
Abstract
Background
In Denmark, specialized multiple sclerosis (MS) clinics offer free-of-charge treatment to people with MS. However, not all people with MS attend regular clinical follow-up.
Objective
To identify people with MS who do not attend Danish MS clinics and identify barriers to treatment.
Methods
The Danish Multiple Sclerosis Registry was linked to other national Danish registries with follow-up from 2000–2020. We used a time-dependent Cox regression to rank factors associated with low attendance to clinical follow-up visits based on the magnitude of hazard ratios (HRs).
Results
We included 10,175 adults with MS, of which 3862 (38%) had less than one visit annually. The five top-ranked factors that reduced the risk of visits occurring included never having received diseases modifying treatment (HR: 0.48; 95%CI: 0.46–0.49), been diagnosed with MS before 2009 (0.79; 0.78–0.81), association with MS center in an outer region of Denmark (0.82; 0.80–0.84), having progressive MS type (0.88; 0.86–0.91) and not having received symptomatic treatment at diagnosis (0.91; 0.89–0.93).
Conclusion
Our results highlight disease-specific and geographic inequalities in the management of people with MS in Denmark. Strategies to prevent this inequality, especially for people with progressive phenotypes and those who need supportive and non-medical treatment and care, should be implemented.
Introduction
Every year approximately 600 people are diagnosed with multiple sclerosis (MS) in Denmark, and more than 18,000 people currently live with MS.1,2 There are large individual variations in consequences and impacts on experienced everyday life. But often it affects people’s physical mobility, self-care and quality of life.3–5 There is an increasing focus on the importance of tracking down physical and cognitive consequences in early stages of the disease to optimize the prevention of lost functional ability.5,6 Thirteen MS clinics and two MS hospitals offer free of charge highly specialized treatment and rehabilitation for people with MS in Denmark. 7 Clinical follow-up visits ensure monitoring for disease development, treatment measures, disease-modifying therapy (DMT), symptomatic treatment and referral to municipal support and rehabilitation. 5
Current guidelines recommend regular neurological MS care for people diagnosed with MS.5,8 Without regular clinical follow-up visits, it is difficult to monitor disease progression, which may lead to insufficient treatment and negative health outcomes. 6 People who do not attend specialized MS clinics have been observed to be older, accessed health services more frequently and have higher rates of comorbidity.6,9,10 Regular neurological visits for people with primary progressive MS (PPMS) and those who are not on DMT are observed to be lower compared to relapsing forms of the disease and could be associated with worse outcomes.6,7,11 However, clinical trials often use clinic-based participants, and research on people with MS that are not clinic based is limited, which may underestimate the true burden of MS. 9
Thus, we aimed to identify people with MS that do not attend regular clinical follow-up visits at Danish MS clinics and identify barriers to treatment. Special emphasis is given to socio-demographic factors such as education, marital status, geographical aspects and clinical factors such as MS phenotype, medication and disability levels, which may be associated with care access barriers.12–15 We hypothesized that people with progressive MS have a lower frequency of clinical visits at Danish MS clinics compared to those with relapsing MS type, which could perhaps be attributed to their anticipated reduced mobility and limited access to DMTs.
Materials and methods
Study design and population
This register-based cohort study identified participants through the Danish Multiple Sclerosis Registry (DMSR), which contains data on all Danish Citizens with MS disease onset since 1948 in Denmark. 16 All people with a confirmed MS diagnosis in Denmark were identified according to the time respective diagnostic criteria for MS and were followed during the period of 2000 until end of follow-up on 31 December 2020, or death.
Inclusion and exclusion criteria
All people with a confirmed MS diagnosis between 2000 and 2020 were included. People with no defined MS phenotype, age below 18 years at diagnosis, no date of diagnosis, no association with an MS clinic, emigration after diagnosis or disease duration of less than two years were excluded from the study.
Outcome
The primary outcome was visits to MS clinics in Denmark. All types of visits that occurred during the follow-up period, regardless of their purpose, were considered as relevant outcome events and included in the analysis. We examined the occurrence of visits from diagnosis (baseline) until end of the follow-up.
Variables
We calculated the mean number of visits per year from the date of diagnosis until end of follow-up and categorized people with MS into people with less than one clinic visit a year, or one or more clinic visits a year, to describe the study population according to annual number of visits. We examined various socio-demographic factors such as sex, age at diagnosis and geographic area of MS clinic. Marital status, education level, employment status, income, regional and municipal area of residence and healthcare utilization were included at the time of diagnosis defining phenotype. Clinical characteristics, including phenotype, most recent Expanded Disability Scale Score (EDSS) and Functional System (FS) score recorded by a neurologist, symptomatic treatment at diagnosis and the use of DMT throughout the follow-up period, were also examined (Supplemental Table 1, Supplemental Table 2).
Data collection
Data obtained from DMSR were linked to national registries by the unique personal identity number (Civil Registration Number, CPR) 17 at Statistics Denmark 18 to obtain information on the study population's geographical and socio-demographic factors.
