
Abstract
Background
The development of personalized interventions aimed at coping with multiple sclerosis is enriched by the understanding of patients’ representations of the illness.
Objective
The aim of this study was to investigate the association between patients’ illness representations versus contextual factors (i.e. presence/absence and type of caregiver, engagement, frequency and type of rehabilitation), fatigue, pain, and neurological impairment.
Methods
Interviews of 28 patients were analysed through an automated text analysis procedure. After a systematic labelling procedure four illness representations were identified: daily life, search for meaning of the disease, relationship to people and the diagnosis, coping and physical growth.
Results
Findings showed that the representation of the relational aspects of the illness was associated with the caregiver's presence, while the representation related to coping and growth tended to be associated with participation in rehabilitation programs. Moreover, the representation related to daily life was associated with lower levels of fatigue compared to the representation related to coping and growth, and with higher levels of neurological impairment compared to the representations related to coping and growth and the relational aspects of the illness.
Conclusion
Exploring illness representations is a key step that can help health professionals to get an integrated perspective that could be useful in designing and calibrating interventions according to specific patient needs.
Introduction
Due to relevant physical and functional consequences of multiple sclerosis (MS)—such as fatigue, pain and neurological impairment—active disease management is a key factor to ensure a better quality of life for people with MS. 1
It was found that caregivers’ support, 2 whether primary or secondary, 3 as well as rehabilitation 4 could play an important role in managing and coping with the disease. Moreover, patients expressed dissatisfaction about the lack of individualized interventions,5,6 in fact the current standard interventions provided by healthcare seem to fail to take into account the specific needs of patients and may reflect the inability of healthcare professionals to listen to the deeper exigencies of the people with MS. 5
Personalized interventions could help patients in the treatment process enhancing their motivation in coping with the disease. 7 According to the narrative medicine approach, achieving the goal of personalized care requires narrative competence that allows access to the subjective dimension of the patient, to understand their suffering and to be clinically helpful. 8 A recent meta-synthesis 9 showed that addressing patients’ support needs and providing them with personalized information could improve adjustment to diagnosis. To this end, there is the need to understand patients’ illness representations (pIR), 10 which seem to influence adaptation to MS. 11
Previous studies have shown that pIR was associated with disabling symptoms and a severe impact on the person's functioning. 12 It was observed that the representation of the illness with a focus on symptomatology, uncertainty of causes, sudden onset, unpredictable course and uncertain prognosis had a strong impact on patients’ adjustment. 12 Vercoulen 13 found that patients who paid more attention to body sensations reported higher levels of fatigue. However, such studies are characterized by the exclusive use of the qualitative or quantitative method. To date, there are no studies that adopt a mixed method which can be of added value in understanding complex phenomena in clinical settings. 14 The present study aimed to fill this gap by investigating the association between pIR and contextual factors, as well as the difference among representations in relation to specific clinical manifestations. Such investigation could provide a more comprehensive view of the needs and challenges of patients with MS and can be helpful in personalizing care and supports, improving patient's quality of life and well-being.
Materials and methods
Participants
The study was conducted at the Paul VI Foundation (Centro Adriatico headquarters in Pescara) and the ambulatory of the Italian Multiple Sclerosis Association (AISM) headquarters in Pescara (Italy) from September 2021 to August 2022. Patients meeting the inclusion criteria of age between 18 and 60 years, a diagnosis of MS based on the McDonald 15 criteria and understanding Italian were recruited on a voluntary basis. Patients with relapses within the previous 30 days and with a history of psychiatric or substance-abuse disorders were excluded, as were those with pregnancy, tumours, rheumatological or diabetic conditions, previous surgery on the spine, cardiovascular disease or other neurological disorders. Patients were on a stable FDA-approved disease-modifying therapy regimen for at least 6 months, according to the indications of the reference neurologist.
Patients were accompanied by the researcher to a comfortable room, where they were asked to answer an open-ended question and fill out a battery of questionnaires. The researcher, who had no relationship with the patient, provided all the information regarding the purpose of the study and the procedures to be followed, then asked the patient to sign the informed consent. Thereafter, the researcher placed herself at an appropriate distance to allow the patient to carry out the task in quiet while remaining available for any questions or clarifications. Patients had the choice of completing the survey in paper or digital versions, using a computer in the room.
