
Abstract
Child and adolescent mental health needs have increased over recent decades. Schools play a vital role in addressing these needs through multi-tiered systems of support, including universal mental health promotion (Tier 1), targeted and intensive services (Tiers 2 and 3). School Mental Health Ontario (SMH-ON) is a provincial implementation support partner to the Ministry of Education focused on enhancing quality, scalability and sustainability of multi-tiered mental health support for Ontario’s 72 school districts. This implementation study examined the acceptability of the SMH-ON strategy through an audit of district action plans (n = 61; 84.7%) for nine key strategic elements. On average, districts referred to 7.25 out of the nine key elements. The most prevalent elements were Tier 1 Mental Health Literacy (96.7%) and Tier 1 Parent, Caregiver & Community Connections (93.4%), indicated in more than 9 of 10 plans. The least prevalent were Tier 2 Early Identification & Student Support (60.7%) and Student Leadership and Agency (70.5%). Potential synergies of implementation activity were observed, providing guidance for implementation planning. Findings underscore the value of provincial leadership in promoting the acceptability of school-based mental health initiatives and highlight priority areas requiring further attention to support comprehensive and sustained implementation.
The past decades have seen a global trend of a rising prevalence of mental health (MH) challenges among children and youth, with the prevalence of diagnosed MH conditions among adolescents increasing 35% between 2016 and 2023 (Sappenfield et al., 2018). Diagnosed anxiety in this time increased 61%, from 10.0% to 16.1%, and depression increased 45%, from 5.8% to 8.4% (Sappenfield et al., 2018). But the need for MH services for children and youth has long been recognised as exceeding the availability of community services (Burns et al., 1995). In this context, schools play an essential role in prevention, identification and support of student MH challenges (Burns et al., 1995). Meta-analysis shows that schools are the most commonly accessed MH service setting among community samples of children and adolescents (Duong et al., 2021). Among young people with elevated MH challenges or formal diagnoses, schools were also the most common locus of MH services, with 22.1% supported at school, compared to 20.6% in outpatient settings (Duong et al., 2021). Within this setting, children and adolescents who experience MH challenges appear to greatly benefit in the provision of school MH services (Cipriano & Maurice, 2024; Kang-Yi et al., 2018, 2024).
At present, schools tend to offer fragmented and siloed MH support (Atkins et al., 2010). On the one hand, regulated MH professionals (e.g., school psychologists, counsellors) may be available to schools to provide intensive treatment for youth experiencing MH challenges, often in reaction to crisis (Hoover & Bostic, 2021; Stephan et al., 2015). On the other hand, universal classroom-based programs focused on topics such as social emotional learning, generally led by educators, provide proactive programming to promote MH (Cipriano et al., 2023; Stephan et al., 2015). This fragmentation contributes to an over-reliance on reactive services and places undue burden on crisis response systems, to the detriment of both student well-being and staff capacity (Atkins et al., 2010; Domitrovich et al., 2010).
A multi-tiered systems of support (MTSS) model is predicated on the belief that effective intervention requires a coordinated and systematic continuum of care (Rowling & Weist, 2004; Schaffer, 2022; Vetter et al., 2024). Multi-tiered systems of support focus on preventive intervention wherein all students are taught to understand how to support their own mental health and engage in help-seeking (if needed) before MH problems arise (Tier 1). Selective activities (Tier 2) are aimed at members who are considered at-risk of developing mental health challenges, through early identification, secondary prevention and early intervention for mild-to-moderate MH needs via brief, targeted interventions. Finally, more intensive services are provided for students who are experiencing a challenge with their MH through access to trained MH practitioners (Tier 3); this also includes efforts to locate and access local service pathways of care, given that schools do not have the capacity to take a lead role in care of more severe, complex, or acute MH problems.
Moreover, it is increasingly recognised that identity and MH are “inextricably linked [such that when] a student feels that their identity is affirmed [. . .] they are more likely to feel a strong sense of positive MH” (Mental Health Commission of Canada, 2025, p. 20). Experiences of discrimination including homophobia, transphobia and racism are well-established risk factors for poor MH (Gajaria et al., 2021). School MH services that are responsive to cultural identity (Clauss-Ehlers et al., 2013) and other identities (e.g., gender; Ghabrial et al., 2023) are most likely to be acceptable and effective with students. Building these concerns into multi-tiered models is another priority for school MH.
