
Abstract
Televideo technology (e.g., Skype) has potential to support adults as they age by facilitating their interactions with people remotely; this potential may be even greater for adults aging with pre-existing mobility impairments, who face challenges interacting with others in person due to lack of transportation or accessibility. Our research employed questionnaire and interview methodologies to investigate this understudied population about their attitudes toward televideo technology for supporting social engagement, healthcare provider access, and physical activity. Participants were 14 adults aging with self-reported mobility impairments (50–70 years of age). Overall, participants were open to accepting televideo technology for social engagement, healthcare provider access, and physical activity. Participants perceived these technologies to be useful and perceived additional benefits, including the feeling of “being there” by enabling the viewing of facial expressions and the environment of the other person. Concerns included perceptions that televideo technologies lack security and privacy. Participants also expressed concerns that these technologies are difficult to use and are difficult to learn to use. The findings have implications for education, training, and deployment of televideo technology for home-based interventions for adults aging with pre-existing mobility impairments.
Keywords
Introduction
The aging population is growing at a rapid rate and currently there are insufficient supports in place to promote the health and wellness of these older individuals. In the United States, it is expected that there will be almost 84 million older adults by 2050. 1 A recent World Health Organization report addressed this growth and the resulting consequences related to world health. 2 Of particular note was the critical need for services and supports to enable older adults, especially those with physical and mental capacity losses, to fully engage in activities that are important to their quality of life; that is, there is a need for interventions to maximize the functional ability of older adults, particularly those with disabilities. Without such interventions, many individuals will be prevented from fully participating in society, including accessing necessary services to support health and wellness.
Individuals with the greatest physical and mental capacity losses have the most to gain from health and wellness services and supports. They have the largest gap between what they can do based on their physical and mental capacities and what they would need to be able to do to maximize their functional ability. Individuals with significant capacity losses comprise a substantial portion of the aging population. Almost 40% of people aged 65 and older report having at least one disability. 3 Of those 15.7 million people, two-thirds reported difficulty in walking or climbing stairs. Given the potential impact and the prevalence of disability in the older adult population, these individuals must be considered when developing and designing health and wellness services and supports.
Technology holds much promise as a vehicle through which to provide support and service interventions to adults who are aging with a disability. For example, televideo technologies facilitate interaction between remotely located people. Televideo is the use of two-way audio and video to exchange information, whether it be through a computer (e.g., Skype or Facetime) or through the use of a telepresence system or robot that allows a person to navigate around a remote environment (e.g., Kubi, Beam). 4 Several studies have focused on developing design concepts of telepresence for older adults and those with disabilities.5–9 Televideo technology may be particularly helpful for people who have barriers to participating in activities in person, such as those with mobility-related disabilities. Barriers faced by adults aging with mobility impairments include lack of accessibility, lack of information and resources, negative attitudes from others towards those with disabilities, lack of transportation, and psychological obstacles which include self-consciousness, lack of support, and fear of failure. 10 Televideo technology may reduce many of these barriers to facilitate participation in health and wellness activities for these individuals.
Televideo has been researched in a variety of health applications, particularly in telehealth. Telehealth can be defined as the delivery of healthcare services and education remotely via communication and information technologies. 11 Within the context of telehealth, televideo has been used to provide neuropsychological assessment of older adults, 12 problem-solving therapy for depressed older adults, 13 and remote rehabilitation.14–17 One such study explored the use of televideo for in home rehabilitation for adults with mobility impairments. 16 Televideo has also been researched in wellness applications, albeit to a lesser extent. These applications include exercise interventions for older adults with dementia, 18 as well as support groups for spouses of older adults with dementia located in rural areas. 19 There is scant literature on wellness applications of televideo for adults aging with mobility limitations. Nevertheless, these studies show some of the possible applications of televideo in the domains of health and wellness.
Given the potential of televideo technology for supporting health and wellness for adults aging with mobility impairments, there is a need for an in-depth understanding of televideo acceptance for this population. Understanding acceptance issues may provide insights for improving design, facilitating deployment, and increasing adoption for a technology. In particular, it is important to understand potential users’ perceptions of usefulness, ease of use, and the benefits/concerns they identify in using televideo technologies, because such factors are predictors of technology acceptance.20–22 One study did investigate perceptions of usefulness of televideo for older adults with a disability, albeit with a small sample size (6 community-dwelling older adults with disability and 6 health professionals). 23 Participants were asked to discuss health-related uses of telepresence technologies. Their ideas included remote monitoring of older adults’ health, social connectedness for the older adult and the caregiver, and a means to reduce travel for healthcare providers. 23 Although these findings provide some initial insights into perceptions of usefulness, more research is needed about televideo technology to assess perceptions of ease of use, and benefits and concerns, as well as to understand perceptions of usefulness in a wider context of health.
