
Abstract
Background
Robotic-assisted gait training, a viable and promising therapeutic option for neurological rehabilitation, is not widely adopted in developing countries because of its high cost. In this paper, we describe the concept and construction of a low-cost robot prototype to restore walking ability in children with neurological dysfunction.
Methods
The proposed robot consists of an orthosis, a treadmill, a body weight support system and two ankle guidance systems that move the ankles along a physiological kinematic trajectory. The spatiotemporal gait parameters of 60 children with typical development and children with cerebral palsy (aged 7–10 years) were obtained through clinical tests and compared with those provided by the robot.
Results
The robotic orthosis presents normative values for stride length, step length and cadence during the typical development of children’s gait speed and allows speed adjustments according to the degree of neuromotor impairment.
Conclusion
The results evidence the high feasibility of developing a low-complexity rehabilitation device compliant with the physiological trajectory of the ankle as well as with several other physiological gait parameters.
Introduction
Children with cerebral palsy (CP) demonstrate gait impairment, which limits their participation in activities of daily living and consequently affect their social interaction.1,2 Gait training is an effective rehabilitation strategy for restoring the ability to walk, and training repetition and intensity crucially influence the motor learning outcomes of this approach. However, these factors are highly variable and are dependent on the individual attributes of therapists.3,4
Conventional gait training is strenuous for therapists; therefore, although patients benefit from long gait training sessions, the high physical demands of these sessions limit their duration. 5 Moreover, as each training session involves hundreds of step repetitions, facilitating symmetrical kinematic step patterns in both lower limbs becomes difficult for therapists. 6
The functional outcomes of conventional rehabilitation programs indicate that the intensity of these programs are inadequate for those with neuromotor dysfunction, including CP. 7 High-intensity and long-duration physical exercise is vital for obtaining satisfactory outcomes pertaining to the general health and in activities of daily living of patients with neuromotor dysfunction. 8
Several robotic devices have been developed to automate and improve gait training and to reduce the physical load on the therapist; these devices are ideal particularly for children whose brain plasticity it is at its maximum. However, the high cost of such devices is a major disadvantage, especially in developing countries, where few individuals have benefitted from these systems.9,10
This paper presents a low-cost rehabilitation robot for restoring the walking ability of children with neurological dysfunctions. The proposed robot is expected to realise robotic-assisted gait training in clinical practice in several developing countries, especially in Brazil.
Design requirements
The fundamental technical requirements of a low-cost gait rehabilitation robot include the development of a device for robotic-assisted gait training that has the following characteristics: the robot (a) can be attached to and synchronised with a treadmill; (b) enables the patient to perform a kinematic trajectory similar to the normal gait pattern; (c) maintains the gait phases (i.e. stance and swing phases) within the physiological range and (d) is affordable.
Design description
Mechanical structure
The hip–knee–ankle–foot orthosis is composed of aluminium uprights with a pelvic band, two articulations (one each at the hip and the knee) and a polypropylene ankle–foot orthosis that maintains the ankle joint in a neutral position (0° dorsiflexion and plantarflexion). The hip–knee–ankle–foot orthosis is connected to the patient through a pin located on the pivot point of the ankle at the level of the lateral malleolus.
The treadmill is synchronised with motors that drive the ankle trajectories, and treadmill speed can be set between 0–3.0 km/h, as recommended by the rehabilitation protocols for robotic-assisted gait training.2,7,11
The body weight support system can be set to support various levels of body weight. This system supports patients by using a harness pulled upwards by a cable that connects to a pneumatic device.
The ankle guidance systems, one for each lower limb, control the ankle’s kinematic trajectory. Each system comprises a cam system, a pull chain, an electric motor, a sprocket that moves the chain, and sensors that determine the beginning and end of the gait phases and consequently the change in speed.