Data sources
The DMSR contains data on all Danish Citizens with MS onset since 1948 who have received an MS diagnosis from a neurologist or a Department of Neurology in Denmark. 16 This registry receives a quarterly list of all patients assigned to each MS clinic in Denmark. The data collection software has an integrated data verification tool to identify missing or incoherent data and ensure high-quality recording, which in turn ensures the scientific validity of the registered data. 16
Statistics Denmark is the central authority in Danish statistics and has collected a large amount of historical register data in a basic databank that is updated at least once a year. The Danish system of unique person identifiers was used to link individuals across registers in an anonymized dataset in Statistics Denmark, which was then accessed through a virtual private network connection from Zealand University Hospital. 18
Information on sex, age, diagnosis, clinic use, area of MS clinic, disability level and use of DMT was obtained from DMSR. Information on health care utilization (general practitioner [GP], doctor on call, clinical psychologist, physiotherapy), time of death and symptomatic treatment was obtained from Danish National Health Data Authority that is responsible for the national health registers 19 (The Danish National Patient Registry, Healthcare Insurance Registry, Cause of Death Registry and Registry of Pharmaceutical Sales). Information on marital status, education, employment, income and residence was obtained from Statistics Denmark (National Income Registry, Education registry and the Employment Classification Module).
Statistical analyses
Data were analyzed using STATA version 18.0. We used descriptive statistics to test for the association between variables in a bivariate analysis using Pearson's χ2 test, Wilcoxon rank-sum (Mann–Whitney) test and Student's t-test as appropriate, to describe the study population according to annual number of visits.
Several variables exhibited missing values, with different patterns and frequencies across the dataset. To handle missing values, a combination of approaches was employed based on the characteristics of each variable. Variables that demonstrated percentage of missingness >20% were excluded from the analysis. Expanded Disability Scale Score had a missing percentage of 10.56% when used as a time-varying covariate (TVC), and Last Observation Carried Forward (LOCF) approach was selected due to the assumption that missing values were likely due to unchanged levels of diseases since last visit. Patients with no recorded EDSS score, primarily due to having 0 visits, were excluded from the analysis. We employed selected deletion to variables presenting small percentage of missing values ranging from 0.41% to 1.66%. Given the large size of the dataset, it was determined that imputing these values could introduce bias into the analysis without significantly changing the results (Supplemental Table 3). In total, 9415 subjects were included for the regression analysis with 124,175 observations.
We performed a time-dependent Cox regression, the Andersen-Gill model, to rank factors associated with low attendance at clinical follow-up. We estimated adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) for the time to visit, with statistical significance set at p < 0.05. Nelson-Aalen cumulative adjusted hazard estimates were used to visually assess the cumulative risk of visits over time for the MS types. We included n = 14 factors in the model and backward selection was terminated at the stopping rule by a threshold of fixed value p < 0.05. To verify the proportional hazards (PH) assumptions of the final Cox model, we employed the Grambsch–Therneau test which indicated that several factors violated the PH assumption. To address this, we adjusted the final model for the factors that interacted with time by incorporating a TVC function within the model. Due to changes over time, we split the follow-up period into intervals to examine time-dependent changes and conducted the Cox model for each interval. As several factors interacted with time, it became challenging to accommodate the specific time of change in all factors simultaneously in a model. Therefore, period intervals were split based on the interquartile range: 0–3 years, 4–9 years and >9 years. Proportional hazard assumptions were tested for each model and found to be violated for some variables. Because further adjustments could yield overly fragmented or complex models, we opted to proceed with existing models; therefore, the results should be interpreted with caution.
To assess the robustness of the results, we conducted a sensitivity analysis using complete case analysis and multiple imputation by chained equations (MICE) with 10 imputations. We compared the imputation methods to assess the effect of each method on the results, and complete case analysis was compared with the imputation methods to evaluate whether the imputation process affected the findings. Additional data regarding technical details, statistical codes and derivative data were available from the principal investigator. Data access for further analyses is possible through direct collaborative agreements or locally managed access arranged through the study's principal investigator.
Ethical statement
This study was reported as anonymized register-based investigation to the National Committee on Health Research Ethics (SJ-971 (anm.nr. 88070) EMN-2022–00118). According to the Danish law, no formal approval or informed consent was needed. 20 The study was reported to and approved by the institutional review board at Zealand University Hospital (Data and Development support, Research inventory, REG-160–2021) and was conducted according to the Declaration of Helsinki 21 and General Data Protection Regulation. 20
Results
The initial study population comprised 13,612 participants, of which a total of 10,175 participants were included in the analysis (Figure 1). The study population includes in total 6915 (68%) females. Median age was 39 (IQR: 31–47) years, and median follow-up time was 10.2 (IQR 5.91–14.9) years.

Flowchart for selection of individuals with multiple sclerosis from the Danish Multiple Sclerosis Registry.
Visits to MS clinics
Among the participants in the study population 3862 (38%) were observed to have <1 annual visit to an MS clinic during the study period and were assessed to have low attendance at clinical follow-up visits.