The goal of this study was to explore issues of televideo acceptance for adults aging with mobility impairments in the context of health, as well as wellness activities (i.e., social engagement and physical activity). Social engagement is associated with improved psychological and physical wellbeing, 24 such as an increased life expectancy. 25 Physical activity increases the overall health of older adults and life expectancy. 26 Not only are these domains critically important to health and wellness, they also pose participation challenges for this population. 27 We examined participants’ attitudes toward three televideo technologies to assess acceptance issues generally, but also issues that may be specific to televideo technologies with particular features (e.g., ability to navigate around a remote location). We used quantitative and qualitative methods to assess perceptions of usefulness, ease of use, as well as benefits and concerns of using televideo technologies for social engagement, healthcare provider access, and physical activity. Using this combined-method approach we aimed to not only understand whether participants perceived televideo technologies as useful and easy to use, but also to understand the reasons driving these attitudes. The findings provide guidance for the design and deployment of televideo interventions for adults who are aging with mobility impairments.
Method
Participants
Participants were 14 community-dwelling adults (50–70 years of age; M = 59.5, SD = 6.87, 8 females). All participants met the following inclusion criteria: between 50–79 years of age, self-identify a lower body mobility impairment that began prior to age 50, and ability to hear and communicate well over the phone. Self-identified mobility impairment was operationally defined as an impairment that caused serious difficulty walking or climbing stairs. 4
This study was approved by the Institutional Review Board of the Office of Research Integrity Assurance at the Georgia Institute of Technology. Participants were recruited by telephone from the Human Factors and Aging Laboratory’s Participant Registry (contains contact information for adult research volunteers, most over the age of 60) at the Georgia Institute of Technology and through outreach at local disability resource organizations (flyers, postings on organization list servers/newsletters). The majority of the participants were well educated, with 64% reporting at least some college education. Ten of the participants were Caucasian, and four were African American. Most participants (79%) reported their general health as “good.” Many (12) participants reported having some experience using some type of televideo software (1 participant did not provide a response). Most participants (7) reported having experience using Skype. No participants reported having any experience using telepresence robots with televideo software, including Beam and Kubi.
Procedure
All participants provided informed consent prior to the research study. Participants were mailed a questionnaire battery and asked to complete it before their interview session. This battery collected information on demographics (e.g., age, gender, race, and education), technology experience, and health, as well as vision, hearing, and mobility capabilities. 28
Participants were interviewed individually in a location of their choosing, either in their home environment or in an interview room at the Georgia Institute of Technology. During the interview, participants were asked about their opinions of three different televideo technologies, all of which provide users with two-way audio and video calling (see Figure 1). Skype, developed by Microsoft, is an application only (no hardware) that can be used on computers, smartphones, or tablets. Skype provides users with two-way audio and two-way video. Kubi, developed by Revolve Robotics, also offers two-way audio/video. Kubi’s hardware includes a stationary base and servos controlled arms (total height = 11.75 inches). The arms hold a tablet and allow a remote user to pan/tilt the tablet (300° pan, ±45° tilt) thereby changing the camera view. The Kubi application that controls the hardware can be used on a computer, smartphone or tablet. Beam is a telepresence system developed by Suitable Technologies. Beam has two-way audio/video as well. Beam’s hardware is comprised of a monitor and computer (Intel-based ultra low power i3 Sandy Bridge processor with 4 GB memory) that are attached to a wheeled mobile base (total height = 62 inches). The wheeled base allows the user to drive the system around the environment (sometimes referred to as “video conferencing on wheels”). The Beam application that controls the hardware can be used on a computer, smartphone, or tablet.
Characteristics of Skype, Kubi, and Beam with respect to their cameras, monitors, speakers, microphones, and mobility.
The technologies were presented to participants in order ranging from the least mobile, to most mobile with respect to users control of the remote camera: Skype (users cannot move the remote video camera (that of the individual(s) with whom they are communicating), Kubi (users can move the angle of the remote video camera to the extent of 300° pan, ±45° tilt via Kubi’s arms however the base itself is stationary), and Beam (users can move the camera via its wheeled base to navigate around the remote location). This ordering was purposeful based on pilot testing that showed participants had difficulty understanding how Kubi and Beam worked differently than televideo technologies they were more familiar with (e.g., Skype). Participants appeared to require the initial discussion of Skype, a technology most had some familiarity with, to understand how the other technologies had added mobility features and that Beam had more mobility than Kubi.
