the sensor selection and require additional signal filtering which is implemented with a digital FIR filter on the main microcontroller. Additionally, an inaudible switching frequency lowers the overall loudness of the motor.
Electronics & control system
The main control system employed by the wrist rehabilitation device is a position control system that generates the desired trajectory and moves the two axes of the device according to this trajectory. As only the individual position of each axis is of interest there is no need to differentiate between the joint space of the device and the task space of the end effector, as the latter is not necessary for its use as a rehabilitation device.
Figure 5 shows a block diagram of the control system. All blocks depicted within the dashed lines are implemented on the used microcontroller, with a main control loop frequency of 1 kHz for the position control as well as for sampling the analog output signal of the two current sensors. The data transmission rate to the PC is reduced to 200 Hz, as the developed VR exercise does not support higher update frequencies.
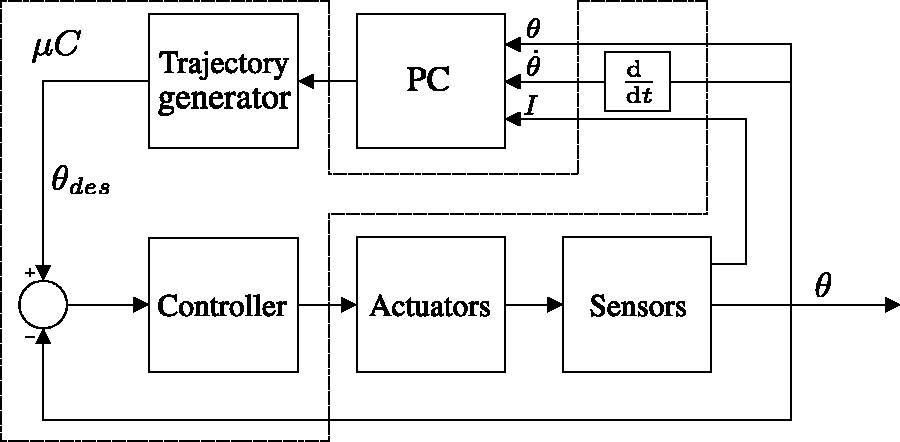
Overview of the employed position control loop. All blocks within dashed lines are implemented digitally on the microcontroller.
This control loop setup can be operated in the microcontroller sufficiently. Therefore, no expensive DAQ equipment is needed, as opposed to using the PC for control as well as for data visualization and running rehabilitation exercises.
The controller block implements a discrete proportional-integral-derivative (PID) controller with trapezoidal integration, backwards Euler derivative and uses a sampling time of 1 ms. To choose appropriate controller parameters, a system identification procedure is done using a grey-box approach. This allows the initial controller design to be done using the pole placement method, which was further modified to prevent saturation of the motor driver and other behaviour that was not accurately modelled in the system transfer function. This results in the system behaviour shown in the unit step response in Figure 6, showing no steady state error and a settling time of approximately 0.17 s for the PS axis joint of the device. The FE axis joint is tuned to achieve a similar time response.

Unit step response of the position controller for the PS axis. (a) Initial position of the arm in this exercise. (b) Arm rotated by 40∘ from the initial position.
The brushed DC motors of the device are driven by an off-the-shelf H-bridge dual motor driver (MDD10A, Cytron Technologies) which is readily available and relatively inexpensive. A further benefit of this motor driver is its support for switching frequencies greater than 20 kHz, which allows operation in the inaudible range. The system also features a safety switch that stops any movement of the device as soon as it is pressed by the patient. This ensures that a patient can safely use the device without assistance, as is necessary for home rehabilitation use.
