
Abstract
Introduction
Workload and stress in excess can lead to work disability. The aim of our study was to determine whether commercially available “activity trackers” can be used to make statements about the work – or stress load of different occupational groups.
Material and methods
The study was conducted at the University Hospital Freiburg, Germany. Four occupational groups with a total of 32 subjects were studied: senior physicians (SP, 4), assistant physicians (AP, 11), nursing staff (NS, 12) and administrative staff (AS, 5). The activity trackers were worn on five working days and one day off. Step frequency, distance and heart rate (HR) were measured, and workload was assessed using a visual analog scale.
Results
The highest workload was reported by SP, the lowest by AS. Male employees feel higher workload than female employees (p = 0.009). NS covered the greatest daily distance, AP the least (p = 0.001). There was a significant difference in average HF between AP and NS (p = 0.008). AS showed higher daily distance and maximum HF on days off compared to work days, and NS showed the opposite behavior. With increasing patient volume for ambulatory care, the average HF increased (p = 0.037) in NSs.
Conclusion
“Activity trackers” reliably provide body data during work. In our small sample, interesting differences and results on workload emerged. More data would require more subjects and more study variables.
Introduction
In today's fast-paced and competitive world, work-related stress and burnout are increasingly becoming major concerns for individuals and organizations alike. High levels of workload, long hours and the need to constantly stay connected to work can all contribute to a heightened sense of stress and anxiety. 1
Especially healthcare professionals working in hospitals face a heightened susceptibility to stress due to the unique challenges and demands inherent in the healthcare environment. The nature of patient care, with its emotional intensity and unpredictability, places healthcare workers under constant pressure. 2 Additionally, the responsibility for critical decision-making, long working hours and exposure to potentially traumatic events contribute to the elevated stress levels. The organizational structure, bureaucratic demands and administrative burdens further exacerbate the stressors faced by hospital personnel. The cumulative impact of these stress factors not only poses a threat to the well-being of healthcare professionals but may also compromise the quality of patient care. Recognizing and addressing these stressors is crucial for fostering a healthier work environment and ensuring the resilience of the healthcare workforce. 3
In the field of urology, stress among healthcare professionals is also a growing area of concern. Urologists, in particular, face unique stressors related to the nature of their work, including the management of complex urological conditions, performing delicate surgical procedures and dealing with emotionally charged patient encounters. 4 Research in urology has highlighted the impact of stress on job satisfaction, mental health and overall well-being among urologists, with implications for patient care and outcomes. 5
However, it is not easy to measure stress in a real-world setting. Wearable devices, such as smartwatches and activity trackers, are becoming popular tools for monitoring and managing stress levels in the workplace. 6 These devices can provide real-time feedback on physiological parameters such as heart rate, respiration rate and skin conductance, which can help individuals identify and manage stress.7,8
Objectives
The aim of the present study was to determine whether data, such as distance and heart rate, collected with commercially available, relatively inexpensive “activity trackers” can be used to make objective statements about the work or stress load of different occupational groups. For this purpose, the recorded data were compared with non-working days and subsequently correlated with objectifiable key figures of the clinic.
Material and methods
Data collection
Subject collective and acquisition
The present study was conducted, after positive vote of the responsible ethics committee (EK-Antrag 63/17) and registration in the local study register (FRKS005207), in the Department of Urology of the University Hospital Freiburg. The clinic's staff council was also involved in the development of the study design and gave its supportive consent to this investigation.
The subject collective included physicians, nursing staff as well as employees from the administration of the Department of Urology. As these professional groups are only available in limited numbers at this Department, infinite scaling and Sample Size Calculation was not possible here and the study functioned as a pilot study.
Employees were informed about the present study by means of a notice board and, if interested, were included in the study after an informative interview. Written consent was obtained from all subjects prior to study participation.
The study was conducted from October 2018 to May 2021. On each of five working days and one day off (also on the day off approximately 8 h), the subjects’ heart rate, step frequency and distance covered were to be recorded using the so-called activity trackers. The recording on the working days took place exclusively during working hours.
