
Abstract
Background:
Cognitive dysfunction is a frequent manifestation of multiple sclerosis (MS) but its effect on locomotor rehabilitation is unknown.
Objective:
To study the impact of cognitive impairment on locomotor rehabilitation outcome in people with MS.
Methods:
We performed a retrospective analysis involving ambulatory patients with MS who were admitted for intensive, inpatient, multidisciplinary rehabilitation at the National Multiple Sclerosis Center of Melsbroek between the years 2012 and 2017. The Brief Repeatable Battery of Neuropsychological Tests (BRB-N) was used to determine the cognitive status of subjects as either impaired (COG–) or preserved (COG+). Locomotor outcome was compared between groups with the difference in 6-minute walk test (6MWT) measured at admission and discharge (Δ6MWT). In addition, individual test scores of the BRB-N for attention (Paced Auditory Serial Addition Test 2” and 3”), visuospatial learning/memory (7/24 Spatial Recall Test), verbal learning/memory (Selective Reminding Test) and verbal fluency (Controlled Oral Word Association Test) were correlated to the Δ6MWT.
Results:
A total of 318 complete and unique records were identified. Both groups showed a significant within-group Δ6MWT during hospitalization (COG+: 47.51 m; COG–: 40.97 m; P < .01). In contrast, Δ6MWT values were comparable between groups. The odds of achieving a minimal clinical important difference on the 6MWT did not differ significantly between both groups. Only attention/concentration was significantly correlated with Δ6MWT (r = 0.16, P = .013).
Conclusion:
Cognitive impairment based on BRB-N results appears not to impede locomotor rehabilitation in ambulatory patients with MS. Attentional deficits are correlated to the extent of locomotor rehabilitation, suggesting the presence of a subtle effect of cognition.
Keywords
Introduction
Multiple sclerosis (MS) is a leading cause of neurological disability in young to middle-aged adults. Among the symptoms, locomotor deficits are highly prevalent and increase fall occurrence, 1 social isolation, 2 and societal economic burden. 3 Intensive rehabilitation has been shown to significantly improve locomotor function in people with MS (PwMS) 4 and can be optimized by identifying potentially hampering factors. More specifically, cognitive dysfunctioning is associated with poorer rehabilitation outcomes on the 2- and 6-minute walk test (2MWT, 6MWT) in other medical conditions.5,6 This effect potentially extends to MS, because cognitive dysfunction occurs in up to 70% of PwMS and can be present from the earliest disease stage. 7 Common manifestations include impairment of information processing speed, short-term memory, attention, executive function, and abstract conceptualization. As patients are intensively guided by a physical therapist during locomotor rehabilitation, these factors might impact understanding, memory, and execution of their instructions, thereby indirectly hindering rehabilitation goal attainability. The specific impact of cognitive status on locomotor improvement is as yet unknown in MS. For this reason, we aimed to compare locomotor improvement after rehabilitation in cognitively impaired versus cognitively preserved PwMS. A secondary analysis comprised exploring associations between locomotor improvement and separate domains of the Brief Repeatable Battery of Neuropsychological Tests (BRB-N), 8 a commonly used and sensitive test to capture cognitive dysfunction in MS. The tests that form the BRB-N assess attention, visuospatial learning and memory, verbal learning and memory, and word fluency.
Methods
Trial design
This study used a retrospective pre-post cohort comparison design. Data were retrieved from the electronic medical databases (KWS and EDMUS) of the National MS Center Melsbroek (NMSC) for all rehabilitation admissions between 2012 and 2017.
Ethics
As stated by the Belgian law of May 7, 2004, informed consent is not needed, and advice of the institutional ethics committee does not have to be sought, for a study that includes the review of clinical files under supervision of a member of the clinical team responsible for the patient. This was the case in our study.
Participants
All rehabilitation admission records of adults (⩾ 18 years) with any type of MS and a score of ⩽ 6.5 on the Expanded Disability Status Scale (EDSS) 9 were considered. The EDSS is a commonly used method of quantifying disability in MS on a score range from 0 to 10, with a higher score indicating higher disability. A score of 6.5 is the highest score at which patients are still considered ambulatory, requiring 2 walking aids to walk about 20 meters without resting. Hence, this score was used for our ambulation inclusion criterion. In case of multiple hospitalizations during the time period between 2012 and 2017, the first hospitalization record for that patient was consistently included.