MTSS models provide a crucial framework for prevention and intervention activities. Ensuring that support exists at each of the tiers is seen as the most likely approach to ensure student need is addressed appropriately (August et al., 2018). Effective interventions exist for each of the three tiers (Arora et al., 2019; Feiss et al., 2019), and the interconnectedness of work across the tiers and the functional flow between tiers is crucial to ensuring that fewer students progress from Tier 1 to Tier 2 (Sugai & Horner, 2009) and Tier 2 to Tier 3 (Lyon et al., 2024). Ensuring supports exist to meet the needs of every student is, then, a chief goal of multi-tiered school MH.
A Sector-Wide Initiative Towards Multi-Tiered School Mental Health
In 2011, Ontario funded two initiatives to support student MH. First, funding was provided for every school district for a MH Leader position dedicated to district-level strategy, capacity-building and partnering with local child and adolescent MH services. At the same time, the School Mental Health Assist program was established, since expanded and rebranded as School Mental Health Ontario (SMH-ON), to act as both central planning support to the government and implementation partner to school districts, providing strategic direction, implementation coaching, resource co-development, evidence-informed supports, and professional learning for school and district staff strategies, resources and services. Every school district is supported by a SMH-ON implementation coach and a wide range of evidence-informed resources and professional learning opportunities. It is important to note that SMH-ON offers support and implementation assistance to all Ontario school districts but does not enforce compliance or adherence. Since 2019, SMH-ON has expanded its focus onto equity and reconciliation as fundamental to culturally and identity-responsive mental health supports.
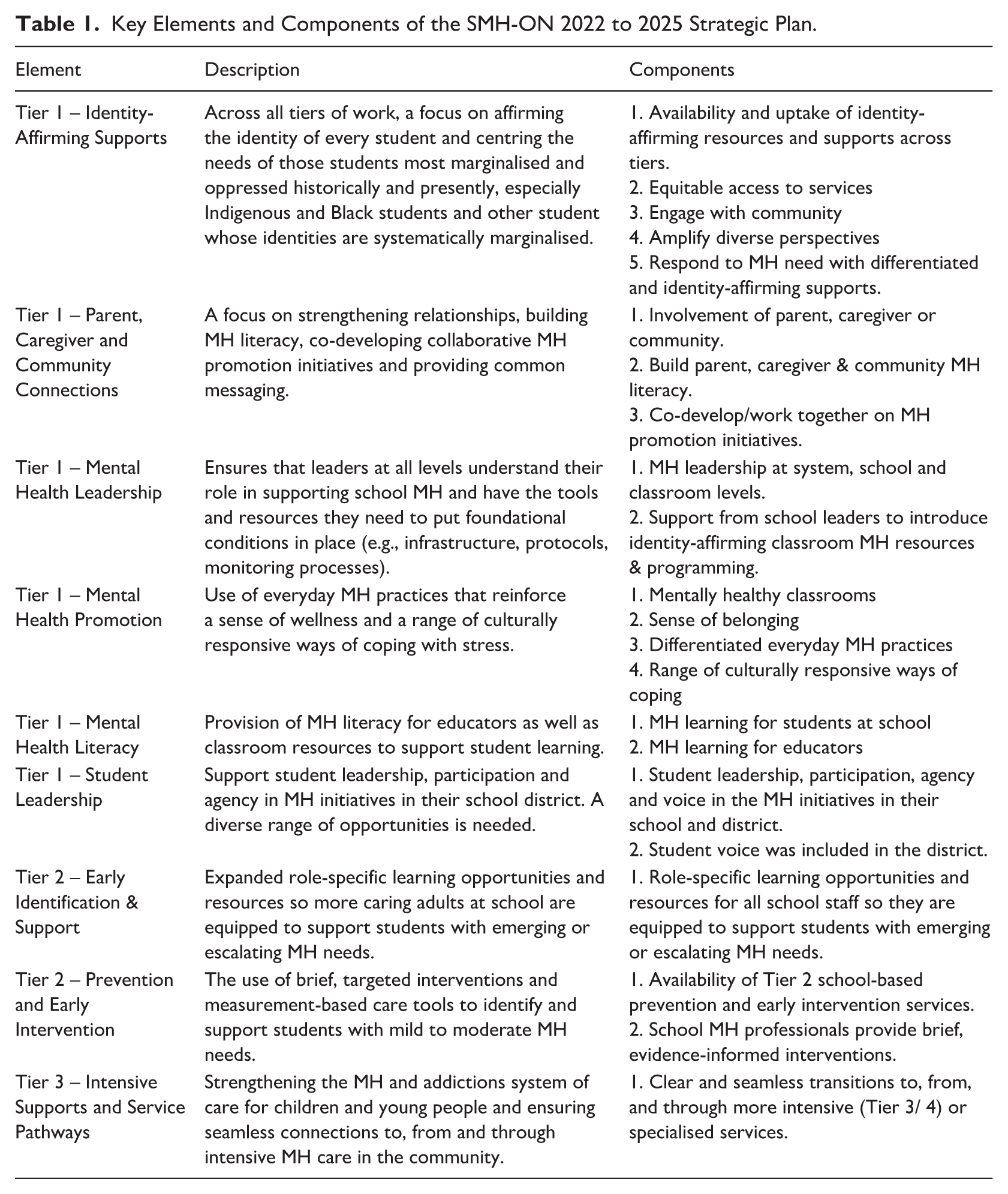
In 2022, SMH-ON published a school MH strategy for Ontario (See Table 1; School Mental Health Ontario, 2022), built upon work on MTSS (Walker et al., 1996; Weist et al., 2002, 2006), to envision identity-affirming student mental health services at different tiers. Supplementing this strategy, the Right Time Right Care initiative, developed by a team of intermediary cross-sectoral partners, including SMH-ON (School and Community System of Care Collaborative, 2022), focused how schools and community MH settings can work to an integrated approach providing the right care at the right time in the right setting, with a focus on Tier 2 identification and Tier 3 support, including measurement-based care.
Key Elements and Components of the SMH-ON 2022 to 2025 Strategic Plan.