Questionnaire
A short questionnaire was handed out to the test persons at the beginning of the study. Here, information on demographic data such as gender, age and marital status was to be provided. Furthermore, the individual workload was to be indicated on a visual analog scale from 0 = very low to 100 = very high. In addition, the subjective workload and stress should be indicated separately for each working day on a numerical rating scale (Supplement 1 and 2).
Monitoring
The devices used were commercially available “activity trackers.” Garmin vívosmart HR® were used to record the data, depending on the area of use.
We used a total of five wrist-based trackers. The participants wore the trackers either simultaneously or in different weeks, depending on their availability and work schedules. In some cases, multiple participants used the devices during the same time period, while in other instances, the data were collected sequentially over different weeks.
In hygienically sensitive areas, such as the operating room, ward or outpatient clinic, an activity tracker was used in combination with a chest strap. This combination allowed the recording of step frequency and distance covered by the activity tracker, as well as the recording of heart rate by the chest strap.
The activity tracker was attached to the trousers during recording to ensure that data recording was as uninterrupted as possible. The step frequency was determined with the help of built-in acceleration sensors within the “Activity Tracker.” The step frequency is continuously recorded and added to 15 min intervals. From the determined step frequency, the device calculates the distance covered during the recording. A GPS measurement of the distance was impossible in our setting for reasons of protecting the employee and personal rights of the participants.
In areas that are not hygienically sensitive, such as administration, an “activity tracker” was worn on the wrist, which continuously records the step frequency, distance and heart rate. This eliminated the need to wear a chest strap in these cases.
Here, too, the step frequency is continuously recorded by acceleration sensors, added to 15 min intervals and the distance covered during the day is determined.
Data evaluation
The recorded data were transferred from the online analysis program of the manufacturer into an Excel table. Subsequently, the data were entered into the statistics program SPSS (version 28.0).
For the metric variables (e.g. distance travelled per hour, steps per hour, average heart rate per hour), the position (median and mean with confidence interval) and also measures of dispersion (standard deviation) were calculated in each case.
For the nominal and ordinal variables (e.g. gender, stress level, or smoking habits), the respective frequencies were presented in cross-tabulations.
In a first step, the data were examined for normal distribution using the Shapiro-Wilk test. In the case of non-normally distributed data, the mean values were then compared using the Kruskal-Wallis test.
By means of one-factorial ANOVA or T-test, the mean values were calculated in case of normal distribution and then, if necessary, further examined with post hoc Bonferroni test.
In some cases, the partial Eta-squared was additionally calculated as a measure of the effect size.
Results
Questionnaires data
Demographic data
The number of test subjects was distributed among the professional groups as follows: 11 residents, 12 nursing staff, 5 administrative staff, 4 senior physicians. All subjects did fill the questionnaires correctly and a total of 32 questionnaires were evaluated. All participants were of Caucasian origin.
The average age of the subjects was 36.77 years (SD ±10.535), with the youngest (32.36 ± 3.355) in the resident group and the oldest (50.00 ± 10.424) among the senior physicians.
Fifty percent of the subjects were female. All administrative staff were female, and all senior physicians were male. Two-thirds of the nursing staff and 3 of 11 residents were female.
Then, 53.1% of participants were married, 12.5% were single, 6.3% were divorced, 21% were in a committed relationship, and 6.2% did not report this.
On average, subjects had been employed for 14.363 years, with senior physicians having been employed the longest, 23.5 ± 8 years, and residents the shortest, 5.5 ± 3.3 years.
Slightly more than half, 56.3% of the participants, reported 1–2× sports per week, and 87.5% of the subjects denied nicotine consumption.
Professional groups
There was a difference between the subjective workload of the individual professional groups, senior physicians reported the highest subjective workload, administrative staff the least, although there was no significant difference (p = 0.349) (Figure 1).