During the interview, participants were shown a short demonstration video of each televideo technology that described each system’s capabilities (videos ranged in length from 1 min 7 s to 1 min 17 s). After each video was shown, the participants were asked several questions to evaluate their perceptions of the technology including their perceptions of usefulness and the benefits and concerns they perceived with regard to using each technology. Participants were then asked to discuss their perceptions of using each technology in the context of three domains (social engagement, healthcare provider access, physical activity). The interview script is available from the first author upon request. Participants completed technology-specific questionnaires after the interview. The following questionnaires assessed opinions and attitudes about each technology and preferences in terms of usage (all were pilot tested to ensure clarity):
[Skype, Kubi, Beam] opinions questionnaire: Adapted from the technology acceptance models TAM and TAM2,20,29 this assessed opinions and attitudes about each televideo technology using a seven-point Likert scale (1 = extremely unlikely to 7 = extremely likely). It comprised six questions pertaining to perceptions of usefulness and six questions pertaining to perceptions of ease of use for each of the televideo technologies. [Skype, Kubi, Beam] contact usefulness questionnaire: This assessed how useful a participant would find each televideo technology to contact various people or places using a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). Televideo features questionnaire: This assessed what features participants found to be most important when using televideo technologies. Televideo familiarity and use questionnaire: Adapted from Smarr et al.,
30
this assessed participants’ experience with various televideo technologies using a five-point Likert scale (0 = not sure what this is, 1 = never heard about, seen or used this technology, 2 = have only heard about or seen this technology, 3 = have used or operated this technology only occasionally, 4 = have used or operated this technology frequently).
A few concluding interview questions were asked at the end of the study about participants’ perceptions of televideo technologies, in general. However, only the results from the opinions questionnaires and the interview data pertaining to perceptions of usefulness, benefits, and concerns will be presented below as they directly address the goals of this paper. Interviews lasted approximately 2 h, and participants were compensated $30 for their time. Interviews were audio recorded and professionally transcribed for analysis.
Results
Overview of quantitative analysis
We collected quantitative data on participants’ acceptance of the three televideo technologies. The opinions questionnaires each comprised six questions pertaining to perceptions of usefulness and six questions pertaining to perceptions of ease of use, 20 for each of the televideo technologies. The data were analyzed using SPSS/Excel to calculate frequencies and descriptive statistics.
Quantitative findings: Perceptions of usefulness and ease of use
We evaluated participants’ ratings of perceived usefulness and ease of use for each technology because these two variables are highly predictive of technology acceptance.
20
The quantitative data from the [Skype, Kubi, Beam] opinions questionnaires showed that participants were generally open to accepting televideo technologies. The overall median score for perceived usefulness was 5 (slightly likely) and the overall median score for perceived ease of use was 6 (quite likely; see Figures 2 and 3, respectively, for response frequency data). Although these data are informative in that they indicate participants’ positive perceptions of televideo technologies, they do not provide insight into what beliefs and attitudes are driving those perceptions. To gain those insights we look to the qualitative data.
Frequency of responses for perceived usefulness subscale of the Telewellness technology opinions questionnaires by televideo technology. Frequency of responses for perceived ease of use subscale of the Telewellness technology opinions questionnaires by televideo technology.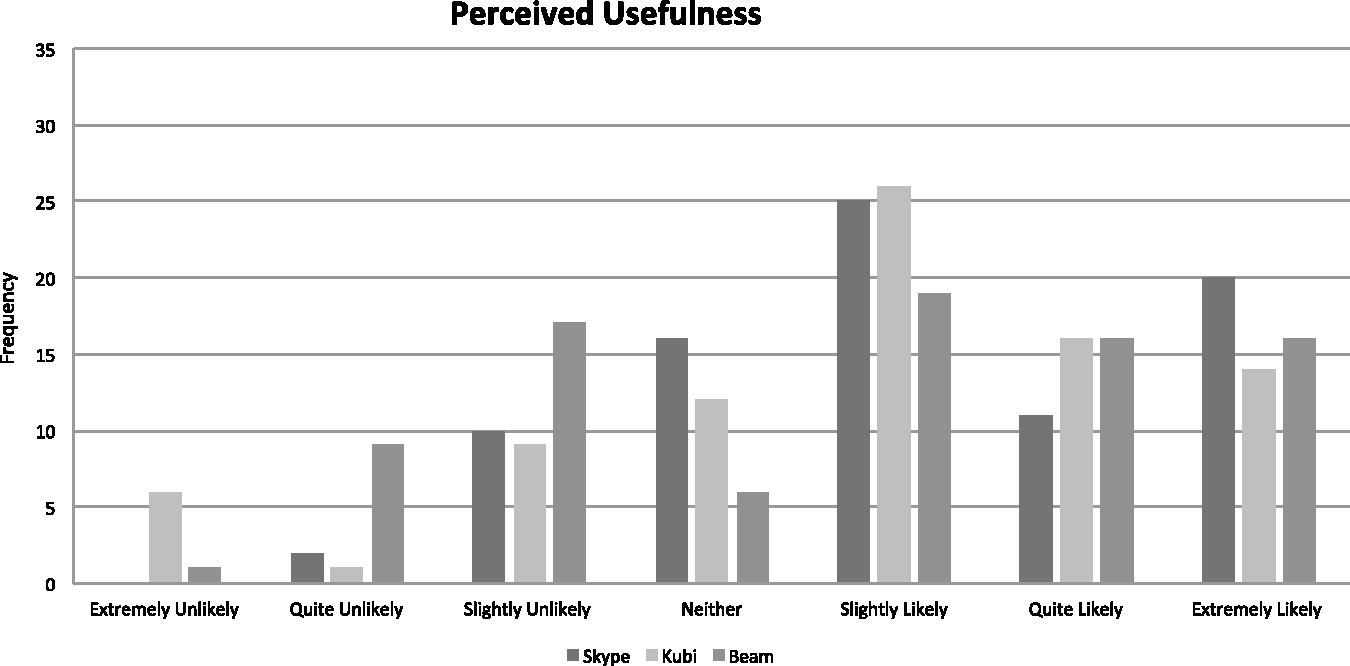

Overview of qualitative analysis
In the interviews, we asked participants about their attitudes regarding using televideo for three domains (social engagement, healthcare provider access, physical activity). Many of the themes identified in the interview data were similar across these domains, thus we will report the data collapsed across domains first and then report domain-specific attitudes. We also asked participants about three different televideo technologies (Skype, Kubi, and Beam); these data are presented together when the patterns were similar and separately when the patterns were different.