This cross-sectional study was created in accordance with the STROBE guidelines, 16 was approved by the Ethics Commission for Research in Psychology of the Department of Dynamic and Clinical Psychology, and Health Studies, Sapienza University of Rome (protocol no. 0001981 of 25/11/2022) and was in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Measures
Open narrative question
Patients were asked to answer the following open-ended question: ‘What does living with multiple sclerosis mean to you?’. The narrative inquiry was used to elicit patients’ ways of making sense of the illness. No time limits were indicated for replying. Patients who used PCs responded using a word file, while the responses of those who chose to use a sheet of paper were transcribed to word files by the researcher. The transcripts were checked for and corrected for possible typos.
Contextual factors
An ad hoc questionnaire was created to collect information about (a) absence or presence of a caregiver (by means of dichotomous variable 0, 1, respectively) and to specify whether it was a family member or a person outside the family; (b) the engagement in rehabilitation (0 = No, 1 = Yes), how often (once, twice, or three times a week), and the rehabilitation type (physiokinesiotherapy, physiokinesio and hydrokinesitherapy, physiokinesio and massotherapy, physiokinesiotherapy and pelvic floor).
Fatigue severity scale (FSS)
Fatigue was detected through the FSS scale. 17 The FSS consists of nine items assessing the impact of fatigue on daily activities and functioning scored on a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree).
Visual analogue scale (VAS)
Pain was evaluated using the visual analogue scale (VAS). 18 This method employs a continuous line which represents a spectrum of pain intensity ranging from ‘no pain’ at the leftmost end (0) to ‘maximum pain’ at the rightmost end (10).
Neurological impairment (Ni)
Pedersen's 19 system was used to detect levels of neurological impairment. The test consists of six items corresponding to six functions (A: mental state; B: visual function; C: sphincteric function; D: upper extremities; E: lower extremities; F: personal efficiency) assessed through a 5-level severity scale (5 = no abnormalities; 0 = requiring constant supervision).
Data analysis
Transcripts of the responses to the narrative question were subjected to the thematic analysis of elementary contexts (TAEC) using the T-Lab software 20 (cf., Thematic Analysis of Elementary Contexts procedure in supplementary material for technical details). The TAEC allows the textual corpus to be divided into clusters using the bisecting K-means method. 21 Each cluster aggregates together the texts that tend to have the same co-occurrences of lemmas or words. Therefore, each cluster is characterized by those patients who talk about the illness in a similar manner. 20 Therefore, according to this clustering method a patient can be associated only to one cluster.
Clusters were labelled by 20 Italian evaluators graduated in psychology, unaware of the research objectives, through a two-step procedure (for details see the two-step procedure for cluster labelling in supplementary material). This procedure has already been used in the literature 22 because it enables to increase in the impartiality, systematicity and reproducibility of the labelling process, by ensuring that the latter could reflect interpretations the more shared as possible. In addition, this method was supplemented with a discussion and consensus procedure 23 within the research team to confirm/adjust the labels to accurately reflect the representation of patients in the specific context.
The chi-square test was performed to test the association between clusters and contextual factors, namely (a) the presence/absence of a caregiver, (b) type of caregiver, (c) engagement in rehabilitation, (d) frequency of rehabilitation and (e) type of rehabilitation. Adjusted standard residuals were considered a post hoc procedure for a statistically significant chi-square test considering cells with absolute value above the threshold of 1.96. 24
The Kruskal–Wallis test was used to detect the differences among pIR on levels of fatigue, pain and neurological impairment of the patients, while also controlling for the presence/absence and type of caregiver, engagement or not in rehabilitation, and cycles of rehabilitation.