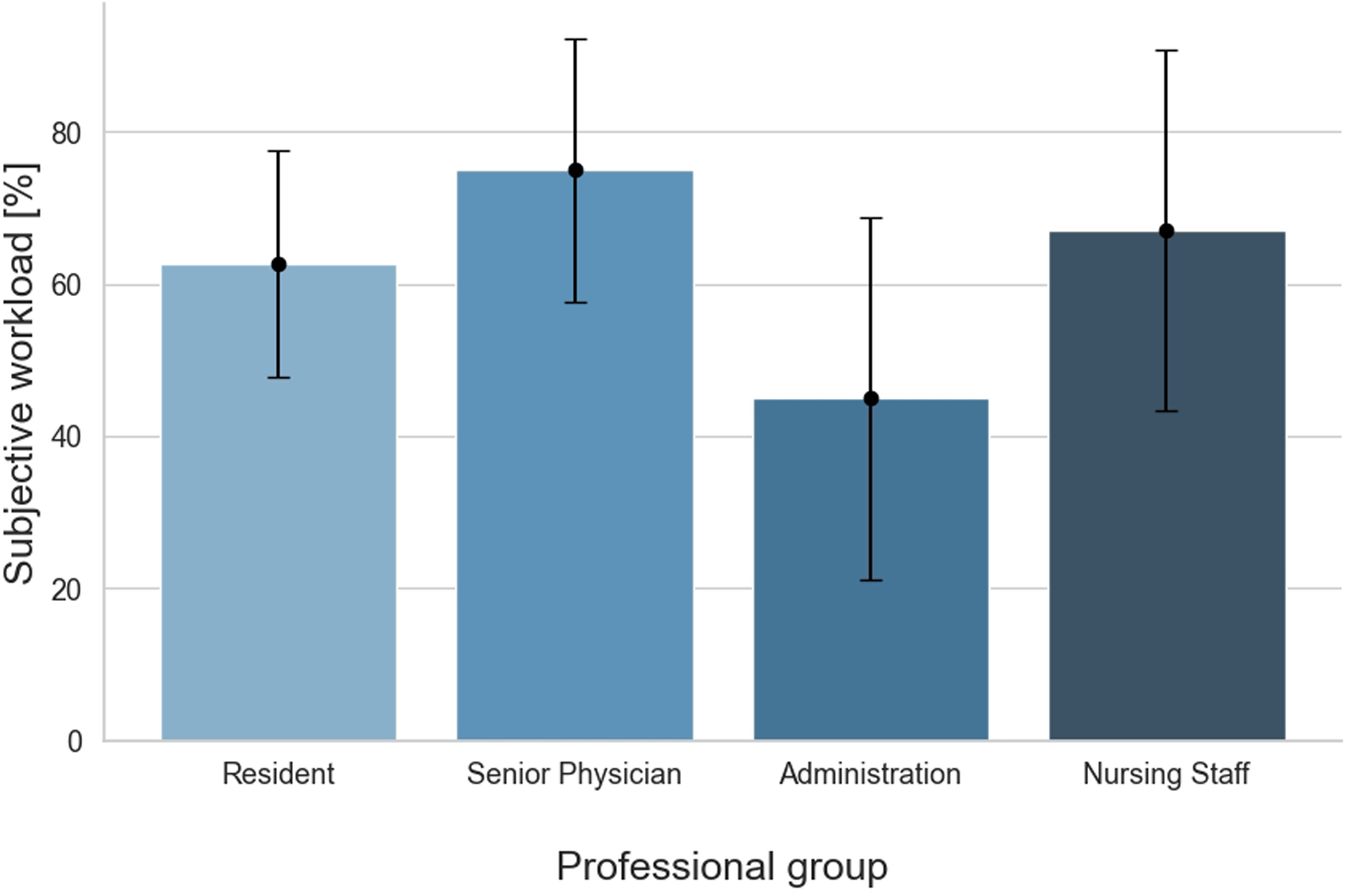
Workload groups.
Genders
We could observe differences in the subjective workload, with a significant difference between the genders: male subjects perceived a higher workload (p = 0.009) (Figure 2).
