
Abstract
Background
Body weight supported treadmill training (BWSTT) has been proven to be effective in rehabilitation of persons with cerebral palsy (CP). However, it has still not found widespread usage, especially in industrially developing countries, due to its high cost. Treadmill training promotes a rhythmical movement of the lower extremities through motor learning, which can be enhanced by BWSTT for persons with CP. Hence, the research and development team of a tertiary level neuromusculoskeletal rehabilitation center designed a low-cost body weight support training (BWST) device. The aim of this study was to evaluate the effectiveness of the BWST device on gait and ambulation in persons with CP post single-event multilevel surgery (SEMLS) of the lower extremities.
Method
A randomized controlled trial was conducted in 50 persons with CP aged between 5 and 20 years, who underwent a type of SEMLS called single-event multilevel lever arm restoration and anti-spasticity surgery (SEMLARASS). They were randomly assigned to two groups: group A (n = 25) received gait training and treadmill training with the BWST device, and group B (n = 25) received gait training and treadmill training without the BWST device. The designed BWST device was manually operated and based on an un-weighing principle in which a vest of different sizes un-weighed 10–30% of the individual’s weight transmitted to the ground by means of adjustable counterweights fixed on a movable metallic frame which had an adjustable top lever (holding the vest) and a handle bar for the patient to hold. The entire cost for the finished BWST device was estimated around 700 USD. The study duration was 5 weeks with 1 h of intervention per day for 6 days per week. Physician Rating Scale (PRS), Dynamic Gait Index (DGI) and Functional Mobility Scale (FMS) were the primary outcome measures.
Results
Group A showed significant positive differences in the scores of PRS (p < 0.001), DGI (p < 0.001) and FMS (p < 0.01) when compared with group B, 5 weeks after the intervention, and the results were maintained at a follow-up of 12 months.
Conclusion
The low-cost BWST device was found to be clinically effective in improving gait and ambulation in persons with CP following SEMLARASS.
Introduction
Positive outcomes of using BWSTT.

Recent systematic reviews of BWSTT in children describe weak evidence with no reported randomized clinical trials.6,8,9 However, the evidence for BWSTT varies by diagnosis, with the strongest evidence suggesting positive outcomes in children with Down syndrome and limited evidence for children with CP.10–16 The limitations of BWSTT include the high cost of equipment and being labor intensive, usually involving two or three staff. Companies such as Biodex, Lode, Glidetrak, LiteGait, Second Step and Rifton sell BWSTT devices at a cost ranging from around USD 10,000 to USD 15,000. The treadmill and body weight suspension system alone may cost up to a maximum of USD 180,000. 17 The outcome of two systematic reviews conducted in 2009 also confirmed the above factors, along with the need for large-sized randomized controlled trials.6,8 Single-event multilevel surgery (SEMLS) refers to the correction of all orthopedic deformities in one session, which has the advantage of requiring one hospital admission and one period of rehabilitation.18,19 BWSTT is one of the most common gait training programs followed in the rehabilitation period post SEMLS. 20 However, no studies have been reported yet in the literature studying the effectiveness of BWST among persons with CP after SEMLS. Hence, the objective of our study was to develop a BWST device at low cost and to evaluate its effectiveness among persons with CP after SEMLS on the parameters of gait and ambulatory function.
Methodology
A randomized controlled trial was conducted among 50 children and adolescents with CP, from a single multidisciplinary rehabilitation center, who were in their post-operative rehabilitation period after SEMLS. The SEMLS was more specifically called single-event multilevel lever arm restoration and anti-spasticity surgery (SEMLARASS). The surgical procedures included intramuscular release and controlled tendon lengthening using the principles of orthopedic selective spasticity control surgery and simultaneous restoration of lever arm dysfunctions, which was followed by plaster immobilization of both lower limbs for 6–10 weeks, and then protocol-based, sequenced multidisciplinary rehabilitation. 20
Selection criteria
The inclusion criteria for the study were as follows: (a) male or female gender, (b) age 5–20 years, (c) diagnosis of spastic or dyskinetic CP, (d) participants post SEMLARASS were in the ambulatory phase of rehabilitation, (e) able to understand commands, (f) GMFCS level 3–5 before SEMLARASS, (g) no other previous orthopedic or neuro surgeries, (h) no previous treatment with botulinum toxin injections or other types of invasive treatments.
Intervention program
After providing informed consent, the participants were randomly assigned to group A (experimental) and group B (control) based on a computer-generated permuted allocation of 25 children in each group. The experimental group underwent the gait training program over-ground and on the treadmill with the low-cost BWST device, whereas the control group underwent the same training program without the BWST device. The training was given for 1 h per day for 6 days in a week, for a total of 5 weeks. The methodology is described in Figure 1, which shows the flowchart of the study process. The gait training protocol provided for both the groups is displayed in Table 2.
Flowchart of the study participant selection process. Gait training protocol provided for the experimental and control group.