Interviews were segmented into units of analysis by one coder to ensure consistency of segmenting across transcripts. A segment was defined as a participant’s complete response to a question (including any responses to follow-up questions relating to the initial question). The coding scheme was based on earlier research on older adults’ acceptance of technology in general, 21 as well as acceptance of telepresence and televideo technologies.31,32 Additional codes were added following a thematic analysis to reflect categories that emerged from the data. Therefore, a combined top-down and bottom-up approach was used to develop the final coding scheme (available upon request).33,34 Each segment (herein referred to as a “response”) was coded on the following dimensions: technology discussed, domain discussed, and concern or benefit.
Three rounds of independent coding on the same three transcripts were conducted to calibrate the three coders. Any discrepancies between the coders were discussed and necessary revisions to the coding scheme were made. The final round of coding yielded interrater reliability of 89% agreement. The remaining transcripts were divided among the three coders to code independently.
Qualitative findings: perceptions of usefulness
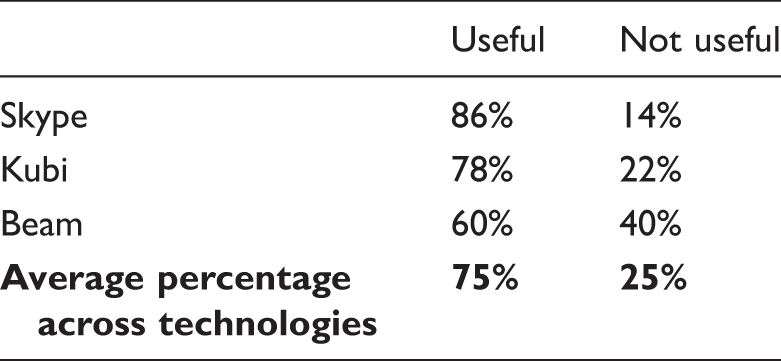
Percentage of responses coded as useful and not useful (total responses = 106).
Benefits
In addition to asking participants if they thought the technologies would be useful, we asked about the benefits they perceived for televideo use. The patterns of perceived benefits were similar across technology, hence the benefits will first be discussed collapsed across technology. Some of the responses (10% of all benefit responses) across all three technologies were general positive statements such as “I think it would be fun. It would make the experience more enjoyable.” and “I think it’s a great idea.” Across all technologies the most frequent specific benefit reported was visualization (see Figure 4). The visualization category included positive responses about being able to see the other person or something else in their environment, or feeling a sense of presence (accounting for 35% of all benefit responses). Examples of statements about the benefit of visualization include: “There’s always a better connection with people when you can visually see them and you’re talking to them. So, it just makes that connection stronger.” and “…I could be present with family. I could see my brother, his wife, their two children, all at once…It would mean a lot.” These statements exemplify participants’ positive attitudes towards being able to see who they are talking to and enable them to feel present and connected even though they are remotely located.
