
Abstract
Many school staff respond to student suicide and suicidal behaviour (S/SB). Secondary traumatic stress (STS) refers to symptoms, such as intrusion, avoidance, arousal and emotional numbing following secondary exposure to a traumatic event. This study investigated whether school staff experienced STS following student S/SB. Aligning with the compassion fatigue resilience model, the relationships between protective factors of self-care, detachment, sense of satisfaction and social support and STS following student S/SB were investigated. Two STS measures were used, with a focus on self (Impact of Event Scale-Revised [IES-R]) and helping others (Secondary Traumatic Stress Scale [STSS]). Australian school staff (N = 134) with experience of student S/SB responded to an anonymous online survey. On average, participants reported STS levels of clinical concern on both measures following student S/SB, measured by previous research benchmarks. Hierarchical regression analyses found fatality and greater sense of satisfaction were significantly related to greater STS–self, and females reported significantly greater STS–helping others. Greater detachment and social support were significantly related to lower STS (self and helping others), supporting further research and interventions on these protective factors. School counsellors are encouraged to advocate for trauma-informed approaches in schools.
Keywords
Introduction
Australian school staff, which include teachers, leaders, school counsellors, psychologists and others, respond to student suicide and suicidal behaviour (S/SB; Kõlves et al., 2017). Suicide refers to the intentional act of a person ending their own life, while suicidal behaviour refers to one or more of suicide ideation, having a suicide plan and suicide attempt (O’Connor & Nock, 2014). Suicide is a leading cause of death for Australian young people, representing 31.8% of all deaths in people aged 15 to 17 years in 2023, up from 16.5% in 2001. Suicide rates for First Nations people aged 0 to 24 years were 3.1 times higher than non-Indigenous Australians (Australian Institute of Health and Welfare, 2025). The most recent reporting of suicidal behaviours for Australians aged 12 to 17 years include 7.5% having suicidal ideation, 5.2% a plan and 2.4% a suicide attempt (Lawrence et al., 2015). Thus, school staff are likely to experience student S/SB, however impacts on staff have received little attention (Kõlves et al., 2017).
One study has explored the impact of student suicide on Australian teachers. Kõlves et al. (2017) sampled 145 teachers and noted 52 (35.9%) had experienced at least one student suicide event, with high levels of distress reported and additional staff support needs identified. Internationally, there has been a historical lack of reporting but recently, Tiech Fire et al. (2023) surveyed counsellors, psychologists, teachers and principals from 29 suicide impacted schools in Israel and found that positive school climate had a favourable effect on staff coping. Further, Tiech Fire et al. (2022) reported Israeli principals and teachers had higher levels of complicated grief and post-trauma symptoms than counsellors and psychologists in these schools. Kim (2019) interviewed Korean teachers following student suicide and found bereavement and shame were present. Finegan (2024) interviewed 11 Irish school guidance-counsellors about student suicide and noted the experience presented potential for moral injury and compassion fatigue.
Secondary traumatic stress
Secondary or indirect trauma exposure provides one lens through which to interpret school staff’s experience of student S/SB. STS has been defined as ‘a constellation of symptoms that may run parallel to those of post-traumatic stress disorder (PTSD), including symptoms of intrusion, avoidance, arousal and emotional numbing’ (Molnar et al., 2017, p. 130) and is also known as compassion fatigue. Research on secondary trauma exposure for school staff is increasing. A US study (Borntrager et al., 2012) reported that 75% of school staff (N = 229) working with traumatised students experienced high STS. Simon et al. (2022) found a direct association between teacher reported levels of student socio-emotional difficulties and teachers’ STS symptoms. In Kolves’ et al. (2017) study, 51 teachers completed the Impact of Event Scale–Revised (IES-R; Weiss, 2004), and retrospectively reported on their experience in the 7 days following the student suicide. Average scores signified stress levels of potential clinical concern.
The Compassion Fatigue Resilience model
The Compassion Fatigue Resilience (CFR) model (Ludick & Figley, 2017) conceptualises the trauma induction and reduction process, including a range of protective factors leading to resilience outcomes, and is proposed as a workplace model covering multiple sectors, including education (see Brown & Biddle, 2023). The CFR model considers multiple components in response to exposure to suffering, with compassion fatigue resilience as the outcome (Figure 1). Self-care describes the practice of behaviours and thoughts that lead to maintenance of good health and wellbeing, to be attended to at individual and workplace levels (Figley & Figley, 2017). Detachment, measured through decentering as recommended by Ludick and Figley (2017), refers to the capacity to notice one’s feelings and thoughts from a detached perspective. Sense of satisfaction refers to fulfilment arising from doing work well and helping others, while social support describes perceived support available to access when needed (Figley & Figley, 2017).