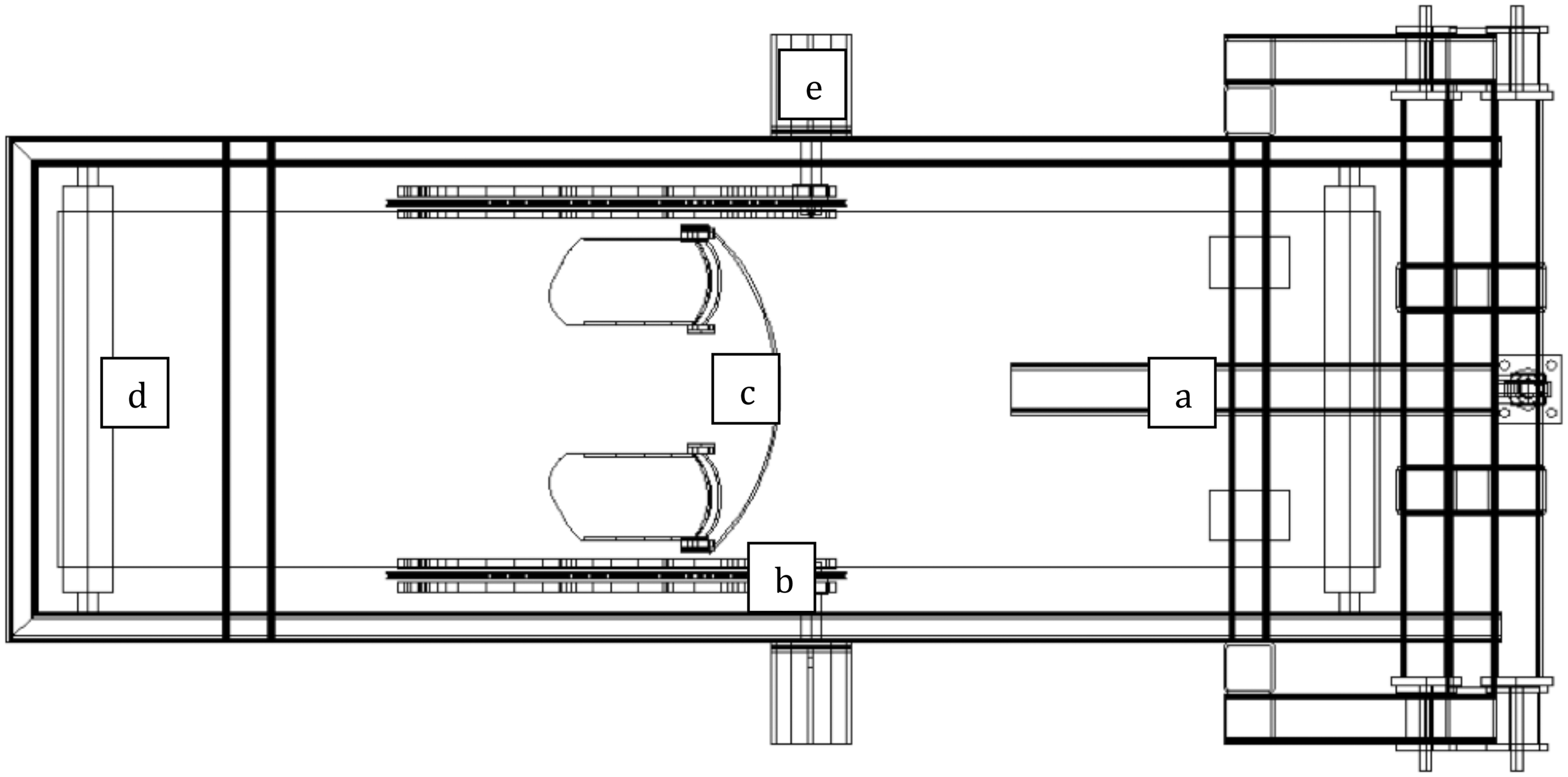
Figures 1 and 2 illustrate the lateral and top views of the device and its components, respectively.
Schema of the lateral view of the device and its components: (a) body weight support system and pneumatic cylinder; (b) ankle guidance system; (c) orthosis for lower limbs; (d) treadmill and (e) gear motor attached to the ankle guidance system. Schema of the top view of the device and its components: (a) body weight support system and pneumatic cylinder; (b) ankle guidance systems; (c) orthosis for lower limbs; (d) treadmill and (e) gear motor attached to the ankle guidance systems.
