
Abstract
Background
Although healthcare practitioners (HCPs) are a valuable source of social support, research on support provided by neurologists to older persons with multiple sclerosis (pwMS) remains limited.
Objectives
To explore expectations of pwMS aged 55 years or older regarding MS care and to identify support types, met and unmet needs within their relationship with neurologists.
Methods
Utilizing a mixed-methods approach, we analyzed survey data from Swiss Multiple Sclerosis Registry participants. Quantitative data included Likert scales gauging the importance of various aspects of MS care for pwMS both in and out of neurological care. Qualitative data were derived from three open-ended questions, focusing on neurologist-provided support for pwMS in neurological care. Data underwent descriptive and deductive thematic analysis, using Cutrona and Suhr framework for coding social support.
Results
Among the 286 participants (median age 61.0 years, interquartile range (IQR) 57.0–66.0; median disease duration 23.5 years, IQR 15.0–31.0), 84.6% (N = 244) were under neurological care. Quantitative findings highlighted the significance of HCP expertise and consultation time. Qualitative analysis identified all social support domains in the neurologist–pwMS relationship, with informational support being most prevalent, followed by emotional support. Neurologists’ expertise, availability, comprehensive advising, listening, and validation emerged as key themes. Unmet needs were relatively infrequent and concerned insufficient information on complementary medicine, empathy, and understanding of symptoms like fatigue.
Conclusions
Older pwMS see neurologists as adequate providers of comprehensive support and particularly value neurologists’ sufficient availability, informational and emotional support. Areas for improvement include attention to complementary medicine and empathy.
Introduction
Healthcare professionals (HCPs) have the potential to contribute to individuals’ well-being by providing emotional, informational and tangible support. 1 These support types fall under the umbrella term of social support, which encompasses perceived support, i.e. the perception of the availability of support and the actual supportive behaviors in interpersonal relationships.2,3
Social support has been recognized as a critical factor contributing to the improved health-related quality of life of older persons with multiple sclerosis (pwMS), with potential to offset deficiencies in other aspects associated with healthy ageing. 4 Research consistently underscores the significance of both emotional and informational support from HCPs for many pwMS, including those in geriatric and palliative care, who may have unique concerns and needs.5–8 Older pwMS attach great importance to the emotional support provided by HCPs, demonstrating a willingness to actively seek out HCPs who can offer emotional support alongside medical assistance and informational support. 9 Furthermore, older pwMS value two-way communication and collaborative relationship with HCPs, perceiving ineffective listening by HCPs as unhelpful. 10
Among all HCPs in MS care, neurologists retain a pivotal role, guiding treatment decisions and serving as a primary source of information for pwMS. 11 While support provision is identified as one of the core roles of neurologists by pwMS, 12 understanding of the support within the neurologist–patient relationship in MS care is limited and predominantly derived from studies that investigated social support from all sources or all HCPs involved in MS care, rather than the support specifically provided by neurologists.
To address the lack of research on neurologist-provided support for older pwMS, we conducted an exploratory mixed methods study within the Swiss Multiple Sclerosis Registry (SMSR). First, we aimed to quantitatively explore expectations of older pwMS regarding care and services provided by MS clinics and HCPs to assess general interest in support provision. Next, we aimed to qualitatively explore perceived social support provided by neurologists to pwMS in neurological care by identifying types of support as well as met and unmet support needs within the neurologist–pwMS relationship, using the social support coding framework by Cutrona and Suhr. 13
Methods
A mixed-methods approach was employed to descriptively analyze data derived from multiple-choice and open-ended survey responses.
