
Abstract
Keywords
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune inflammatory disease of the central nervous system. 1 It is commonly found in women and primarily affects people of ∼40 years of age.2,3 In Mexico, the adjusted prevalence of NMOSD is 0.71/100,000, and adjusted incidence is 1.87/1,000,000 person-years. 4 Individuals with NMOSD exhibit common clinical features, including optic neuritis, myelitis, brain syndromes, cognitive, and neuropsychiatric problems.5–8
Patients with NMOSD often experience significant functional limitation, high rates of disability, and cognitive impairment.9–15 Disability resulting from NMOSD has a significant economic impact on the health care and social system.16,17 Previous studies describe factors associated with cognitive impairment.18–20 However, differences in healthcare systems among certain countries is an important determinant. In Mexico, there is a lack of information about the characteristics associated with cognitive impairment (CI). Therefore, the purpose of this study was to evaluate the factors associated with CI in patients diagnosed with NMOSD in Mexico.
Materials and methods
We conducted a cross-sectional study in the neurology department of a tertiary care center (Centro Médico Nacional de Occidente at Instituto Mexicano del Seguro Social) in Guadalajara, Mexico. The present study included 65 Mexican adults diagnosed with NMOSD who were divided into two groups. The first group consisted of 34 NMOSD patients with CI (CI group), and the second group comprised of 31 NMOSD patients without CI (non-CI group). Inclusion criteria consisted of (a) a diagnosis of NMOSD (following the 2015 International consensus diagnosis criteria for NMOSD. 1 Importantly, all medical records of NMOSD patients were reviewed by neurologist researchers; (b) have a signed informed consent form; (c) be between 18 and 60 years of age at the time of the cognitive assessment; and (d) have no visual or auditory problems that could affect cognitive tests performance (information was corroborated in the neurology consultation). The study excluded participants who (a) reported a history of a neurological or psychiatric diagnosis; (b) substance and/or alcohol consumption; (c) having relapsed within the last 30 days of cognitive assessment; and (d) having received corticosteroid treatment within the last 30 days.
Definition of CI group and non-CI group
The CI group was described as patients with scores of two or more standard deviations below the mean compared to healthy controls (HCs) in Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS) tests. Additionally, patients with scores below the mean by two or more standard deviations in two or more cognitive impairment domains were classified as having CI. The non-CI group was described as patients with an NMOSD diagnosis, who did not have CI.
We selected the CI criteria based on the clinical experience of the neuropsychologist participating in this study, and previously published reviews.21–24
Three steps were required to determine CI in NMOSD patients. First, we included 65 HCs. HCs were recruited from the general population in Guadalajara, Mexico. These 65 HCs were selected to match the NMOSD sample on demographic characteristics. The groups did not differ in age (p = 0.900), years of education (p = 0.540), and sex (p = 0.677). Second, we compared the cognitive functioning of NMOSD patients and HCs. A student’s t-test showed statistically poor performance by NMOSD patients compared to HCs on all three neuropsychological tests scores. This difference was observed in the symbol digit modalities test (SDMT) (p < 0.001); the California verbal learning test (CVLT-II) (p < 0.001), and the brief visuospatial memory test-revised (BVMT-R) (p < 0.001) (Table 1). Third, a Student’s t-test showed statistically poor performance in the CI group compared to the non-CI group on all three neuropsychological tests scores. This difference was observed in the SDMT (p = 0.004), the CVLT-II (p < 0.001), and the BVMT-R (p < 0.001) (Table 2). Neuropsychological tests were conducted by trained assistants and master’s students under the guidance of a board-certificate clinical neuropsychologist.
Demographics characteristics and neuropsychological test scores between patients with NMOSD and HCs.