Construction of the low-cost BWST device
The BWST device was constructed with stainless steel (SS), and was designed by some of the authors and constructed by a rehabilitative and assistive devices manufacturer who had experience in making various rehabilitation devices with SS material. The entire cost of the finished BWST device was approximately 700 USD. The BWST device consisted of the following components, shown in Figure 2, showing the lateral view of the BWST device with a suspended model: vertical SS frame (a), which was fixed to a 3-sided platform base (b). There were two movable segments which ran up and down on the vertical SS frame: segment 1 (c) overhead top lever system (refer to Figure 3, showing the top view of the overhead system): Y-shaped (the width of the “Y” spanned the average shoulder width such that the user, after suspension, remained un-twisted) adjustable recoiling top lever to which the loaded weights were suspended by a metallic rope which ran through a pulley fitted at the top end of the vertical SS frame, and segment 2 – (d) Y-shaped adjustable handle bar or hand rail. The other external components were (e) body vest (available in three different sizes) for holding and suspending the patient with the top lever by means of dog clips and (f) removable weights of 500 g per unit which could be added up based on the user’s body weight.
Lateral view of the BWST device with a suspended model. Top view of the overhead system of the BWST device.

Measurements of the low-cost BWST device
The measurements (refer to Figure 2 and 3) of the BWST device are as follows: (a) to (b) (distance of the pulley bar which holds the overhead pulley to the vertical frame) = 14 cm; (b) to (c) (distance between the top to bottom of the vertical frame) = 158 cm; (c) to (d) (ground clearance distance from the bottom of the vertical frame, which is fixed to the platform base to the floor) = 15 cm; (e1) to (f1) = (e2) to (f2) (distance of the horizontal bars of the platform base) = 120 cm; (e1) to (e2) = (f1) to (f2) (clearance distance between the two horizontal bars of the platform base) = 80 cm; (g1) to (h1) = (g2) to (h2) (distance of the length of the hand rails) = 95 cm; (i1) to (j1) = (i2) to (j2) (distance of the long stem of the Y-shaped overhead system) = 55 cm; (k1) to (l1) = (k2) to (l2) (distance of the short extended split stem of the Y-shaped overhead system) = 28 cm; (k1) to (k2) = (l1) to (l2) (clearance distance between the two short extended split stem of the Y-shaped overhead system) = 35 cm; the breadth and width of the vertical frame is 10 cm × 10 cm; the breadth and width of the overhead and platform horizontal bars are 5 cm × 2.5 cm; the breadth and width of pulley bar is 14 cm × 2.5 cm; the diameters of the hand rail and the rod connector from the vertical rod to the platform base are 8 cm.
Specific features of the low-cost BWST device
Key factors of the BWST device.

Assistance requirements in the low-cost BWST device
Assistance by physiotherapists was required in training to facilitate correct kinematics for swing and stance. One therapist usually stood behind the participant, to facilitate trunk alignment (trunk and hip extension) and weight shifting. The second therapist or caregiver sat beside the participant to facilitate the knee and foot position for weight bearing or limb loading and swing during stepping of the legs, to ensure heel strike at initial contact and prevent knee hyperextension. A third person or assistive straps might be required to support hemiplegic arm or assist with trunk control.
Outcome measures
The outcomes of control group and experimental group were measured before and after the 5 weeks of intervention. A follow-up measurement was performed 12 months after the intervention. The outcomes measures used were the Dynamic Gait Index (DGI), Physician Rating Scale (PRS) and Functional Mobility Scale (FMS). DGI measures the mobility function and dynamic balance in walking and stair climbing. There are eight items on the DGI and each item was scored on a 4-point scale as (3) Normal; (2) Mild impairment; (1) Moderate impairment; (0) Severe impairment, with a maximum score of 24. The eight items include walking, walking with speed changes, walking with vertical and then horizontal head turns, walking with a quick pivot stop, walking over objects, walking around objects and walking up and down stairs. 24 PRS is an observational clinical evaluation of gait in the sagittal plane on the parameters of foot contact, crouch, hip flexion, knee flexion and dorsiflexion.25,26 The FMS is a six-level clinician-administered self-report ordinal scale that rates mobility within the different environmental settings of the home, school and community based on the assistance persons with CP require. 27
Statistical analysis
Descriptive statistics were reported using mean and 95% CI for continuous variable and numbers and percentages for categorical variables. Independent t-test and paired t-test were used to analyze the significant difference between and within the experimental and control before, after 5 weeks and 12 months of intervention. A p-value less than 5% was considered statistically significant. The data were analyzed using SPSS version 17.
Results
Mean age and weight of participants in the study.