Rehabilitation
For the aforementioned reasons it is of utmost importance for rehabilitation of an affected limb to perform training exercises frequently. In this section training modalities are categorized to passive-, active-, assistive-, active-assistive- and resistive training. Furthermore, the section gives an overview on how the represented device can be used to perform training exercises in the mentioned categories. 22
Passive training can be applied for patients suffering from flaccid paralysis. Therefore, the patient’s hand is fixed to the end effector and FE as well as PS movements of the wrist are performed by the device in order to preserve the joint mobility and avoid contractures of the joint as well as muscle contraction. In conventional occupational therapy passive motion of joints is performed with the intention to prevent an eventual spasticity or to lessen the same.
In an assistive training the device can be used to compensate a resistance in the joint or to compensate gravitational force which plays a minor part for the wrist movement.
The aim of an active-assistive training would be to increase the active range of motion (aROM). Therefore, a patient would move the wrist as far as it is actively possible without any support. From this point the device would assist the movement until a certain range. Therefore, the passive range of motion (pROM) would be determined first.
A resistive training approach could be used for low-threshold strength training where the motor of the device provides resistance against the movement of the patient’s impaired limb. This is done until a certain movement threshold is reached, where afterwards the movement of the end effector is allowed. 48
In a patient active mode the motion is performed by the patient and the system is used for measurement purpose which is further described in a subsequent section of this paper. A further increase of rehabilitation performance comes with the implementation of a virtual reality environment.
Training in virtual reality environments
This is the case, as virtual reality environments are an effective way to motivate patients to complete rehabilitation exercises and can therefore increase the effectiveness of robotic rehabilitation. Furthermore, the willingness to increase the duration and frequency of therapy is fostered, which is particularly important, as the aforementioned neuroplasticity of the brain benefits from a high frequency of rehabilitation exercises. 22
Figure 7 shows an example of an active or active-assistive VR rehabilitation exercise, which mimics the act of unlocking a door by turning a key in the lock. This activity of daily living is modelled as a pure rotation of the patient’s arm around its PS degree of freedom, though both degrees of freedom of the presented device can work in unison if the VR scenario supports this. The patient has to rotate their arm on the PS axis until a certain angle is reached. This angle can be changed when repeating the exercise and, through this be adapted to meet the patient’s needs. The repetition of this movement provides the desired rehabilitation effect. In order to provide an assistive torque that helps the patient complete the desired movement different approaches are available, one of which is presented in Ref. 49

VR exercise mimicking the act of unlocking a door. (a) Initial position of the arm in this excercise, (b) Arm rotated by 40° from the initial position.
For this exercise the patient uses the rehabilitation device as an input device to the main PC running the VR environment. Additional force feedback can be provided to the user.
To simplify and streamline the development of VR rehabilitation exercises the Unity game engine is used, which allows for fast development cycles and includes a variety of 2D- & 3D-assets that can be used.
In order to minimize the latency between the VR environment and the real device the Ardity 50 package for Unity is used. Ardity supports serial communication with a microcontroller board over USB, which further simplifies the process of developing VR exercises.
Furthermore, the Unity-based VR environment can also be used as a general data visualization platform that could be used to graphically display the recovery process, for example by showing the improvement in ROM over time.
Measurement principle
As stated previously the presented device employs position and current measurements for its main assessment principle.
The measurement of the motor current is used to determine the motor torque that is required for the device movement. The relationship between current and motor torque is dependent on the motor type that is used, and in the case of a brushed DC motor, it is a linear relationship 
For the assessment, only the patient component is of interest, as it represents the torque necessary to move the patient’s limb. Therefore, the static device component TD, which somehow represents a model of the mechanical system, has to be subtracted from the total torque T. This is done by measuring TD when the rehabilitation device moves through the desired trajectory without a patient using it. This has to be redone for all different trajectories that are being used in the evaluation procedure. This torque component therefore, encompasses all mechanical losses through friction and other causes, as well as the torque required for accelerating and decelerating the device.
