
Abstract
Background
Assessment of physical outcomes in patients with cerebral palsy (CP) is considered an effective way to monitor their progress, evaluate interventions and guide health care policy. However, no study using an activity monitor (AM) as a biofeedback device in treatment of people with CP has been published. Hence, the objective of this study was to evaluate the use of the AM as a biofeedback device in individuals with CP after a type of single-event multilevel surgery (SEMLS) called Single-Event Multilevel Lever Arm Restoration and Anti-Spasticity Surgery (SEMLARASS).
Method
A randomized, controlled trial was conducted among 40 individuals with CP in the age group between 10 to 20 years who underwent SEMLARASS. They were randomly assigned to two groups: Group A (n = 20) and Group B (n = 20). Both groups received intensive rehabilitation including different types of activity-based training for around three hours per day. Both groups were assessed with standard subjective outcomes (Physician Rating Scale (PRS), Dynamic Gait Index (DGI) and Functional Mobility Scale (FMS)) and objective outcomes with the use of an AM (IntenzLife, Model No. 56084-1) for measuring step count, distance walked and calories used. During the intervention, for Group A, they were also given an AM after presetting individualized stride length and body weight, to monitor their daily activity levels. The AM was worn around the neck of the person throughout the day and provided a daily report of the measurements and acted as a biofeedback device for individuals with CP who were given specific targets to achieve on a weekly basis. Both groups were evaluated before and after eight weeks of intensive rehabilitation.
Results
Group A showed significant differences in the scores of step count (p < 0.001), distance walked (p < 0.001), PRS (p < 0.001), DGI (p < 0.010) and FMS (p < 0.001) when compared to Group B after intensive rehabilitation. However, the calories used (p < 0.086) was not significantly different.
Conclusion
The AM, which is considered to be a valid and reliable tool for assessing the level of physical activity in CP, can also be used as a biofeedback device for improving specific walking parameters in persons with CP post-SEMLARASS.
Keywords
Introduction
Cerebral palsy (CP) is a group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to non-progressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of CP are often accompanied by disturbances of sensation, perception, cognition, communication, and behavior, by epilepsy, and by secondary musculoskeletal problems. 1 CP is the most common form of childhood disability, occurring in approximately two to three per 1000 live births. 2 Although considered a pediatric condition, the majority of children with CP will live well into adulthood. 3 The motor impairments associated with CP result in an increased energy cost of locomotion compared to able-bodied people.4,5 This increased energy requirement is associated with difficulties in performing activities of daily living and low levels of physical activity.6,7 Single-event multilevel surgery (SEMLS) refers to the correction of all musculoskeletal deformities in one operative session, which has the advantage of requiring only one hospital admission and one period of rehabilitation.8,9 Further rationale for SEMLS is the prevention of secondary deformities that can occur because of interdependence of lower extremity joints when only a single joint deformity is addressed. 9 Biofeedback has long been viewed as a vital link in several control mechanisms in the body. Homeostasis is dependent on biological information being returned, in part, to the control center from which it originates. Such information is used by the controller tissue (e.g. central nervous system) to alter the effector output (e.g. muscle). Over the years, the technology of instrumentally augmented biofeedback has evolved, which allows a person to monitor a given physiological process and attempt to control it. An example would be having a person observe the step count while walking with a monitoring device and then attempt to alter the walking pattern by increasing the speed or slowing it down. Thus, using biofeedback techniques, one would be able to control a physiological process that was previously considered beyond conscious control. In many neuromotor disorders, an individual is limited in the performance of everyday activities because of a lack of gross or fine muscular control. Biofeedback treatment has been shown to be effective in the treatment of neuromotor disorders such as CP.10–12 However, no study using an activity monitor (AM) as a biofeedback device in treatment of patients with CP has been published.10,13 A primary therapeutic goal for many individuals with CP is to attain the ability to walk. The clinical gold standard for measuring walking ability is gait speed. 