The cam system is a track for the chain and is designed to reflect the physiological trajectory of ankles of children aged 7–10 years. The determination and description of this trajectory on a treadmill for healthy adults is described in the literature. 12
According to Ganley and Powers,
13
the gait kinetic and kinematic parameters of a 7-year-old child are similar to those of an adult and differ only in the movement generated by the ankle; this is due to anthropometric differences. Hence, although the ankle kinematic trajectory for children is not described in the literature, given the similarity of the kinematic patterns of a child and an adult, the trajectory can be derived from the step length of children aged 7–10 years (see Figure 3). The step length of children aged 7–10 years has been reported to be 0.43 ± 0.04 m;
14
hence, the step length of the device was set at 0.429 m.
Ankle joint trajectory of children aged 7–10 years derived from the corresponding trajectory of an adult.
A 3/8 inch simplex roller chain that conforms to ISO/ABNT 06 A, with a width between inner plates of 4.78 mm and roller diameter of 5.08 mm, was used. Traction was provided by a 9-tooth sprocket with a pitch diameter of 27.85 mm that conforms to DIN 06B; we used this sprocket because it is the smallest one available commercially and because its radius is similar to that of the trajectory at the end of the swing phase. Because the parameters and length of the chain trajectories differ in the swing and stance phases, a variable-speed three-phase electric gear motor set to operate at different frequencies in the two phases were used (Figure 4); the motor was powered using 0.33 kW alternating current and a 1:15 reducer.
Mounting scheme of the ankle guidance systems.
The swing and stance phases account for 38% and 62% of the total gait cycle; the proposed device was designed such that the speeds of the swing and stance phases correspond to their lengths. The novel aspects of the proposed device are as follows.
– The device can be attached to and synchronized with a treadmill. – The device has two ankle guidance systems, one for each lower limb, to control the kinematic trajectory of the ankle. – The ankle guidance system was designed considering the physiological trajectory of the ankles of children aged 7–10 years. – The swing and stance phases account for 38% and 62% of the gait cycle, respectively. – The device is affordable enough for use in rehabilitation clinics in developing countries.
Device control
The concept underlying the rehabilitation robot is speed control of the ankle attachment in order to create a realistic trajectory of the user’s feet. Because the path of the patient’s ankle joint is controlled by the robot, an appropriate velocity profile that complies with the following requirements must be determined and implemented. The velocity profile must be such that the actual ankle speeds of a human can be mapped to the rehabilitation device; further, the ankle speeds should be able to synchronise with various treadmill speeds.
In the current design, to ensure that the robot simulated a physiologically realistic velocity profile, gait data were recorded using a marker attached to the user’s ankle. The marker was fixed to the lateral malleolus of the user because the interface between the patient and the rehabilitation device is designed to be at this level. 15
An implementable velocity profile was generated from the measured gait data as follows: First, the recorded three-dimensional data were mapped to the sagittal plane because the rehabilitation robot is a two-dimensional device. Figure 5 depicts the resulting path of the marker in the sagittal plane over multiple gait cycles, and Figure 6 depicts the velocity profile of the lateral malleolus in the sagittal plane calculated from this two-dimensional trajectory.
Path of the lateral malleolus marker in the sagittal plane. Velocity profile during the treadmill gait over one gait cycle.

The measured data must be simplified, generalised and parameterised so that they can be used in the robot at various speeds. Therefore, the velocities were first quantified into four discrete values (Figure 7), and accordingly, four speeds Discretely quantified velocities. Square-cut velocity profile with adjustments and constants.