Ontario provides an example of a decentralised educational jurisdiction in which school districts, while guided by provincial policy, retain autonomy for local prioritisation, planning and implementation. For over a decade, school MH initiatives were supported through the School MH Strategy described above rather than formal requirements. This shifted in 2024 with the introduction of a policy mandate requiring districts to adopt key elements of school MH, including multi-tiered systems of support and formalised planning cycles. However, district plans developed in the first year of this mandate are best understood as building on extensive prior investment in implementation of infrastructure and capacity, rather than new efforts.
The Current Study
The comprehensive suite of multi-tiered school MH activities, such as those mapped in Table 1, can be daunting for schools and districts. Significant barriers—including limited infrastructure, workforce capacity and a lack of robust data systems for decision-making—often hinder the uptake, scalability and sustainment of these programs (Hoover & Bostic, 2021; Short, 2016). Consequently, districts must prioritise their implementation efforts systematically.
However, little is known about the real-world “state of play” regarding these priorities. Certain components of school MH may be better aligned with system-level planning than others. Supported by SMH-ON, this study descriptively analysed the collective efforts of Ontario’s 72 autonomous school districts (serving over two million students). We examined which components of an identity-affirming, multi-tiered strategy have achieved widespread uptake and which have remained less implemented.
As jurisdictions transition from guidance-based to mandated MH approaches, baseline system-level evidence is critical. While recent research has documented large-scale initiatives (e.g., Qu et al., 2024; Vetter et al., 2024), the field lacks data on how implementation unfolds across an entire jurisdiction operating under a shared framework. By auditing publicly available district action plans, this study assessed how local planning reflects prior capacity-building and alignment with an evidence-informed provincial framework. These action plans provide a vital baseline for understanding system readiness and implementation variability at the outset of a new mandate.
This study specifically asks: To what extent do district action plans reflect the foundational elements of the provincial strategy developed prior to the new mandate? We interpreted variability across districts as a potential indicator of differential implementation and, by extension, inequities in service provision.
Given the existing implementation supports and SMH-ON Strategy (see Table 1), we proposed the following hypotheses:
Methods
Design
Quantitative manifest content analysis (Kleinheksel et al., 2020) was used to examine how well the public-facing action plans aligned with SMH-ON strategic elements. Quantitative manifest content analysis focuses on describing and enumerating identifiable and observable data in a text, rather than interpreting hidden meanings; as opposed to latent content analysis which focuses on discerning deeper meaning from text (Bengtsson, 2016). Multiple coders were deployed and inter-rater reliability for derived variables was computed to ensure rigour.