Percentage of benefit responses per category (collapsed across all three televideo technologies; only included codes that captured at least 5% of all benefit responses). Percentage of concern responses per category (collapsed across all three televideo technologies; only included codes that captured at least 5% of the concern responses).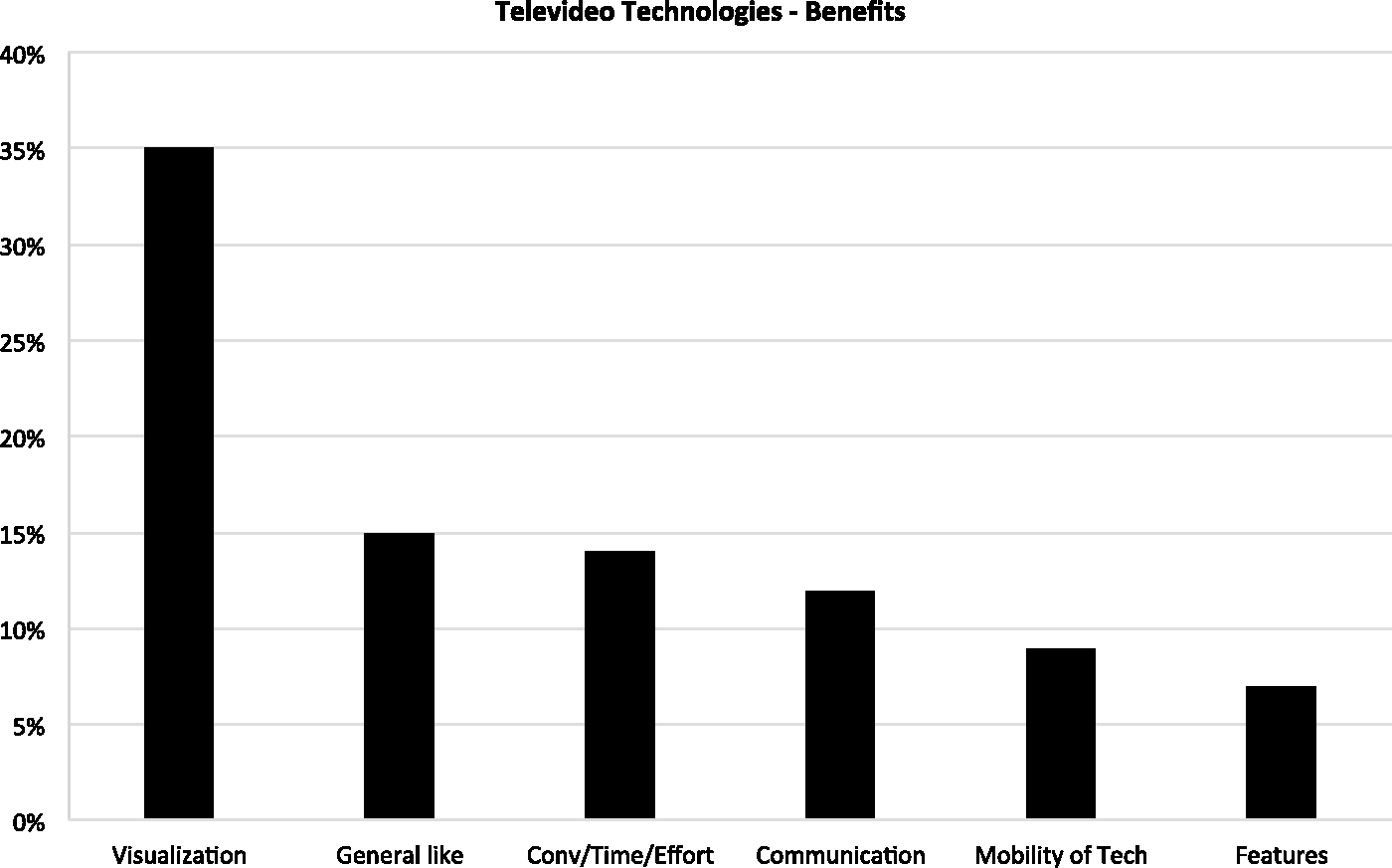

Additional benefits were reported, including convenience/time/effort, communication, mobility of the technology, and features. However, these categories were reported less frequently than visualization (each category accounted for less than 15% of all benefit responses). The convenience/time/effort category included responses about the technology making life easier in some way by saving effort or time or by allowing a task to be accomplished from home. Examples of the convenience/time/effort perceived benefits include: “Sometimes getting to the doctor’s office isn’t conducive to my day, so being able to do it from my office or home would make it a lot easier.” and “You would be able to see the people do the exercise and be able to mimic what they’re doing, so I would think that would be the useful thing. And you wouldn’t have to travel so you would save on gas.” The communication benefits mentioned were mostly general comments about televideo enabling or enhancing communication, such as “…I could see where it could enhance communication.” The mobility category included comments about the ability to move and control what they see in the video, for example “the ability to move yourself…around the room as you’re talking to someone…who wants to describe things, show you things. I thought that was really neat technology.” Comments were also made about the technology’s beneficial features; that is, the technology’s physical/interface properties such as “It’s hand free and it looks like it’s on eye level so you could see it easily.” Together, these data show that participants perceived a variety of benefits of use across the three televideo technologies, including convenience and time and effort savings, enhanced communication, the ability to control the view of their video (i.e., mobility) and the features of the technology. Nevertheless, participants focused most on the benefits of visualization, including being able to see the person they are talking to (e.g., their facial expressions) and that person’s environment.