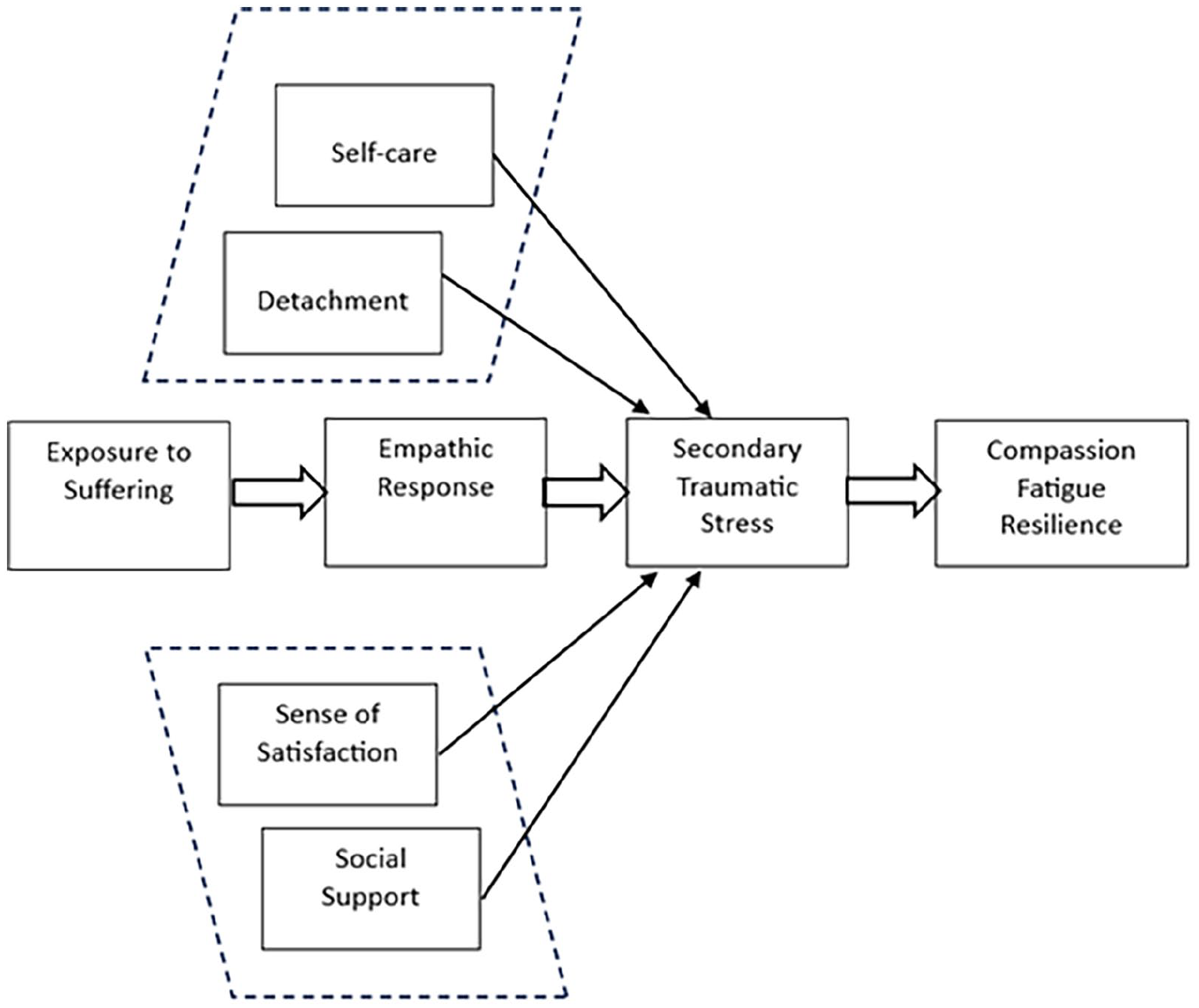
Protective factors (in dotted lines) within the compassion fatigue resilience model (amended from Ludick & Figley, 2017, p. 114).
The present study
There is little research on the impact of student S/SB on teachers (Kolves et al., 2017). This study investigated staff reports of student S/SB and employed the compassion fatigue resilience component of Ludick and Figley’s (2017) model as a framework to examine associations between protective factors and STS. STS includes the effects of indirect trauma exposure on self (self) and in roles involving helping others (helping others). It was hypothesised that staff would experience STS following student S/SB. Further, the paths from the four factors self-care, detachment, sense of satisfaction and social support to each type of STS would be negative and significant, after taking into account age, gender, years of experience in schools at time of event and event fatality status.
Method
Participants
Approval was provided by Charles Sturt University Human Research Ethics Committee (H19105). An information statement including informed consent and support services was provided to participants. The study was open to current and previous school staff in Australia and was commenced by 196 school staff, with 124 (63.3%) completing all questions. Demographic and student S/SB questions were completed by 139 (70.9%) participants, including 119 (85.6%) females and 20 (14.4%) males. Mean age was 40.76 years (SD = 10.11) and average school workplace experience was 16.05 years (SD = 9.50). Roles included 72 (51.8%) teachers, 52 (37.4%) school leaders including principals, deputy principals, head of welfare/wellbeing and other leaders and 15 (10.8%) others, including school counsellors and psychologists.