14 However, gait speed may not accurately reflect the actual walking activity that people with CP engage in while at home and in the community. Advances in sensor technologies and signal processing techniques have provided a method to accurately and precisely measure walking activity in the home and community in an unobtrusive manner. Accelerometers, gyroscopes and force-sensitive resistors are among the different types of sensors that have been used either alone or in combination as wearable, mobile health AMs.15–17 The sensors generate different signal patterns as users move about in their home and community wearing the AM. These patterns then are analyzed using machine-learning techniques to identify distance walked, calories burned and the number of steps taken by the user.17–20 Examples of the AMs that are currently available commercially include the StepWatch Activity Monitor (SAM) (Orthocare Innovations, Oklahoma City, OK, USA), Intelligent Device for Energy Expenditure and Physical Activity (IDEEA) (MiniSun LLC, Fresno, CA, USA), activPAL (PAL Technologies Ltd, Glasgow, UK), and ActiGraph (ActiGraph LLC, Pensacola, FL, USA).21–26 These AMs gather a variety of data such as steps taken, activity counts, time in sedentary versus upright postures, and energy expenditure. These AMs appear to be primarily designed for use by researchers and may not be easily usable in a clinical environment because of high cost and time constraints in setting up the device and analyzing the data. Also, some of these AMs may not be accurate in identifying stepping activity in people with neurological disorders and older adults who walk at slower speeds.25,27,28 More recently, AMs that are geared toward consumer or patient use have been developed. Devices such as the Nike Fuelband (Nike Inc, Beaverton, OR, USA), Fitbit Ultra (Fitbit Inc, San Francisco, CA, USA), and Body Media (Body Media Inc, Pittsburgh, PA, USA) track steps taken, calories burned, and other health-related variables. These AMs also have interactive websites on which the user can view and interact with their data. These body-worn sensors appear to be geared primarily toward promoting weight loss. 29 These patient-use AMs might be a useful alternative to the more research-geared AMs for medical professionals to track walking activity in patients with CP and other neuromotor disorders. However, the algorithms used to analyze the sensor data and identify stepping activity in these types of AMs often are developed from people who are healthy, while individuals with CP may walk at slower speeds and may have movement patterns different from that of the normal population. The published studies on AMs are to assess only the validity, reliability and accuracy of the AMs in patients with CP, and no study has investigated the use of an AM as a biofeedback device for individuals with CP.30,31 Hence, with this background of knowledge and a gap in the literature, this study was conducted using an AM as a biofeedback device to evaluate specific walking parameters of patients with CP post-SEMLS.
Methodology
A randomized, controlled trial was conducted comparing specific ambulatory parameters with and without the use of an AM as a biofeedback device for people with CP following a type of SEMLS called Single-Event Multilevel Lever Arm Restoration and Anti-Spasticity Surgery (SEMLARASS). The surgical procedures included intramuscular release and controlled tendon lengthening, using the principles of Orthopedic Selective Spasticity Control Surgery and simultaneous restoration of lever arm dysfunctions. 32 This was followed by plaster immobilization of both lower limbs for 6–10 weeks, and then protocol-based, sequenced multidisciplinary rehabilitation. During intensive rehabilitation, participants were exposed to various kinds of activities and exercises like progressive strengthening, functional training, cycle or treadmill training, mechanical hippotherapy and aquatic training.
Study participants
A total of 40 participants between the age group of 10 to 20 years and diagnosed to have CP of spastic diplegia and quadriplegia types and who underwent SEMLARASS were recruited for this study. After providing informed consent, they were randomly allocated based on a computer-generated permuted randomization into two groups with Group A as experimental (n = 20) and Group B as control (n = 20) (see Figure 1, showing the flowchart of the participant selection process).
Flowchart of study selection process.