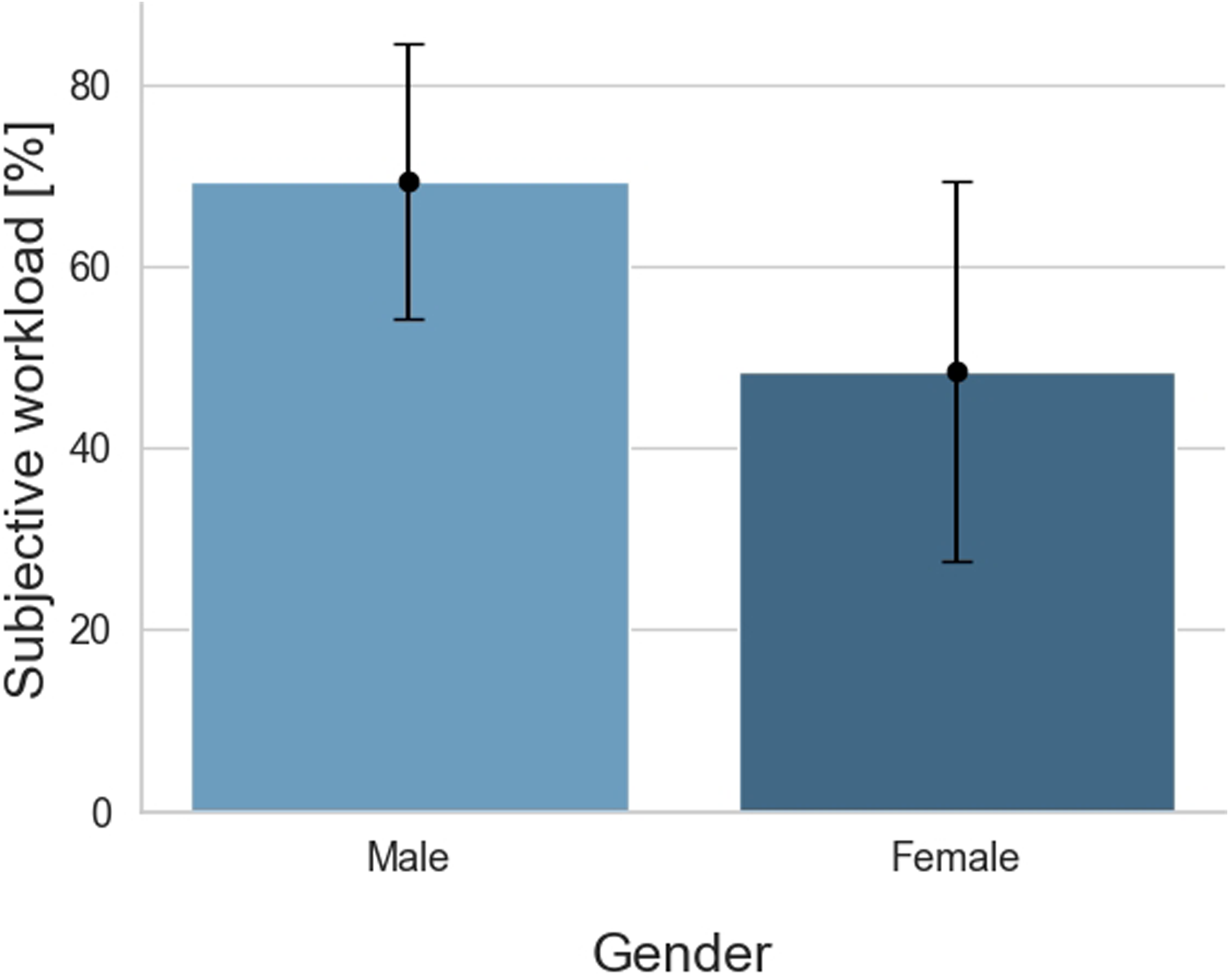
Workload gender.
Activity trackers data
Professional groups
Distance
Nursing staff covered the longest distance with an average distance of 4351 m per day, followed by the administrative staff 3373 m and the senior physicians 3265 m. The shortest distance was covered by residents with a distance of 3035 m. A significant difference (p = 0.001) was demonstrated between residents and nursing staff. There was no difference between the average distance meters of male and female participants (p = 0.070) (Figure 3).

Distance groups.
Heart rate
In a pairwise comparison, there was a significant difference in the average heart rate between residents (M = 79; SD =7.9) and nurses (M = 89; SD =9.6) (p = 0.008). There was no difference between the maximum heart rate of each professional group (p = 0.465). Additionally, there was no difference between the mean average heart rate of men and women (p = 0.212) (Figures 4 and 5).