People with low attendance versus control subjects were more likely to be older at the time of diagnosis, diagnosed between year 2000 and 2009, married, and had, in general, a lower level of education. Moreover, people with low attendance vs. controls were more often on disability pension or retired, had a lower income, resided in rural and upland municipalities, less likely to attend a clinical psychologist and were more often connected to MS clinics in the North or Zealand regions (Table 1).
Sociodemographic characteristics of individuals with multiple sclerosis according to attendance at MS clinics.
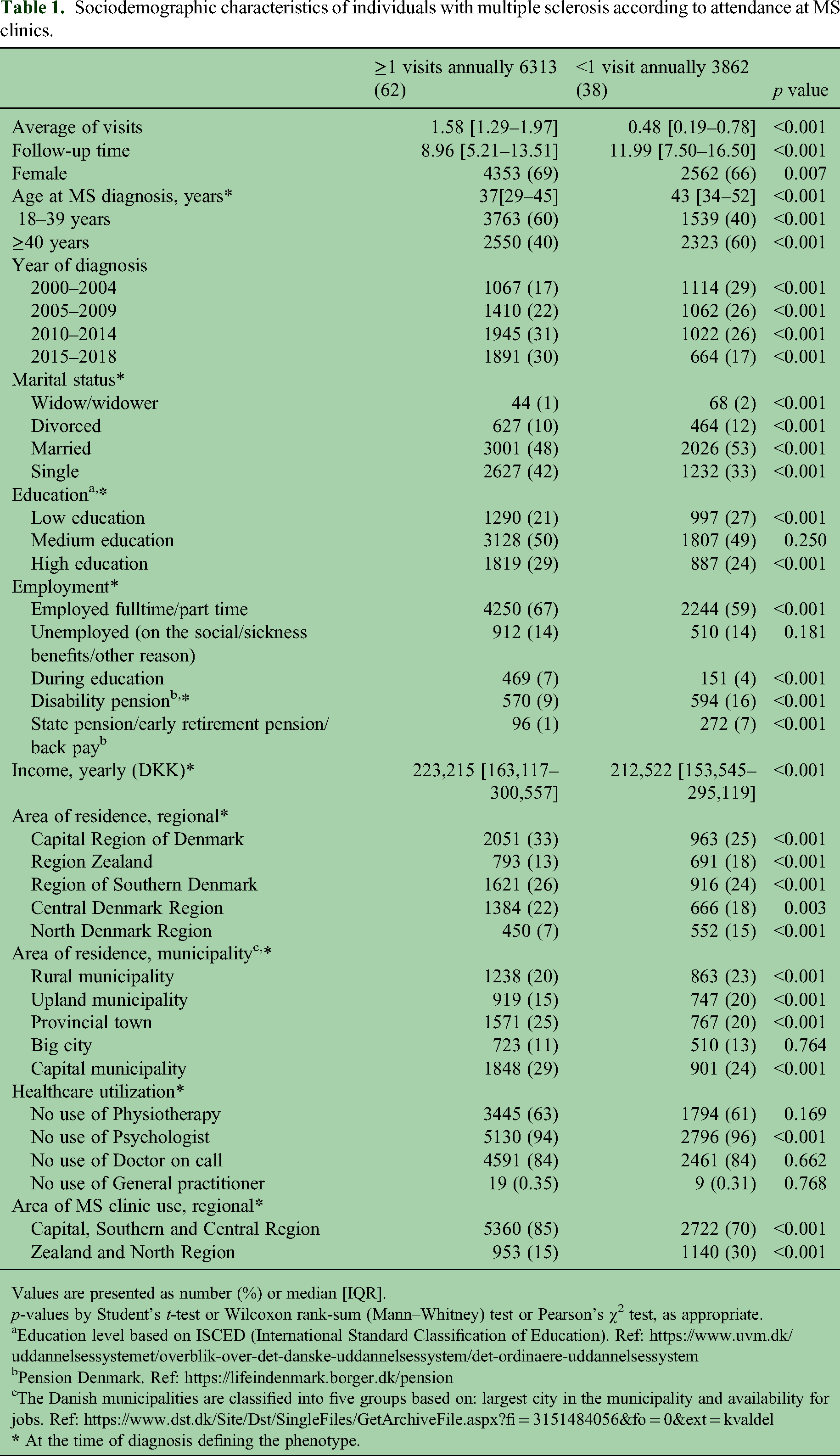
Values are presented as number (%) or median [IQR].
p-values by Student's t-test or Wilcoxon rank-sum (Mann–Whitney) test or Pearson's χ2 test, as appropriate.
Education level based on ISCED (International Standard Classification of Education). Ref: https://www.uvm.dk/uddannelsessystemet/overblik-over-det-danske-uddannelsessystem/det-ordinaere-uddannelsessystem
Pension Denmark. Ref: https://lifeindenmark.borger.dk/pension
The Danish municipalities are classified into five groups based on: largest city in the municipality and availability for jobs. Ref: https://www.dst.dk/Site/Dst/SingleFiles/GetArchiveFile.aspx?fi = 3151484056&fo = 0&ext = kvaldel
Based on clinical characteristics, people with low-attendance vs. controls were more likely to have PPMS and were observed to live with higher level of disability based on the most recent EDSS score of ≥4.5 recorded by a neurologist (Table 2). We also examined FS scores separately to observe specific functions that affected their disability levels. People with low-attendance vs controls were more likely to have mild, moderate or marked paraparesis or hemiparesis; mild, moderate or severe ataxia, severe nystagmus or inability to swallow or speak; moderate or marked decrease in touch or pain, mild, moderate or frequent urinary hesitancy, urgency or retention; a marked decrease in mentation; and a decreased ability to walk without the need for assistance (Table 2). When examining medication use, we observed that people with low-attendance compared to those with higher attendance more likely never received DMT (Table 2).