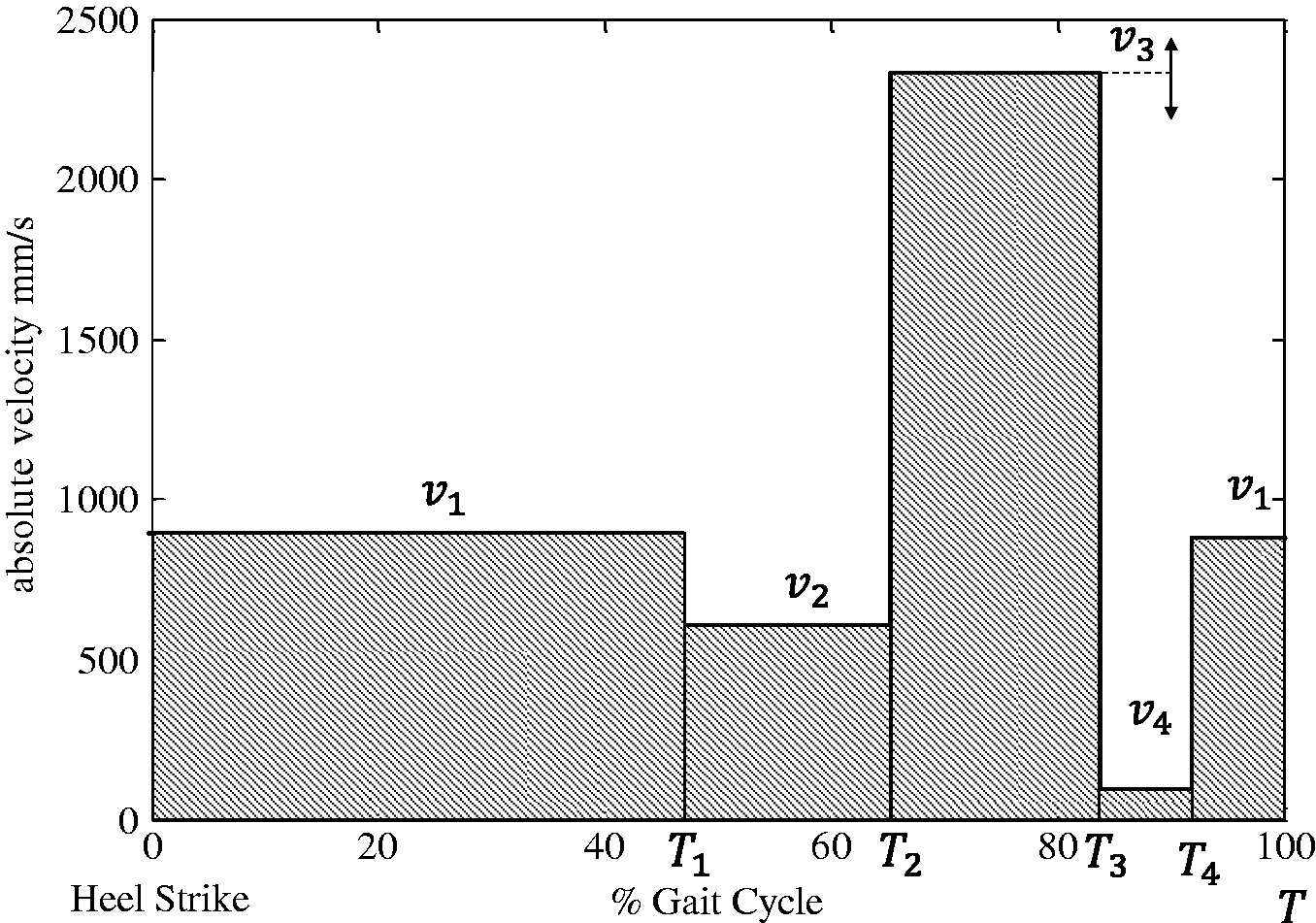
These four speeds and their duration are then defined to comply with the boundary conditions: v1 (i.e. speed during the stance phase) is set as the treadmill speed to synchronise feet and treadmill motion. Next, the absolute values of v2 (speed during transition from the stance phase to the swing phase) and v4 (speed during the end of the swing phase) are set to
Similarly, the durations that these speeds must be maintained for is calculated such that the 62%:38% ratio of the stance and swing phases is preserved. Finally, v3 is adjusted to comply with the requirement that one gait cycle (i.e. perimeter of the foot path) is completed within a defined cycle time T; that is, in T, the ankle covers a distance equal to the device perimeter (equation 1)

Although the resulting square-cut profile satisfies the formulated requirements, the associated movement is fitful and entails high device accelerations. Hence, to smoothen the profile and more closely approximate the measured gait data in a simple manner, velocity ramps are applied (Figure 9). The symmetrical nature of these ramps ensures that the distance covered on the track in one gait cycle remains unchanged.