Materials
Demographic items included gender (male/female/other/prefer not to say), age (18–70 years), professional role (teacher/school leader/principal/other) and years of school experience (0–50). Participants were asked if they were aware of a student who died by suicide or demonstrated suicidal behaviours while working at school (yes/no). A no response ended the survey, and a yes response continued with a question concerning frequency of experiences (1–20 and 20+). Participants were asked to consider the event with greatest personal impact for all following questions, including event recency (0–6 months ago, 6 to 12 months, each of 1 to 9 years and 10+ years); their role at the time, (teacher/school leader/principal/other) and fatality status.
Scales
Two measures of STS were employed, each with a different focus. The Impact of Event Scale-Revised (IES-R, Weiss, 2004) measures subjective distress response to an event and the impact of this experience on self (‘STS–self’). It measures three clusters of symptoms aligned with PTSD: intrusion, avoidance and arousal (Weiss, 2004). It was used in a similar study with student suicide and teachers (Kõlves et al., 2017), and client suicide and social workers (Ting et al., 2011). Participants responded using a 5-point scale from 0 (not at all) to 4 (extremely) with respect to the 7 days following the incident, in line with previous studies (Kõlves et al., 2017; Ting et al., 2011). Higher summed total scores reflected greater traumatic stress. Internal consistency was excellent, Cronbach’s α = .94.
The Secondary Traumatic Stress Scale (STSS, Bride et al., 2004) is a 17-item self-report scale that measures symptoms of arousal, avoidance and intrusion related to indirect exposure of helpers to others’ experience of traumatic events (‘STS–helping others’). The STSS has been previously used with school personnel (Borntrager et al., 2012). Participants responded using a 5-point scale with respect to the 7 days following the event (1 = never to 5 = very often). Higher summed total scores reflected greater traumatic stress. Internal consistency was excellent, Cronbach’s α = .95.
The Denyes Self-Care Practice Instrument (DSCPI, Denyes, 1990) measures self-care in healthy populations. Participants answered using a scale from 0 (none of the time) to 100 (all of the time) to rate their responses to statements from the revised 12-item scale (Andrews et al., 2009). Higher summed total score indicated greater self-care. Internal consistency was excellent, Cronbach’s α = .94.
The Experiences Questionnaire-Decentering (EQ-D, Fresco et al., 2007) is an 11-item scale which measures decentering, the capacity to notice and attend to one’s thoughts and feelings in a detached way. Participants responded using a 5-point scale (1 = never to 5 = always), with higher summed total scores reflecting greater ability to notice and attend to one’s experiences. Internal consistency was excellent, Cronbach’s α = .92.
The Professional Quality of Life Scale, Compassion Satisfaction subscale fifth edition (ProQOL-CS, Stamm, 2010) measures the pleasure one experiences when feeling able to help others. It is a 10-item instrument utilising a 5-point scale (1 = never to 5 = very often), with higher summed total scores reflecting greater sense of satisfaction. Internal consistency was excellent, Cronbach’s α = .91.
The Social Support Scale (SSS) measures the perceived availability of social support to an individual (Sherbourne & Stewart, 1991). The four items chosen from the 18-item self-report survey had been used for brevity by Figley and colleagues in previous work with trauma exposed professional populations (Adams et al., 2006). Participants responded using a 5-point scale (1 = none of the time to 5 = all of the time). Summed total scores reflected greater social support. Internal consistency was excellent, Cronbach’s α = .84.
Procedure
The online survey used a cross-sectional design with a sample of Australian school staff who had experienced student S/SB. Volunteer participants were anonymously recruited via social media (Facebook, LinkedIn and Twitter) and confidentiality was assured. Participants were also recruited from the university student population (n = 12, receiving course credit), and the Prolific research recruitment website (n = 6, receiving nominal payment). Quantitative analyses were conducted in IBM SPSS Statistics Version 25 for Windows.
Results
Frequency of school staff experience of student S/SB
Of the 139 participants who completed demographic and experience of student S/SB questions, 134 (96.4%) had experienced student S/SB. 18.7% (n = 25) noted one instance, 17.9% (n = 24) indicated two instances, 47.7% (n = 64) named three to nine instances and 15.7% (n = 21) stated 10 or more instances. Participants were asked to consider the event with greatest personal impact for all following questions. Fifty-four participants (40.3%) reported a suicide event, and 80 (59.7%) reported a suicidal behaviour event. Time since the event included 25.4% (n = 34) in the last 6 months, 17.9% (n = 24) between 6 and 12 months, 29.1% (n = 39) between 1 and 3 years prior, 21.6% (n = 29) 4 to 9 years prior and 6% (n = 8) occurring 10+ years prior.
Inferential analyses
Two hierarchical multiple regression analyses were conducted, one with STS-self as the criterion variable and one with STS–helping others as the criterion variable. Both analyses entered gender and years of experience at time of event at Step 1, fatality status at Step 2 and self-care, detachment, sense of satisfaction and social support at Step 3. Descriptive statistics and Pearson’s bivariate correlations are reported in Table 1.
