
Abstract
Introduction
Gait impairments due to stroke impact millions of individuals throughout the world. Despite the growing interest in automating gait therapy with robotic devices, there is no clear evidence that robot-assisted gait therapy is superior to traditional treadmill-based therapy.
Methods
This work investigates the effect of perturbations to the compliance of the walking surface on the paretic leg of impaired walkers. Using a novel robotic device, the variable stiffness treadmill, we apply perturbations to the compliance of the walking surface underneath the non-paretic leg of two hemi-paretic walkers and analyze the kinematic and neuromuscular response of the contralateral (paretic) leg with motion capture and surface electromyography systems.
Results
We present results of evoked muscle activity (predominately tibialis anterior) and increased dorsiflexion in the paretic leg during the swing phase of gait at stiffness values of 60 kN/m and less for all subjects.
Conclusions
This work provides evidence for the first time of reducing the drop-foot effect in the impaired leg of hemiparetic walkers in response to unilateral perturbations to the compliance of the treadmill platform, thus providing direction for targeted robot-assisted gait rehabilitation.
Keywords
Introduction
Gait impairments due to stroke or other neurological disorders impact millions of individuals throughout the world and have become an important problem of the 21st century. Stroke is a leading cause of long-term disability with 795,000 new strokes occurring each year in the United States alone.1,2 Nearly 90% of stroke survivors require therapy, but the majority of patients only achieve poor functional outcome five years after the onset of stroke.2,3 Since a primary goal of impaired patients is to walk independently, 4 improved gait therapy will significantly improve the well-being of millions of individuals.
Neural plasticity, or the brain’s ability to learn and adapt, is believed to be the basis for relearning after neurological injury. 5 Thus, the aim of gait therapy after stroke is to provide interventions that facilitate neural plasticity in the brain.6,7 The use of robotics in gait rehabilitation is an emerging field in which gait training is largely automated.8,9 A benefit of robot-assisted gait therapy is that robots can perform many repetitions with high accuracy, thus replacing the physical effort required of a therapist and allowing more intensive, repetitive motions which are important for facilitating neural plasticity. 5 A variety of robotic rehabilitation devices have been developed in the last several years for gait therapy.10–15 However, there is no clear evidence that robot-assisted gait training is superior to conventional physiotherapy for either chronic or subacute stoke patients.9,16–19
A limitation of the robotic devices used for gait therapy is that they do not consider mechanisms of inter-leg coordination and how the sensory feedback from one leg affects the motion of the other leg. 20 Rather, the state-of-the-art devices, ranging from kinematically controlled exoskeletons 21 to impedance controlled orthotic devices,22,23 impose motion on the impaired limb. A recent review suggests that utilizing inter-limb coupling in stroke rehabilitation therapies will lead to improved functional outcome. 24 We have proposed, and are currently investigating, a novel approach to robot-assisted gait therapy which takes advantage of mechanisms of inter-leg coordination. 25 This approach consists of providing therapy to the affected limb in hemiparetic gait by only interacting with the unaffected leg. One of the most significant advantages of this approach is the safety of the patient since there is no direct manipulation of the paretic leg.
Our previous work of investigating mechanisms of inter-leg coordination with healthy subjects has shown a systematic and scalable contralateral response to unilateral stiffness perturbations. 25 Moreover, recent electroencephalography (EEG) experiments have shown that these responses in healthy subjects are mediated through the brain. 26 A particularly exciting result from a clinical perspective is the repeatable evoked muscle activation in the tibialis anterior (TA), and resulting dorsiflexion, during the swing phase of gait. 20 A major impairment after stroke or other neurological injury is insufficient activity in the TA (which is the primary muscle creating dorsiflexion) in the swing phase of gait which results in decreased dorsiflexion. Insufficient dorsiflexion during walking, referred to as drop-foot, is a problem that most impaired walkers suffer from, and is the leading cause of after-stroke falls.27,28 Therefore, the aim of this work is to investigate the evoked contralateral response to unilateral perturbations to the walking surface stiffness with hemiparetic subjects, thus providing additional insight into the applicability of this approach in robot-assisted gait therapy.
Methods
Experimental setup
Unilateral perturbations to the walking surface stiffness were induced using the variable stiffness treadmill (VST) system shown in Figure 1. The VST provides a unique platform for investigating mechanisms of inter-leg coordination through stiffness perturbations. Advantages of the VST over other experimental platforms include (1) a wide range of controllable stiffness while maintaining high resolution, (2) the ability to apply low stiffness perturbations at any phase of the gait cycle and (3) body-weight support (BWS) for the walker in order to suppress mechanisms of balance and posture. The system has been detailed in previous work29,30 and will not be described in this paper for brevity.