Smoothening the velocity profile of the device by applying ramps.
Potential smoothening-induced asynchronous movements of the foot and treadmill in the stance phase are negligible because they occur only in the heel-strike and the toe-off phases.
The proposed system comprises a programmable logic controller (PLC; S7-1200, Siemens ), two frequency inverters, two encoders and four sensors. The PLC commands the two frequency inverters in a closed loop by using encoders attached to the motors and sensors that monitor the change in gait phase.
The PLC controls and maintains the walking speed at the desired levels (62% for stage support and 38% for the balance phase) by using a proportional–integral–derivative (PID) controller for each limb. The PID controller varies the analogue output to drive and monitor the motors by using the encoders (which are connected to the PLC fast inputs) and to measure the pulse frequencies (which are converted to values of speed through internal calculations).
The overall speed of the process can be preset or varied during the process by using a potentiometer installed in the device panel. A gradual acceleration system was employed to avoid leaps when the system is turned on. Through fixed-frequency measurements, the duration of the swing and stance phases were determined to establish the interphase relationship.
Inductive sensors are used to determine the change in speed during phase transition by detecting the position of the coupling pin of the device. The main advantage of this sensor is that its operation does not involve physical contact; in other words, detection is performed through simple approximation of an object, which in our case is a pin; this approach ensures high durability, high-speed switching and high reliability. The two sensors were installed on each limb to connect the end of the swing phase with the beginning of the stance phase and the end of the stance phase with the beginning of the swing phase.
The system was operated through four buttons installed on the device control panel: the start button (black), the emergency stop button (red) and a pin-moving button (green) for controlling each limb (Figure 10). To ensure device stability at high speeds, the frequency inverters were programmed for vector control.
System control panel: (a) inside view of one of the ankle guidance systems showing both inductive sensors and (b) encoder attached to the chain drives.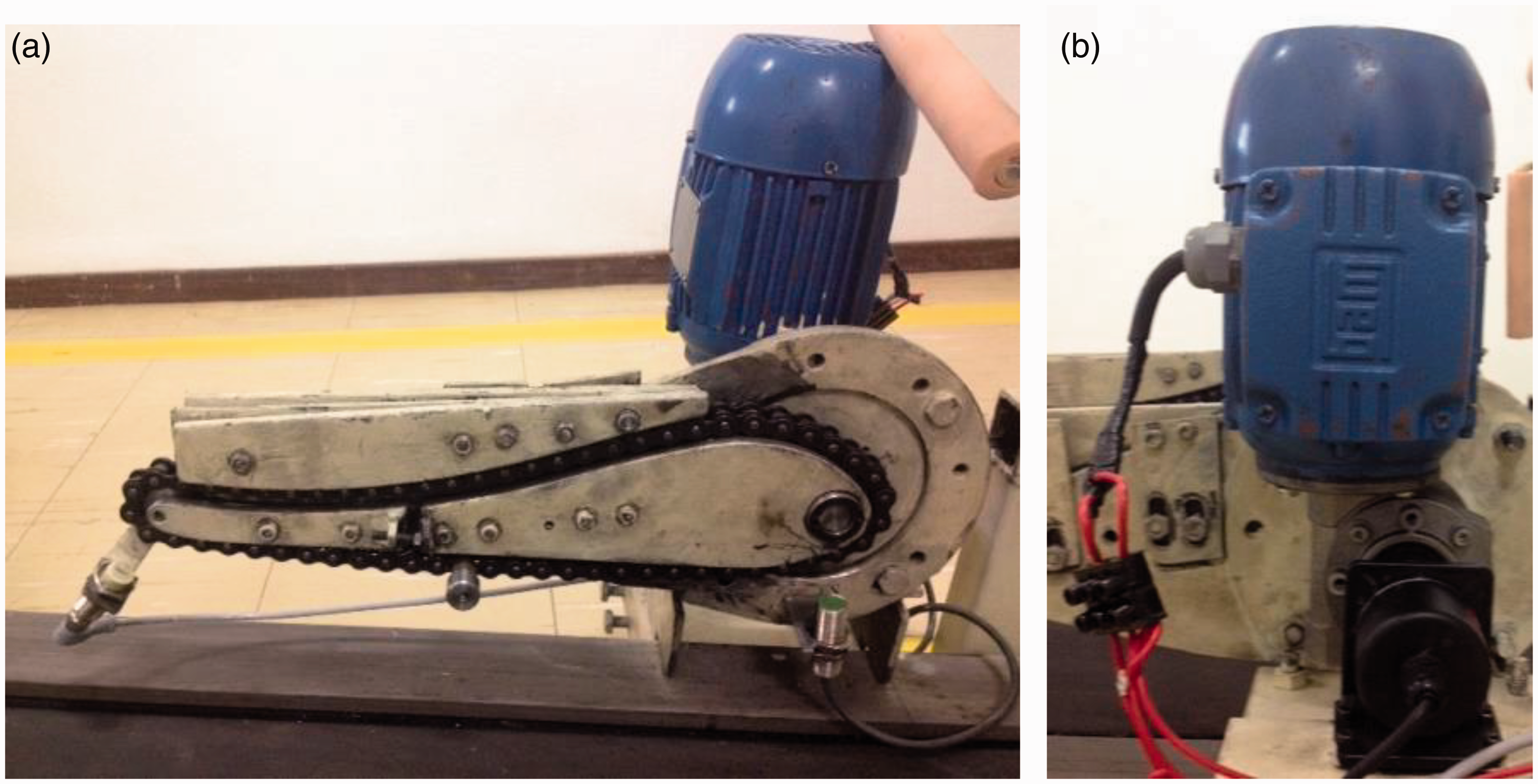
Clinical methodology
