
Abstract
We aimed to evaluate mortality and causes of death among Argentinean neuromyelitis optica spectrum disorder (NMOSD) patients and identify predictors of death. Retrospective study included 158 NMOSD patients and 11 (7%) patients died after 11 years of follow-up for a total exposure time of 53,345 days with an overall incidence density of 2.06 × 10.000 patients/day (95% CI 1.75–2.68). Extensive cervical myelitis with respiratory failure (45%) was the most frequent cause of death. Older age (HR = 2.05, p = 0.002) and higher disability score (HR = 2.30, p < 0.001) at disease onset were independent predictors of death. We found an 11-year mortality rate of 7% in Argentinean NMOSD patients.
Introduction
Neuromyelitis optica spectrum disorder (NMOSD) is a rare neuroinflammatory and severe disabling disease, affecting particularly optic nerves, spinal cord, and the brain/brainstem.1,2 Disability in NMOSD patients accumulates with each attack.1,2 Observational studies have reported varying NMOSD mortality worldwide depending on many factors such as ethnicity, age, relapse rate, recovery from attacks, type and location of lesions, among others.3–9 NMOSD mortality may be high and the estimated mortality rate in different cohorts was 15–32%.3–5 However, recent estimates allowed establishing a lower mortality rate (3.3–7%),6–9 probably based on an earlier diagnosis and aggressive treatment. 2 NMOSD mortality data in Argentina and in the region is lacking. Therefore, we aimed to evaluate the mortality rate and causes among Argentinean NMOSD patients and independent predictors of death.
Demographic, clinical, and paraclinical characteristics and treatments of included cohorts.

AQP4-Ab: aquaporin-4 antibody; NMOSD: neuromyelitis optica spectrum disorder; ON: optic neuritis; TM: transverse myelitis; CBA: cell-based assay; IIF: tissue-based indirect immunofluorescence; AZA: azathioprine; MMF: mycophenolate mofetil; RTX: rituximab; n: number; SD: standard deviation.
Predictors of death in NMOSD patients according to univariate and multivariable Cox proportional hazards models.
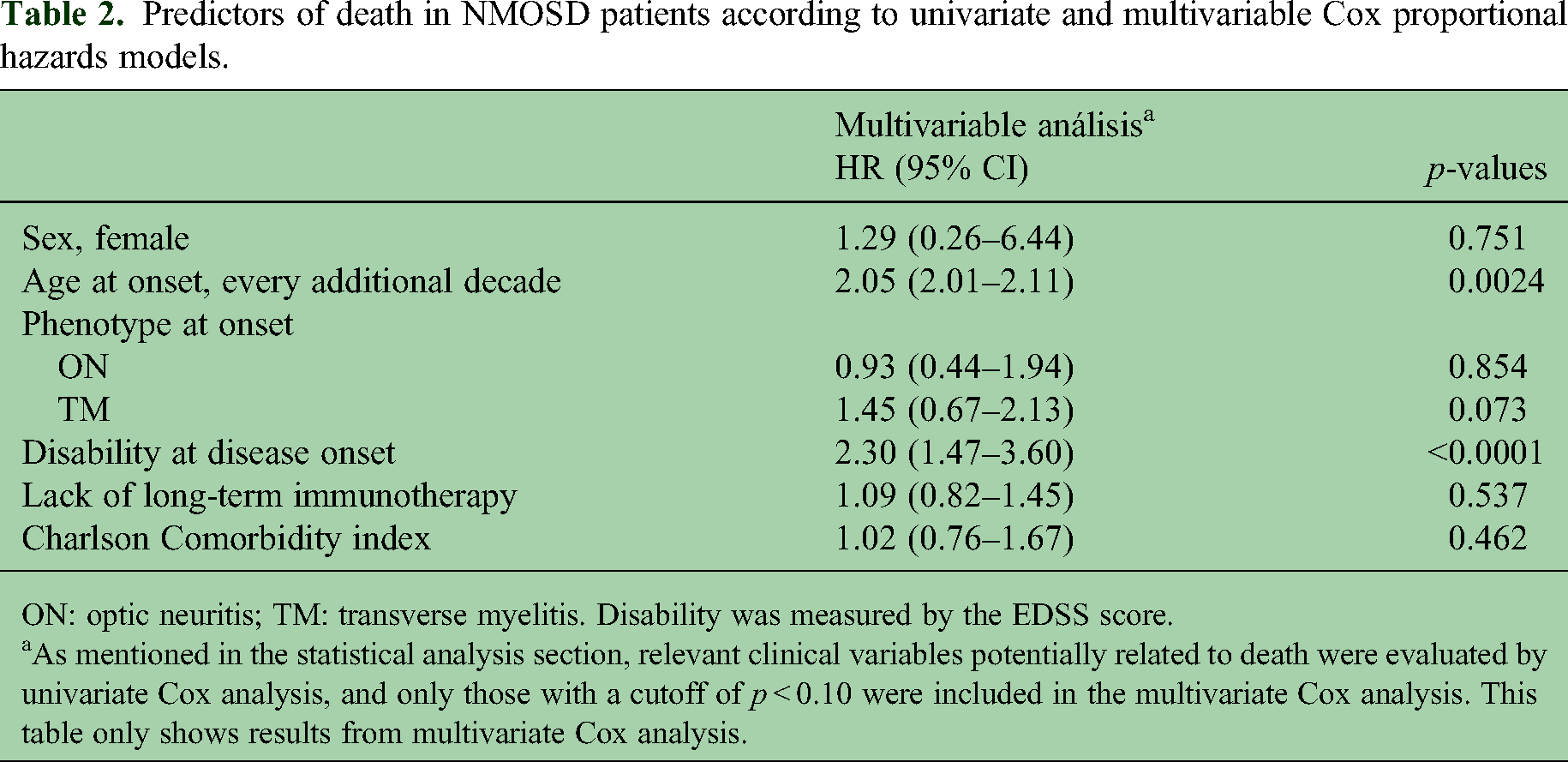
ON: optic neuritis; TM: transverse myelitis. Disability was measured by the EDSS score.
As mentioned in the statistical analysis section, relevant clinical variables potentially related to death were evaluated by univariate Cox analysis, and only those with a cutoff of p < 0.10 were included in the multivariate Cox analysis. This table only shows results from multivariate Cox analysis.