Although, the pattern of benefit category frequencies was similar across all three technologies (Skype, Kubi, Beam), there was an exception for the mobility category. Mobility was perceived as a benefit of using Kubi (8% of all Kubi benefit responses) and Beam (21% of all Beam benefit responses), the two technologies that had mobility functionality. For example, when observing how the Kubi worked a participant noted, “…I liked the way when you’re with a group it revolves so that everybody can participate.” With respect to Beam a participant stated, “…it gives you more control of viewing things on the other side…the remote [side]. Me being the remote person dialing in then they can…move around more where [for] the Kubi…once you put [it in] the stand there you just have the 360 versus [Beam] where you can move from room to room if possible. That’s more virtual than the Kubi.” These quotes demonstrate how the added functionality of mobility was seen as a benefit to some because it offers greater control to visualize the remote environment. Not surprisingly, mobility was not mentioned as a benefit of Skype. This finding provides evidence that the participants indeed understood that Skype did not offer this functionality.
Concerns
Despite evidence of openness to accepting these televideo technologies and a greater number of benefits reported by participants as compared to concerns, participants did report concerns to televideo use. In fact, although there were fewer concern responses, they were more varied in content, as compared to the benefits. That is, the number of categories for concerns (10 categories each accounted for at least 5% of all concern responses) was greater than the number of categories for benefits (6 categories each accounted for at least 5% of all benefit responses).
We found a similar pattern of concerns across all three technologies (Skype, Kubi, Beam), therefore we will first discuss the data collapsed across technology. Across all three technologies participants reported a wide variety of concerns (see Figure 5), with the most frequently reported concerns being privacy/security (20% of all concern responses), ease of use (17% of all concern responses), and use by others (11% of all concern responses). Privacy/Security responses included concerns about invasion or breach of privacy, exposure of one’s personal information/surroundings/life, lack of security, exposure to a computer virus, and misuse of technology to gain sensitive information or incur harm. Privacy and security concerns included: “My main concern is the security. Because like I said you don’t want anybody and everybody having access to it.” and “My concern is… the privacy issue. Because you got so many hackers out there on the Internet that they can get into your account and get all your information and they can also get your friends’ and family information.” Ease of use was the second most frequently mentioned category of concern. The ease of use category included comments about the ease with which participants thought they could interact with the technology and do what they wanted to do with the technology (e.g., easy to control and operate). Examples of ease of use concerns include: “It would just get real tricky. I worry that I wouldn’t feel comfortable. I don’t know why. Maybe it’s just because I’m not a super high-tech person. It just doesn’t appeal to me.” and “To me it’s cumbersome in learning it and getting used to it.” Use by others was the third most frequent concern category and was defined as concerns about other people owning or being able to use the system. Use by others concerns included: “And then my concern would be, so many of my friends are not computer literate. So they might have a problem with doing it.”
Below is a list of some of the less frequently mentioned concerns (each category accounted for less than 9% of all concern responses):
Etiquette: “You need to be dressed [and] you need to be presentable when you use Skype.” General dislike: “It would be boring.” Lack of presence: “My preference is person to person, face to face. I just think there’s more power in it in terms of engagement.” Time/effort: “To me it just entails more work.” Mobility: “[It is a concern] physically. Since it moves around I would have to practice with it so I don’t run into it or it doesn’t run into me.” Technical difficulties: “The technology isn’t perfect yet in that it’s sort of jerky sometimes and it freezes sometimes.”
In sum, despite a wide range of concerns identified in participants’ responses, the most frequently reported concerns were that televideo technologies lack of privacy/security, may be difficult to use, and may not be owned or used by people with whom the user would like to communicate.
Although a similar set and frequency of concern categories were reported for all three technologies there were some technology-specific findings. Just as Kubi and Beam’s mobility was seen as beneficial, participants also expressed concerns about the technology mobility. For Kubi one participant stated, “As far as rotating side to side, most people don’t like that. You know, because who wants to be changing their eyes and moving around with the screen when you’re trying to keep the focus on somebody.” And for Beam, a participant said “I have concerns about it really working smoothly [and] getting around obstacles.” For Beam participants also noted concerns that it could damage them or their environment (e.g., “I think I would have a concern then cause as I’m exercising and moving around, my concern would be am I going to knock it over you know or damage it in some kind of way. That would be my concern.”). Again, concerns about mobility were only expressed for Kubi and Beam, as Skype does not have that functionality.