Heartrate groups.

Heartrate gender.
Impact of workload on other variables
Workload and distance, heart rate
There was no significant difference in distance meters covered with a subjective workload greater or less than 50 (p = 0.698). There was also no significant difference in mean heart rate when the workload was above or below 50 (p = 0.400).
Days with high and low workloads
We examined whether there was a connection between the clinic's objective key figures and the test subjects’ recorded tracker data. The tracker data and therefore dependent variables included the categories distance meter, average heart rate and maximum heart rate. In the inpatient area, the respective bed occupancy, admissions and discharges as well as the number of patients in the outpatient department were used as objective key figures for the clinic and thus as independent variables.
There was a significant connection between patient volume as an independent variable (R² = 0.245; p = 0.037) and the average heart rate as a dependent variable in nursing staff. The average heart rate appears to increase as the number of patients increase (Figure 6). There were no significant relationships in the HR Max and distance meter categories.
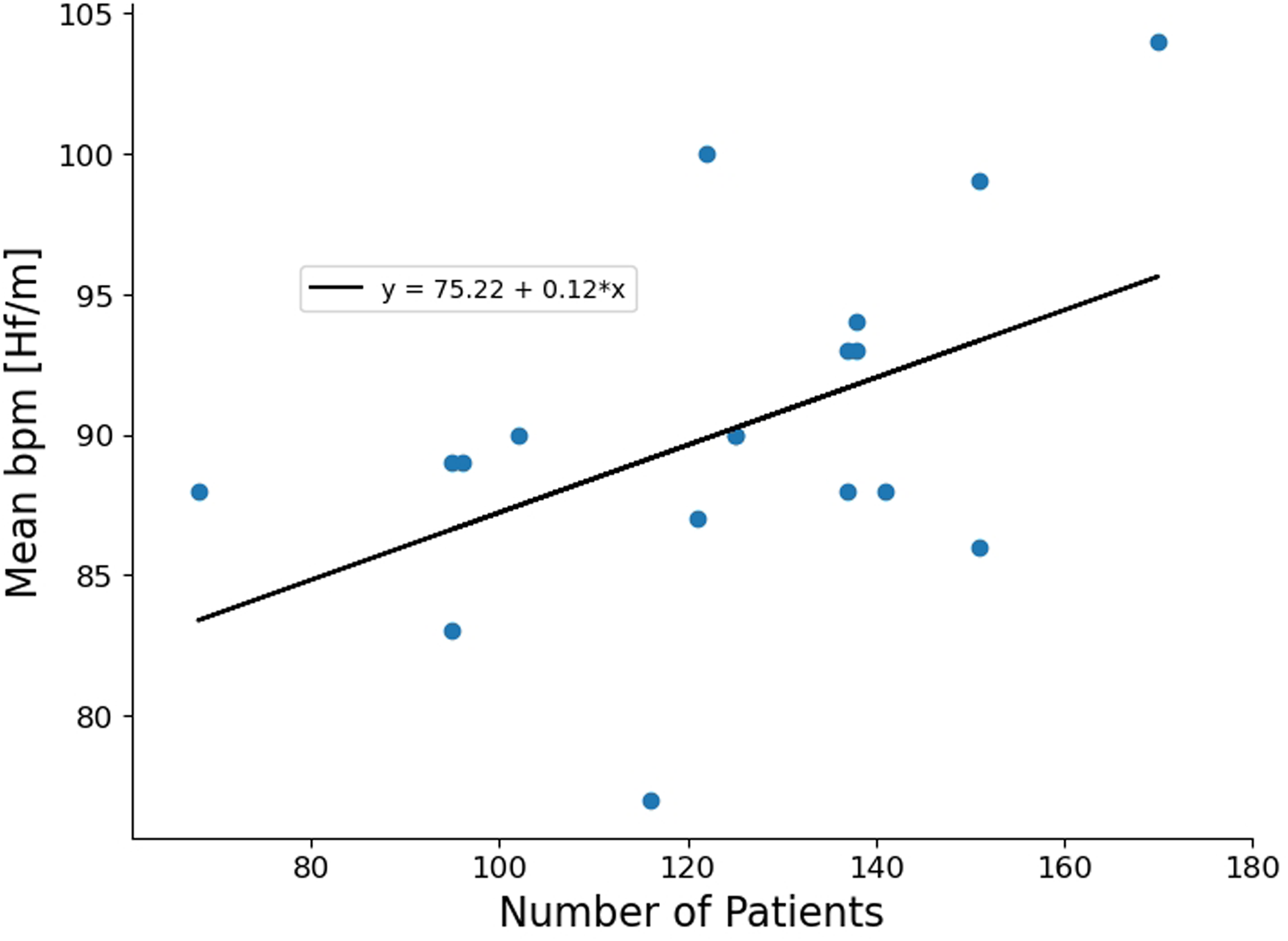
Bpm patients nurse.