The variable stiffness treadmill (VST) setup. Subsystems shown include: (a) variable stiffness mechanism, (b) split-belt treadmill, (c) custom-made harness-based body-weight support, (d) BWS loadcells, (e) motion capture system.
Study participants
Two individuals who experience drop-foot on their right side were recruited to participate in this study.
The first subject was a 29-year-old female (weight 123 lbs) who had a hemorrhagic stroke 5.5 years prior to this study. The cerebrovascular accident occurred in the left hemisphere and resulted in right hemiparesis (dominant side). She has received physical therapy and occupational therapy, which was first focused on recovering her right arm function. She has minimal voluntarily controlled activation of her right TA and no voluntary contraction of the plantarflexors (i.e. gastrocnemius (GA) and soleus (SOL)). However, the subject is ambulatory because the muscles work in synergy such as when walking. The subject wears the NESS L300 Foot Drop System (Bioness Inc.) to reduce drop-foot while walking during routine activities. However, she wears an articulated ankle-foot orthosis (AFO) with a plantarflexion stop instead of the NESS L300 when wanting better ankle stabilization when walking. The subject wore her AFO while participating in this study. The subject provided informed consent before the experiment.
The second subject was a 17-year-old male (weight 155 lbs) who had a traumatic brain injury 18 months prior to the study. A left basal ganglia hemorrhage with surrounding edema and left frontal hematoma resulted in hemiparesis in his right (dominant) side. He demonstrates decreased right ankle dorsiflexion and utilizes a right hip hike to clear his right foot during swing phase. He currently does not use any assistive devices for walking. Informed consent from the subject and his parents was obtained at the time of the experiment.
Experimental protocol
The first subject participated in four sequential trials with a brief (approximately 5 min) rest break in between trials. For all trials, the subject was offloaded by 30% of her bodyweight. This was done to provide some postural support and to be consistent with experiments with healthy subjects previously performed.25,20 In each trial, she walked for approximately 7 min on the treadmill at a self-selected speed of 0.51 m/s. The right treadmill belt was not allowed to deflect for the duration of the experiment, thus preventing any direct perturbation of the right leg. The walking surface underneath the left leg (i.e. left treadmill belt) was commanded to maintain a stiffness of 1 MN/m, which is very high and considered to be rigid, for 30 gait cycles at the beginning of the experiment. Then, after a random number n of steps, where (a) Subject 1 and (b) subject 2 each experiencing a low stiffness perturbation to the left walking surface.
The experimental protocol for subject 2 was the same as for subject 1, with a few differences in order to accommodate the preferences and needs of this subject. The subject did not feel comfortable with the BWS, and therefore walked with 0% BWS. The subject wore the harness and was safely attached to the BWS system but was not offloaded with any force. This subject only experienced perturbations at the 80 and 60 kN/m stiffness levels. A picture of the subject experiencing a perturbation is shown in Figure 2(b). These experimental protocols are approved by the Arizona State University Institutional Review Board (IRB ID#: STUDY00001001).
Data collection and processing
Kinematic data for both legs were obtained at 140 Hz using an infrared camera system that tracked 12 infrared LEDs (6 on each leg) placed as pairs on the thigh, shank, and foot. These data were also utilized in real time for timing of the stiffness perturbation.
The muscle activity of both legs was obtained using surface electromyography (EMG) via a wireless surface EMG system (Delsys, Trigno Wireless EMG) and recorded at 2000 Hz. The use of surface EMG for measuring muscle activation during gait experiments is widely used throughout the literature.31,32 Electrodes were placed on the TA, GA and SOL of both legs. Raw EMG signals were processed by finding the moving root mean square envelope of each signal with a 250 ms window. After computing the EMG linear envelope, the data were normalized to the maximum value of that EMG signal.
The kinematic and EMG data corresponding to the gait cycles of normal conditions and the cycles pertaining to the perturbations were found and normalized temporally to percent gait cycle in order to eliminate discrepancies due to natural variations in gait patterns (i.e. stride length, cycle duration, etc.). The data of each gait cycle were resampled at each 0.01% of the gait cycle (approximately 0.15 ms) during the normalization to percent gait cycle. The first 30 gait cycles and the cycles in between perturbations during the normal conditions are included in the unperturbed data set. One gait cycle following a perturbation is not included in the unperturbed set in order to eliminate any residual effects from the perturbation. This processing results in normalized EMG signals as a function of percent gait cycle, where 0 and 100% correspond to the heel-strike of the left (perturbed) leg.