The patient torque component TP of the upper extremity is used for the assessment functionality to calculate the torsional stiffness

The available sensors also allow the device to be used for further measurements. Particularly noteworthy in that regard is the measurement of the aROM and pROM of a patient, which is a parameter, where improvement through robotic rehabilitation training has been studied extensively, 4 for example in Ref. 49 Although, this has not yet been verified with the presented device.
Evaluation of stiffness measurement
The proposed system has been verified to deliver accurate measurement values for the device torque T and the torsional stiffness

(a) CAD rendering of the setup used for verifying the measurement capability on a torsional spring. (b) Torsion spring in normal and displaced configuration.
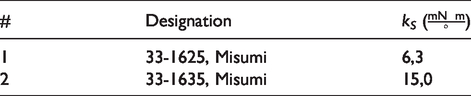
The evaluation process is carried out by angularly displacing one leg of the torsional spring (see Figure 8(b)) by an angle θ and measuring the current that is required to generate the necessary force F for this movement. The known spring stiffness kS can then be compared with the stiffness 
The trajectory used for this process is a symmetrical triangular trajectory, with an amplitude of
Verification procedure using a spring with
Spring stiffnesses for the used springs.
The deviation of the measured stiffness
Furthermore, the torque measurement error 
Mean and standard deviation of the error of the torque measurement.

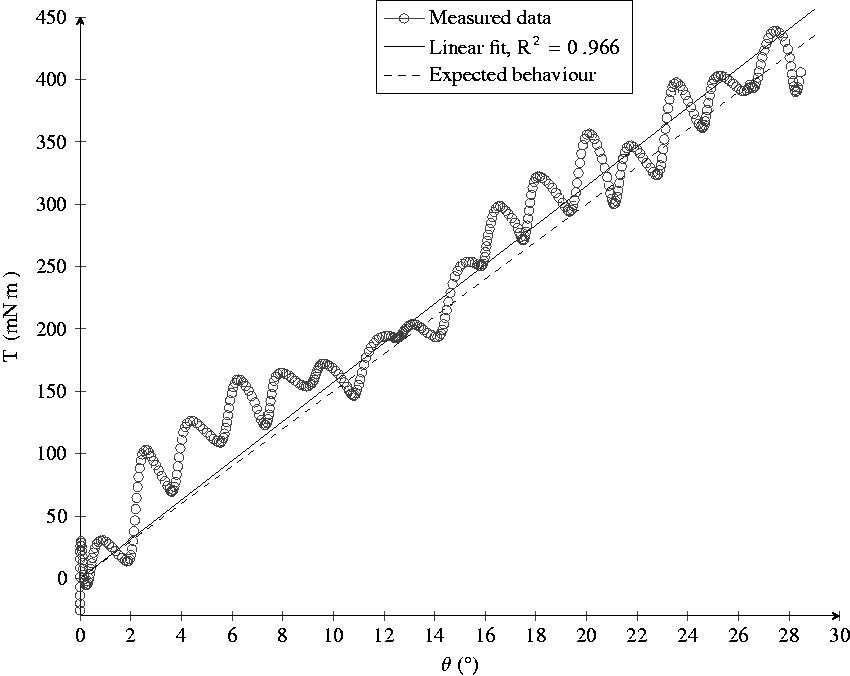
The raw torque data gathered during the evaluation process with two different springs is depicted in Figure 10. This also clearly shows that a spring with a higher stiffness kS results in a higher torque T, which further reinforces the feasibility of the proposed measurement system.