Bivariate Pearson’s correlations between variables and descriptive statistics.
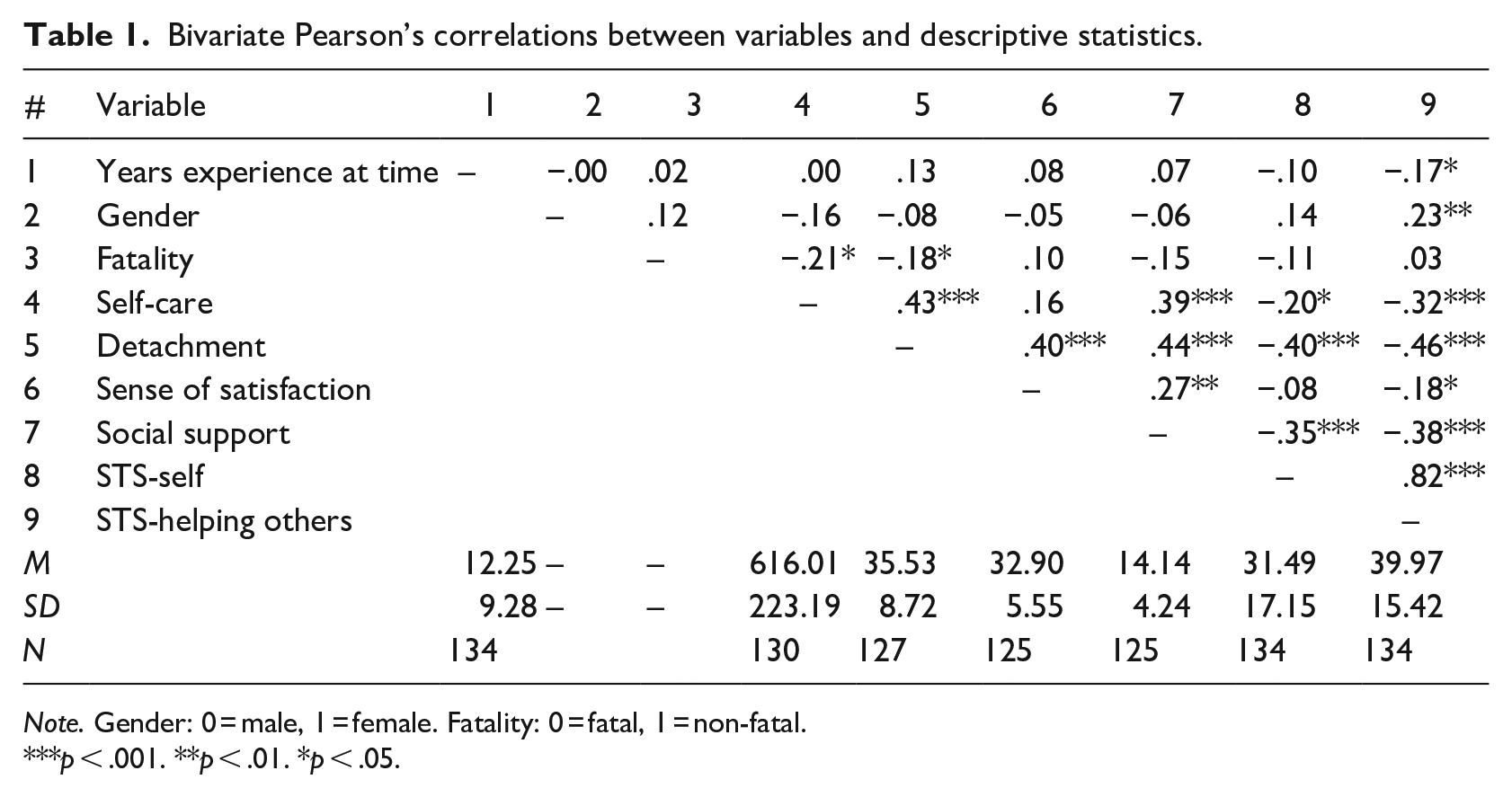
Note. Gender: 0 = male, 1 = female. Fatality: 0 = fatal, 1 = non-fatal.
p < .001. **p < .01. *p < .05.
Assumptions
A statistical power analysis using G*Power 3 (Faul et al., 2007) for hierarchical multiple regression with seven predictors showed a sample of 85 was required to achieve power of 0.80, using a medium effect size of f 2 = 0.15 and alpha of .05. The sample size (N = 124) was adequate. There were no univariate or multivariate outliers. Shapiro Wilk’s tests of normality indicated significant concerns (p < .05) for years of experience at time of event, STS–self, STS–helping others, sense of satisfaction and social support. To address non-normality bootstrapping with 5,000 bootstrap samples was used (Tabachnick & Fidell, 2013). All other assumptions were met.