Study population and data source
We used data from participants enrolled in the SMSR, an ongoing observational study in adults with MS residing or receiving treatment in Switzerland. The SMSR employs the citizen science approach to determine focus topics and develop questionnaires for the collection of self-reported data. Participation in the registry is voluntary and requires the completion of a consent form along with confirmation of MS diagnosis. The SMSR was approved by the Ethics Committee of the Canton of Zurich (PB-2016–00894; BASEC-NR 2019-01027). Additional information about the SMSR can be found elsewhere.14,15
Both quantitative and qualitative data utilized in this study primarily originate from the SMSR follow-up questionnaire released in November 2021. In addition to the questions on the disease status, medication usage and other MS and health-related questions typically included in the SMSR follow-up questionnaires, this questionnaire also included questions about participants’ expectations and the significance they assigned to services provided by MS practices and HCPs, along with open-ended questions on perceived support provided by neurologists. These questions were informed based on insights from a July 2021 focus group workshop involving five SMSR participants, aimed at exploring the importance of various dimensions of MS care to pwMS. The invitation to complete the follow-up questionnaire was sent to all active participants. However, this study only included participants aged 55 years or older at the time of questionnaire completion who responded to at least one question of interest for this study. Quantitative analysis included all participants meeting the specified criteria, whereas qualitative analysis involved only those currently undergoing neurological treatment. Additionally, we utilized sociodemographic data from the baseline SMSR questionnaire.
Quantitative data collection and analysis
Quantitative data concerned participants’ sociodemographic, MS-related, and health-related characteristics. Information on age, sex (female or male), Swiss citizenship (yes or no), highest education level (university degree, higher professional education, mandatory, high school, and apprenticeship), marital status (married and in a registered partnership or not), and gait disability (categorical, mild, moderate, or severe) as measured by Self-reported Disability Status Scale, 16 was collected in the SMSR baseline questionnaire. The duration of MS in years was calculated based on the year of diagnosis collected at baseline, up until the completion date of the follow-up questionnaire used in this study. The SMSR follow-up questionnaire included self-reported MS type, previously shown to have satisfactory validity and reliability 17 (relapsing-remitting MS (RRMS), primary progressive MS, secondary progressive MS (SPMS), clinically isolated syndrome, and transition between RRMS and SPMS), and a question regarding current treatment by a neurologist (yes or no). These data were used to describe the study sample and were analyzed using descriptive statistics, reporting frequencies, medians, or means.
The follow-up questionnaire included two Likert scales to evaluate participants’ expectations and the importance they attributed to services and care provided by MS practices and HCPs. The statements in the questions were developed using input from SMSR participants provided during the focus group workshop. Each statement reflects aspects of care that were identified and collectively agreed upon by the focus group participants as key elements of care provision in clinics, or as essential qualities of HCPs. The Likert scales comprised five response options: “not important at all,” “less important,” “no opinion,” “important,” and “very important.” Participants were instructed to select the response option that best aligned with their perception of the construct's importance. Additionally, participants were asked to evaluate the support they receive from their neurologists on a scale ranging from 1 to 10, using a slide-bar. These questions served as an introduction to the open-ended questions about neurologist-provided support and were analyzed descriptively, whereby the different care aspects were ranked by their perceived importance.
All questions utilized in the quantitative analysis are provided in the Supplemental material. All quantitative analyses were conducted in R and R studio. 18
Qualitative data collection
Qualitative data were collected through three open-ended questions specifically addressing the support provided by a neurologist. To best reflect current standards in neurological care and avoid recall bias, these questions were only accessible to participants who indicated ongoing neurological treatment. Participants were first prompted to describe the type of relationship they aspired to have with their neurologist. They were then asked to identify the most valuable aspects of support provided by their neurologist and provide reasons for their choices. Finally, participants were given the opportunity to express whether there was any additional support they would have liked to receive from their neurologists. Questions are provided in the Supplemental material.
Data were collected in Switzerland’s three official languages: German, Italian, and French. To ensure confidentiality, anonymized data from the three open-ended questions were automatically translated for analysis into English using the DeepL Pro desktop version for iOS. Prior to translation, the data underwent a thorough review to ensure the absence of any identifying information that could compromise anonymity. Translated data were manually inspected for quality, and occasional spot checks were conducted by a native speaker or a coauthor with native-level proficiency in the respective language.