Methods
We conducted a retrospective study with a mean 11-year follow-up in a cohort of NMOSD patients followed in specialized centers from Argentina and enrolled in RelevarEM (from January 2005 to December 2022), a nationwide, non-mandatory, longitudinal, and observational registry of NMOSD patients (https://www.latambase.com.ar/login). 10 RelevarEM procedures and methods have been previously published elsewhere. 10 NMOSD was defined by the 2015 NMOSD diagnostic criteria. 2 Data on demographic factors, clinical (including Charlson Comorbidity index), paraclinical, and long-term immunosuppressant treatment (IST) strategies, including the cause of death during the follow-up period were confirmed by site researchers. 10 The clinical data of included patients were collected and followed every 6 months. These data were evaluated retrospectively and patients with insufficient or missing data were excluded (n = 15). Aquaporin-4 antibody (AQP4-Ab) status was determined in each participating center by cell-based assay (CBA) in 65.2% of patients, followed by tissue-based indirect immunofluorescence in 34.8%.1,2 Myelin oligodendrocyte glycoprotein (MOG)-antibodies were tested in all AQP4-Ab-negative patients using CBA in all cases and negative results were found.1,2
Statistical analysis
Categorical data were presented as count (proportion); continuous data were presented as mean ± standard deviation (SD). Cumulative incidence of death was reported for the whole cohort as well as incidence density (which is expressed per 10,000 patients/day with 95% confidence intervals [CIs]). Sub-analysis of the incidence of death by serostatus was also done expressed per 10,000 patients/day with 95% CI. Kaplan–Meier analysis was used to establish the survival curve of NMOSD patients and to calculate incidence density. Cox proportional hazard models were constructed to estimate the hazard ratios (HRs) for death and to identify independent risk factors for mortality in NMOSD patients. Relevant clinical variables potentially related to death were evaluated by univariate Cox analyses, and those with a cutoff of p < 0.10 were further included in the multivariate Cox analysis. HRs and 95% CIs were calculated to estimate the risks associated with predictors. Significance was set as p-value of <0.05 in the multivariate Cox regression analysis. Variables included in the models were age at disease onset, gender, and disability stratified by EDSS < 6 or ≥6. Statistical analyses were conducted using STATA software.