Hierarchical regression: STS-self
Tables 2 and 3 report the hierarchical regression analysis for STS–self. As shown in Table 2, none of the variables at Step 1 and Step 2 were significant, but the overall model at Step 3 was significant, with 29% of variance accounted for. The combined effect size was large (f 2 = 0.40; Cohen, 1988). The four factors of self-care, detachment, sense of satisfaction and social support contributed significantly to the total variance (Table 2), and individually three of these four factors were statistically significant (Table 3). Detachment contributed 9%, sense of satisfaction 3% and social support 5% of unique variance to STS–self. Self-care was not significantly associated with STS–self. Greater detachment and social support were significantly associated with lower STS–self, and greater sense of satisfaction was significantly associated with greater STS–self. At Step 3, fatality was significantly associated with greater STS–self, contributing 6% unique variance. Gender was not significant.
Hierarchical multiple regression for STS-self (criterion variable): gender, years’ experience (step 1), fatality status (step 2), self-care, detachment, sense of satisfaction and social support (step 3).
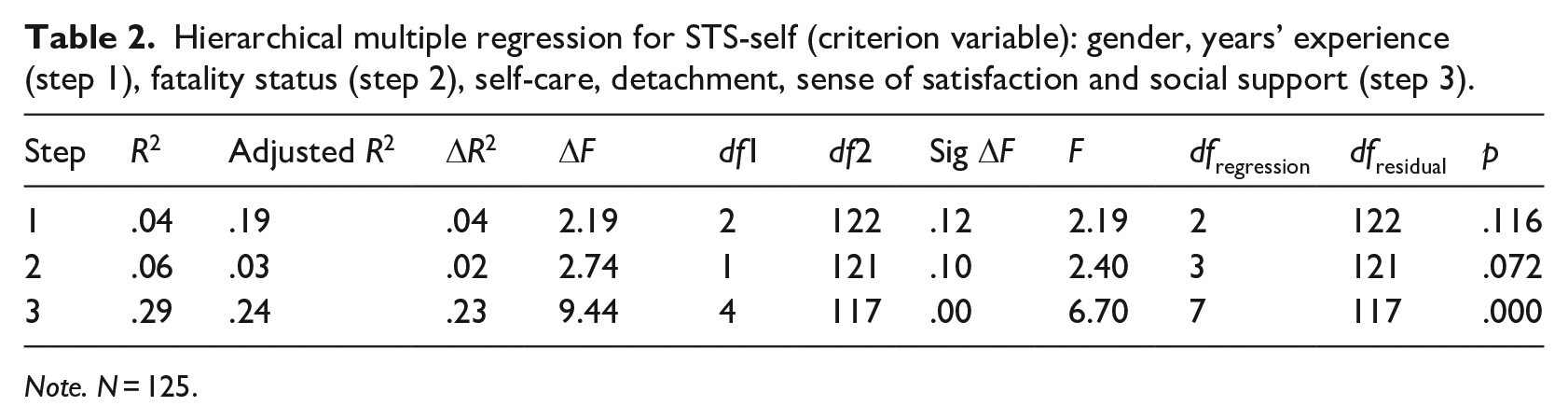
Note. N = 125.