Qualitative data analysis
Applying deductive thematic analysis, we explored and categorized types of support reported by the participants, as well as their fulfilled and unmet support needs, using the framework developed by Cutrona and Suhr. 13 The framework comprises five main categories (informational, emotional, tangible, esteem, and network support) and 23 subcategories and has previously been employed in pwMS. 19 To ensure the applicability of the framework to the local context of the MS community, we adapted the definitions of the subcategories of support in a collaborative process with an SMSR participant and citizen scientist who was over 55 years of age (IR).
Data from all three questions on support were independently coded by two coders (MS and JS). The results were then compared to establish a consistent and reliable coding procedure, and any discrepancies in codes were resolved through discussion between the coders. The first author then revisited the data through an iterative process to ensure adherence to the established coding consensus. Any data that did not fit into the predefined categories of the adopted coding framework were analyzed to identify new themes.
Finally, we provided a quantitative overview of the qualitatively analyzed data by displaying the numbers and frequencies of codes for the different types of support. Codes falling within the same support category were counted only once per participant.
Data analysis was conducted using the MAXQDA software for qualitative data analysis. 20
Results
Sample description and quantitative analysis
A total of 2238 invitations were sent to SMSR participants, of which 786 were aged 55 or older at the time of invitation. Of these invitations, 1016 participants responded to the survey, of whom 302 were 55 years of age or older. This represents a response rate of 45.4% for the entire cohort and 38.4% for those aged 55 years and over. The median age of nonresponders was 62.0 years with interquartile range (IQR) of 58.0 to 68.0 years, and 66.2% of them were women.