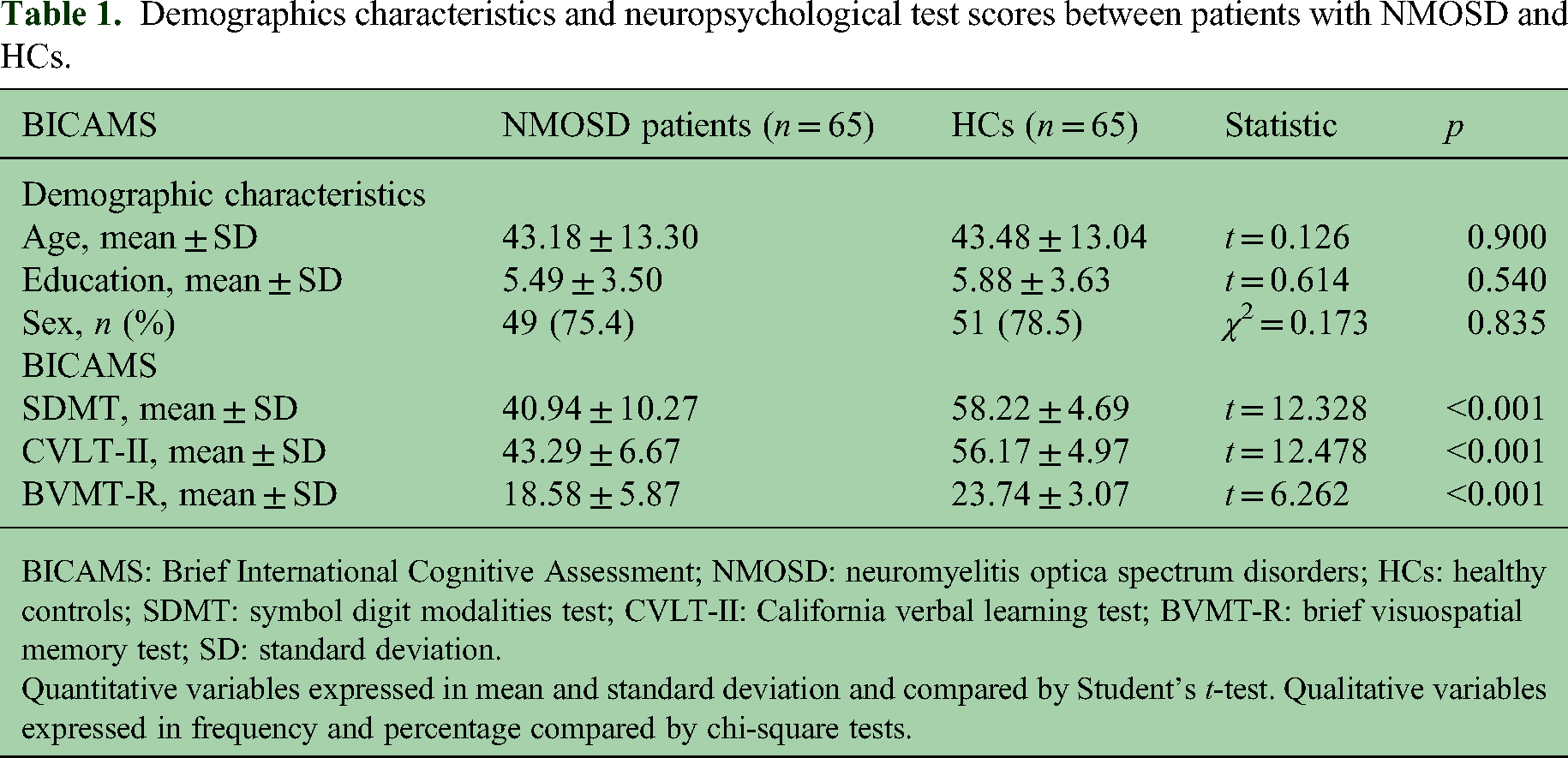
BICAMS: Brief International Cognitive Assessment; NMOSD: neuromyelitis optica spectrum disorders; HCs: healthy controls; SDMT: symbol digit modalities test; CVLT-II: California verbal learning test; BVMT-R: brief visuospatial memory test; SD: standard deviation.
Quantitative variables expressed in mean and standard deviation and compared by Student’s t-test. Qualitative variables expressed in frequency and percentage compared by chi-square tests.
Neuropsychological test scores between patients with cognitive impairment (CI group) versus patients without cognitive impairment (non-CI group).

BICAMS: Brief International Cognitive Assessment; CI group: patients with cognitive impairment; non-CI group: patients without cognitive impairment; SDMT: symbol digit modalities test; CVLT-II: California verbal learning test; BVMT-R: brief visuospatial memory test; SD: standard deviation.
Quantitative variables expressed in mean and standard deviation and compared by Student’s t-test.
Potential risk factors
We identified several factors associated with CI. We selected potential risk factors based on the clinical experience of our neurologists and neuropsychologists participating in this study; and a review of factors previously reported in the literature.18,20,25–33 Risk factors included (1) sex (classified as male and female), (2) age divided into two groups (<50 years of age and ⩾50 years of age), (3) educational level (classified as 1 to ⩽6 years of education and >6 years of education), (4) time from onset from first symptoms of NMOSD to diagnosis (<12 months and ⩾12 months), (5) time from onset to treatment (<60 months and ⩾60 months), (6) presence of aquaporin-4 antibody (AQP-4-ab) (AQP-4-ab-positive and AQP-4-ab-negative), (7) immunosuppressive treatment indicated by the neurologist (azathioprine (AZA) and rituximab (RTX)), (8) brain lesion, (9) Expanded Disability Status Scale (EDSS) at the first appointment (<4.0 and ⩾4.0), (10) hospitalization by NMOSD (yes and no), and (11) relapses by NMOSD ⩾ 4 (yes and no).