Regression coefficients, confidence intervals and significance of predictors of STS-self.
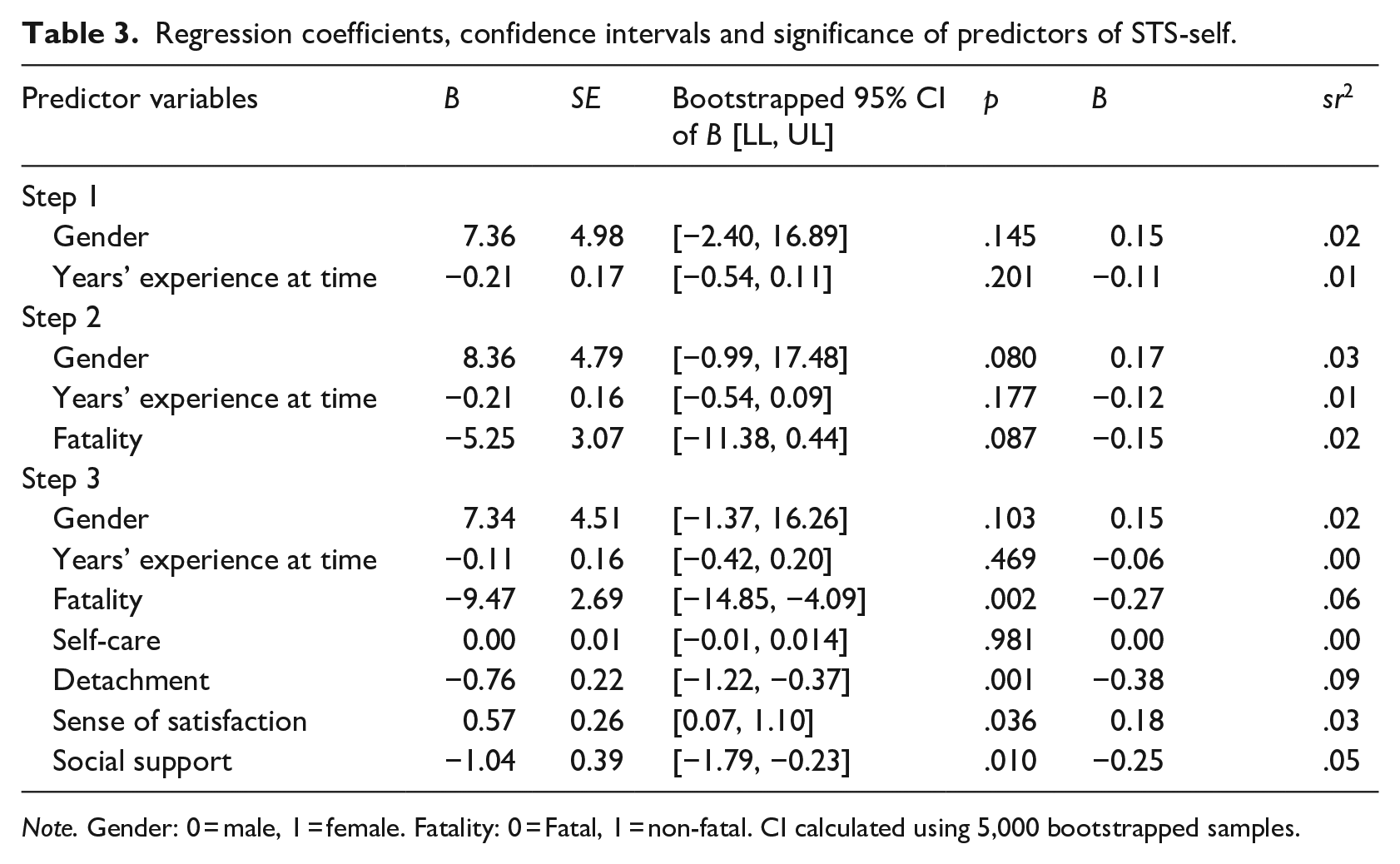
Note. Gender: 0 = male, 1 = female. Fatality: 0 = Fatal, 1 = non-fatal. CI calculated using 5,000 bootstrapped samples.
Hierarchical regression: STS–helping others
Tables 4 and 5 report the hierarchical regression analysis for STS–helping others. All steps in the model were significant (Table 4), with 32% of variance in STS–helping others explained at Step 3 and a large effect size (f 2 = 0.46, Cohen, 1988). In Steps 1, 2 and 3, gender contributed significant unique variance, with females associated with greater STS-helping others (Table 5). Years’ experience at the time was not significant at any step, and fatality status was also not significant in Steps 2 or 3. At Step 3, greater detachment was significantly associated with less STS–helping others, contributing 7% unique variance. Social support was borderline significant, with confidence intervals from bootstrapped B values supporting significance. Self-care and sense of satisfaction were not significant.
Hierarchical multiple regression for STS-helping others: gender, years’ experience (step 1), fatality status (step 2), self-care, detachment, sense of satisfaction and social support (step 3).
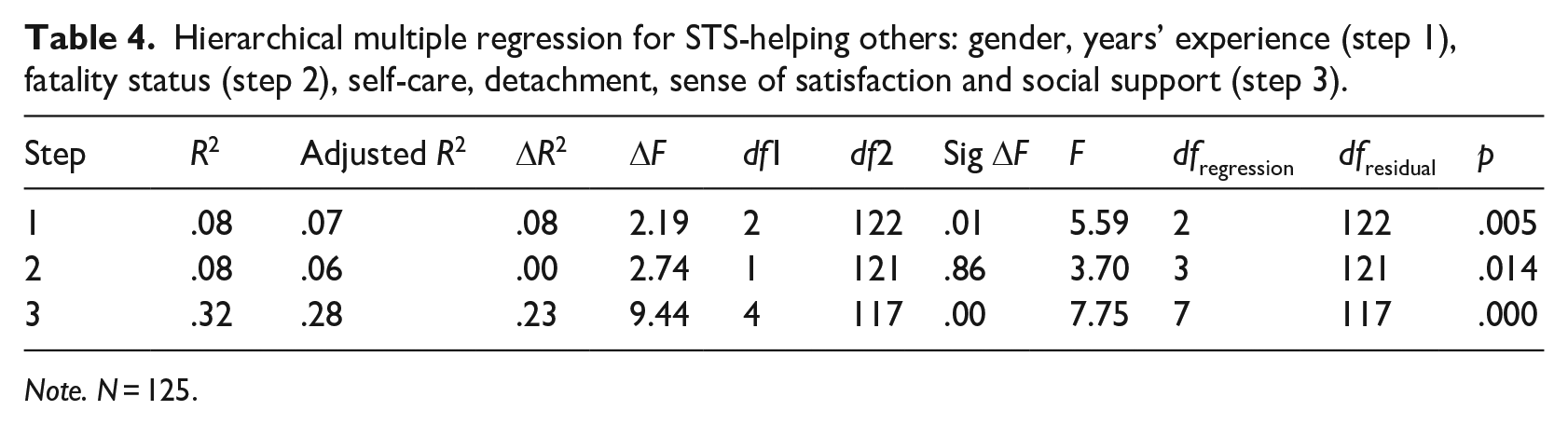
Note. N = 125.