The quantitative analysis included data from 286 participants aged 55 or older at the time of questionnaire completion, among whom 44 participants (15.4%) were not receiving neurological care (Figure 1). The median age was 61.0 years, with an IQR of 57.0 to 66.0 years. Two-thirds of the participants were female (N = 191, 66.8%), and the majority had RRMS (N = 138, 48.3%). Participants who were not receiving neurological care were more frequently female (N = 34, 77.3% compared to N = 157, 64.9%), older (median age of 64.5, IQR 61.0 to 70.0 years compared to 60.0, IQR 34.0 to 56.0 years), and had been living with MS for a longer duration compared to those who were receiving neurological care (median of 23.5, IQR 18.3 to 38.3 years compared to median of 21.0, IQR 15.0 to 30.0 years) (Table 1). Participants who were in neurological care rated the neurologist-provided support with a median score of 8.0 (IQR 7.0 to 9.0), out of a maximum score of 10.0.

Study design flowchart.
Socio-demographic, health and MS-related characteristics of the study sample.
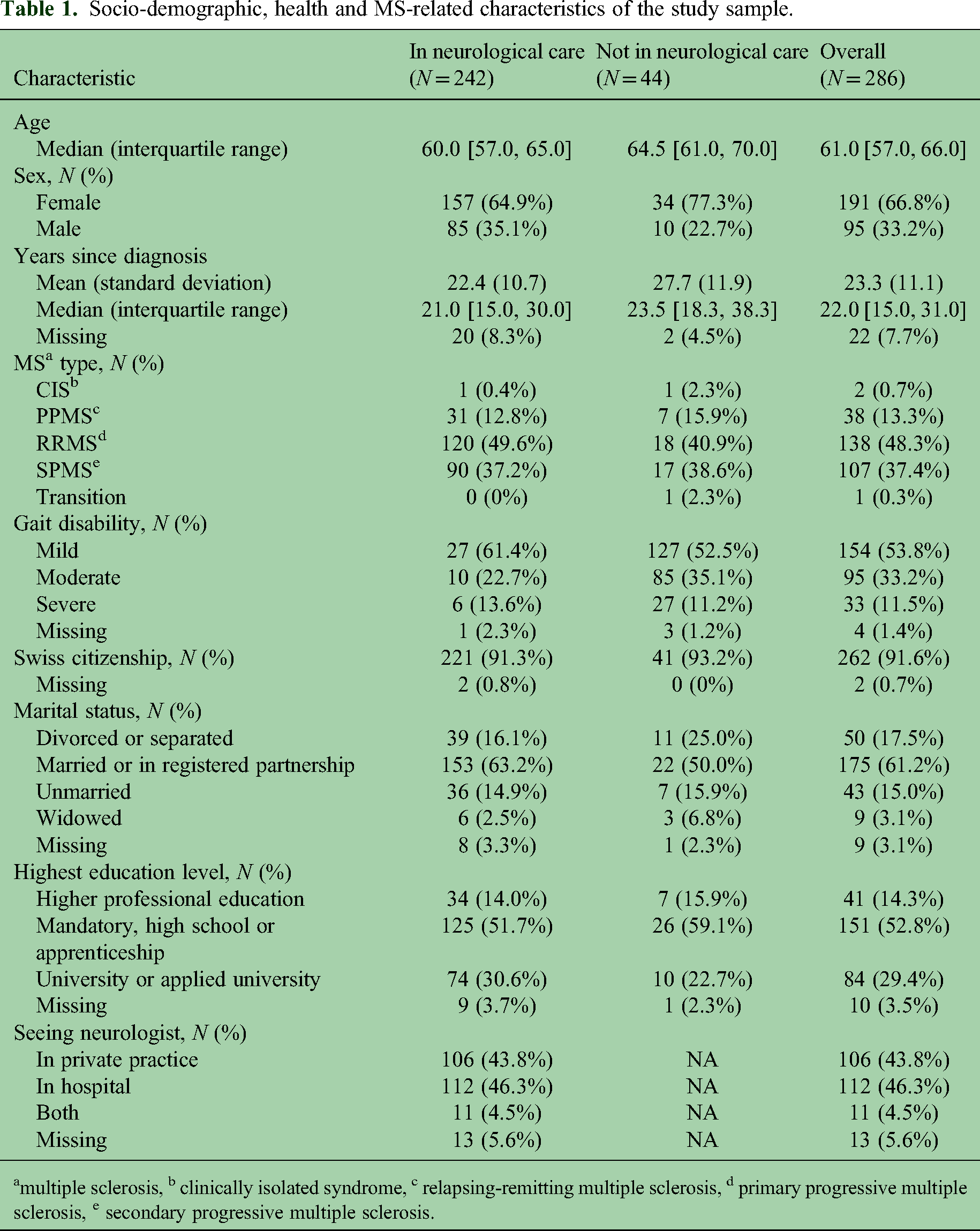
multiple sclerosis, b clinically isolated syndrome, c relapsing-remitting multiple sclerosis, d primary progressive multiple sclerosis, e secondary progressive multiple sclerosis.
Figure 2 illustrates the distribution of importance ratings given by participants to services and infrastructure in practices, clinics, and rehabilitation centers. Participants receiving neurological care prioritized experience and expertise in MS of the practice staff over practical aspects such as infrastructure. For participants not receiving neurological care, easy access to the practice or clinic was also very important. Figure 3 shows the distribution of importance participants attached to qualities and expertise of HCPs in MS care. Participants rated the allocation of sufficient time by HCPs and their MS expertise as most important, while the provision of emotional support by the HCPs was perceived as comparatively less important. Supplemental material provides visual analysis of Likert scale questions by MS type subgroup, as well as mean scores for each statement by subgroups of sex, age, MS duration, MS type, and gait disability.