The proposed device was subjected to a clinical study approved by the Research Ethics Committee of the Federal University of Minas Gerais, Brazil (UFMG-COEP 688.895/14). The objectives of the clinical study were two-fold: (a) to assist in treatment planning, estimate deviations in the normative values of the spatiotemporal gait parameters, speed, cadence, stride length and step length, between children with normal development (ND) and children with CP in Brazil by analysing data obtained from a 10 m walking test (10-MWT) and (b) to compare the spatiotemporal gait parameters of participants with the parameters generated by the proposed device to infer its ability to generate adequate stimulus to assist in gait rehabilitation.
In total, 60 children (aged 7–10 years), 30 with CP (mean age, 8.1 (SD = 0.79)) and 30 with ND (mean age, 8.6 years (SD = 0.76)), selected through convenience sampling agreed to participate in the study. The inclusion criterion for the children with ND was a lack of history of any musculoskeletal condition, and those for children with CP were good vision, the ability to comprehend instructions, and the ability to walk continuously for 14 m with or without aid. Prior to the tests, voluntary informed consent was obtained from each participant and from their parents or guardians, according to Resolution 196/96 of the Health National Council. The 30 children with CP underwent a Gross Motor Function Classification System (GMFCS) assessment by a physical therapist; the resulting classification was as follows: GMFCS I (n = 11), GMFCS II (n = 8) and GMFCS III (n = 11). 16
Children with CP classified as GMFCS I and II performed the 10-MWT without using any hand held mobility device, whereas those classified as GMFCS III used a walker. The test was performed three times with a rest period of 3–5 minutes between the tests. After each test, the number of steps, step length and stride length were assessed, and the average walking speed and cadence were calculated. Walking times were measured using a digital stopwatch.
Statistical analysis
Data were statistically analysed using GraphPad Prism® (version 6.0f, GraphPad Software, Inc., CA, USA). Data for children with CP and ND were compared using the Student’s t-test. One-way analysis of variance, followed by the Newman–Keuls test, was used for multiple comparisons. Significance level was set at 0.05 for all tests.
Results and discussion
Spatiotemporal gait parameters of children with ND and CP.

= Significant differences (p < 0.05).
CP: cerebral palsy; ND: normal development
Preliminary analysis of the spatiotemporal parameters of the device
Spatiotemporal parameters of the device and the study groups.

= Significant differences between the spatiotemporal parameters of the children and the corresponding device (p < 0.0001).
CP: cerebral palsy; ND: normal development
The spatiotemporal parameters differed significantly between the device and the children with CP as well as between the device and children with ND (p < 0.0001). The parameters of the device were closer to the normative values than to the parameters of the children with CP.