Data Sources
In total, data from 61 school districts from a total of 72 possible districts in Ontario (84.7%) were collected, ranging across English Public, English Catholic, French Public and French Catholic school districts.
Ethical Considerations
This study involved analysis of publicly available school district action plans and did not involve human participants or identifiable personal data. In accordance with institutional guidelines, formal research ethics approval was not required. Although district-level documents were publicly available, findings are reported in aggregate to avoid evaluative comparisons of individual districts.
Procedure
Beginning in July 2024 a search was conducted of school districts websites for publicly available action plans, and with monthly searches of any outstanding districts, finishing on December 1, 2024. Action plans were downloaded for content analysis based on the categorical elements using deductive coding.
Coding Framework
Predetermined codes were derived from the SMH-ON Strategy described previously (see Table 1), with coders examining the action plans for the presence of elements. Any reference to an element of that Strategy was sufficient to indicate presence of the element in the action plan. The presence of each component was evaluated by a primary and one of two secondary coders.
Data Analysis
Raters coded for each element of the strategy using dichotomous ratings of the presence/absence of the element. For elements with multiple components (see Table 1), an ordinal summed score of the number of components included in the action plan was computed. All elements included multiple components except Tier 2 Early Identification and Student Support and Tier 3 Intensive Supports and Service Pathways.
To determine inter-rater reliability, two coders randomly selected and coded thirteen of the 61 available action plans, for a total of 26 districts (42.6%) coded by two raters. To select district action plans randomly for dual coding, all available school districts were assigned a random number using Excel’s RAND function; from this sorted list of random numbers. Each coder then coded the 13 selected plans in full. Upon review of the dual-coded districts, any disagreement regarding an element’s presence triggered a structured resolution process for resolution. Coders discussed each case of disagreement until consensus was met, with an adjudicator (author one) moderating when consensus was not forthcoming. Such an approach to rectifying anomalies in coding practices offers methodological rigour in iterative analyses of qualitative data and enables improved transparency and confidence in organising and interpreting data (Cascio et al., 2019). Clarifications were documented to provide a record of what details were needed to indicate the presence of an element (see Supplementary Table 1).
Analytic Approach
Associations of elements were examined using chi-square tests to examine associations of dichotomous variables (i.e., dependency of presence of one element based on presence of another element). To provide an alternate test of the relationship between implementation of the various elements, non-parametric associations were examined between elements using Kendall’s Tau B rank-correlation estimates, which examines associations between ordinal variables (i.e., number of components per element discussed in the plan). This second analytic approach tests whether there is a significant association between greater breadth of implementation between two elements.
Results
Inter-Rater Reliability
For inter-rater reliability, the overall Cohen’s kappa was 0.79, with an overall agreement of 98.0%. All but two categories scored 100% agreement, indicating that both coders agreed on whether districts were referring to some work in that element area. Those two categories (Tier 1 – System, School, Classroom MH Leadership & Tier 3 – Intensive Supports & Service Pathways) had 92.3% agreement between coders.
Strategic Elements of Multi-tiered School Mental Health
To test H1, we examined whether districts reported activity in at least five of the nine SMH-ON Strategy elements. On average, action plans referred to 7.25 of the nine elements (80.5%). In total, 31.1% of districts included plans for all nine school MH strategic elements. Seventy percent of districts referred to at least seven of the nine school MH strategic elements. Only nine districts (14.8%) referred fewer than six elements, and no districts referred to fewer than three elements.
Examining the strategic elements explicitly mentioned in these plans, the most common element referred to in the districts’ action plans was Tier 1 – MH Literacy (59 districts, 96.7%) and the least common was Tier 2 – Early Identification and Student Support (37 districts, 60.7%). Table 2 provides details on the prevalence of each element and component. For Identity-Affirming Supports, districts were more likely to refer to the identity-affirming resources and supports being available and taken up across tiers of intervention (42 districts; 68.9%). Fewer than half of districts included a focus on differentiated responses to mental health needs (24; 39.3%); amplifying diverse perspectives in the district (20; 32.8%); engagement with diverse communities (17; 27.9%); or provision of equitable access to services (14; 23.0%).