Intervention
Patients hospitalized for 3 to 4 weeks in NMSC Melsbroek are offered a multidisciplinary rehabilitation program, designed according to principles described in Khan et al. 10 Briefly, the approach consists of an individualized program, 3 hours per day, 5 days per week including physical therapy, occupational therapy, respiratory therapy, psychotherapy, nursing, and social support.
Grouping variable
The BRB-N developed by Rao et al 8 was used to measure cognitive status. The BRB-N consists of 4 tests: Paced Auditory Serial Addition Test (PASAT) 2” and 3” version for attention, 11 7/24 Spatial Recall Test (SPART) for visuospatial learning and memory,12,13 Selective Reminding Test (SRT) for verbal learning and memory, 14 and the Controlled Oral Word Association Test (COWAT) for verbal fluency. 15 For each test in the battery, a score of 0, indicating impairment on the corresponding cognitive domain, was assigned if the score was less than the 5th percentile of normative data from a reference population for that test. Otherwise a score of 1 was assigned. 16 As suggested by Rao et al,8,16 patients were classified as “cognitively impaired (COG–)” if the total score on the BRB-N was 0, 1, or 2, and “cognitively preserved (COG+)” if the BRB-N score was 3 or 4. This cutoff criterion is consistently used in the literature. 17
Primary outcome measure
Standard practice at NMSC Melsbroek includes assessment of locomotor function at baseline and discharge by means of the six minute walk test (6MWT) in each patient admitted for rehabilitation. Differences between baseline and discharge scores in the COG– group were compared with those of the COG+ group. 18
Statistical analysis
We used 2 approaches in our main analysis. First, we performed a Wilcoxon signed-rank test and Mann-Whitney U test to compare mean Δ6MWT within and between groups, respectively. In addition, Fisher exact test for categorical/frequency variables was used to compare the odds of obtaining a minimal clinically important difference (MCID, ⩾ 9% relative improvement) 19 in the cognitively impaired versus the cognitively preserved group.
In our second approach, we individually correlated the test scores of the BRB-N with the Δ6MWT.
Significance level was α = 0.05 for all analyses. Microsoft Excel was used to collect the data, MATLAB v2017a 20 and Python version 3 were subsequently used to perform statistical analyses and for visualization purposes.
Results
A total of 1129 records from our clinical database met the inclusion criteria in the period 2012 to 2017. As most patients were admitted more than once in this timeframe, 469 unique and first hospitalization records were retrieved. A total of 318 contained all required information to describe patient characteristics and perform analyses (82 patients in the COG– group and 236 in the COG+ group). Group characteristics are displayed in Table 1. The age-related MS severity score (ARMSS) was additionally calculated to display disease severity of the included population. 21 Group characteristics were comparable except for education level, measured by the amount of years of education participants followed, which differed significantly between groups (difference = 1.49 years, P < .01).
Group characteristics table.

Abbreviations: ARMSS, age-related multiple sclerosis severity score; COG–, cognitively impaired; COG+, cognitively preserved; EDSS, Expanded Disability Status Scale; LOS, length of stay.
Notation: Age: Mean (SD); Sex: M = Male, F = Female; LOS: Mean (SD); ARMSS and EDSS: Median; Interquartile range; Education level: Mean (SD).Statistics: independent t-test was used for Age and Education level, Mann-Whitney U test was used for Sex, LOS, ARMSS and EDSS.
For our main analysis, both groups improved significantly during hospitalization, COG+: 47.51 m (SD: 64.79 m, P < .01), COG–: 40.97 m (SD: 44.94 m, P < .01). No correlation was found between Δ6MWT and baseline 6MWT values (r = –0.04, P = .45). We found no significant difference (6.54 m, SD: 60.33 m, P = .46, Figure 1) in locomotor improvement between the COG– and the COG+ group. Furthermore, we created a 2 × 2 contingency table based on BRB-N scores and a second categorization variable, being the MCID on the 6MWT (Table 2). Fisher exact test yielded a nonsignificant odds ratio of 1.19 (P = .52, Table 2).