Participant selection criteria
Participant selection criteria included individuals with CP who (a) underwent SEMLARASS and were in the ambulatory phase of postoperative rehabilitation, (b) were able to take steps with minimal adult assistance or assistive devices and with orthotic devices such as an ankle foot orthosis or floor reaction orthosis, and (c) were able to follow verbal commands. Individuals with a severe cognitive impairment, uncontrolled seizure activity and any acute lower limb injury or pain were excluded. The participants involved in this study were earlier not introduced to any kind of AMs as a part of their rehabilitation. Participants were at level I, II or III on the Gross Motor Function Classification System (GMFCS). The GMFCS is a classification system that allows individuals with CP to be classified according to their level of functional mobility and use of mobility aids. People at level I can walk and run independently but may have difficulty with coordination or speed. People at level II can walk independently but may have difficulty running. People at level III require mobility aid to walk independently and may use wheeled mobility to travel long distances. The procedures involved in the study were fully explained to participants and their caregivers (in the case of participants less than 18 years of age or with a mild-to-moderate intellectual disability).32,33
Description of the AM used in the study
The AM used in the study was IntenzLife, Model No. 56084-1 (Figure 2). This AM is a small, light, commercially available device that can be worn around the neck. The device contains a three-dimensional accelerometer and therefore the position or direction of the unit is not crucial as long as it remains relatively still and does not swing. Based on proprietary algorithms, the device is able to estimate number of steps taken, distance walked and calories expended. The AM step counts cannot be reset to 0 within the course of a 24-hour period. Data were stored in the memory of the AM and processed by connecting the AM to a computer using a universal serial bus (USB) cable.
Activity monitor used for the study.
Study protocol
Both the control and experimental groups received intensive rehabilitation including various activity-based training for around three hours per day for eight weeks. The only difference between the groups was that the participants in the experimental group were allowed to wear the AM throughout the intensive rehabilitation as a biofeedback device and were instructed to achieve a set goal by increasing the step count by 30% at the end of every week and the progress was monitored at the end of every week for eight weeks (Figure 3 shows a child with CP using the AM). Specific instruction was given to the participants not to use the AM while being carried by the caregiver, while sitting in the wheelchair or during other activities of mobility that were not performed by the participant. The study protocol is described in Table 1.
Child with cerebral palsy using the activity monitor. Study protocol. AM: activity monitor.

Outcome measurements
The following demographic information and outcome measures were recorded: age, gender, type of CP, Dynamic Gait Index (DGI), Physician Rating Scale (PRS) and Functional Mobility Scale (FMS). Both groups were also assessed by using the AM for objective outcomes measures such as step count, distance walked and calories used. The measurements of the control group and the experimental group were taken at three intervals: (a) day before the surgery, (b) day before the start of intensive rehabilitation in the postoperative period and (c) last day of the eighth week of intensive rehabilitation. The DGI measures mobility function and dynamic balance in walking and stair climbing. There are eight items on the DGI and each item is scored on a four-point scale as (3) normal; (2) mild impairment; (1) moderate impairment; (0) severe impairment, with a maximal score of 24. The eight items include walking, walking with speed changes, walking with vertical and then horizontal head turns, walking with a quick pivot stop, walking over objects, walking around objects and walking up and down stairs. 34 The PRS is an observational clinical evaluation of gait in the sagittal plane on the parameters of foot contact, crouch, hip flexion, knee flexion and dorsiflexion.35,36 The FMS is a six-level, clinician-administered self-report ordinal scale that rates mobility within the different environmental settings of the home, school and community based on the assistance required for use in children with CP. 37
Statistical analysis
Descriptive statistics were reported using mean and 95% confidence interval (CI) for continuous variable and numbers and percentages for categorical variables. Analysis of variance (ANOVA) was used to analyze the significant difference for more than two grouped variables among group means of both between and within the experimental and control groups before surgery and before and after eight weeks of intensive treatment. A p value less than 5% was considered statistically significant. The data were analyzed using SPSS version 17.
Results
Mean age of participants in the study.

Frequency distribution of demographic profile of the participants.

GMFCS: Gross Motor Function Classification System.
Mean scores of all the outcome measures used to examine the AM.