Clinical characteristics of individuals with multiple sclerosis according to attendance at MS clinics.
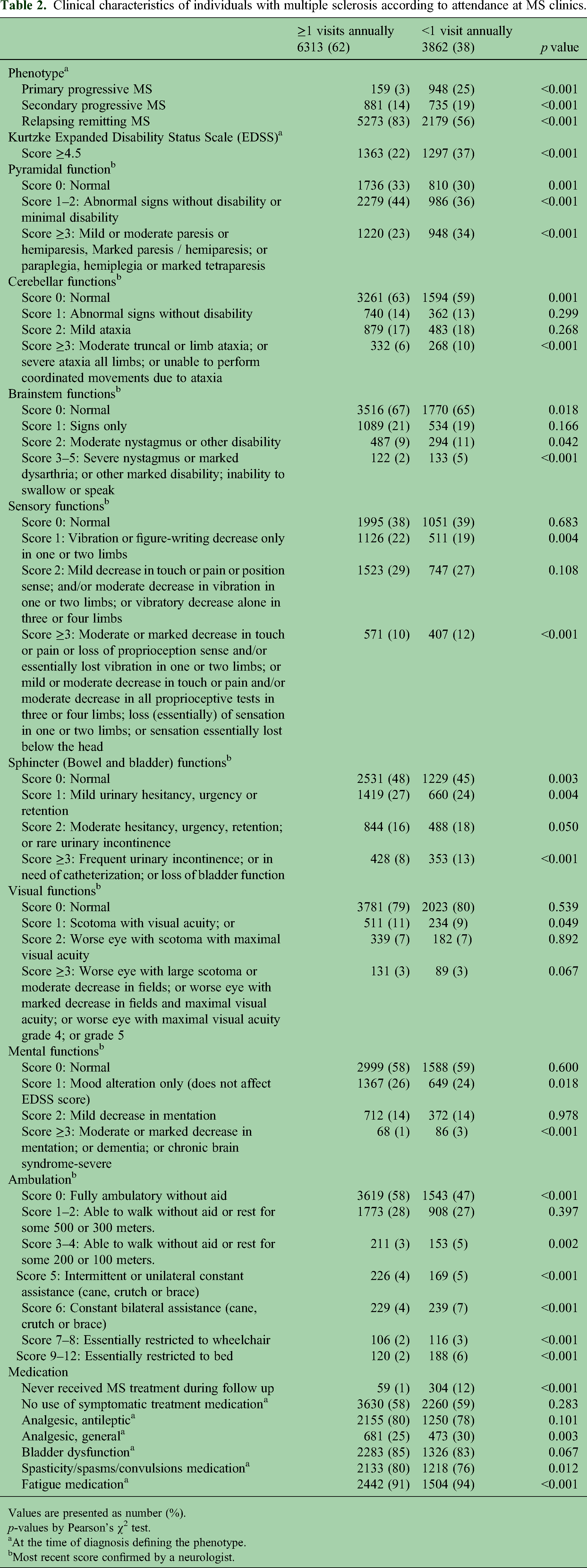
Values are presented as number (%).
p-values by Pearson's χ2 test.
At the time of diagnosis defining the phenotype.
Most recent score confirmed by a neurologist.
Andersen-Gill Cox regression model
Patients not receiving treatment had a significantly lower risk of recurrent visits compared to those receiving treatment, with an HR of 0.48 (95% CI: 0.46–0.49) (Table 3). However, the effect diminished over time, HR 0.75 (0.74–0.76), with the risk of recurrent visits remaining lower. Patients diagnosed between 2000 and 2009 had a lower risk of recurrent visits compared to other time periods with an HR of 0.79 (0.78–0.81). The TVC HR 1.11 (1.10–1.13) suggested that this association changed over time. For patients in centers in outer regions, there was a lower risk of recurrent visits compared to those in other regions with an HR of 0.82 (0.80–0.84). This association diminished over time with HR of 0.96 (0.95–0.97), with the risk of recurrent visits remaining lower. For patients with progressive MS, there was a lower risk of recurrent visits compared to those with relapsing MS types with HR of 0.88 (0.86–0.91). This risk increased over time with TVC HR of 1.09 (1.08–1.11). Patients who did not receive symptomatic treatment at diagnosis had a reduced risk of recurrent visits with an HR of 0.91 (0.89–0.93). However, the TVC HR of 1.02 (1.01–1.03) suggested a changed risk over time. Each unit increase in EDSS was associated with a slight reduction in the risk of recurrent visits with HR of 0.99 (0.98–0.99). However, this association reversed over time, with a TVC HR at 1.02 (1.01–1.02). Income was not significantly associated with the risk of recurrent visits: HR 0.99 (0.98–1.01, p = 0.280). Age at diagnosis showed a minimal decrease in risk of visits with each unit increase with an HR of 0.99 (0.99–1.00), with marginal change over time: HR 1.00 (1.00–1.00). Certain factors showed a slight increase in risk for recurrent visits, including patients from rural and upland areas HR 1.02 (1.01–1.03), married patients HR 1.02 (1.01–1.04) and female patients HR 1.02 (1.01–1.04) (Table 3, Figure 2).