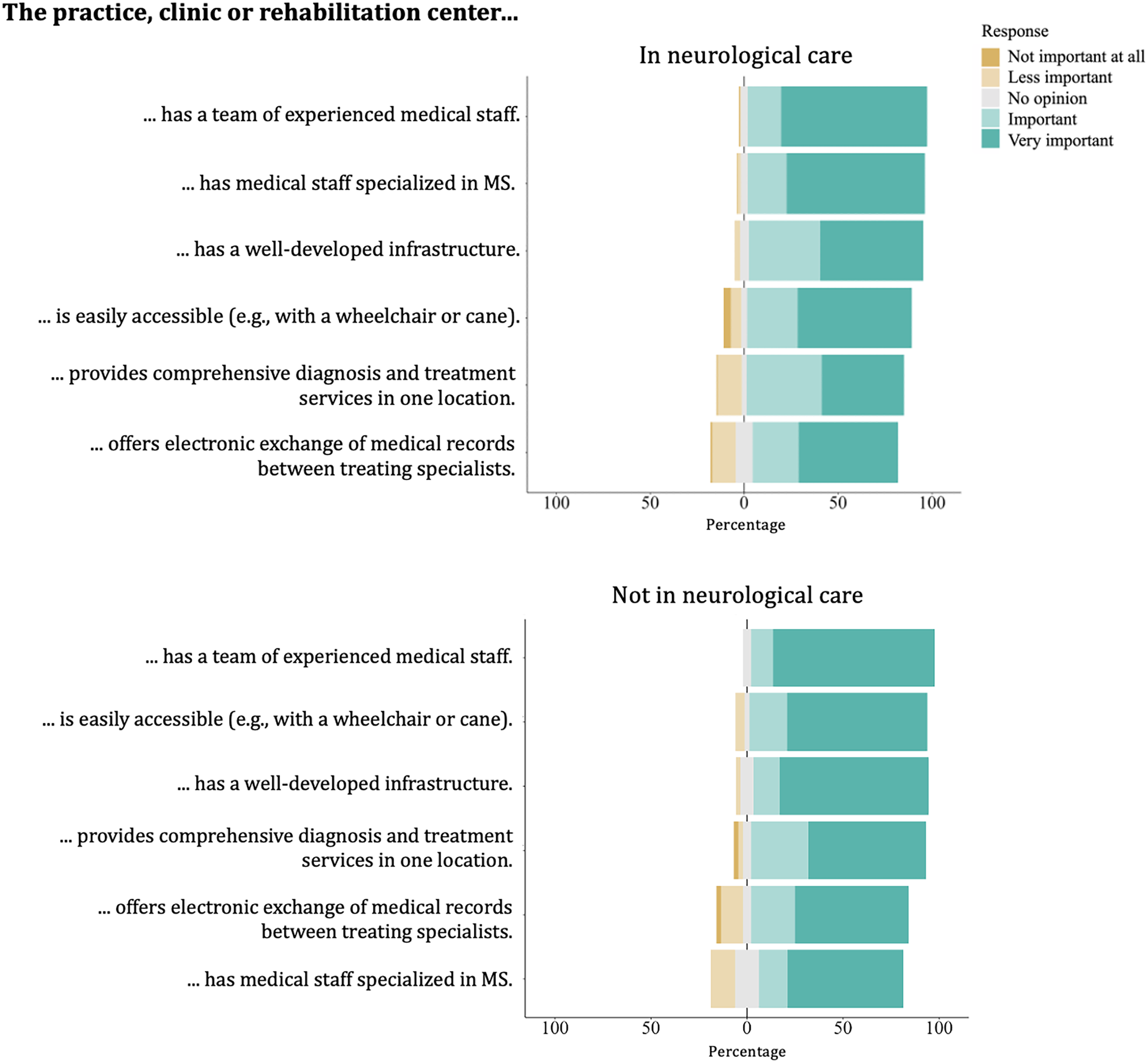
Participants’ ratings of the importance of services and infrastructure in practices, clinics, and rehabilitation centers.

Participants’ ratings of the importance of the qualities and expertise of healthcare professionals in providing MS care.
Identified dimensions of support and met needs in the neurologist–pwMS relationship
We identified all five support dimensions following Cutrona and Suhr's framework 13 in 489 free-text inputs from 230 participants who answered at least one open-ended question (Figure 1). However, some framework proposed subcategories were not supported by the data. Figure 4 illustrates both identified and unsupported subcategories along with contextual adaptations and explanations.