When the device was set to the average speed of children with ND, cadence was approximately 27% higher than that of the children with ND because the step and stride was approximately 29% shorter (Figure 11); nevertheless, these values are consistent with Dusing and Thorpe
14
. The device speed can be adjusted according to the individual’s neuromotor level of impairment, which is especially relevant because the clinical results confirm that speed directly affects cadence.
(a) Cadence, (b) stride length and (c) step length of children with ND and the device set to the average speed of children with ND. Stride length and step of the device were 23.01% and 22.59% lower than those of children with TD, respectively, whereas the cadence of the device was 27.84% higher. **** p < 0.0001; ND: normal development.
When the device was operated at a speed similar to that of the children with CP (i.e. 77.41% higher step length and stride compared with a child with ND), cadence decreased (Figure 12). Under these settings, the user took wider and longer steps, especially in the swing phase, which is typically reduced in CP. Stride length and step length of the device differed from those of the children with CP by 34.13% and 31.08%, respectively.
(a) Cadence, (b) stride length and (c) step length of children with CP and the device set to the average speed of children with CP. ****p < 0.0001. Cadence was directly affected by the speed.
The device is depicted in Figure 13. The clinical results show that the device provides spatiotemporal gait parameters closer to those of children with ND than to those to children with CP. In addition, the parameter values of the device depart from the normative values depending on the level of motor impairment.
Prototype of the robotic orthosis attached to the treadmill.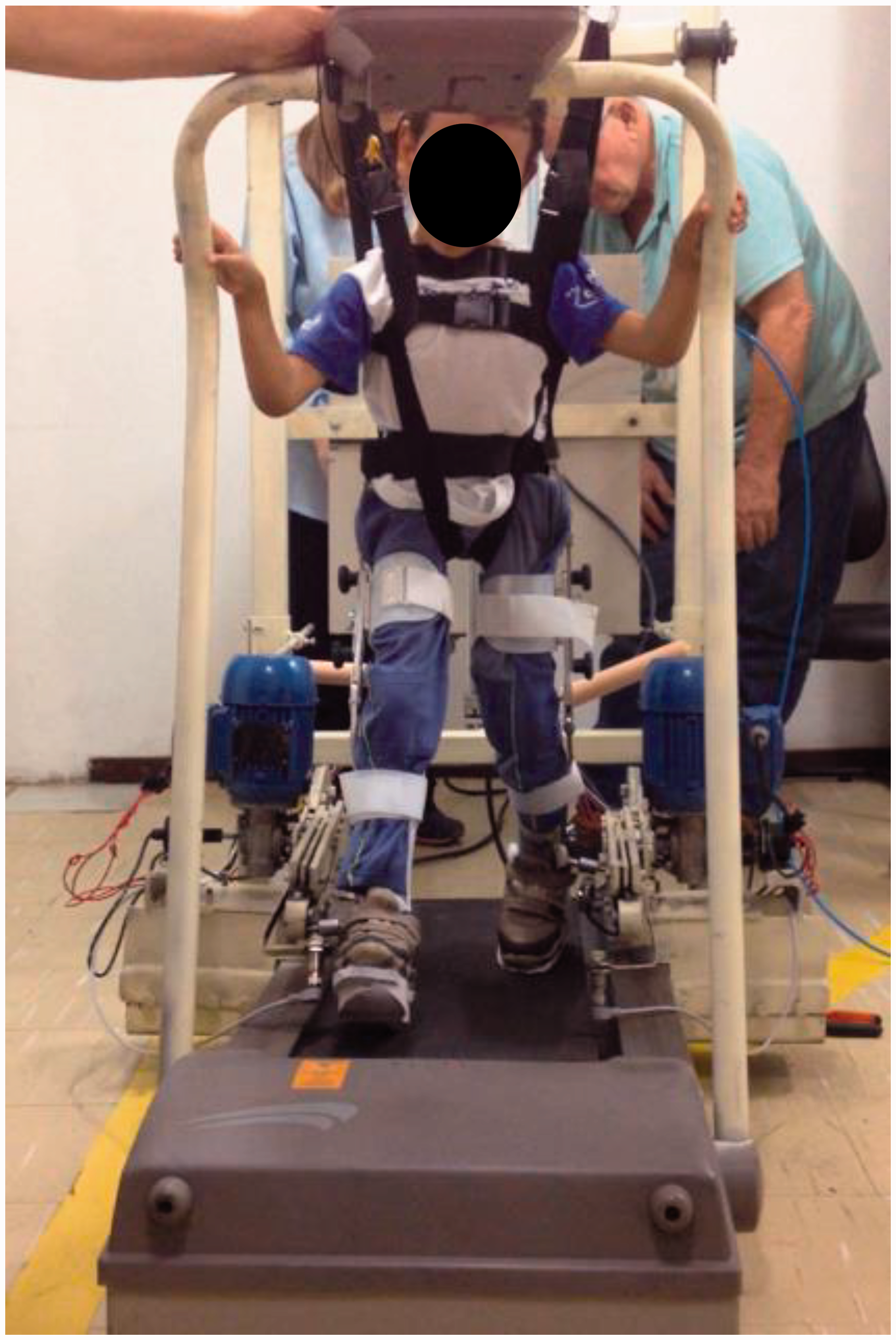
The average speed of our sample was slightly higher than that reported by Dusing and Thorpe 14 ; thus, the cadence reported in this study was lower than that in their study, which may be due to differences in sample size and the clinical methodology.
The results of this study are consistent with the literature on the importance of the gait pattern offered patients during treatment. For example, Banala and colleagues 20 evaluated the effect of robotic-assisted training on patients’ ankle trajectory; they considered patients with trajectories closer to those of healthy patients to have improved. Only kinematics of ankle trajectory was evaluated in their study.
Prototype manufacturing costs
Most robotic devices for rehabilitation are not commercially available in developing countries such as Brazil, primarily because of their high cost. Therefore, developing a low-cost robotic rehabilitation device is imperative. A major characteristic of our device is its low cost of production compared with devices available commercially for recovery of functional gait ability.