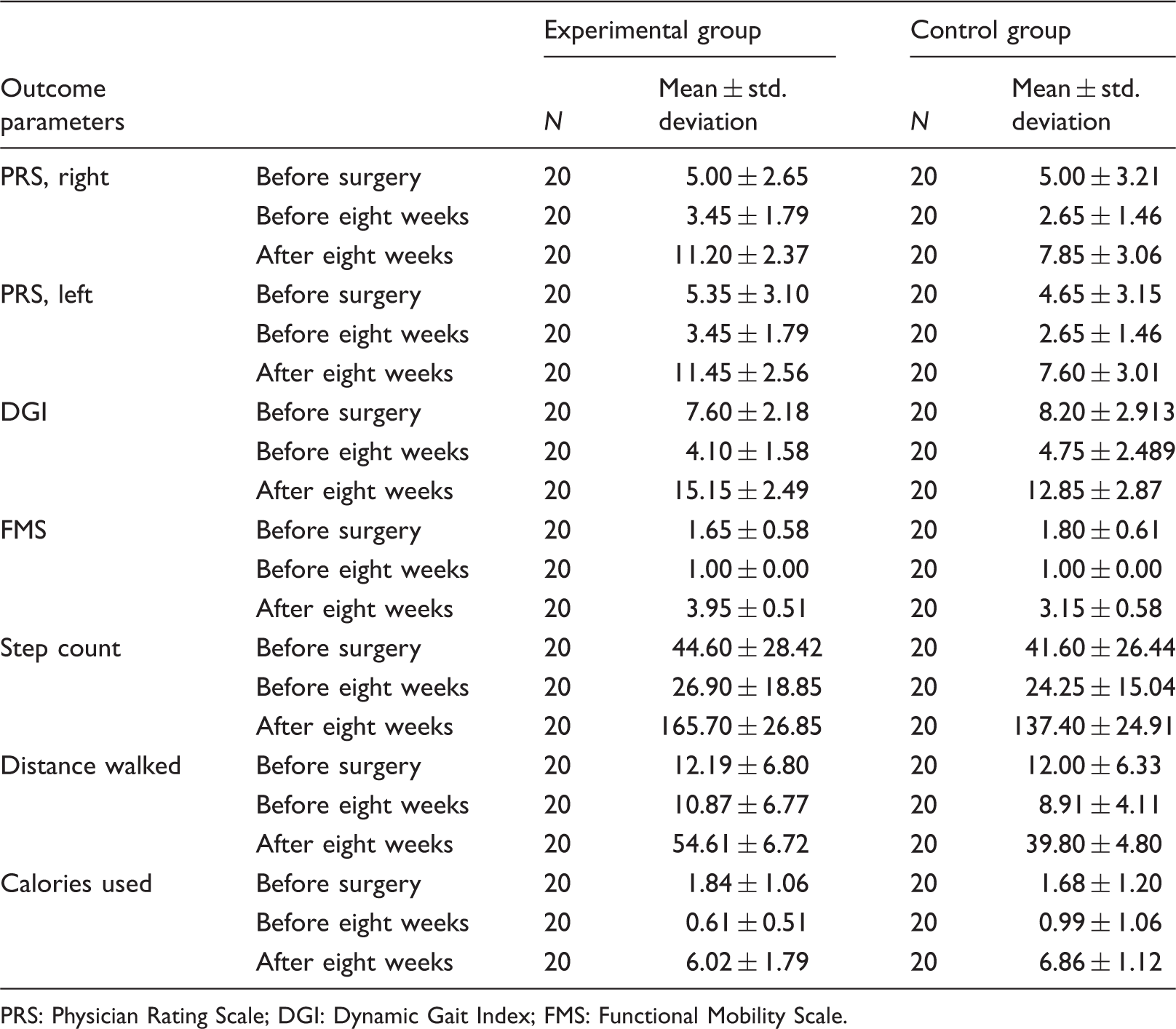
PRS: Physician Rating Scale; DGI: Dynamic Gait Index; FMS: Functional Mobility Scale.