In order to evaluate the significance of recorded kinematic and EMG responses when compared to the normal condition, statistical significance was determined using an unadjusted unpaired t-test at each time instance. The unpaired t-test was selected in this case because it is a comparison of two independent distributions (i.e. gait cycles with and without perturbation) which have similar variances but different sample sizes. Each statistical test was performed at the 95% confidence level. Any potential Type I errors from tests being performed at each 0.01% of the gait cycle were eliminated by only concluding significance if at least 400 tests (i.e. 4% of the gait cycle) in a row indicated significance.
Results
The results of the experiment show that significant contralateral muscle activity can be evoked in the paretic leg of impaired walkers by unilateral perturbations to the stiffness of the walking surface. The analyses for this paper will be focused on the effects of the perturbation on the response of the contralateral leg, even though the left leg was directly perturbed through the stiffness change of the left walking surface, since the aim of this work is to investigate the evoked contralateral responses with hemiparetic subjects.
Results: Subject 1
The muscular response of the affected (unperturbed) leg to the low stiffness perturbations of magnitudes 20 and 40 kN/m is shown in Figure 3. The normalized EMG amplitude for the TA, GA and SOL (mean and standard deviation) for all gait cycles pertaining to each of these two surface stiffness levels is shown. The data are plotted as a function of the gait cycle percentage, where heel-strike and toe-off of the right leg are indicated on the figure as HS and TO, respectively. Black bars underneath an asterisk are included to indicate when statistically significant changes are observed. An indication of the timing of the perturbation of the left walking surface is also shown.
Comparison of averaged muscle activity of the unperturbed (affected) leg for subject 1 during normal (red) and perturbed (blue) gait cycles as a function of percent gait cycle, where 0% corresponds to heel-strike of the left (perturbed) leg. Plotted in rows from top to bottom are the normalized TA EMG, normalized GA EMG, and normalized SOL EMG for two levels of stiffness perturbation (20 and 40 kN/m), from left to right, respectively. Mean (darker lines) and standard deviations (lightly shaded areas) values are shown. Statistically significant changes are indicated by black bars placed beneath a black asterisk. Heel-strike and toe-off of the right leg are indicated by HS and TO, respectively. The duration of the gait cycle for this subject is approximately 1.4 s.
As indicated by the black bars in Figure 3, there are significant increases in TA and GA activation during the swing and stance phases, respectively, for both levels of stiffness. There was no evoked activation in any muscle for either the 60 or 80 kN/m stiffness levels, and therefore are not plotted for simplicity. There was no significant change in SOL activation at any of the stiffness levels. The most significant result is that there was muscle activity evoked in the paretic leg, showing the existence of mechanisms of inter-leg coordination after neurological injury. Moreover, the same result from this study (i.e. increased contralateral TA activation during swing phase) has been shown with healthy subjects in previous work.
25
This additional activation in the right TA also created significant dorsiflexion in the right ankle, as shown in Figure 4. Moreover, there are also increases in hip flexion and knee flexion for this subject, which was also seen with healthy subjects.
20
Comparison of averaged kinematics of the unperturbed (affected) leg for subject 1 during normal (red) and perturbed (blue) gait cycles as a function of percent gait cycle, where 0% corresponds to heel-strike of the left (perturbed) leg. Plotted in rows from top to bottom are the kip, knee, and ankle angles for two levels of stiffness perturbation (20 and 40 kN/m), from left to right, respectively. Mean (darker lines) and standard deviations (lightly shaded areas) values are shown. Statistically significant changes are indicated by black bars placed beneath a black asterisk. Heel-strike and toe-off of the right leg are indicated by HS and TO, respectively. The duration of the gait cycle for this subject is approximately 1.4 s.
Results: Subject 2
The results from subject 2 are similar to those from subject 1. This includes no significant contralateral response due to stiffness perturbations of 80 kN/m, but significant TA activation and dorsiflexion during swing phase due to stiffness perturbations of 60 kN/m. The contralateral muscular and kinematic response to the 60 kN/m stiffness perturbations is shown in Figure 5. The data are plotted as a function of the gait cycle percentage, where heel-strike and toe-off of the right leg are indicated on the figure as HS and TO, respectively. Black bars underneath an asterisk are included to indicate when statistically significant changes are observed.