Regression coefficients, confidence intervals and significance of predictors of STS-helping others.
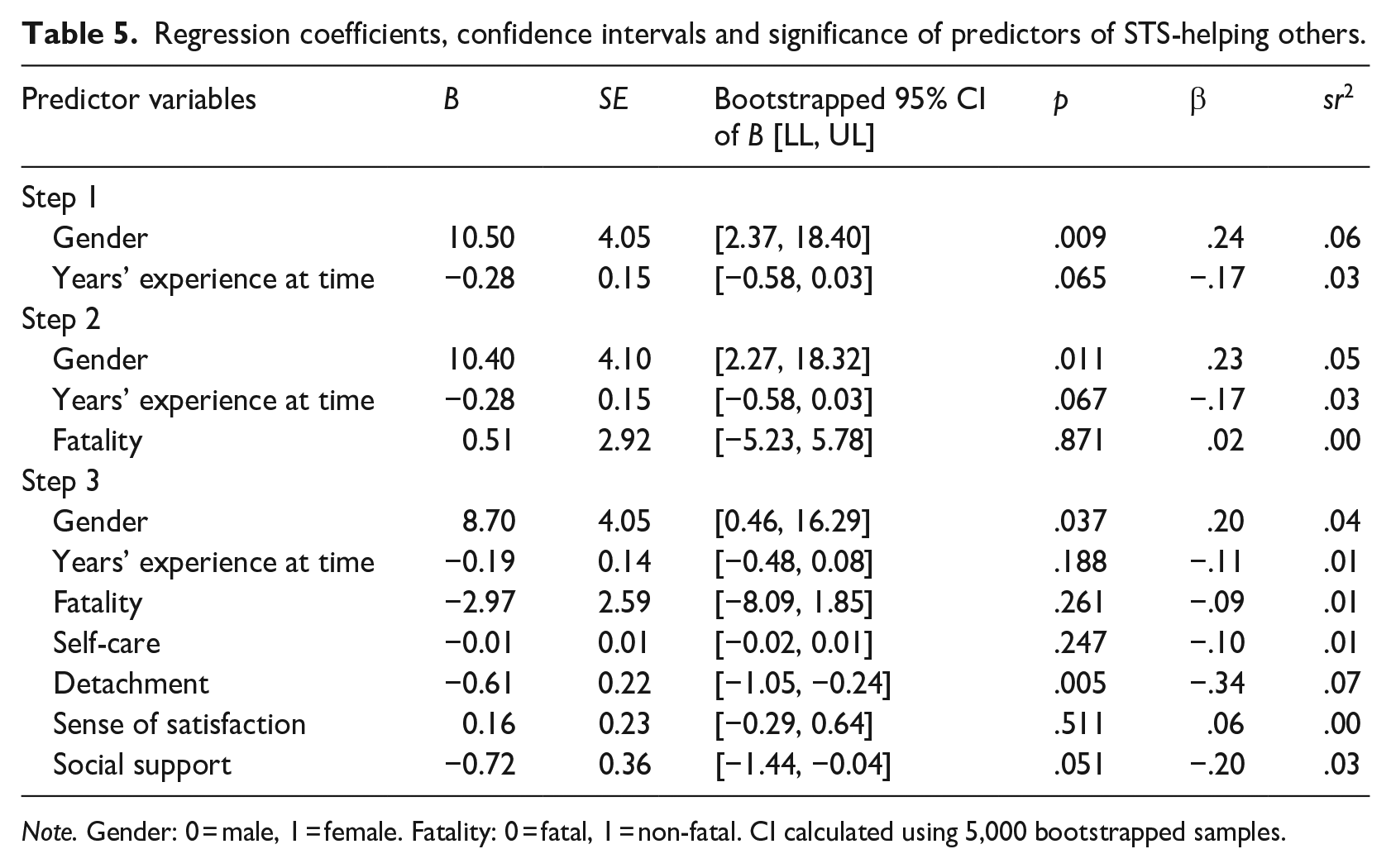
Note. Gender: 0 = male, 1 = female. Fatality: 0 = fatal, 1 = non-fatal. CI calculated using 5,000 bootstrapped samples.
Discussion
The study aimed to investigate the traumatic stress impacts of student S/SB on school staff, and to explore protective factors that may mitigate these impacts from the CFR model (Ludick & Figley, 2017). The first hypothesis that staff would experience STS following experiences of student S/SB was supported, with staff average scores suggesting concerning levels of STS on both measures. The second hypothesis that the four protective factors of self-care, detachment, sense of satisfaction and social support would each significantly negatively predict each type of STS was partially supported. As expected, greater detachment and greater social support predicted lower STS on both measures. Unexpectedly, greater sense of satisfaction predicted higher STS–self. Fatality also predicted higher STS–self, and female gender predicted higher STS–helping others.