Ranking of factors associated with low-attendance to clinical follow-up in patients with multiple sclerosis overall (upper panel), and according to disease phenotype (lower panel). Factors associated with low-attendance in multiple sclerosis were identified from stepwise backward exclusion process of multiple logistic regression modelling. HR = hazard ratio. CI = confidence interval
Ranking of factors associated with low attendance in MS clinics.

Factors were identified from stepwise backward exclusion process of time-dependent Cox model and stratified by center and adjusted for factors that interacted with time.
Time-varying covariates (TVC) interacted with ln(_t).
By splitting the follow-up into distinct periods, we could estimate HRs specific to each time frame. The captured time-varying effect of how risk factors diminish or increase the risk within each specific time frame is shown in Table 4.
Adjusted HRs across different time periods.
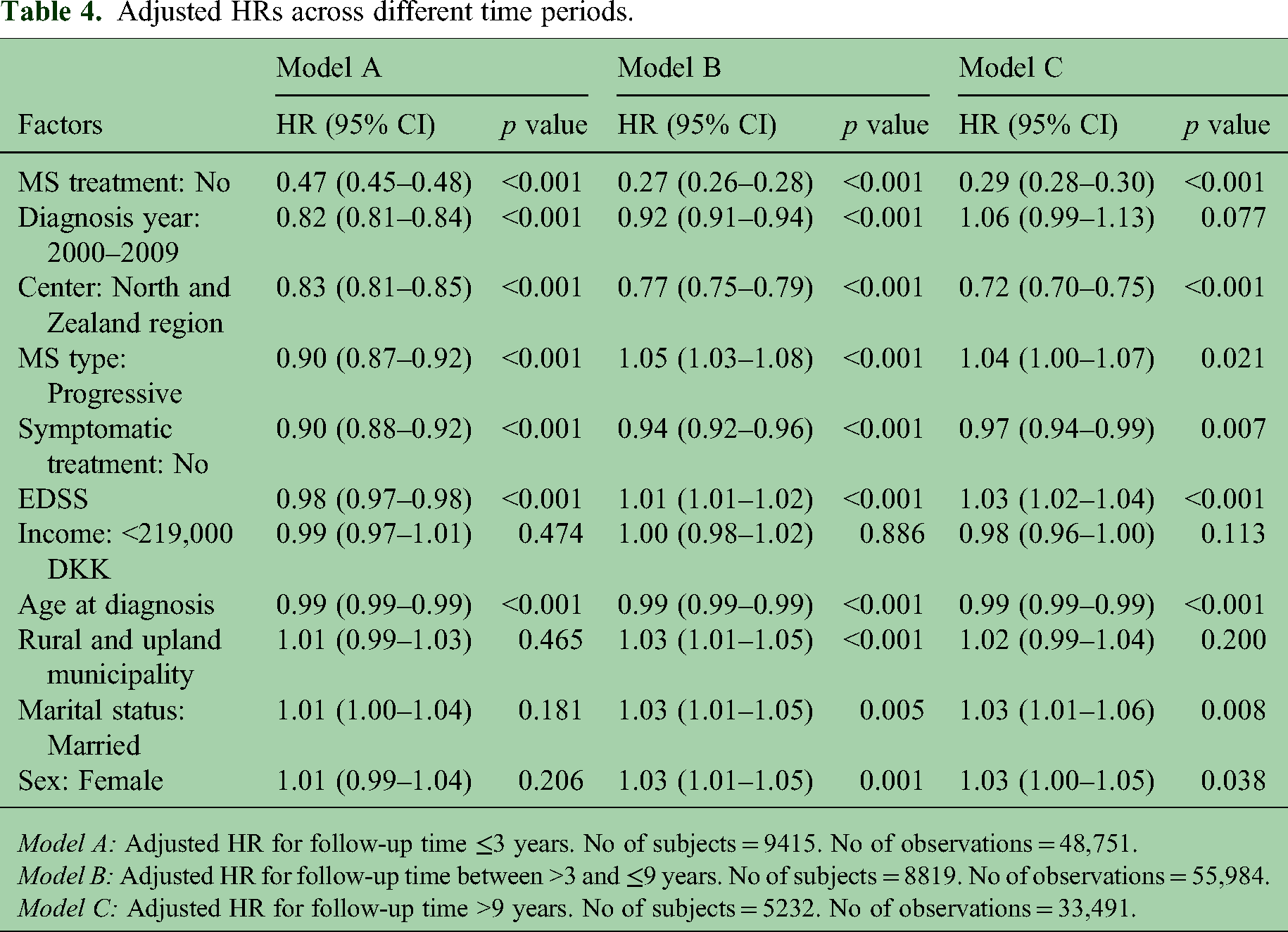
Model A: Adjusted HR for follow-up time ≤3 years. No of subjects = 9415. No of observations = 48,751.