Rates of Key Elements and Components, Sorted by Prevalence of Element.
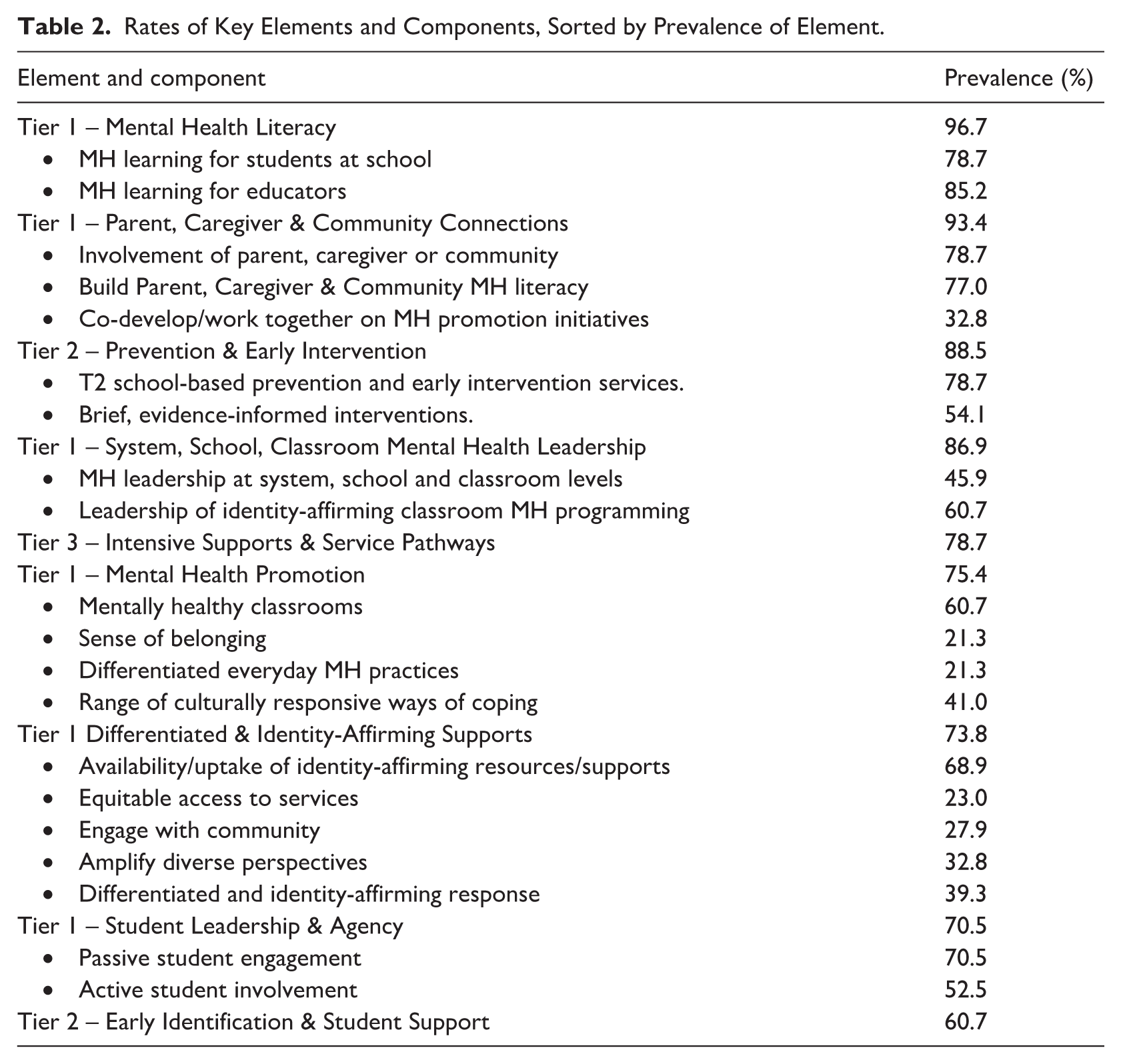
Other components that were explicitly addressed by fewer than half of districts included:
the co-development of MH Promotion initiatives with parent/caregiver or community (32.8% of districts);
addressing MH Leadership at system, school and classroom levels (45.8% of districts);
focusing on sense of belonging as part of MH Promotion (21.3%);
differentiation of everyday MH practices in MH Promotion (21.3%);
addressing culturally responsive ways of coping in MH promotion (41.0%).