Domain specific benefits and concerns
While overall patterns of benefits and concerns (i.e., category frequencies) were similar across the three domains, some of details of the benefits and concerns mentioned were specific to the context of a particular domain. For social engagement, participants focused on the benefit of enhanced communication for people who are remotely located (e.g., “You can reach anybody anywhere in the country.”), and the “enhanced” and “enriched” experience of being able to see the facial expressions of the person with whom they are communicating (e.g., “I think it would be good that you would be able to see people’s expression and their voice, emotions and that type of thing.”). For physical activity, participants honed in on the benefit of being able to follow or “imitate” an instructor better by seeing visual cues (e.g., “You could just see what the other person is doing more and try to follow their lead. Now I take physical therapy one day a week locally here and that’s proved to be useful, so this probably would [be] too.”) Participants also commented on the benefit of being able to access an instructor/physical therapist who would have knowledge and training about working with people who have physical limitations (e.g., “I would hope if I was able to get it on Skype I would be in touch with someone who knew the physical limitations of the handicap that I have and therefore they would [demonstrate an exercise] that I could do rather than just in general that everyone [else] could do.”) With respect to healthcare provider access, participants noted the benefit of being able to show their doctor something remotely rather than having to go to their office (e.g., “It would eliminate travel and take less time out of your day.”). While many participants did not see this as a replacement for in-office visits (e.g., “I think it’s hard to substitute this for face-to-face interaction, especially if there’s something that needs to be clearly seen and evaluated.”), they did view it as an alternative for less urgent issues (e.g., “I think it would be useful when I have questions that don’t necessitate me going to the office. I mean if I had questions about medications or my symptoms or if I should even make an appointment or that type of thing.”).
Participants noted concerns that were specific to a domain, as well. For social engagement, participants expressed concerns about having to be presentable and avoid distractions, such as “You’ve gotta be kind of in a good place, you need to be dressed or at least presentable. You need to…limit distractions that are going on behind you…I wouldn’t want to talk to them in the middle of grand central station.” For physical activity, participants discussed concerns of televideo use causing damage or harm to themselves or something in their environment, such as “The only thing that I would be concerned about is that I would be paying attention to the video and drop something or roll over something and fall out of my chair or be trying to do a move and watch the video and try to do this move and really pull a muscle or you know have an accident.” For healthcare provider access, participants were concerned about the lack of presence and in person contact, such as “[The healthcare provider] could advise you on what he or she would want you to do as far as the illness is concerned, but as far as getting the diagnosis right you need to…have person to person contact.” These examples provide insight into some of the reasoning driving participants’ perceptions about televideo use in different contexts.
Discussion
The goal of this paper was to evaluate televideo acceptance by adults aging with mobility impairments in the context of health and wellness (i.e., social engagement, healthcare provider access, physical activity). We examined participants’ attitudes toward three televideo technologies that varied in their mobility to explore acceptance issues generally, but also issues that may be specific to televideo technologies with mobility functionality. We assessed perceptions of usefulness and ease of use, as well as other benefits and concerns regarding using televideo technologies for social engagement, healthcare provider access, and physical activity. Participants were generally open to accepting televideo technology, as reflected by their ratings of perceived usefulness and ease of use, and the benefits of televideo use they identified. However, participants also voiced concerns about using televideo technologies. Our findings provide evidence that televideo technology does have potential to be adopted by adults aging with mobility impairments. Yet, adoption may be facilitated by considering the details of this potential user groups’ perceptions about benefits and concerns when developing televideo systems and televideo-based interventions.
It is important to understand how potential users view a technology with respect to its usefulness, as well as other benefits to its use. Older adults have been shown to be benefit-driven in their acceptance of new communication technologies. 22 The perception of a technology as being useful is especially important given that perceived usefulness is a predictor of technology acceptance. 20 It is critical that potential users can envision an application for a technology that serves a meaningful purpose in their life. When asked about the usefulness of televideo technologies, participants in this study were largely positive, endorsing the usefulness of all three televideo technologies for engaging in social engagement, healthcare provider access, and physical activity.
Participants perceived other benefits of the technologies, in addition to usefulness, predominantly focusing on the benefit of visualization. Visualization was discussed positively across all three technologies as providing a feeling of ‘being there’ and enabling someone to see the facial expressions and environment of another person who is remotely located. Visualization via the technology’s two way audio and video functionality has been identified in previous studies as a benefit of televideo technology.31,32,35 Another benefit discussed across all three technologies was that televideo technology would be convenient, time-saving, and/or effort-reducing. This finding is consistent with previous research showing that older adults focus on convenience issues when discussing the benefits of technology. 21 The perception that televideo technology enhanced communication was also discussed as benefit across all three technologies. These findings suggest that interventions that use televideo technologies should highlight the visualization, convenience, and communication enhancing qualities of these technologies in promotional, educational, and training materials.
Although the majority of participants’ comments focused on the benefits of televideo technologies, a wide range of concerns were discussed across all three technologies. The most frequently mentioned concerns across technologies were perceptions about lack of privacy and security, the difficulty of using these technologies, and the possibility that the person they wanted or needed to contact would not have (or able to use) the corresponding technology. Participants’ concerns about security are consistent with previous research about what older adults dislike about technology. 21 Televideo technology interventions, therefore, should address these concerns directly in the design of the technology (e.g., added privacy features, encryption software). In addition, privacy and security education should be included in training materials to provide guidance about how to optimize privacy and security and to clarify possible misconceptions.