Model B: Adjusted HR for follow-up time between >3 and ≤9 years. No of subjects = 8819. No of observations = 55,984.
Model C: Adjusted HR for follow-up time >9 years. No of subjects = 5232. No of observations = 33,491.
When ranking the factors associated with low-attendance to clinical follow-up according to MS phenotype, we observed differences between variables, but the same main factors remained associated with low-attendance (Figure 2). Cumulative risk of visits over time according to MS phenotype showed a consistently higher risk of visits occurring for people with Relapsing type compared to Progressive type (Figure 3).
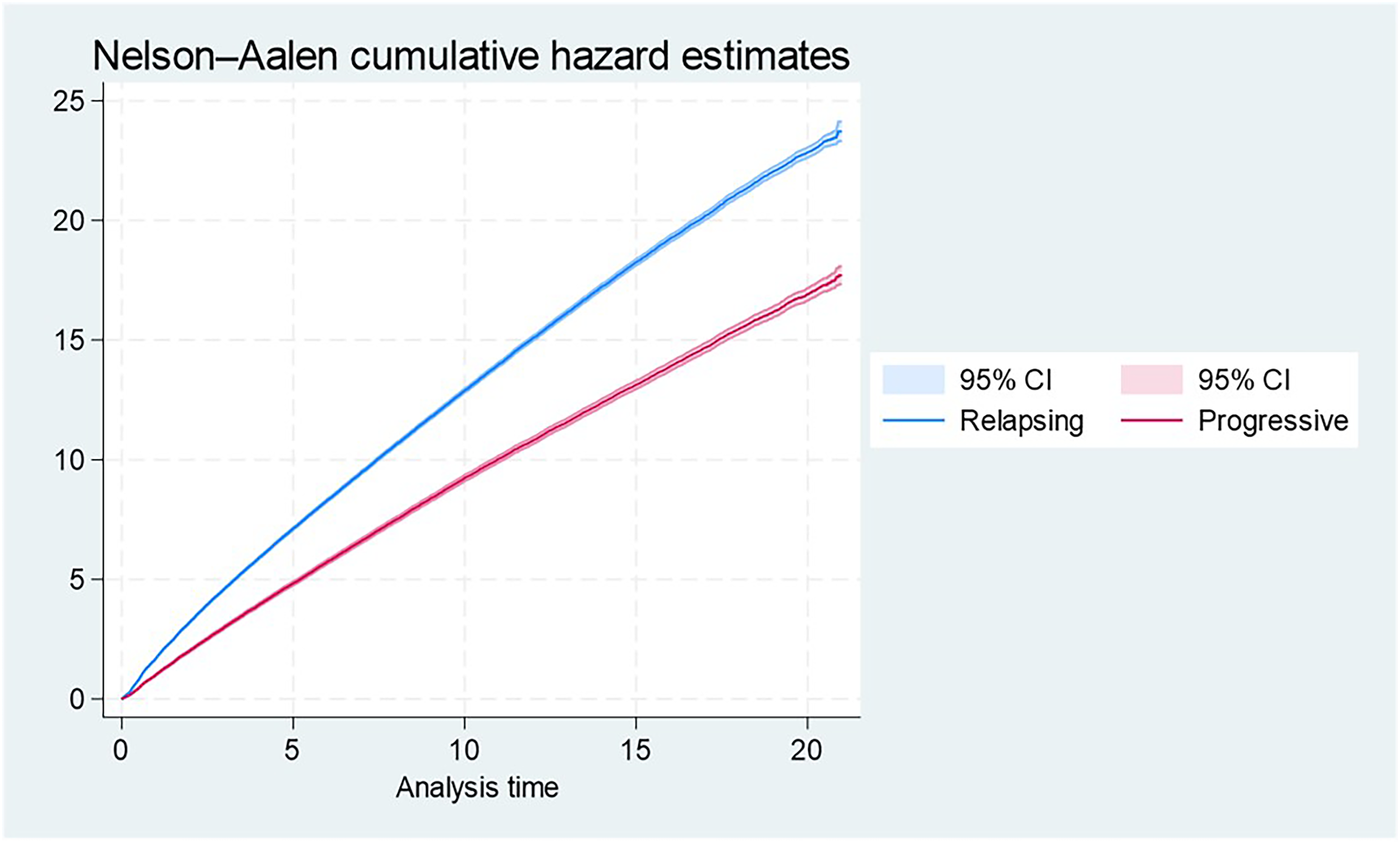
Cumulative risk of visits over time according to MS phenotype by the Nelson-Aalen analysis.