Δ6MWT distribution per group. The white dot within the boxplot denotes the median value, whereas the box indicates the interquartile range.
A 2 × 2 contingency table.

Abbreviations: MCID, minimal clinically important difference; COG–, cognitively impaired; COG+, cognitively preserved.
For our secondary analysis, we calculated the Pearson correlation coefficient and the accompanying P value between all subscores of the BRB-N and Δ6MWT, of which an overview is displayed in Table 3. In addition, visual representations of these analyses are provided in Figure 2A to E. Attention as quantified by the PASAT 2” score showed a weak but significant correlation with Δ6MWT (r = 0.16, P = .013).
Correlation table.
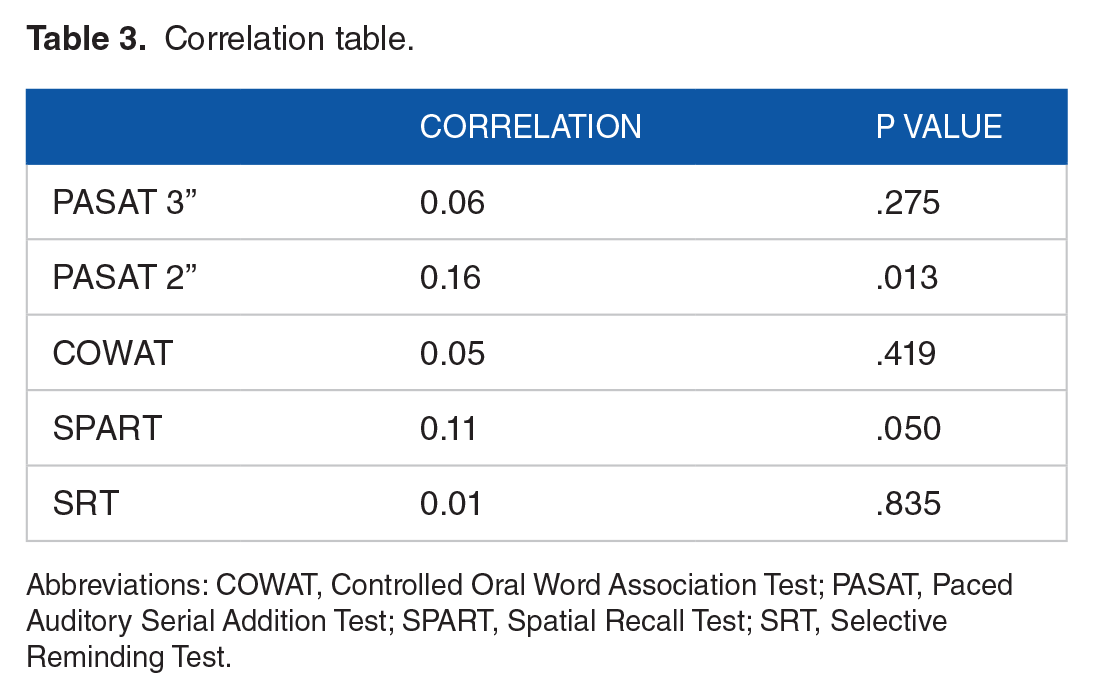
Abbreviations: COWAT, Controlled Oral Word Association Test; PASAT, Paced Auditory Serial Addition Test; SPART, Spatial Recall Test; SRT, Selective Reminding Test.