Frequency distribution of demographic profile of the participants.

VDRO: varus derotation osteotomy; FDRO: femoral derotation osteotomy; OSSCS: orthopedic selective spasticity control surgery
Mean scores of all the outcome measures used to examine the BWST device.

Independent t-test between the experimental and control group on all the studied outcome parameters.

Denotes highly significant difference
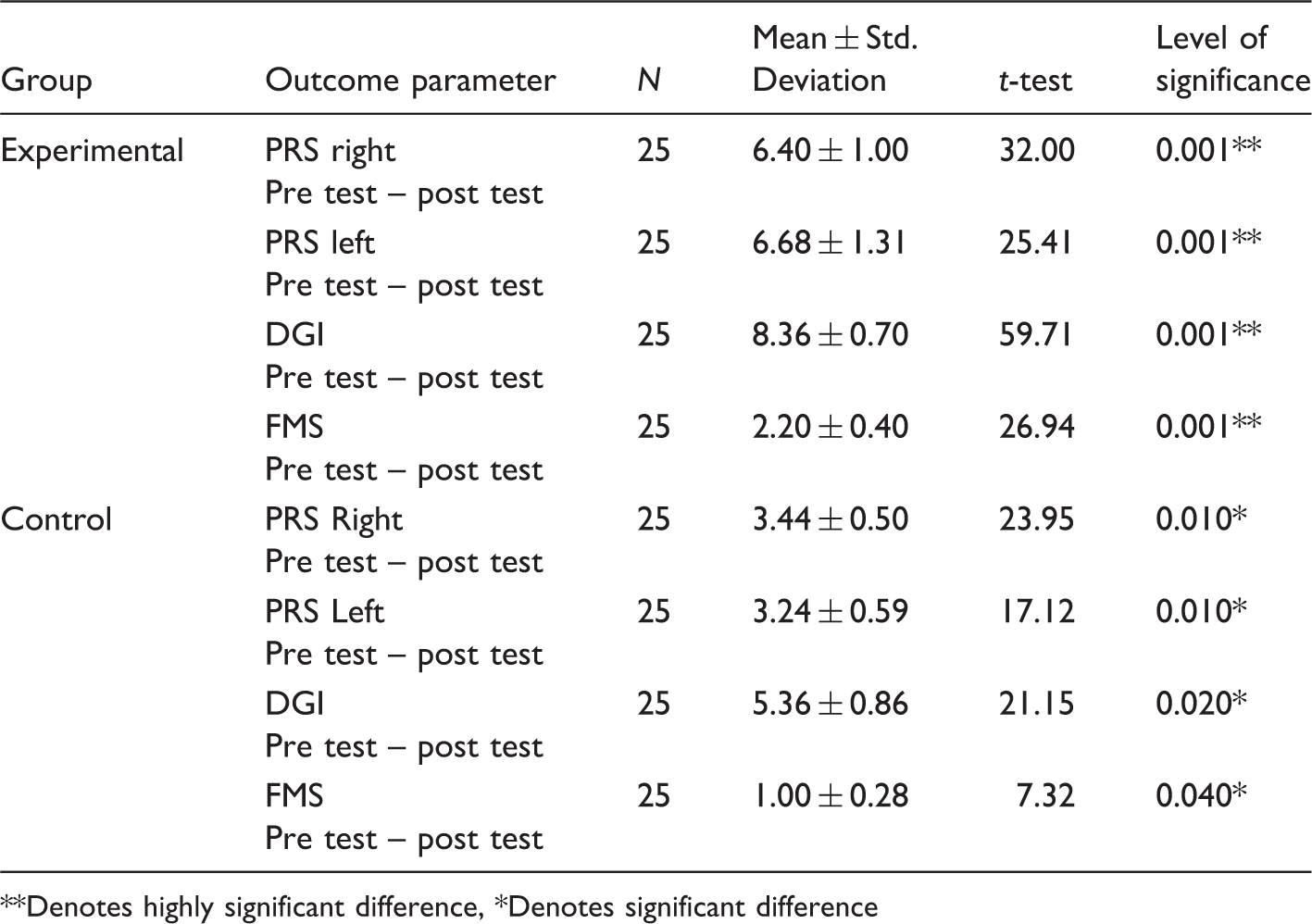