Despite general consistency across technologies regarding the benefits and concerns noted by participants, there was an exception with the category of mobility. Mobility was mentioned as a benefit and a concern when participants were discussing Kubi and Beam (note: Skype does not have the functionality that allows someone to control the camera on the remote device). For Kubi and Beam, participants perceived mobility as beneficial for allowing the remote user more control of what they are viewing in the remote space. The concerns about mobility focused on the difficulty of viewing/tracking a moving image and potential dangers of the technologies colliding with themselves, their wheelchairs, and items in their homes. The findings regarding concerns about collision and obstacle avoidance are consistent with earlier research. 36 It should be mentioned that these concerns arose despite the fact that the video shown to participants about Beam specifically referenced its collision avoidance features. Hence, televideo technologies should not only include collision avoidance as a feature, but also provide the necessary education about how this feature works to allow users to ensure their own safety and the safety of their environment.
We found generally consistent patterns of benefits and concerns for using televideo in the context of social engagement, healthcare provider access, and physical activity. However, some of the details or reasons behind the perceptions were domain-specific. For example, visualization was the most frequently mentioned perceived benefit in all three domains yet the specific reason(s) driving that perception varied. In the context of social engagement, participants focused on how visualization allowed the exchange of facial expressions, whereas in the context of social activity participants focused on how visualization enabled an individual to follow an instructor better by seeing visual cues. In the context of healthcare provider access, participants focused on how visualization allowed patients to show their doctor something remotely (e.g., a symptom). Participants also expressed some concerns that were domain-specific. In the context of social engagement, participants were particularly concerned about having to be presentable and avoid distractions while using televideo technologies. In the context of physical activity, participants made specific note of their concern for physical harm trying to use the televideo technology at the same time as making physical movements. In the context of healthcare provider access, participants focused on the importance of having a physical encounter with their physician and therefore were concerned that televideo lacked in-person presence and contact. These details regarding benefits and concerns should be considered when designing televideo interventions for improving social engagement, healthcare provider access, and physical activity for adults aging with mobility impairments.
We were able to gather rich details about participants’ attitudes about televideo technologies by employing a qualitative approach. Although these details provide many important insights, larger scale research is needed to understand how attitudes may differ based on variables such as participant demographics and technology experience. Usability research is also needed with this population to better understand facilitators and barriers to the use of televideo technologies by adults aging with a mobility disability. In the present study, participants observed videos of the capabilities of three televideo technologies. As a next step for this area of research, it will be important to have adults aging with mobility impairments use these technologies for health and wellness applications and assess if those interactions affect their attitudes.
We assessed acceptance of televideo use in the context of health, social engagement, and physical activity because televideo may be valuable for delivering interventions to adults aging with pre-existing mobility impairments in these domains. Individuals with mobility impairments can face barriers to participating in these activities in person. Such barriers include lack of transportation and lack of accessibility. 10 Televideo technologies may be able to bridge some of these barriers but they can only do so successfully if they are adopted by the end users. Our findings shed light on overall acceptance issues of televideo technologies by older adults with mobility impairments.
Conclusion
Televideo systems and televideo-based interventions may be particularly beneficial to adults aging with a mobility impairment, as these technologies may help to reduce participation barriers (e.g., social engagement, healthcare provider access, physical activity). Our findings suggest that this population may be open to accepting televideo technology for use in health and wellness applications. To facilitate acceptance and adoption of these technologies the following recommendations should be considered when deploying them for use by adults who are aging with a disability:
Education materials
Highlight the benefit of visualization for providing a feeling of “being there.” Highlight the benefit of convenience for facilitating remote communication, such as when transportation is not safe (e.g., icy conditions) or available. Provide information about privacy and security safeguards (dispel any misconceptions). Discuss how to use the technology safely (e.g., avoiding distractions and collisions).
Training
Demonstrate use and provide opportunity for potential user to participate in a demonstration trial in which they can experience seeing the remote user as well as the remote environment. This experience will likely enable the potential user to understand how televideo can enhance communication. Provide basic training for using the televideo technology. A Quick Start Guide may be useful for overcoming any initial usability barriers. Provide training focused on advanced driving features, such as obstacle avoidance. Provide guidance about how to optimize privacy and security.
These recommendations provide direction for improving the design and facilitating the deployment of televideo interventions for adults aging with mobility impairments. Future research is needed to assess usability of televideo technologies by this population, particularly for health and wellness applications.
Footnotes
Acknowledgment
The authors wish to thank Lawrence Chan for his assistance with data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institute on Disability, Independent Living, and Rehabilitation Research (Department of Health & Human Services, Administration for Community Living) (grant number 90RE5016-01-00) under the auspices of the Rehabilitation and Engineering Research Center on Technologies to Support Successful Aging with Disability (TechSAge; ![]() ). The contents of this paper were developed under a grant from the Department of Health & Human Services, Administration for Community Living. However, those contents do not necessarily represent the policy of the Department of Health & Human Services, Administration for Community Living.
). The contents of this paper were developed under a grant from the Department of Health & Human Services, Administration for Community Living. However, those contents do not necessarily represent the policy of the Department of Health & Human Services, Administration for Community Living.