The prototype developed in this study cost €6400; we estimate its commercial production, with improvements in device mechanics, electronics, and aesthetics, to cost €25,000, which is less than 10% of the price of the only device currently available in Brazil for robotic gait rehabilitation.
Children with CP develop slowly and abnormally. When children with ND learn a new task, they practice it through repetition until the learning is established and the task can be easily performed. This learning process is the same for children with CP: Reinforcement of abnormal movement patterns prevents gait improvement and leads to muscle contractures and bones deformities. 21 Similarly, repetition of appropriate coordinated movements is essential in restoring gait. 5
Locomotor therapy to restore walking ability is based on the principle of increasing neuroplasticity through specifically training a particular task performed in a physiological pattern. 4 This therapy is effective in rehabilitating patients with disorders of the central nervous system. 11 These and other findings of many neuroscience studies indicate that continued practice of a specific task is crucial for realising permanent changes in motor system networks, motor learning and motor function. 22
Overall, the robotic device proposed in this study enabled children with CP to walk in a pattern close to that of children with ND, without using abnormal compensatory strategies.
Conclusion
We developed a low-complexity, simple and low-cost prototype of a robotic device for the gait training of children with CP. Preliminary tests showed that the spatiotemporal parameters of this device are closer to the normative values than they are compared with the average values of children with CP. Thus, the device can assist in the functional recovery of gait of such children. In addition, the device supports gait with high speed and long duration, which are crucial for creating new motor connections in the brain.
The major drawbacks of this prototype are its low user-friendliness and high difficulty of making adjustments. Further, the device mechanics, electronics and aesthetics can be improved. Nevertheless, the device has high potential for application in the clinical practice of robotic-assisted gait rehabilitation in children with neuromotor dysfunction at a fraction of the cost of currently commercially available alternatives in developing countries such as Brazil.
Footnotes
Acknowledgements
This research was conducted in part at the Bioengineering Laboratory of Federal University of Minas Gerais, Brazil and at the Sensory-Motor Systems Lab in ETH Zurich, Switzerland.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) (grant number 1038-31-3) and the Conselho Nacional de Desenvolvimento Científico e Tecnológico(CNPq), Brazil.