Results
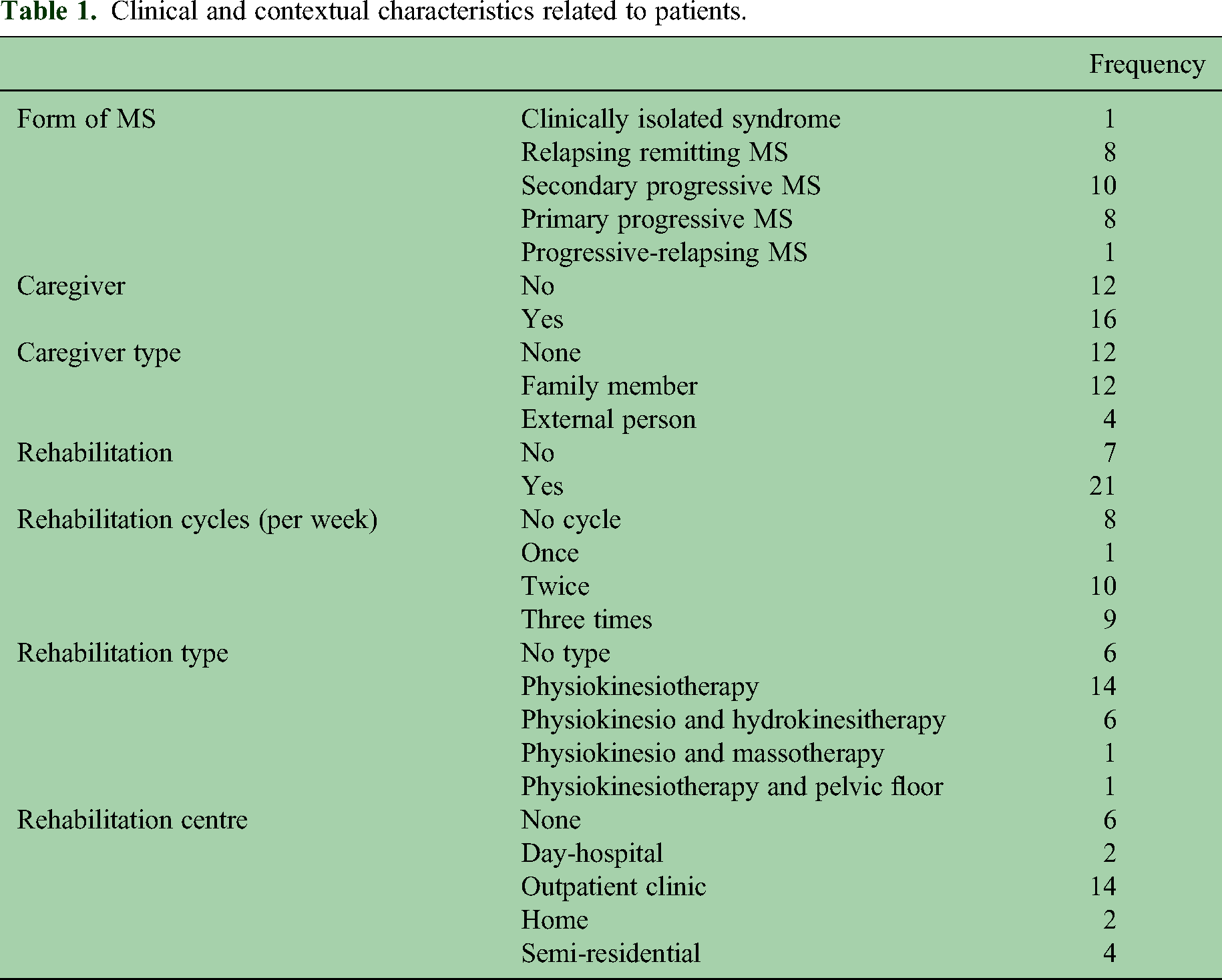
Twenty-eight Italian patients, mostly women (N = 20) with a mean age of 54.8 years (SD = 19.8), took part in the study. A bachelor's degree had been obtained by 42.9% of the patients, 35.7% had a high school diploma, 14.3% had a middle school diploma and 7.1% had an elementary school diploma. In addition, 35.7% of participants were single, 50% were married, 3.6% were divorced and 10.7% were widowed. Patients had been living with the disease for an average of 19.21 (SD = 13.46) years and reported a mean expanded disability status scale (EDSS) of 4.5 (SD = 2.4), a mean body mass index (BMI) of 24.9 (SD = 4.1) and a mean mini-mental state examination (MMSE) of 28.7 (SD = 2.1). Table 1 shows patients’ characteristics about the form of MS, presence and type of caregiver, presence of rehabilitation pathway, number of rehabilitation cycles, type of rehabilitation and rehabilitation centre.
Clinical and contextual characteristics related to patients.