Associations Across Implementation of Strategic Elements
To test H2-4, we conducted tests of association on the presence of elements in the action plans and the extent to which the “breadth” of implementation (i.e., implementation of multiple components of an element) is associated across elements (see Table 3). Significant associations (all positive) that were concordant across chi-square (above the diagonal) and Kendall tests (below the diagonal) were (a) Identity-Affirming Support with MH Promotion and with (b) Student Leadership. Tier 1 MH Promotion was also associated with (c) Parent, Caregiver and Community Connections and (d) MH Leadership. Finally, Tier 2 Early Identification & Support and Supports & Service Pathways were significantly associated.
Tests of Association across School Mental Health Multi-tiered Elements.
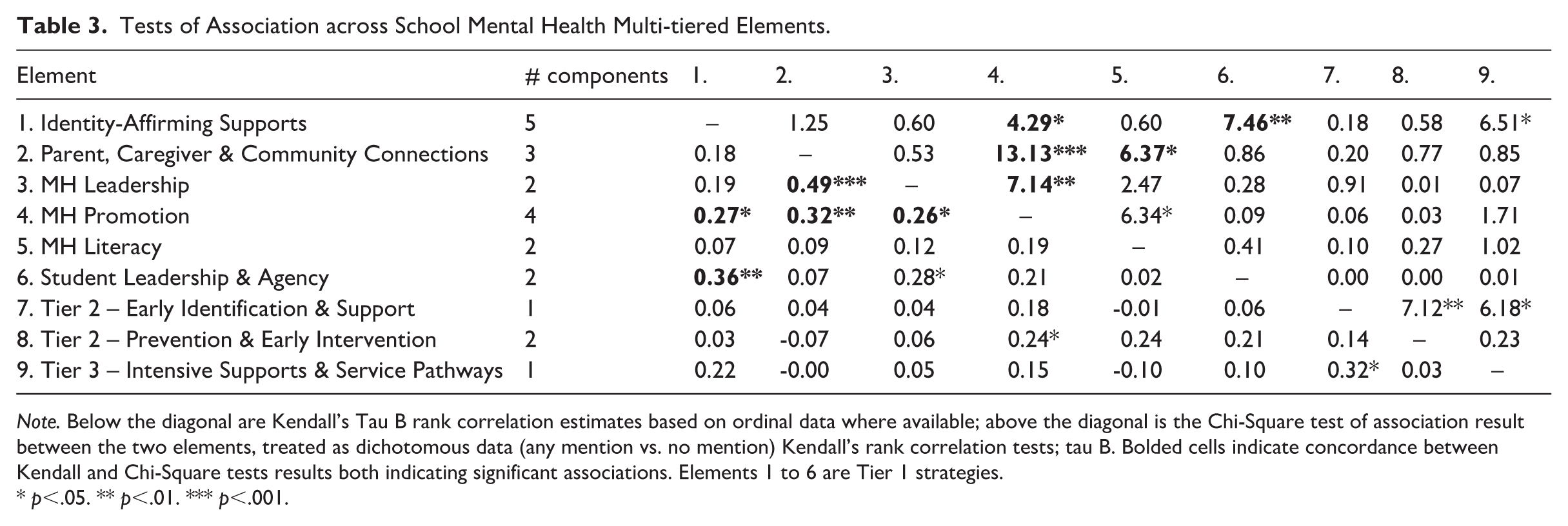
Note. Below the diagonal are Kendall’s Tau B rank correlation estimates based on ordinal data where available; above the diagonal is the Chi-Square test of association result between the two elements, treated as dichotomous data (any mention vs. no mention) Kendall’s rank correlation tests; tau B. Bolded cells indicate concordance between Kendall and Chi-Square tests results both indicating significant associations. Elements 1 to 6 are Tier 1 strategies.
p<.05. ** p<.01. *** p<.001.
Other associations were observed by one method but not the other. Chi-square associations were significant for (a) Parent, Caregiver & Community Connections with Tier 1 MH Literacy; (b) Tier 1 MH Literacy and Tier 1 MH Promotion; and (c) Tier 2 Early Identification & Support with Tier 2 Prevention & Early Intervention. These indicate that the presence of one in an action plan means the presence of the other is more likely but does not speak to the breadth of work on that element.