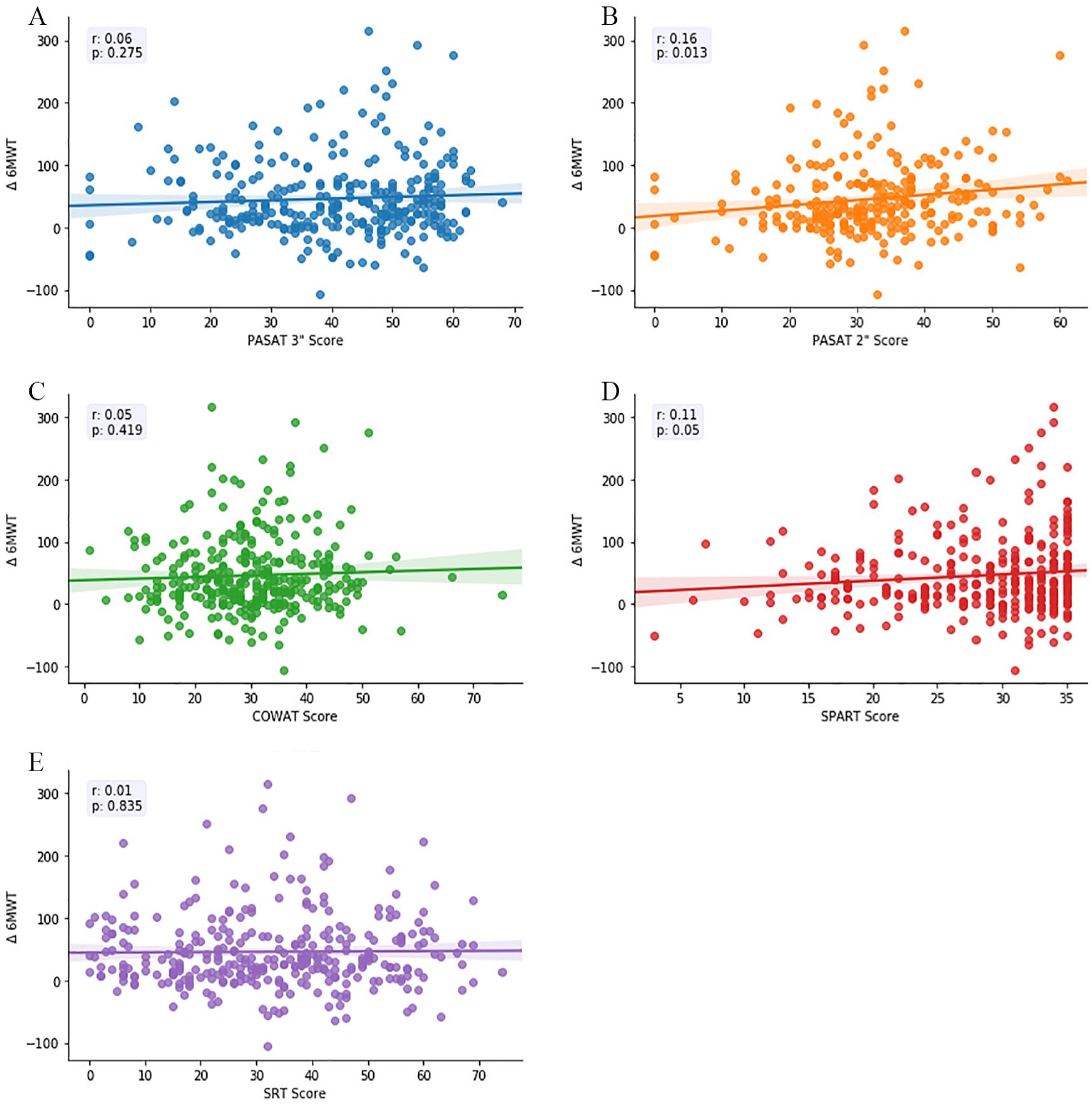
Scatterplots of Δ6MWT (y-axis) and BRB-N subscores (x-axis). Each plot contains a regression line and statistics box (left upper corner), containing Pearson correlation (r) and its related P value: (A) PASAT 3”, (B) PASAT 2”, (C) COWAT, (D) SPART, (E) SRT.
Discussion
We present the first study exploring the impact of cognitive function on the efficacy of locomotor rehabilitation in PwMS. This intervention yielded a significant improvement on walking ability, as reflected by ameliorated 6MWT results, in relatively large cohorts of both cognitively preserved and impaired subjects recruited at the NMSC Melsbroek. Our findings suggest that cognitive status does not affect locomotor rehabilitation potential, and cognitively impaired patients with MS therefore seem to be equally fit to achieve significant and clinically relevant physical improvements as their cognitively preserved counterparts. However, we found attention to be weakly correlated with Δ6MWT. This leads us to hypothesize that patients with higher attentional capacity might be more capable to pay sufficient attention to therapist instructions during rehabilitation.