The responses to the narrative inquiry that composed the text corpus had a mean length of 46 words. The text corpus was statistically processable because the type (distinct words)/token (occurrences) ratio (0.15) was below the recommended threshold of 0.20.25,26
Cluster analysis performed on the text corpus revealed four clusters (Calinski–Harabasz = 8.0; Davies–Bouldin = 0.6; ICC = 0.3) (Table SM1 in supplementary materials shows the characteristic lemmas of each cluster). The two-step procedure (see two-step procedure for cluster labelling in supplementary material for details) and the discussion among the members of the research group resulted in the following labelling of clusters:
Cluster 1 (33.3%): Daily life. Lemmas concerning common aspects of everyday life (e.g. work, help), as well as temporal units (e.g. moment, day).
Cluster 2 (21.2%): Search for meaning of the disease. The effort to find remedies to the disease condition (e.g. try, difficulty, strength, problems) and the process of making sense of such condition (e.g. meaning, seek).
Cluster 3 (15.2%): Relationship to people and the diagnosis. Interpersonal bonds (e.g. friend, husband) and the motivation to cope with disease through active behaviours (e.g. accept, learn).
Cluster 4 (30.3%): Coping and physical growth. The recovery of bodily functionality (e.g. body, own) and the ability to cope with the disease through different means (e.g. coping, find).
Of the 28 patients, 33.3% were associated with a life-related representation, 21.2% were associated with a meaning-related representation, 15.2% were associated with a relationship-related representation and 30.3% were associated with a coping and growth-related representation. Examples of text, and their characteristic words (in bold), associated with each cluster are given below.
Daily life: At the At the present time I have no I think my It means
Standardized adjusted residuals.

A trend toward significance emerged between pIR and the rehabilitation variable (χ2[3, 28] = 7.6, p = .056). The adjusted standard residuals (Table 2) showed that pIR daily life tended to be associated with not doing rehabilitation, while pIR coping and physical growth tended to be associated with doing rehabilitation. No significant association was found between pIR, cycles and type of rehabilitation (respectively: χ2[6, 20] = 6.1, p = .4; χ2[9, 22] = 9.0, p = .435).
The Kruskal–Wallis test (Figure 1) showed a significant difference between pIR in the levels of fatigue (H = 11.2, p = .010) and neurological impairment (H = 8.7, p = .033). The pairwise comparisons (Table 3) indicated that pIR coping and physical growth reported higher levels of fatigue than pIR daily life. Moreover, pIR daily life had lower levels of neurological impairment than pIR coping and physical growth and relationship to people and the diagnosis. No significant difference was found between pIR in relation to pain (H = 1.7, p = .626).

Pairwise comparisons of the independent-samples Kruskal–Wallis Test. Note. FSS: Fatigue Severity Scale; NI: neurological impairment. Each box in the graph covers an average of 50% of the data. The lower and upper edges (hinges) of the box indicate the first and third quartiles, respectively. The middle line of the box indicates the median. The length of the box is the interquartile range (IQR). The whiskers show the range of the remaining 50% of the data and extend to the extreme values (minimum and maximum values).
Kruskal–Wallis pairwise comparisons.

Note. FSS: Fatigue Severity Scale; NI: neurological impairment. 1: Daily life; 2: Search for meaning of the disease; 3: Relationship to people and the diagnosis; 4: Coping and physical growth.
The Kruskal–Wallis test controlling for the presence/absence of a caregiver showed that among patients who did not have a caregiver (H = 6.4, p = .040), those with a daily life representation had lower levels of fatigue than those with a coping and physical growth representation (p = .012). No significant difference emerged among patients who had a caregiver. However, if the caregiver was a family member (H = 8.0, p = .045) patients with a daily life representation showed lower levels of fatigue than patients with a search for meaning of the disease (p = .049) and coping and physical growth (p = .015) representation. No difference emerged between patients’ representations controlling for caregiver presence/absence and type in relation to pain and neurological impairment. Finally, no difference emerged between patients’ representations controlling for engagement or not in rehabilitation and cycles of rehabilitation in relation to fatigue, pain and neurological impairment. Table 4 summarizes these results.
Kruskal–Wallis pairwise comparisons in fatigue levels.

Note. 1: Daily life; 2: Search for meaning of the disease; 3: Relationship to people and the diagnosis; 4: Coping and physical growth.
Discussion
The results of the textual analysis showed that patients with MS represented their illness in terms of daily life, search for meaning of the disease, relationship to people and the diagnosis, coping and physical growth.
Similar content has emerged in other studies,12,27–29 suggesting that patients with MS tend to represent and communicate their condition in similar ways.