Adapted social support coding framework by Cutrona and Suhr, incorporating context-modified descriptions of the purpose of supportive behaviors. The dimensions of social support identified in the relationship between neurologists and older persons with multiple sclerosis (pwMS) are represented in black. In
Among the five support dimensions outlined by the framework, informational support was most frequently mentioned, with 187 mentions from 123 participants, followed by emotional support, identified 105 times in inputs from 78 participants. Esteem support was the least prevalent category, mentioned in 26 instances by 21 participants. Supplemental material offers an overview of the frequency of codes by sex and MS type.
Table 2 presents participants’ perceived support and met needs across support categories and subcategories, narratively summarizing key themes alongside example quotes and brief keyword summaries. Identified themes were found to be interconnected, with similar themes recurring across multiple subcategories (e.g., perception of expertise, clear communication, and shared decision-making in teaching, advice, and suggestions). Subcategories were also interdependent, with factors such as continuous presence facilitating long-term relationships and trust, and sufficient consultation time enabling patient inquiries to be addressed effectively.
"Through the long-standing doctor–patient relationship, we know that we can trust each other."
Overview of identified types of perceived support and met support needs in the relationship between older pwMS and neurologists.

pwMS: persons with multiple sclerosis.
Unmet support needs in the neurologist-pwMS relationship
Unmet needs within the support domains were relatively uncommon compared to met needs. Present in the data of 36 participants, the most commonly observed unmet need was for informational support, followed by emotional and network support, each mentioned by 11 participants. Similar to met needs, there was an interdependency between support domains, notably prominent with insufficient time allocation or the absence of long-term availability of the same neurologist resulting in lacking emotional support.
“As the doctors always change, the emotional support also stays out.”
Table 3 presents an overview of key themes concerning unmet needs, including a call for improved educational and advisory services, communication tailored for lay comprehension, and the integration of teaching on complementary medicine. Additionally, there was an emphasized need for heightened empathy and increased availability of neurologists.
Overview of identified types of unmet support needs in the relationship between older pwMS and neurologists.

pwMS: persons with multiple sclerosis.
Absence of need for emotional support
Finally, 21 participants explicitly stated that they did not need emotional support. Their perspective is rooted in their preference for the neurologist's primary role to be focused on medical guidance. Mild disease course, satisfaction with support from friends and family, and a preference for keeping emotional matters private in interactions with HCPs contributed to the participants’ lack of need for neurologist-provided emotional support. Supplemental material shows characteristics of these participants.
“Since my MS has been calm since the first relapses and I have only minor complaints, I do not need any emotional support-I feel very well taken care of by my wife and family.”
Discussion
In this mixed-methods study, we analyzed survey data from 286 participants aged 55 years or older in the SMSR. Participants rated the importance of MS care aspects and provided free-text insights into the support provided by their neurologists. Quantitative analysis showed that participants prioritized HCP expertise and sufficient time for consultations, with less emphasis on HCP-provided emotional support and practical services. Qualitative analysis focused exclusively on the relationship with the neurologists and largely mirrored the quantitative results by highlighting the importance of sufficient consultation time and informational support. Emotional support from neurologists, characterized by empathy and understanding, was also a highly valued aspect of support in the qualitative analysis. Finally, instances of unmet needs were relatively uncommon across support categories, with informational and emotional support representing primary areas for improvement.
Neurologists are regarded as the preferred source of information for pwMS, 11 who in turn recognize information provision as a core role of neurologists. 12 Similarly, among various information sources, older pwMS predominantly seek informational support from HCPs. 9 Our findings confirm this trend, with participants rating HCP information provision as paramount and emphasizing the significance of informational support from neurologists, particularly in educational aspects. Informational support was the most favorable when it was expertise-based, using understandable language, and providing actionable guidance and comprehensive care that includes information relevant to daily life with MS. This aligns with earlier research indicating that older pwMS expressed concern over the lack of specificity in neurologists’ instructions 6 and valued HCPs who not only facilitated access to information and services but also offered guidance on day-to-day issues. 8 Furthermore, neurologists who actively sought patient input were commended for considering patients’ perspectives and engaging in shared decision-making, addressing not only treatment-related decisions but also other aspects such as employment.