We ranked factors associated with low attendance using data where missing values were handled by selected deletion and LOCF method. A comparison of results from the LOCF and MICE methods showed the findings remained consistent (Supplemental Table 4). This suggests that the results do not change significantly with respect to the multiple imputations method used. Similarly, comparing results from the complete case analysis with those from LOCF and MICE methods revealed no significant changes, indicating that the imputation process did not substantially affect the results.
Discussion
Based on the magnitude of the HRs, we ranked the factors associated with low-attendance. The five top-ranked factors that reduced the risk of visits occurring included not receiving DMT, been diagnosed with MS before 2009, association with MS center in an outer region of Denmark, having progressive MS type and not having received symptomatic treatment at diagnosis. For people diagnosed before 2009 and progressive type, the risk of recurrent visits increased with time.
For people with progressive MS, symptomatic therapies are an essential component of care. They heavily rely on non-medical support and symptomatic treatment, and the importance of supportive care increases with increasing disability level, as they have greater challenges in performing daily activities and managing their health. 22 Regular visits to a neurologist for people with progressive MS has been observed to be lower compared to RRMS. This discrepancy could be attributed to the limited availability of DMT's for PPMS. 23 Moreover, people living with MS often feel the amount of effort and energy required to access healthcare services is not justified by the potential benefits or outcomes of seeking care. 24 National neurological treatment guidelines for MS suggest medication for symptoms as fatigue, bladder dysfunction, spasticity and gait disorders. 25 Only treatment with Fampridine requires annual follow-up. Other symptom monitoring is individual based and can be done in other specialties, including general practice. 25 However, guidelines for training, physiotherapy, specialized rehabilitation and psychological support are lacking.
We observed being diagnosed before 2009 reduced the risk of visits. A recommendations report on cross-sectoral care pathways for people with MS in 2021 showed that patients aged 65 or older had an increase in outpatient visits of 58.2% during the period from 2014–2018, and this increase encompassed various types of outpatient visits, including medical consultations, treatments and medication dispensing. 5 About 45% of the MS population had at least one contact with a neurological department per year from 2014–2018. 5 This is consistent with our results that showed an increase in visits occurring after 2009.
Being followed in clinics located in North and Zealand regions was also observed to be associated with a decrease in visits in clinical follow-up, even after adjusting for the residence of the participants. Denmark is divided into five regions responsible for the healthcare system, and the geographical and economic sizes differ significantly among those regions. 8 North and Zealand region have relatively low population numbers compared to other regions, making them the smallest in terms of population size. However, geographically area covered by North and Zealand is extensive with many remote areas, which can present challenges in terms of accessibility to essential health care services. Previous studies have identified geographic factors, such as living in rural areas, appear to limit access to neurologists.15,26,27 People with longer distances to specialized MS clinics may face challenges in navigating in traffic, geography and administration, which can be especially challenging for those with disabilities requiring wheelchair and people of older age.15,26,27 Moreover, MS clinics are the only units authorized to prescribe DMTs and predominantly provide outpatient care for people with MS. 8 Danish Medicines Council has described the monitoring of pathways with the use of DMT in structured treatment guidelines that clinics must follow. 25 Lack of structured recommendations and guidelines for symptomatic treatment can contribute to the under-prioritization of symptomatic treatment, as initiating rapid treatment with DMT is important to prevent relapses and disease progression.8,25
We identified increasing age at time of diagnosis and never receiving DMT was associated with a decrease in visits occurring to clinical follow-up. Few studies have compared people with MS that attend MS clinics compared to those that do not, and similar to our results they identified older age at diagnosis and low use of DMT among those with low-attendance, compared to those with higher attendance.28–30 Low attendance among older people to specialized treatment could be due to various factors. These may include differences in perception of health compared to younger people, difficulties related to accessibility (especially for those with disabilities or residence in remote areas) and people’s beliefs and attitudes towards healthcare.15,24,31,32
However, looking at our overall results, the high frequency of progressive types among the low-attendance group could perhaps in part explain some of the other factors associated with low-attendance. Previous studies have shown that people with progressive MS are older at diagnosis, more affected by their MS with higher disability levels, lower education levels and lower income.23,33 Moreover, people with progressive MS have not been able to receive DMT for many years, and there is still a lack of availability. We observed higher levels of disability in the low-attendance group. People with neurological disabilities and complex needs are known to be more vulnerable to suboptimal healthcare, and there are issues regarding accessibility, fragmentation of health services and inadequate preventative care. 34 Healthcare is often managed by GPs, however, in our results, we did not observe significant differences in use of GPs in the low-attendance group compared to those with higher attendance.
During the COVID-19 pandemic, clinical video telemedicine (CVT) became widely adopted. 35 While CVT can be inadequate for evaluating MS-related neurological symptoms, 35 it proves beneficial for counselling on treatments, managing side effects and monitoring patient well-being remotely.36,37 It also aids in assessing neurocognitive status and psychological symptoms, potentially guiding the necessity for in-person visits.36,37 Barriers such as older age and visual impairments affect usability, highlighting the need for improvements to ensure equitable access.36,38
This study had some limitations. Data in Danish administrative registers were collected systematically without the purpose of being used for specific research. 35 Therefore, the selection of variables that can be included in the study is dependent on the availability of data in the source registers, making some variables of interest, for example, lifestyle related information, absent in this study. We combined panel and cross-sectional data and included selected socio-demographic variables at a certain point in time. We did not take into account certain factors that could be associated with attendance in specialized MS clinics, such as the number of magnetic resonance imaging (MRI) sessions, the type of treatment received and the frequency of relapses. These variables have the potential to contribute to the frequency of visits for patients in MS clinics.