Discussion
The first hypothesis, that over 50% of districts would have made progress on a five or more of the nine tiered MH elements, was supported. In fact, 90% of districts included at least five elements of the Strategy, and seven in ten districts referred to seven or more elements. The most common strategies ranged across the full MTSS spectrum including Tier 1 strategies (e.g., MH Promotion; MH Literacy), Tier 2 Prevention & Early Iintervention services and Tier 3 Intensive Supports. The presence of these elements in over 75% of district action plans indicates a high level of acceptance and planned implementation activity for MTSS as advocated in the SMH-ON Strategy. Differentiated and Identity-Affirming Supports were also included by almost three out of four districts, with resources and supports the most common implementation targets. This, too, aligns with the SMH-ON Strategy and indicates high acceptance.
Some elements of planning were less prevalent: Tier 2 Early Identification & Student Support and Tier 1 Student Leadership & Agency were the least common elements mentioned in plans. Although this study cannot explain why these are less common than others, the research literature provides some possibilities. Student leadership and voice require agency in the school context and active forms of leadership in particular require adults in the school setting to behave in intentional ways to create opportunities that translate into real change (Pate et al., 2023). Many barriers exist to such agency in the school setting, from adult perceptions of students’ competence to make such decisions through to system-level issues with school and district structures with regard to decision making (Kontak et al., 2025). In particular, such barriers may come into play for active involvement in planning.
A similarly low rate of co-development of Parent, Caregiver & Community Connections initiatives (32.8%) was found. Engaging with parents in an active way shares comparable barriers to granting agency to students (e.g., Garbacz et al., 2020). Culturally sensitive practices are needed that consider and plan for parents/caregivers who do not choose to engage with school, whether due to traditional/cultural backgrounds (e.g., for newcomers from Asian cultures who view schools are outside their sphere of influence; Lin & Yang, 2025) or due to the parent/caregiver’s own negative experiences of their own educational history (e.g., Murray et al., 2014). Structural issues are also of paramount concern here, as those parents/caregivers living in disadvantaged conditions, for example, may face challenges including the need to work during the times when schools can engage, or depend upon public transit services that make the commute too challenging (e.g., Guo & Zhao, 2025; Murray et al., 2014).
In the SMH-ON strategy, Tier 2 Early Iidentification & Support focuses on role-specific learning opportunities to enable and empower more school staff members to identify and support emerging or escalating MH needs. For example, not all school staff have a background in MH – educators in particular – and experience challenges in this area (Reinke et al., 2011) and ambiguity in roles can arise (Beames et al., 2022). Ensuring schools have the capacity to identify students at risk of MH difficulties is particularly important for facilitating MH service use (Green et al., 2013), making this a high priority target for school MH strategic planning.
Hypothesis 2 was partially supported, with significant associations observed between Identity-Affirming Support and Student Leadership. The hypothesised associations of these elements with Parent, Caregiver and Community Connections were not observed. Identity building has been recognised as a key component of MH promotion for students (Brown & Shay, 2021), in particular those with marginalised identities, such that districts clearly see the importance of working proactively with students to ensure identity-affirming support is acceptable to students. The importance of working with parents/caregivers and the broader community may not be as clear to district implementation planners.
Hypothesis 3 was fully supported, with robust associations between Tier 1 elements MH Promotion, Student Leadership and Identity-Affirming Support. This provided support for the fourth hypothesis. Districts may find synergies in planning for these elements. The association with student leadership was not anticipated. MH promotion activities may arise as a priority for districts that engage deeply with students. MH Promotion was also associated with Parent, Caregiver & Community Connections with MH Leadership (school, district and classroom leadership development), although those latter two elements did not themselves show significant associations). It is possible that MH promotion plays a role as an activity hub, linking work across other and activating work in these other areas, although further research is required to replicate and understand how particular elements of school MH strategies may catalyse other work.
Finally, Hypothesis 4 was supported, with significant association between Tier 2 Early Identification & Support and Tier 3 Intensive Supports & Service Pathways. However, these elements both had only component each, making the two tests of association functionally equivalent. Tier 2 and Tier 3 services support students with a variety of MH needs/concerns depending on their level of need. The need to link Tier 2 identification and Tier 3 support was a key part of the Ontario Right Time Right Care initiative, developed by a team of intermediary cross-sectoral partners, including SMH-ON (School and Community System of Care Collaborative, 2022), suggesting that this initiative may have influenced how districts have been planning their own work.