The inspection of the standardized adjusted residuals of the chi-square test showed that the representation that foregrounded aspects related to the search for meaning of the disease was associated with the absence of a caregiver, while the representation focused on the relationship with people and the diagnosis was associated with presence, suggesting that patients with a caregiver might have access to more practical and emotional support, which could lead to emphasizing relational dynamics, and this regardless of whether the caregiver was a family member or an external person.
Moreover, the standardized adjusted residuals of the chi-square test showed that patients with a representation of illness centred on aspects of daily life tended to be associated with not doing rehabilitation, while the representation focused on coping and physical growth tended to be associated with doing rehabilitation. This trend might suggest that attention to growth aspects could influence and be influenced by the benefits of rehabilitation practices at the physical, mental and social levels. 30
Similarly to a previous study, 13 the finding of the present one showed that patients’ illness representation that foregrounded the aspects related to coping and physical growth reported higher levels of fatigue than patients with a representation focused on daily life aspects. This difference characterized patients who had no caregiver and those who had a primary caregiver (i.e. a family member), suggesting that patients with relative caregivers or without caregivers could feel greater levels of fatigue in relation to growth programs than patients supported by professional caregivers. Moreover, patients who emphasized the aspects of search for meaning of the disease reported higher levels of fatigue than patients with a daily life-related representation.
Finally, patients’ illness representation centred on daily life aspects had less neurological impairment than patients whose representation foregrounded the aspects related to coping and physical growth and relationship to people and the diagnosis. This result could suggest deepening the motivations and real needs of patients with a daily life-related representation of illness to clarify the origin of this specific meaning that could be a real expression of a lower impact of the disease, but that in the subsequent years could facilitate a denial mechanism of the degenerative aspects of the disease. Furthermore, it is worth noting that the search for meaning of the disease representation that emerged in the present study seems to be characterized by aspects related to seeking a sense of control over the disease, which has been seen to be associated with better outcomes in a previous systematic review. 11
Overall, the findings of the present study offer some clinical insights. To promote a representation that considers the relational aspects of the illness could act as a protective factor 31 in patients without a caregiver. Promoting narratives related to coping and physical adaptation could incentivize patients to engage in rehabilitation programmes and develop greater adherence to treatment, as attention to the body dimension has been seen to result in a sense of well-being. 32 To consider that pIR related to the relationship and the growth that seems to present a greater neurological impairment and fatigue compared to pIR that emphasize the aspects of daily life could help the clinician to interpret the subjective symptoms of the patients.
In conclusion, consistent with a personalized approach to care and the need for an interdisciplinary dialogue between medical and psychological areas, exploring pIR becomes a preliminary step in building a body of knowledge useful to develop tailored interventions according to the specific needs of the patient.
Limitations and future research
The cross-sectional design of this study does not allow to determine whether it is pIR that influences contextual and clinical factors or whether it is the other way around. The small sample size does not allow for the generalization of results, and examining a larger sample would improve statistical power. Although the differences between clusters were significant with respect to fatigue levels and neurological impairment, as shown in Figure 1, the clusters were not clearly differentiated. This may be due to the small sample size, which, if increased, might reveal these distinctions more clearly. The lack of instruments to measure psychological factors makes it difficult to ascertain their impact on pIR. Although cluster analysis allows for the differentiation in how patients use the same word based on its co-occurrence with other words, it does not identify potential different meaning attributed to the same word within the same cluster. Future research could include a confrontation with patients useful for verifying the accuracy of the interpretation of the different clusters.
The authors plan to conduct a further longitudinal study to understand the direction of the associations found in the present study. In addition, they plan to recruit a larger sample and integrate the investigation of the association between pIR and psychological factors as well as how these relationships influence coping strategies and adjustment to illness.
Supplemental Material
sj-docx-1-mso-10.1177_20552173241271755 - Supplemental material for Illness representation in patients with multiple sclerosis: A preliminary narrative medicine study
Supplemental material, sj-docx-1-mso-10.1177_20552173241271755 for Illness representation in patients with multiple sclerosis: A preliminary narrative medicine study by T Paolucci, M Reho, C Ciacchella, G Veneziani, I Santoro, G Fiorentino, F Galli and C Lai in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors would like to thank the Paul VI Rehabilitation Center in Pescara and the Italian Multiple Sclerosis Society (AISM).
Data availability
The data of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.