Procedures
The present study was designed in accordance to the principals of the 64th Declaration of Helsinki (last revision in Fortaleza, Brazil, 2013). Participants who met the inclusion/exclusion criteria were invited to complete the BICAMS. 34 BICAMS comprised of the SDMT, the CVLT-II, and the BVMT-R.35–39 Data collection from NMOSD participants began in January 2021 and ended in December 2022. All participants in both groups were volunteers and received no financial compensation for their participation.
Statistical analysis
We used statistical software R version 4.0.3 (R console Team 2020) to perform statistical analyses. Kolmogorov–Smirnov and Levene’s tests were utilized to evaluate normal distributions and homoscedasticity of quantitative variables in both groups. A majority of scores met the assumption of normality and homoscedasticity. Qualitative variables were described as frequencies (%). For univariate analyses we used chi-square tests or Fisher’s exact tests (when required). To compare means of quantitative variables between NMOSD versus HCs and CI group versus non-CI group, Student’s t-tests were performed. Logistic regression analyses were performed to evaluate variables associated with CI. The following covariates were included in the model: (1) education ⩽6 years, (2) time from onset to diagnosis ⩽12 months, (3) time from onset to treatment ⩾60 months, (4) brain lesion on magnetic resonance imaging (MRI) before AZA or RTX, (5) EDSS ⩾4.0 during first appointment, (6) hospitalization by NMOSD, and (7) relapses by NMOSD ⩾4. Additionally, odds ratios (ORs) and 95% confidence intervals (95% CI) were computed.
Results
A total of 65 NMOSD patients were included in this study. Among the 65 patients diagnosed with NMOSD, 34 (52.3%) were in the CI group, and 31 (47.7%) in the non-CI group. Table 3 shows sociodemographic and disease characteristics by group. Compared to the non-CI group, the CI group exhibited less years of education (p = 0.019), longer intervals between onset of symptoms and diagnosis (p = 0.018), and longer intervals between onset of symptoms and initial treatment (p = 0.047). Additionally, the CI group had a higher proportion of patients with brain lesions (p = 0.019), higher EDSS ⩾4.0 during the first appointment with the neurologist (<0.001), higher hospitalization rates (0.001), and higher rates of relapse by NMOSD ⩾ 4 (p = 0.004).
Comparison of sociodemographic and disease characteristics in patients with cognitive impairment (CI group) versus patients without cognitive impairment (non-CI group).

CI group: patients with cognitive impairment; non-CI group: patients without cognitive impairment; NMOSD: neuromyelitis optica spectrum disorders; AQP-4: aquaporin 4; EDSS: Expanded Disability Status Scale; AZA: azathioprine; RTX: rituximab; MS: multiple sclerosis; MRI: magnetic resonance imaging.
Qualitative variables expressed in frequency and percentage compared by chi-square tests or Fisher’s exact tests.
Furthermore, a univariate logistic regression was performed. Variables associated with CI were education (⩽6 years of schooling; OR 4.37, 95% CI 1.41–13.52, p = 0.010), disease duration (⩾60 months; OR 8.22, 95% CI 2.68–25.20, p < 0.001), time from onset to diagnosis (⩾12 months; OR 3.70, 95% CI 1.21–11.31, p = 0.022), brain lesion (on MRI before AZA or RTX; OR 3.46, 95% CI 1.20–10.00, p = 0.022), and relapses by NMOSD diagnosis (⩾4; OR 4.48, 95% CI 1.57–12.76, p = 0.005). We adjusted time from onset to diagnosis (⩾12 months), time from onset to treatment (⩾60 months), and brain lesion (on MRI before AZA or RTX) in multivariable logistic analyses. Factors associated with CI were education (⩽6 years; OR 5.92, 95% CI 1.57–22.23, p = 0.008), disease duration (⩾60 months; OR 5.73, 95% CI 1.69–19.40, p = 0.005), and relapses by NMOSD diagnosis (⩾4; OR 5.79, 95% CI 1.70–19.72, p = 0.005) (Table 4).
Factors related to cognitive impairment in the crude and multivariate model.

OR: odds ratio; 95% CI: 95% confidence interval; NIM: not in the model; MRI: magnetic resonance imaging; AZA: azathioprine; RTX: rituximab; NMOSD: neuromyelitis optica spectrum disorders.
Adjusted analysis was obtained using the forward stepwise methods.