Working day and day off data
It was examined whether there were significant differences in the recorded tracker data between the working day and the day off.
There were significant differences among the administrative staff in the maximum heart rate category (p = 0.004; η² = 0.314). The average maximum heart rate on working day was M = 127 ± 16, on their day off M = 156 ± 23.4. There were also significant results (p = 0.000; η² = 0.273) for the nursing staff in the distance meter category. The nursing staff covered an average of 4306 m on a working day and an average of 2788 m on a day off. Eta square showed a large effect in both cases.
Discussion
The aim of this study was to determine whether data collected using commercially available, relatively affordable “activity trackers,” such as distance and heart rate, can provide objective insights into the work-related or stress levels of different professional groups. To achieve this, the recorded data was compared with days off work and subsequently correlated with objective clinic metrics.
The study also highlights variations in work-related stress and physical activity across professional groups. Senior physicians faced the highest stress levels, while nurses were the most physically active. Gender differences showed men experienced more stress, while women had higher heart rates during work.
Limitations of the study
Limitations of the study were the limited availability of staff at the clinic and the resulting impossibility of calculating a sample size. In addition, we used non-validated questionnaires and non-specifically validated trackers for the tested working environment.
Also the use of wrist-based activity trackers, which are primarily designed for consumer use rather than professional environments, may have impacted the accuracy of certain metrics, such as walking distance and step counts. Wrist-worn devices can sometimes fail to capture movement accurately, especially in environments with complex or non-linear motion patterns, as seen in clinical settings. This limitation is consistent with findings from Kluge et al. (2024), 9 who reported similar challenges in the professional use of activity trackers.
Work-related stress variations
The elevated levels of work-related stress reported by senior physicians are consistent with previous research highlighting the substantial stressors associated with their responsibility for making critical medical decisions, managing complex cases and coping with high patient loads can contribute to these heightened stress levels. 10 Nurses also reported significant stress, which can be attributed to their roles as frontline caregivers responsible for patient outcomes. 11 Administrative staff, although experiencing lower stress levels, are not exempt from workplace stressors, such as administrative demands and interactions with patients and healthcare professionals.12,13
The findings of this study provide valuable insights into the complex interplay between work-related stress and physical activity among healthcare professionals in a hospital setting. The observed variations in work-related stress and physical activity across professional groups underscore the importance of considering these factors in the context of occupational well-being. 14
The observed gender differences in stress levels, with men reporting higher stress than women, warrant further investigation. 15 Previous studies have documented gender disparities in stress responses, indicating potential factors such as work-home conflicts and differing coping mechanisms that may contribute to these variations. 16 However, it is important to note that attributing differences in stress levels solely to gender in our study context is challenging, as only men or women were examined within some of the professional groups (all nurses were female, all senior physicians were male). Therefore, understanding the underlying causes of these gender differences requires careful consideration of various factors beyond gender alone, which is crucial for tailoring interventions aimed at effectively reducing workplace stress.
Physical activity patterns
Despite facing high levels of work-related stress, nurses emerged as the most physically active professional group in terms of distance covered and steps taken during work hours. This finding underscores the resilience and dedication of nurses who manage to engage in physical activity despite the demanding nature of their roles. 17 Administrative staff also demonstrated a commitment to physical activity, reflecting the importance of promoting movement in sedentary work environments.