A recognized gap in HCP-provided informational support for pwMS includes information on disease course, treatment options, available services, diet, exercise, and complementary medicine.21,22 In our study, the most frequently cited unmet information need was for complementary medicine, alongside mental health and prevention. Increased interest in complementary medicine, less emphasized in prior research, may stem from the limited range of disease-modifying therapeutic options available to older pwMS, prompting exploration of alternative treatments. Effective information provision, along with motivation, especially by neurologists, is crucial as it can positively influence behavioral changes in pwMS, improving their physical, psychological, and social well-being. 23–25 However, constraints like time, training gaps, and insurance issues have been identified as barriers for promoting exercise among neurologists, 26 and may similarly affect other aspects of comprehensive informational support, such as offering guidance on complementary medicine. Therefore, involving other HCPs in MS care, such as MS nurses, occupational therapists, or physiotherapists, could address the unmet informational needs of pwMS, ensuring comprehensive care delivery.
Thus far, there has been limited understanding of more subtle support aspects, such as emotional and esteem support. Although HCP-provided emotional support ranked lower in importance in quantitative analysis, in qualitative analysis neurologist-provided emotional support emerged as highly valued. Our participants valued encouragement, understanding, and empathy from their neurologists, with a minority expressing a desire for increased empathy, aligning with previously identified unmet needs. 6 Neurologists and physicians caring for pwMS perceive physical functions, such as mobility and ambulation, as the most important bodily function, 27 leading them to prioritize treatment of physical symptoms. 28 As a result, less attention may be given to providing emotional support. However, according to our findings, neurologist–pwMS relationships focusing solely on medical treatment can be satisfactory, especially for those with milder disease courses or strong social support from other sources.
Regardless of disease course or emotional support needs, the availability of neurologists, continuous care, and remote communication were pivotal in fostering effective relationships between older pwMS and neurologists. Approachable HCPs and readily available services were previously found to be appreciated by older pwMS. 4 Additionally, HCPs who supported older pwMS in acquiring knowledge and confidence contributed to strengthening patients’ self-management over time. 10 While the notion of neurologists providing hope, as previously observed in individuals with disabling MS, 12 was not evident in our study, encouragement, motivation, validation, and respectful treatment further fortified the doctor–patient relationship and mutual trust. Previously, persons severely affected by MS expressed a desire for increased respect from physicians. 21 Although this did not surface as an unmet need, our study highlighted a desire for supportive language and validation of participants’ perceptions of symptoms, particularly regarding fatigue. Considering that fatigue has been recognized as one of pwMS’ major concerns, 28 dedicating greater attention to its management may lead to improvements in patient-reported outcomes.
Finally, several subcategories of support proposed by the framework, such as relief of blame, compliments, or physical affection, were not observed in our data either as met or unmet needs. This suggests that the support provided by neurologists is not exhaustive, nor is it expected to be. Neurologist support constitutes only a component of overall support and should not replace support from other relationships, including both other healthcare professionals involved in MS care, as well as friends and family, which are recognized as crucial sources of support for pwMS.29–31
Strengths and limitations
To our knowledge, this study is the first to exclusively explore neurologist support for older pwMS, enabling detailed investigation of the specific needs of older pwMS. By integrating quantitative and qualitative methods and analyzing data from over 200 participants, we ensured data saturation and the comprehensiveness of our findings. Nonetheless, there are limitations to this study. The use of exploratory rather than validated questionnaires and scales to assess expectations about MS care and to measure support may have provided a less reliable assessment of these aspects. Additionally, the COVID-19 pandemic and the sequence of the questionnaire, with support-related questions placed at the end, may have contributed to selection bias, affecting response rates and completion. The pandemic may also have influenced participants’ perceptions of support from their neurologists, especially since some consultations may have been conducted online; however, no evidence of such influence was supported by the data. Lastly, our findings are shaped by Switzerland's healthcare landscape, including virtually universal insurance coverage and healthcare access. Certain findings, such as unmet needs related to changing neurologists, may be context-specific.