ANOVA between and within the experimental and control group on all the studied outcome parameters.
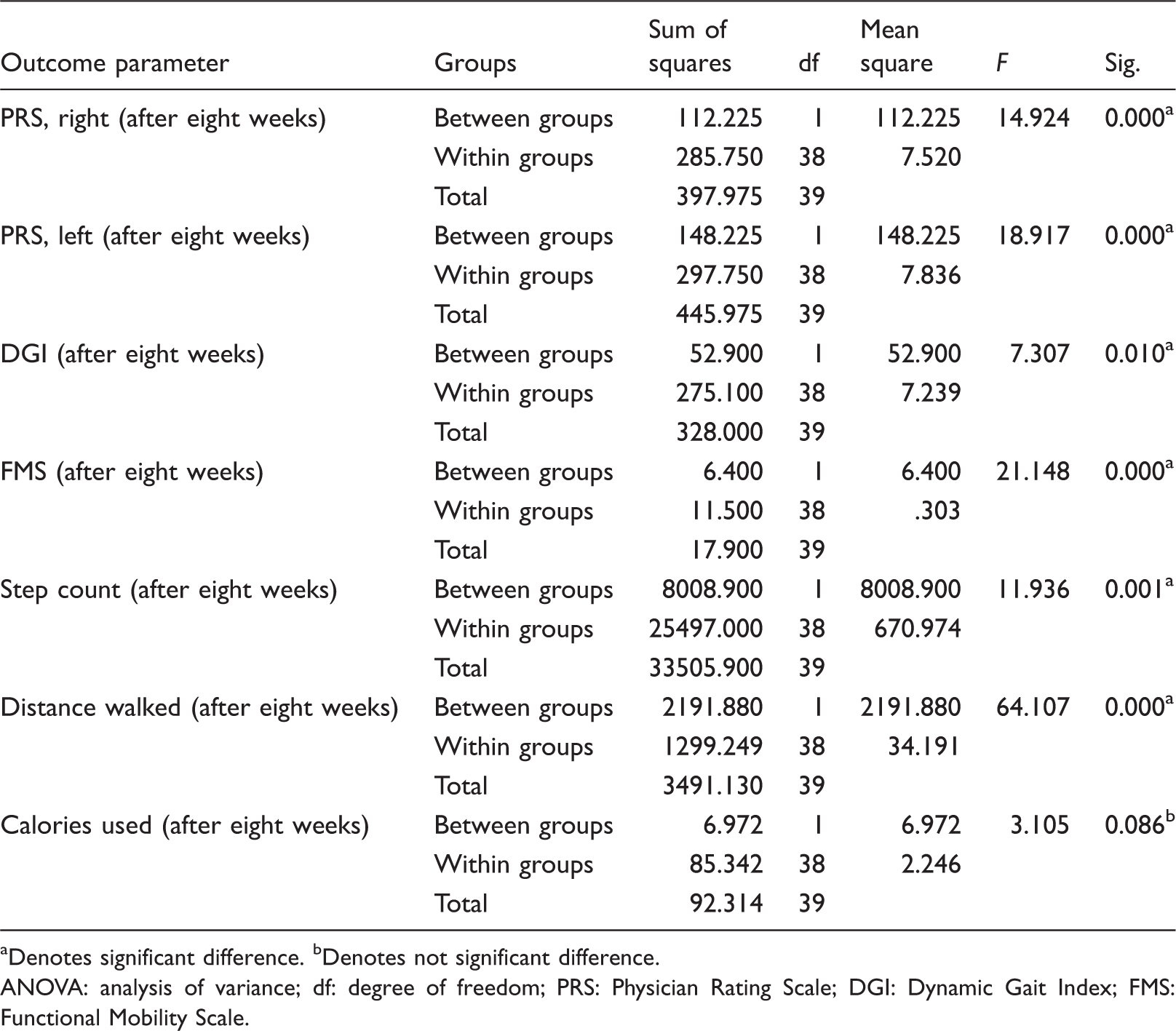
Denotes significant difference. bDenotes not significant difference.