Paired t-test between pre test and post test between the experimental and control group on all the studied outcome parameters.
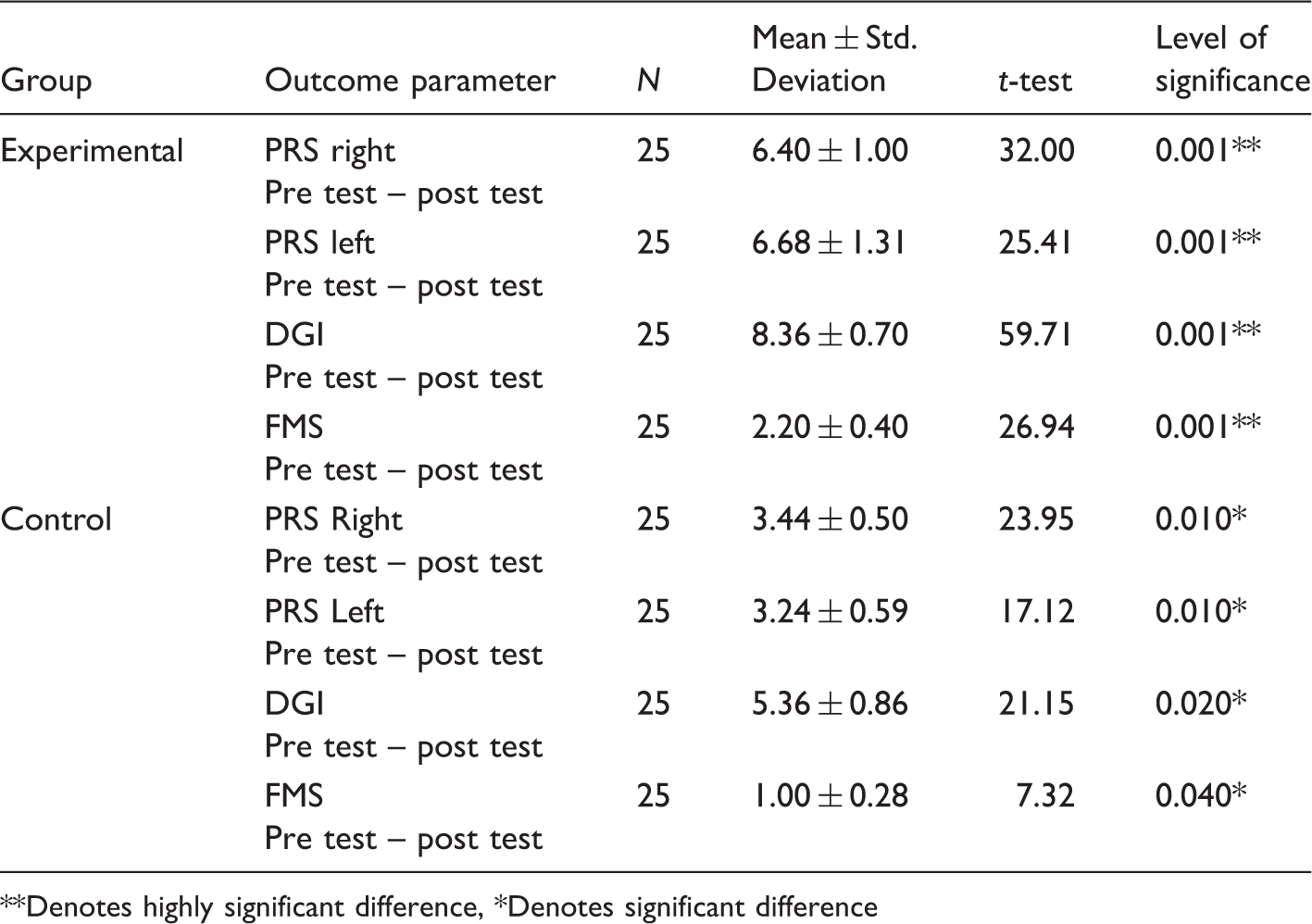
Denotes highly significant difference, *Denotes significant difference
Independent t-test between the experimental and control group on all the studied outcome parameters: follow-up test data.
Denotes highly significant difference
Paired t-test between post test and follow-up test between the experimental and control group on all the studied outcome parameters.