Results
We included 158 (72.8% female and 64.5% seropositive for AQP4-Ab) NMOSD patients (Table 1). A total of 11 (7%) patients died during follow-up for an exposure time of 53,345 days, with an overall incidence density of 2.06 per 10,000 patients/day (95% CI 1.75–2.68). We stratified the frequency by serostatus, and we observed eight cases in the AQP4-Ab positive group (exposure time 33,675 days) with an incidence density of 2.37 per 10,000 patients/day (95% CI 2.15–3.12), while three cases were observed in the AQP4-Ab negative (exposure time 1960 days) with an incidence density of 1.52 per 10,000 patients/day (95% CI 1.11–2.11). Median age at death was 61.1 ± 9 with a median disease duration of 6.8 ± 3.7 years. Extensive cervical myelitis with respiratory failure (45%) was the most frequent cause of death followed by respiratory infection (36%). The multivariate Cox analyses showed that older age at disease onset (HR = 2.05, 95% CI 2.00–2.11, p = 0.002, every increasing decade of onset age increased the risk of death 2.05 times) and higher disability score measured by EDSS at disease onset (HR = 2.30, 95% CI 1.47–3.60, p < 0.001) were independent predictors of death (Table 2).
Discussion
After a median 11-year follow-up, 11 (7%) of 158 Argentinean NMOSD patients in this cohort died. Almost half of deaths were related to NMOSD relapses, particularly extensive cervical myelitis with respiratory failure and respiratory infections were the second most frequent cause of death. Three-quarters of deceased patients experienced myelitis at onset with subsequent severe disability (median EDSS: 5) over time and their mean age at disease onset was more than 50 years. Importantly, we found that both higher age and disability score at disease onset were independent predictors of death in our model.
In this cohort, the overall mortality rate is in line with recent studies (3.3%–13%).4,6–9 Pre-AQP4-Ab studies have reported a 5-year mortality rate of 32% with a median survival of 17.5 years. 3 Most recently, mortality rate is estimated in approximately 25% of NMOSD patients with a disease duration of less than 10 years. 5 Consistent with other studies from the USA and Asia,3–7 extensive cervical myelitis with respiratory failure was the most common cause of death. Mealy et al. 7 reported that 70% of deaths were preceded by an attack in the brainstem and/or upper cervical spinal cord within the previous 1 year despite long-term IST in 80% of patients at the time of the fatal attack, in line with our results where 100% of patients were on long-term IST at time of the deceased. However, in a recent study, the most frequent cause of death was secondary infections, 6 which was the second cause of death in our cohort (respiratory infection: 36.4%).
The median survival time from disease onset to death has been reported between 6.9 and 17.5 years,3–5 in line with our results (median of 6.8 ± 3.7 years). However, a Chinese study reported a median of 3.4 years. 6 The authors hypothesized that the median age at onset of the deceased NMOSD patients was older (53.3 years old) than in other studies (23.5–45.4 years). Nevertheless, in the present study, the median age of the deceased NMOSD patients was 61.1 years. This difference may be explained because 62.5% of deceased NMOSD patients were without any long-term IST compared to 100% in our cohort. Notably, older age was a predictor of death in our study, consistent with previous studies.3–7 Thus, early NMOSD diagnosis associated with timely use of aggressive treatments are expected to improve the overall mortality rate in these patients. 2
African descendant ethnicity has been associated with a greater mortality rate. 7 However, in this cohort there were no patients of African descent, as this ethnicity is extremely rare in Argentina.
The retrospective design of this study is a limitation as well as the used assays in some patients, and findings should be interpreted with caution. However, these results reflect real-world evidence of everyday clinical practice.
In conclusion, this study showed that the overall cumulative incidence for the observed period was 7% with an overall incidence density of 2.06 × 10,000 patients/day. Older age and higher disability score at disease onset were independent predictors of death. Future prospective studies are needed in this region to corroborate our findings.
Footnotes
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.