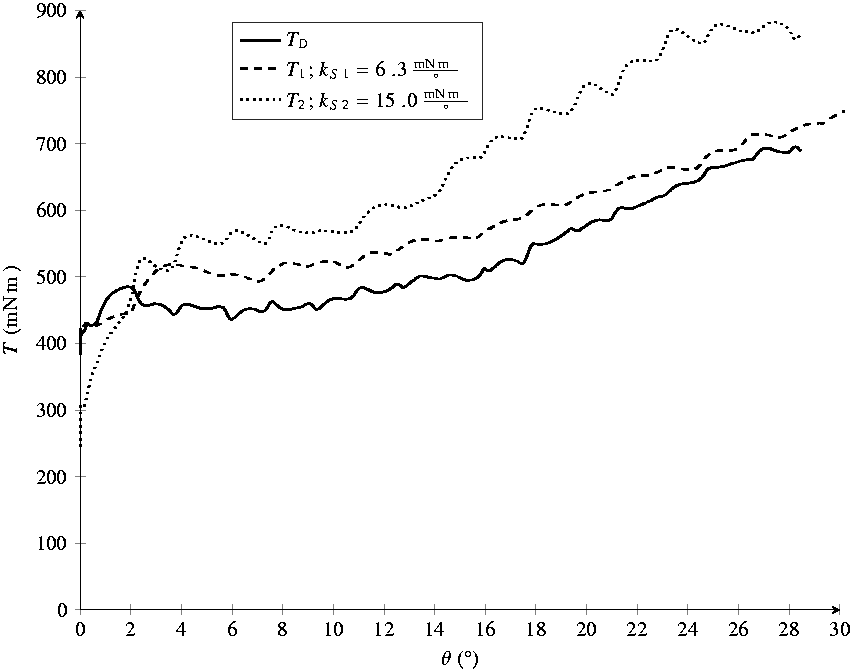
Raw torque data gathered during evaluation with two different springs. Device torque TD is measured without any spring.
Additionally, it can be seen that the resulting graphs are similar in shape, which indicates the difference
The periodic nature of the measurement signal stems from the inexpensive motors used in the device which show increased resistance at 10 locations over one full rotation. Verifying this claim can be done by calculating the angle moved between peaks
Conclusion
Current rehabilitation devices generally focus on the gross movement of the extremity which results in large devices. They are not suitable for a home rehabilitation setting, because of their size and cost. Furthermore, there is a lack of devices with assessment capabilities, in particular for spasticity.
The presented wrist rehabilitation device has two actuated joints for the PS and FE DOF, with a ROM of
The device features a price point of approximately €230.00 and a small size that makes usage in a home environment possible. This price point only considers the mechatronical components, broken down in Table 6, as well as the acrylic, aluminium profiles and miscellaneous hardware required for its construction. This is done in order to easier compare it to similar rehabilitation devices where the price can also only be estimated based on the used components. In the cost estimation, the costs associated with manufacturing, which greatly depend on the employed methods are not considered. In order to create a viable rehabilitation platform out of the presented device design changes are necessary to enable the use of manufacturing techniques more suitable for serial production. Based on a production volume of 1000 units the authors roughly estimate the additional manufacturing and assembly costs can be brought to less than €300. Furthermore, a decrease in price of the mechatronic components stated in Table 6 can also be expected at these production quantities. For the end user further costs associated with the VR exercises in a PC or tablet device would be considered.
Gross price of mechatronic components.

The small size of the device also allows it to be used in conjunction with other rehabilitation devices. One example of this is a planar motion device 51 that supports the gross movement of the upper extremity while carrying the presented device for rehabilitation of the wrist. It further provides a novel approach to assess the stiffness of the wrist, which has been evaluated in a constructed test setup. Because of this unique feature set we believe the device will have a positive impact on rehabilitation.
The evaluation of the presented measurement functionality showed that a higher stiffness results in a measurable increase in current necessary for moving the device joint. This current can then be related to a torque and used to calculate the linear regression between position and torque, which represents the stiffness. To fully evaluate the effectiveness of the device, in particular the spasticity assessment functionality, a clinical study has to be conducted that can verify a possible link between torsional stiffness
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
YK.
Contributorship
MP developed and manufactured the first version of the presented device and wrote the first draft of the manuscript in conjunction with MN. AM and YK contributed to the design and implementation of the research and to the writing of the manuscript. All authors edited and reviewed the manuscript and therefore approved the final version of the manuscript.