Discussion
The purpose of the current study was to evaluate the factors associated with CI in patients with NMOSD. Key findings revealed (i) the neuropsychological profile of NMOSD patients and (ii) the factors associated with cognitive impairment after adjusting for confounders such as education (⩽6 years), disease duration (⩾60 months), and relapses by NMOSD (⩾4).
Results from this study indicated poor cognitive performance in NMOSD patients compared to HCs. These results are consistent with those described in the literature.40–43 Additionally, in an observational study, Salama and colleagues 23 reported that cognitive performance was significantly worse in NMOSD patients compared to HCs for verbal memory, processing speed and visuospatial memory. In this context, we previously reported that 70% of NMOSD patients had CI in two or more cognitive domains. 24
In our NMOSD patients, we identified that the CI group had a higher proportion of patients with a lower educational level (76.5%). In a review study, Czarnecka et al. reported that the level of education can influence the cognitive performance in NMOSD patients. 6 Furthermore, we found that lower educational levels had a 5.92-fold risk of CI in NMOSD patients. This risk factor has been consistently reported in previous studies of NMOSD patients.7,43,44
Several studies have shown that a lower educational level is a predictor of poor performance on cognitive assessment in patients with demyelinating diseases. A study conducted by Estrada-López et al. evaluated 65 patients with multiple sclerosis. Participants were divided into three groups based on educational level: primary education (6 to 8 years of formal schooling), secondary education (8 to 12 years), and higher education (⩾15 years). Their results showed that patients with only primary education obtained significantly lower scores in verbal fluency compared to those with higher education. 45 These findings are consistent with the work by Kong et al., who evaluated 66 patients with NMOSD and 22 HCs using a neuropsychological assessment. Their results showed that NMOSD patients with worse cognitive function had lower educational levels (primary schooling). 46
A study conducted by Kim et al. found that a lower educational level was associated with poor cognitive performance in patients with NMOSD. 19 Additionally, an observational retrospective study conducted by Vlahovic et al. evaluated demographic and clinical characteristics associated with cognitive function in NMOSD patients. Their findings showed that educational level, race, and neurological disability significantly correlated with cognitive dysfunction. 20
We identified that a disease duration of ⩾60 months had a 5.73-fold risk of CI in NMOSD patients. A retrospective study conducted in Portugal by Lopes et al. demonstrated that duration of disease and level of disability were associated with CI. 18 In Mexico, a study by Rivas et al. investigated the relationship between cognitive impairment and clinical variables in NMOSD patients. The study included 30 NMOSD patients and 30 HCs. Their findings showed no significant associations between cognitive dysfunction and disease duration, AQP-4, lesion burden, and depression. 47
Although previous studies have reported some factors associated with CI in NMOSD; to the best of our knowledge none have specifically examined the potential outcome of relapses by NMOSD (⩾4). Our study demonstrated that relapses are associated with CI in NMOSD patients and remained significant after controlling for potential confounders in the multivariable analysis.
About 52% of patients in the present study had CI, mostly in tests of processing speed information and verbal memory. These findings suggest that NMOSD patients require cognitive assessment and cognitive rehabilitation by expert neuropsychologists.
We consider it essential that the cognitive assessment instruments used in NMOSD patients be standardized and validated in the Mexican population. Appropriate normative data are critical and for guiding the design of cognitive rehabilitation programs for patients with cognitive impairment.48,49
The results from the current study need interpretation in the context of its limitations. First, patients were evaluated at a single point in the time. A longer follow-up period would provide information on cognitive function changes of patients with NMOSD. Second, some factors associated with CI in NMOSD patients can change depending on geographical location due to different sociodemographic characteristics. Third, patients came solely from a tertiary-care center. Patients in tertiary-care centers frequently require more immunosuppressant treatment and hospitalization compared with NMOSD patients in secondary-care centers. The characteristics of our sample can be generalized to patients being cared in tertiary-care centers. However, future studies should include NMOSD patients who have been cared for at secondary-care hospitals in Mexico.
Conclusion
This study observed that 52% of NMOSD patients exhibited CI. The factors associated with CI in our NMOSD patients included: education (⩽6 years), diseases duration (⩾60 months), and relapses by NMOSD (⩾4). This information is crucial for designing cognitive intervention programs aimed at assessing and recognizing cognitive deficits, as well as implementing cognitive rehabilitation strategies.
Footnotes
Acknowledgments
The authors acknowledge members of the research group investigating factors related to cognitive impairment in patients with neuromyelitis optica spectrum disorders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research was approved by the local Ethics and Research Committee of Centro Medico Nacional de Occidente at the Instituto Mexicano del Seguro Social (code of approval: R-2021-1301-023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.