Limitations
A first limitation was that publicly available action plans had no template or requirements regarding form or content, so plans looked vastly different between school districts. Plans varied in form from one page with brief references and general actions through to detailed reports spanning multiple pages and including information on tiers of services and intended audiences. Thus, while some districts may not explicitly reference work in an area, this could be due to the depth of the action plan as a public document, rather than genuine inaction. This may have resulted in an under-estimate of the true extent of activity by districts.
Second, it is important to note that a reference in an action plan does not guarantee action. Whether action plans delivered the planned actions could not be assayed directly and would require a different research design than that used here. However, the presence of planning of an element is an indicator of acceptability of that element.
Third, it cannot be categorically concluded that the Ontario school MH Strategy and work of SMH-ON played a causal role in prioritisation of elements by school districts. Districts were also guided by the expertise available in their own MH lead and within-district expertise, as well as by the Policy/Program Memorandum 169 (PPM169; Ontario Ministry of Education, 2023), which set expectations for work in support of student mental health. Although assessment of the role of PPM169 on action planning is beyond the scope of this work, it is important to note that PPM169 requirements align with SMH-ON strategy elements in many cases. For example, PPM169 refers to mandatory MH literacy for students and family MH literacy and awareness, which are a key part of the SMH-ON strategy and maps onto the two most prevalent elements observed in action plans across Ontario’s districts.
Finally, the review of district action plans speaks to the acceptability and prioritisation of strategic elements but provides less insight into the background foundational work required for implementation. Ensuring the organisational conditions for the uptake and sustainment of school MH activities requires deliberate efforts to ensure the buy-in and commitment of district and school leaders. As well, clear communication of the vision, strategy and action plans are needed to ensure that policies and protocols are enacted and roles are clarified, to sustain the efforts required to engage meaningfully with students, families and the broader school community, and to ensure a culture of data-driven decision making (Dryburgh et al., 2025). These implementation foundations are related to elements examined in this article, some of which were among the most prevalent (e.g., Tier 1 MH Leadership; Tier 1 Parent, Caregiver & Community Connections). However, this study is limited in not providing insight directly into the implementation foundations.
Conclusion
This study found that Ontario school districts, as outlined in their district action plans, demonstrated a higher-than-anticipated level of alignment with the school MH provincial strategy. This underscores the value of provincial direction and implementation support to achieve systemic change within school districts and within the districts’ system of care. Deeper research into the on-the-ground implementation of these planned actions is needed to provide further insight into how to enact jurisdiction-wide student mental health supports.
In identifying areas of correlated planning, this study begins to lay a conceptual foundation for multi-tiered school MH activity that can inform research and practice in school settings. The descriptive information on the progress of school districts in implementing specific elements of a multi-tiered school MH strategy may enable more efficient implementation planning by system leaders. Identification of potential areas of complementary or synergistic elements may further be used to and scaffold implementation of associated activity. Identifying specific roles within districts and schools that align with those correlated elements may enable more proactive and effective collaboration between professionals whose work is integral to different but associated elements. Although these associations require replication, they may provide insight into the “natural history” of implementation of school MH activities, which may be leveraged to expedite implementation planning.
Supplemental Material
sj-docx-1-spc-10.1177_20556365261450641 – Supplemental material for Acceptability of a Multi-Tiered, Identity-Affirming School Mental Health Strategy: An Audit of Ontario School District Action Plans
Supplemental material, sj-docx-1-spc-10.1177_20556365261450641 for Acceptability of a Multi-Tiered, Identity-Affirming School Mental Health Strategy: An Audit of Ontario School District Action Plans by Kevin Runions, Naya Moser, Trisha Woehrle, Tracy Weaver, Michelle Bates and Robert Chin-See in Journal of Psychologists and Counsellors in Schools
Footnotes
Acknowledgements
All authors were employed by School Mental Health Ontario during conduct of the audit. We thank Kathy Short for her insightful comments on the manuscript.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Authors were employed by School Mental Health Ontario, a provincial program of the Ministry of Education in Ontario, which may experience benefits from this publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.