Comparison of averaged muscular (left column) and kinematic (right column) response of the unperturbed (affected) leg for subject 2 during normal (red) and perturbed (blue) gait cycles as a function of percent gait cycle, where 0% corresponds to heel-strike of the left (perturbed) leg. Plotted in rows from top to bottom are the normalized TA EMG, normalized GA EMG, and normalized SOL EMG (left column) and hip, knee, and ankle angles (right column). Mean (darker lines) and standard deviations (lightly shaded areas) values are shown. Statistically significant changes are indicated by black bars placed beneath a black asterisk. Heel-strike and toe-off of the right leg are indicated by HS and TO, respectively. The duration of the gait cycle is approximately 1.8 s.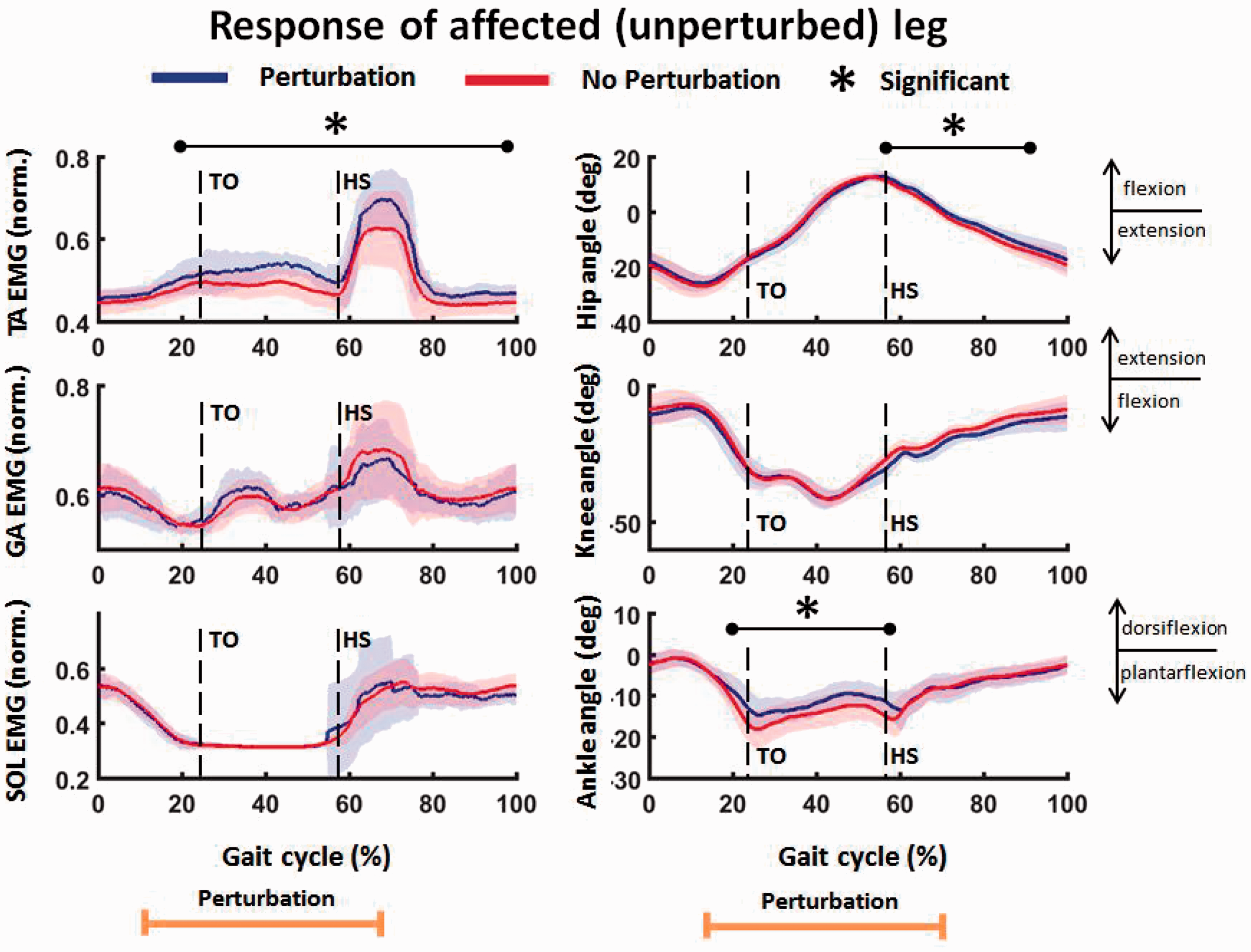
Discussion
The results of the experiment show that significant contralateral muscle activity can be evoked by unilateral perturbations to the stiffness of the walking surface. This supports the conclusion that mechanisms of inter-leg coordination still exist after neurological injury 24 and has strong potential for medical application in a novel approach to robotic gait therapy for hemiparetic walkers.