Extent of school staff’s secondary traumatic stress
On average, school staff reported concerning levels of traumatic stress in both analyses, with fatality status accounting for unique significant variance in STS–self. Similar to previous studies using the IES-R (Séguin et al., 2014), a cut-off point of 25 identified those with levels of potential clinical concern of STS–self. In this study, participants’ mean score on the IES-R was approximately 6.5 points above this cut-off (Table 1), higher than the previous study of teachers (Kõlves et al., 2017) and psychiatric nurses (Takahashi et al., 2011), who had experienced client loss by suicide.
Similarly, the STSS–helping others scale author (Bride, 2007) advised a cut-off score of 38 identified those with levels of potential clinical concern. In this study, the mean score was approximately two points above this cut-off (Table 1) and was similar to school personnel supporting traumatised students (Borntrager et al., 2012), and higher than social workers who had experienced a client suicide (Ting et al., 2011). The data supports student suicide and suicidal behaviour leading to notable effects for school staff wellbeing, a substantial finding due to both the prevalence of student suicidal behaviour, and the differing work contexts of school staff from the mental health sector requiring different school and systemic responses.
The CFR model: Protective factors
Detachment (decentering) contributed the greatest amount of unique variance to overall traumatic stress scores in both analyses, with greater detachment associated with less STS. The study’s findings align with research supporting decentering or trait mindfulness as inversely related to post or secondary traumatic stress symptoms in workers (Yuan et al., 2022). Greater social support was associated with lower STS on both measures and align with literature supporting the mitigating role social support can play in STS (Hensel et al., 2015). School staff who perceive they have sound support networks may feel connected and have their needs met as they respond to the needs of others (Figley & Figley, 2017). Sense of satisfaction had a significant, positive contribution to STS–self. This positive contribution is opposite to what was hypothesised but is consistent with research by Borntrager et al. (2012). Sprang et al.’s (2024) systematic literature review reported that STS and compassion satisfaction are often both present in workers in helping professions.
Strengths and limitations
The study’s strength is that it provides evidence for previously anecdotal knowledge concerning the impacts of student S/SB on school staff. It identifies selected protective factors of STS and supports international studies (Cafaro et al., 2023; Newton at al., 2024) that promote systematic delivery of trauma-informed professional development and practices in schools. That said, the cross-sectional design limits predictive capacity and the convenience sample, with males under-represented, limits generalisability. While the CFR model was supported, it contains 13 constructs (Ludick & Figley, 2017) and only five were investigated. It is noted that some factors did make significant contributions in directions associated with ameliorating STS. Following similar studies (Kõlves et al., 2017; Ting et al., 2011), instructions for the scales were amended to ask participants to consider the 7-day period following the event, however it is noted that recall bias may have impacted participant responses, given the time since the event covered a large span.
Implications
Given the evidence of concerning levels of STS in school staff, school-wide trauma-informed interventions have the capacity to reduce these symptoms (Sprang & Garcia, 2022). There is growing support for these initiatives internationally, with accompanying systematic reviews and meta-analyses (Cafaro et al., 2023; Newton at al., 2024). Many Australian schools are introducing trauma-informed initiatives (Rodgers et al., 2021), although they are not yet systematically provided. Inclusion in policy, and research on the effectiveness of these interventions with a focus on staff wellbeing, would be valuable contributions. Australian school counsellors overwhelmingly hold tertiary qualifications in counselling, social work or psychology and many government schools employ only psychologists. Their varied role may include critical incident management or support, as well as trauma-informed approach advocacy and mentoring, all of which they are well placed to offer.
The study found evidence supporting some relationships from the CFR model within schools. The decentering scale used to measure detachment links to mindfulness and self-compassion (Fresco et al., 2007) and research and interventions focussed on increasing staff’s capacity to decentre, and also access social support may be beneficial. Future research to support the model in school settings should incorporate other CFR model elements.
Conclusion
This study offers valuable new evidence on the impact of student suicide on school staff, and illuminates key protective factors. Notwithstanding limitations, an important finding was that, on average, staff experience concerning levels of STS symptoms following student S/SB. Greater detachment and social support were related to lower STS, supporting further research and interventions on these factors from the CFR model. School counsellors are encouraged to advocate for trauma-informed approaches within their schools.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by both authors. The first draft of the manuscript was written by Melinda Phillips. Donnah Anderson reviewed and edited all subsequent versions of the manuscript. All authors read and approved the final manuscript.
Data availability statement
Data is published in figshare: 10.6084/m9.figshare.26891296.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Ethics was approved by the Charles Sturt University Human Research Ethics Committee: Approval/Protocol Number: H19105.
Informed consent statement
Participants gave their informed consent to participate in the study, for publication and for a summary data file to be stored in a public data repository.