Senior physicians and residents, while experiencing substantial work-related stress, engaged in slightly less physical activity during work hours. This trend may be attributed to the time-intensive nature of their responsibilities, including patient consultations, administrative tasks and rounds. Nevertheless, it is important to note that these professionals still engaged in a considerable amount of physical activity during their work shifts, highlighting the potential for incorporating movement into daily routines, even in high-stress environments. 18
Correlations and implications
The weak correlations between work-related stress and physical activity metrics suggest that while there is a modest association between stress and physical activity, other factors likely play a significant role in determining activity levels among healthcare professionals. It is plausible that individual coping strategies, workplace support systems and personal motivations also influence physical activity behaviors. 19
These findings have several practical implications. Firstly, interventions aimed at reducing work-related stress should be tailored to the specific needs of professional groups, with a focus on senior physicians and nurses who reported the highest stress levels. Additionally, promoting physical activity within the workplace, particularly among physicians and assistant physicians, can contribute to overall well-being and stress reduction. Furthermore, gender-specific stress management strategies should be considered, acknowledging the distinct stress experiences of men and women in healthcare roles.
Conclusion
First, this study allows us to conclude that inexpensive activity trackers can be used to reliably collect data from employees in a hospital setting.
The data collected in this study has shed light on the relationships between work-related stress and physical activity among healthcare professionals in a hospital setting. The variations in stress levels and physical activity patterns across professional groups emphasize the need for targeted interventions to support occupational well-being.
Senior physicians and nurses, who reported the highest stress levels, may benefit from stress management programs tailored to their specific needs. Promoting physical activity within the workplace can be particularly effective for physicians and other health care professionals, who may face time constraints but still engage in substantial physical activity during work hours.
The gender differences observed in stress levels and heart rate responses underscore the importance of considering gender-specific approaches to address workplace stress and burnout risk.
While this study has provided valuable insights, it is essential to recognize that work-related stress and physical activity are influenced by a multitude of factors. Future research should explore these relationships comprehensively, considering additional variables such as coping strategies, social support and organizational policies. Our pilot study has several limitations; in the future a larger cohort should be studied, possibly more accurate trackers used and validated questionnaires issued. By gaining a more comprehensive understanding of these dynamics, healthcare institutions can develop evidence-based strategies to promote the well-being of their professionals, ultimately leading to improved patient care and outcomes.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241293924 - Supplemental material for How does urology work? Evaluation of activity trackers in the assessment of workload and stress burden among employees in the Department of Urology of a German University Hospital: A prospective pilot study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241293924 for How does urology work? Evaluation of activity trackers in the assessment of workload and stress burden among employees in the Department of Urology of a German University Hospital: A prospective pilot study by Philippe Fabian Pohlmann, Maximilian Glienke, Christian Ehrmann, Christian Gratzke, Arkadiusz Miernik and Dominik Stephan Schoeb in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076241293924 - Supplemental material for How does urology work? Evaluation of activity trackers in the assessment of workload and stress burden among employees in the Department of Urology of a German University Hospital: A prospective pilot study
Supplemental material, sj-pdf-2-dhj-10.1177_20552076241293924 for How does urology work? Evaluation of activity trackers in the assessment of workload and stress burden among employees in the Department of Urology of a German University Hospital: A prospective pilot study by Philippe Fabian Pohlmann, Maximilian Glienke, Christian Ehrmann, Christian Gratzke, Arkadiusz Miernik and Dominik Stephan Schoeb in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank all employees of the Department of Urology for their participation, assistance and interest in this research. We would also like to thank the clinic's staff council for their support. We acknowledge support by the Open Access Publication Fund of the University of Freiburg.
Contributorship
PFP, CE, and DSS researched literature and conceived the study. AM and CG were involved in protocol development, gaining ethical approval and test subjects recruitment. CE handed out the activity trackers to the test subjects and collected the results. PFP wrote the first draft of the manuscript. MG performed the data analysis and created the figures. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The ethics committee of the University of Freiburg approved this study (EK-Antrag 63/17).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
DSS.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.