Inter-leg coordination
This paper shows results for the first time that increased TA activation, and subsequent dorsiflexion, in the unperturbed leg of neurologically impaired subjects is created by unilateral low stiffness perturbations. The increased TA activity in the affected leg is observed during the swing phase of the gait cycle when the TA is active during normal walking. This adds support to a previous hypothesis that the stiffness perturbations amplify existing neural commands as opposed to facilitating the generation of new commands. 20 Moreover, the significant changes in TA activity are only seen for the 20 and 40 kN/m perturbations, but not for the 60 and 80 kN/m perturbations for subject 1. Similarly for subject 2, significant changes in contralateral TA activity are seen at the 60 kN/m stiffness level, but not at the 80 kN/m level. As the level of stiffness decreases, there is a proportional increase in treadmill deflection (with a constant foot force across gait cycles) which suggests that there is a minimum deflection required to stimulate the mechanism of inter-leg coordination. 33 This is also supported by the result that evoked activation was observed for subject 2 at 60 kN/m, while it was observed for subject 1 at stiffness levels less than or equal to 40 kN/m. As subject 2 weighs more than subject 1 by over 30 lbs, a higher level of stiffness would be required to maintain an equal deflection of the treadmill.
The results of this experiment not only suggest the preservation of sensorimotor mechanisms of inter-leg coordination after neurological injury, but this mechanism appears to be robust across injuries and level of impairment. The contralateral response of increased TA activation and increased dorsiflexion was consistent across the two subjects despite differences between the subjects. A few of these differences include the time after injury, level of impairment, and compensatory strategies.
Our previous work with healthy subjects has shown systematic and scalable increases in contralateral TA and dorsiflexion in response to the unilateral stiffness perturbations. 25 Moreover, recent work suggests that these responses are mediated through the brain. 26 Therefore, the results presented in this paper suggest that the same mechanisms of inter-leg coordination observed in healthy subjects also exist after neurological injury. Moreover, the evoked TA activity and subsequent dorsiflexion during the swing phase of gait seen in the hemiparetic walkers in this work provides support for a unique approach to provide therapy to an impaired leg through physical interaction with the healthy leg in hemiparetic gait.
Possible clinical application
From a clinical prospective, the results of this study can be disruptive since they suggest a possible novel approach to robot-assisted gait therapy for hemiparetic patients who experience drop-foot. This approach would entail manipulation of the healthy leg through stiffness perturbations in order to evoke TA activity in the paretic leg during the swing phase of gait. As mentioned in the Introduction, a main deficiency in stroke survivors and other neurologically impaired walkers is insufficient TA activity during swing phase which leads to decreased dorsiflexion and greater risk for falls. The results presented in this study show that TA activation can be evoked during swing phase of the paretic leg (which induces increased dorsiflexion) in two different subjects who experience drop-foot. This suggests the feasibility of a solution to drop-foot by altering the stiffness of the walking surface underneath the healthy leg in hemiparetic gait.
Conclusions
This paper presents results of evoked dorsiflexion and TA activation in the contralateral (affected) leg of two hemiparetic walkers in response to unilateral low stiffness perturbations. Statistically significant changes are seen during the swing phase of the affected leg. This work provides evidence for the first time of reducing the drop-foot effect in the impaired leg of hemiparetic walkers in response to unilateral perturbations to the compliance of the treadmill platform. While this study is not conclusive considering the limitation of only having two participating subjects, the results from this study suggest the feasibility of a novel approach to gait training in which therapy for drop-foot is provided to the impaired leg by only interacting with the healthy leg in hemiparetic gait. Future research will include further development of this approach by investigating the effect of repeated perturbations (i.e. a change in walking surface stiffness during every gait cycle) in both healthy and impaired populations. Additionally, research into the effect of long-term therapeutic interventions (i.e. repeated gait training sessions over several weeks with impaired walkers) with the proposed methodology will be pursued.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Virginia G. Piper Charitable Trust and in part by the National Science Foundation under Grant #1727838.
Guarantor
PA.
Contributorship
JS and PA designed the experiments. JS conducted the experiments, collected and analyzed the data. Data interpretation was done by JS and PA. JS drafted and wrote the manuscript. PA reviewed the draft and made substantial comments. PA was responsible for funding. All authors have read and approved the final manuscript.