In our main analysis, the cutoff criterion of 2 or less on the BRB-N, which has been proposed by Rao et al, 16 is commonly used in the MS literature. 17 It shows excellent sensitivity and specificity for cognitive deterioration in MS compared with an elaborate screening battery with 31 cognitive parameters. 16 Furthermore, this cutoff criterion of 2 or less on the BRB-N was shown to be predictive for impact on social functioning and employment. 22 However, dichotomization of cognitive impairment might be considered a coarse approach, as it ignores the multidimensional aspects of cognitive impairment. For example, if a patient scores below the 5th percentile on the SRT, but scores in the normal range on the other 3 BRB-N tests, the patient might be categorized as being cognitively preserved, while in fact they might experience severe cognitive problems potentially negatively influencing health outcomes.
In our second analysis, we therefore avoided classification by correlating Δ6MWT with individual test results assessing specific cognitive domains. Our results reflect that the impact of cognitive dysfunction might be more subtle, because we found that only attention (PASAT 2”) was related to the extent of locomotor yields.
Preserved cognition was shown to positively affect walking test performance in transcatheter aortic valve implantation (TAVI) 6 and lower limb amputation (LLA). 5 These studies also used a multidomain cognitive assessment to draw conclusions regarding locomotor rehabilitation but reported a different impact compared with our first analysis. This discrepancy could potentially be explained by the fact that measures of cognitive function varied across the respective studies, because the Montreal Cognitive Assessment (MoCA) 23 was used in the TAVI subjects and the Mini-Mental State Examination (MMSE) 24 in those with LLA. BRB-N is more sensitive to detect mild cognitive impairment compared with MMSE in MS, 25 while the latter might better reflect a person’s generalized cognitive performance. The COG– group in their analyses might thus be more impaired than our COG– group. Moreover, MoCA assesses executive functioning as part of the total cognitive screening, whereas BRB-N does not. 23 We might therefore hypothesize that executive dysfunction is associated with reduction in locomotor rehabilitation potential. We recommend future research to also investigate its domain-specific impact.
There are limitations to our study. First, the COG+ and COG– groups were not matched for education level, shown by a significantly higher amount of years of eduction in the COG+ group compared with the COG– group. Furthermore, large cohorts were retrieved based on a rigorous selection procedure but patients with MS can be admitted to the NMSC Melsbroek for various reasons, e.g. disease exacerbation and adjustment of pharmacological therapy. This heterogeneity may insert rehabilitation potential bias in our results. Another caveat might be that the administered interventions and baseline/discharge testing are not necessarily conducted by the same physical therapist and thus prone to interindividual variability. Finally, definite conclusions may be precluded by its retrospective design.
Conclusion
Cognitive impairment in MS, as assessed by the BRB-N, did not affect locomotor outcome during multidisciplinary inpatient rehabilitation in a specialized MS center. However, attention was weakly but significantly correlated with locomotor improvement, indicating a possible subtle effect of cognition on locomotor rehabilitation potential.
Author Contributions
Study concept was developed by SD, JVS and GN. All authors contributed to the progress of the study. LV, BG, and TM ensured quality of intervention and data entry by members of the multidisciplinary team. AVR collected data from the EDMUS database. SD and ADC structured and analyzed data. MD and MBD provided methodological feedback. SD wrote the original paper draft and all authors reviewed subsequent drafts.
Footnotes
Funding:
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: S.D. is supported by an unrestricted grant to G.N. by Roche Belgium. J.V.S. is supported by a post-doc scholarship by Flanders Research Foundation (FWO, ![]() ) (12I1817N). GN is a senior clinical research fellow at the Flanders Research Foundation (FWO, www.fwo.be) (1805620N).
) (12I1817N). GN is a senior clinical research fellow at the Flanders Research Foundation (FWO, www.fwo.be) (1805620N).
Declaration of conflicting interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.