Denotes highly significant difference; NSDenotes no significant difference
Discussion
The addition of the low-cost BWST device to conventional gait and treadmill training provided significant improvements in the specific gait and mobility parameters when compared with conventional gait and treadmill training only. The maintenance of the positive outcomes for the participants who underwent BWST at a follow-up of 12 months showed that the effect of training was long lasting. The amount of weight used for unloading is dependent on the ability of the participant to carry body weight on the affected legs during single limb stance while maintaining proper trunk and limb alignment. Gradually, the unloading weight was reduced to reduce the support as the participant was able to tolerate loading the legs in stance without the knee buckling, maintaining the ability to swing the leg independently and maintaining hip extension in weight bearing.13,15,28,29 The speed of treadmill was kept as slow as possible in the initial phase to maintain the integrity of gait pattern, namely maintaining adequate step length and swing through, which was also supported by previous studies.6,8,16,23 The duration of treadmill training was not determined in previous studies. 8 In this study, the duration of treadmill training was set at approximately 30 min (in a 60-min session which included another 30 min of over-ground walking) with adequate breaks in between. Our BWST device had a handrail which has been shown to increase single limb support and improve gait symmetry, but ultimately the arms should swing as part of the normal gait pattern, as supported by previous studies. 28 This study further adds to the rationale behind the use of BWST for persons with CP and also describes specific protocol parameters, so that generalizing its use across different groups of persons with CP is possible.13–16 In contrast to an earlier study which suggested that self-selected over-ground walking tended to be the most functional for safety of an individual, our study observed that both over-ground and treadmill walking was functional and safe.29,30 The effectiveness seen for the group which used the BWST device in both over-ground and treadmill walking can be explained by earlier studies which reported that stretching the hip flexors in terminal stance activated the muscles and initiated the leg to come forward. In addition, the increased tension placed on the triceps surae muscle by loading the limb in mid-stance during BWST was also found in the cited studies to facilitate muscle activation.30,31 BWST has been reported to be beneficial as a treatment method because the movement of the lower extremities into extension facilitated by the treadmill assisted in stimulating a stepping response not elicited in an over-ground walking training. In addition, the upright and safe position of the participant achieved by the BWST device through the vest was not only functional, but it also allowed the physiotherapist to handle and guide the participants more effectively.6,9,21,32 Also, no accidental falls were observed during the training program for participants in the experimental group when compared with the control group, which highlighted the safety aspect of the BWST device, similar to previous studies.31,32 Safety is an important concern, especially in the rehabilitation phase of post SEMLARASS, because falls often lead to fractures due to low bone mineral density, and lead to a fear of walking.
The limitations of the present study are as follows. Firstly, as the adjustments (overhead system, handrails and counterweights) were done manually, and the manual effort of a therapist plus more than one further therapist or caregiver was needed for handling each participant. Secondly, other outcome measures of gait, balance, quality of life, functional outcomes and more detailed evaluation were not taken for the study. The limitations would be rectified in a future research study with a larger sample size and a longer follow-up. Further improvements in the present design of the BWST device can be developed with this study as a baseline, such as provisions for reducing manual effort for suspending the patient in the device, and shifting the vertical frame to the sides or to the back, which can help in cueing the patient to get the visual feedback from a mirror for better reinforcement and also would be useful in additional therapies, for example use of a visual display unit (incorporating BWST with a virtual reality-based therapy) or vibration plate (for whole body vibration therapy).
Conclusion
BWST was found to be effective in improving the gait and mobility parameters in persons with CP when compared with the group which did not use the BWST device. The low-cost BWST device helped improve both the over-ground and treadmill walking in the studied group of a population with ambulatory deficits.
Footnotes
Acknowledgement
We thank Dr. Esther Lydia, Loyola College, Chennai, India for the statistical guidance.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.