ANOVA: analysis of variance; df: degree of freedom; PRS: Physician Rating Scale; DGI: Dynamic Gait Index; FMS: Functional Mobility Scale.
ANOVA between and within the experimental group’s studied outcome parameters across 10 measurement intervals: before surgery, before eight weeks, after week 1, after week 2, after week 3, after week 4, after week 5, after week 6, after week 7, after week 8.

Denotes significant difference. ANOVA: analysis of variance; df: degree of freedom.

Mean values of the progression seen in the activity monitor (AM) parameters of step count, distance walked and calories used.
Discussion
This is the first study of this kind to use an economical, commercially available AM suitable for industrially developing countries as a biofeedback device to improve specific walking parameters among patients with CP, post-SEMLARASS. Our results indicate that an AM can be used as a biofeedback device to improve walking in individuals with CP post-SEMLARASS. There was a significant improvement in the objective parameters of step count and distance walked in those participants who wore the AM on a regular basis along with serial guidance by a monitoring physiotherapist with weekly target setting for a period of eight weeks during the postoperative intensive rehabilitation. A few studies have reported the use of biofeedback for patients with CP, and augmented biofeedback has been reported as a successful training technique in controlling head and neck posture 3 and developing a functionally efficient and cosmetically smooth gait pattern.38–43 In contrast to a previous study that exhibited an inaccuracy in the measurement of step count by an AM (activPAL) because of difference in wearing the AM on the affected or unaffected legs, our study’s measurement on step count was not affected as it was worn around the neck. 44 The other important factor that affected step count and also distance walked was the gait speed. Participants in our study walked at slower gait speeds than able-bodied people. During the initial weeks of rehabilitation, participants had a lesser step count compared to the pre-surgical status because of the slow gait speed, which could be due to fear of falls, pain, and muscular weakness due to plaster immobilization. But as the patients underwent intensive rehabilitation for eight weeks, they started to improve gradually in gait speed and accuracy with an improved state of balance and gait exhibited through improvements in the PRS, DGI and FMS scores. Inspection of the raw data demonstrated that all steps had been registered by the accelerometers. However, the energy expenditure was not significantly changed as much as the other two parameters, which can be attributed to the fact that before surgery and during the initial period of rehabilitation, the energy expenditure was more because of the muscular force generated and subsequent fatigue, which implies that even as they took fewer steps and covered lesser distances, the energy expenditure was relatively high. But as rehabilitation progressed, the step count and distance ambulated increased proportionately but with a similar or slightly higher energy expenditure, which implied that the training had imparted the adaptability, less fatigue and better use of muscular force. Our results also support a previous study that implied that motor function assessment of children can be monitored through wearable sensors. 45 But in our case progress in sensor or the AM parameters was proportional to the progress seen in motor performance. The limitations of the study are as follows. Firstly, even though the AM accurately registered movements and steps, it was not only in walking activities but also sometimes in other sedentary activities. Secondly, as this AM was not waterproof, participants were not allowed to use it during aquatic therapy. Thirdly, other outcome measures of gait, balance, quality of life, and functional outcomes were not included. Finally, the follow-up of the participants is still ongoing, hence the long-term follow-up results of the participants are not reported in this study. The limitations would be rectified in a future research study with a larger sample size and a longer follow-up.
Conclusion
AMs can potentially be used by children and adolescents with CP, especially during post-SEMLARASS ambulatory rehabilitation for improving specific gait parameters. The AM studied had the advantage of being economical and easy to use, and it provided real-time feedback. Walking speed and balance did not affect the ability of the AM to detect steps.
Footnotes
Acknowledgments
We thank Marleen Maas, Better4u, Eindhoven, the Netherlands, for supporting the study by donating the AMs. We also thank Dr Esther Lydia, Loyola College, Chennai, India, for the statistical guidance.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.