Conclusions
Older pwMS see neurologists as adequate providers of informational, esteem, network, emotional, and tangible support. Older pwMS value neurologists who provide comprehensive care, bringing expertise, guidance, and teaching, coupled with attentive listening and understanding. Continuous care, regular consultations, and remote communication are key in forming mutual trust and a reassuring doctor-patient relationship. Unmet needs, primarily insufficient information on complementary medicine, empathy, and understanding of symptoms like fatigue, are relatively uncommon within support categories. Our findings can aid neurologists in identifying and addressing support gaps to meet their patients’ needs.
Supplemental Material
sj-docx-1-mso-10.1177_20552173241281458 - Supplemental material for Exploring the relationship between neurologists and older persons with multiple sclerosis through the lens of social support theory
Supplemental material, sj-docx-1-mso-10.1177_20552173241281458 for Exploring the relationship between neurologists and older persons with multiple sclerosis through the lens of social support theory by Mina Stanikić, Felix Gille, Jonas Schlomberg, Paola Daniore, Susanne Kägi, Andrew Chan, Christian P Kamm, Chiara Zecca, Pasquale Calabrese, Patrick Roth, Claudia Baum, Irene Rapold, Milo A Puhan and Viktor von Wyl in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of competing interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mina Stanikić, Jonas Schlomberg, Paola Daniore, Irene Rapold, Claudia Baum, Susanne Kägi, Milo Alan Puhan, and Viktor von Wyl declare no competing interests. Felix Gille receives funding from the Digital Society Initiative, University of Zurich, Novartis International AG and Sanitas Krankenversicherung (Stiftung) outside of the submitted work. Andrew Chan has received speakers'/board honoraria from Actelion (Janssen/J&J), Alexion, Almirall, Bayer, Biogen, Celgene (BMS), Genzyme, Merck KGaA (Darmstadt, Germany), Novartis, Roche and Teva all for hospital research funds. He received research support from Biogen, CSL Behring, Genzyme, and UCB, the European Union, and the Swiss National Foundation. He serves as associate editor of the European Journal of Neurology, on the editorial board for Clinical and Translational Neuroscience and as topic editor for the Journal of International Medical Research. Christian P Kamm has received honoraria for lectures as well as research support from Biogen, Novartis, Almirall, Teva, Merck, Sanofi Genzyme, Roche, Janssen, Eli Lilly, Celgene and the Swiss MS Society. Ente Ospedaliero Cantonale (employer) received compensation for Chiara Zecca's speaking activities, consulting fees, or research grants from Almirall, Biogen Idec, Bristol Meyer Squibb, Lundbeck, Merck, Novartis, Sanofi, Teva Pharma, Roche. Chiara Zecca is recipient of a grant for senior researchers provided by AFRI (Area Formazione accademica, Ricerca e Innovazione), EOC. Pasquale Calabrese has received honoraria for speaking at scientific meetings, serving at scientific advisory boards and consulting activities from Abbvie, Actelion, Almirall, Bayer-Schering, Biogen, EISAI, Lundbeck, Merck Serono, Novartis, Sanofi-Aventis and Teva. He also receives research grants from the Swiss Multiple Sclerosis Society (SMSG), and the Swiss National Research Foundation. Patrick Roth has received honoraria for lectures, consulting or advisory board participation from Alexion, Bristol-Myers Squibb, Boehringer Ingelheim, Debiopharm, Galapagos, Laminar, Midatech Pharma, Novocure, QED, and Roche, travel support from Sanofi and research support from Merck Sharp and Dohme and Novocure.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Swiss Multiple Sclerosis Registry (SMSR) is funded by the Swiss Multiple Sclerosis Society (SMSG).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.