The data are limited to people who had been diagnosed with or treated for MS in Denmark, where access to specialized treatment is free of charge. It cannot be precluded that the study underestimates the frequency and proportion of low attendance in countries where people have to pay for treatment. However, we feel confident that these results can be useful in countries with similar healthcare systems as Denmark.
Most patients had one outpatient trajectory, and one MS clinic was responsible for the treatment. Our study did not differentiate between the type of consultation and type of specialist, whether the MS specialist was a nurse or doctor. Our categorization into less than one MS clinic visit is a pragmatic solution to describe attendance and utilization of MS clinics. This approach resembles the categorization applied in previous studies,28–30 and the recommendation on regular follow-up for people diagnosed with MS in Denmark. 8
We handled missing values using selected deletion and LOCF which resulted in a slight reduction in the number of subjects but allowed us to retain more observations per subject. This approach enhances the accuracy of modelling within-subject changes over time and time-varying effects, contributing to the reliability of estimates. While having fewer subjects may reduce the ability to detect between-subjects effects and differences, the remaining number of subjects is assessed to be sufficient, and having a sufficient number of observations per subject was prioritized to ensure more stable estimates. Furthermore, a limitation of this study is the non-proportionality for certain variables. We addressed this by incorporating TVC and analyzing separate time intervals, but results should still be interpreted with caution.
A key strength of this study is the robustness of findings across different methods for handling missing data, that showed consistent results. Additional strength is the large representative size of study population and use of data from nationwide Danish registers, including the nationwide complete Danish MS registry that followed the Danish MS population for more than 70 years, which allow us to link variables on geographic, socio-demographic and clinical factors through individual identification number. The data have high validity and completeness because they are continuously collected, and the provided clinical care is quality-controlled and recorded by specialized healthcare professionals in diverse medical fields. 16
Conclusion
Barriers identified to follow-up visits at Danish MS clinics included never having received DMT, been diagnosed before 2009, association to MS center in an outer region, having progressive MS type and not having received symptomatic treatment at diagnosis. Our results provide information to improve strategies aimed at reducing inequality in access to specialized treatment, especially for people with progressive MS, and those requiring supportive and non-medical care. While research on this subject is limited, one can hypothesize that attending fewer follow-up visits in specialized MS clinics, may contribute to a lack of referral to effective therapies and symptom management, potentially resulting in poorer outcomes. Early treatment and new medications for progressive MS are becoming available, making it essential to promote visits to MS specialists, to ensure patients are not deprived of novel treatment options as they become available. Our results present associations rather than establishing causal relationships. In order to gain a deeper understanding of this issue and acquire a more profound comprehension, we initiated a qualitative study to explore the experiences of individuals with less than one annual clinical follow-up. Our aim is to explore factors contributing to the low follow-up rate and gain insight into their self-care and everyday lives.
Supplemental Material
sj-docx-1-mso-10.1177_20552173241307619 - Supplemental material for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study
Supplemental material, sj-docx-1-mso-10.1177_20552173241307619 for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study by Agata Beczek, Eskild Morten Landt, Lars Kristian Storr, Malene Beck, Luigi Pontieri, Melinda Magyari and Morten Dahl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-2-mso-10.1177_20552173241307619 - Supplemental material for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study
Supplemental material, sj-docx-2-mso-10.1177_20552173241307619 for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study by Agata Beczek, Eskild Morten Landt, Lars Kristian Storr, Malene Beck, Luigi Pontieri, Melinda Magyari and Morten Dahl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-3-mso-10.1177_20552173241307619 - Supplemental material for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study
Supplemental material, sj-docx-3-mso-10.1177_20552173241307619 for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study by Agata Beczek, Eskild Morten Landt, Lars Kristian Storr, Malene Beck, Luigi Pontieri, Melinda Magyari and Morten Dahl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-4-mso-10.1177_20552173241307619 - Supplemental material for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study
Supplemental material, sj-docx-4-mso-10.1177_20552173241307619 for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study by Agata Beczek, Eskild Morten Landt, Lars Kristian Storr, Malene Beck, Luigi Pontieri, Melinda Magyari and Morten Dahl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-5-mso-10.1177_20552173241307619 - Supplemental material for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study
Supplemental material, sj-docx-5-mso-10.1177_20552173241307619 for Barriers to clinical follow-up visits in multiple sclerosis: A nationwide register-based study by Agata Beczek, Eskild Morten Landt, Lars Kristian Storr, Malene Beck, Luigi Pontieri, Melinda Magyari and Morten Dahl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors thank participants and staff of the Danish Multiple Sclerosis Register for their important contribution.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Ministry of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.