
Abstract
Background
Computerized training in persons with multiple sclerosis (PwMS) seems to enhance working memory (WM)/information processing (IP), but factors associated with the efficacy of the treatment have not been sufficiently explored. Objective: To identify clinical and radiological characteristics associated with positive WM/IP training responses.
Methods
Radiological and neuropsychological assessments were carried out on a sample of 35 PwMs who were divided into “WM/IP-impaired” and “WM/IP-preserved.” All participants underwent adaptive n-back training for 10 days and were assessed post-training. Between-group differences (“WM/IP-impaired” vs. “WM/IP-preserved”) in training-induced cognitive improvement were assessed and exploratory correlational/ regression-based methods were employed to assess the relationship between cognitive improvement and clinical and radiological variables.
Results
All PwMS exhibited WM/IP benefits after training, but those with preserved WM/IP functions showed greater positive effects as well as transfer effects to other WM/IP tests when compared to the impaired group. Additional analyses revealed that positive response to treatment was associated with WM/IP baseline capabilities and greater gray matter volume (GMVOL) in relevant areas such as the thalamus.
Conclusions
Restorative cognitive training is suitable to improve cognition in PwMS but its effective outcome differs depending on the baseline WM/IP capabilities and GMVOL.
Keywords
Introduction
Neuropsychological deficits are common in persons with multiple sclerosis (PwMS) and have been shown to negatively affect various aspects of cognitive functions, with a prevalence of working memory (WM) dysfunctions and slow information processing (IP). 1
There is positive evidence in favor of some restorative techniques to improve WM/IP efficiency. In this regard, different studies using computerized n-back training have reported enhancements in the trained task,2,3 with some studies even further describing positive near transfer effects to another test that assesses WM/IP.4–7 In a previous study conducted in our laboratory, 8 we observed a general improvement in the execution of the 2- and 3-back tasks in a sample of PwMS with different cognitive statuses after undergoing an n-back training. 8 Some of the participants (but not all), were able to transfer this optimization to other tests that measure WM/IP such as the Paced Auditory Serial Addition Test (PASAT), the Symbol Digit Modalities Test (SDMT), and the Letters and Numbers Sequencing Test (LNST).
One of the main goals of making further progress in the field of cognitive rehabilitation in PwMS is not only to detect the most appropriate cognitive treatments, but also to identify the clinical conditions associated with the disease which are capable of predicting the effectiveness of such treatments. Considering the results previously observed in our laboratory, 8 the main aim of this study was to explore the influence of clinical and radiological variables on predicting the positive effects of WM/IP training in a sample of PwMS with different cognitive statuses. Based on the results of previous studies,9–12 we specifically hypothesized that PwMS with preserved WM/IP abilities and/ or less gray matter atrophy in brain areas sustaining WM would benefit more from this training program.
Materials and methods
Ethics committee approval
All PwMS provided their written informed consent to participate in this study, according to the Declaration of Helsinki, and were awarded €250 for their participation. The study was also approved by the Ethics Committee of the Universitat Jaume I (UJI) and was registered in the ClinicalTrials.gov registry as NCT05270239.
Participants
The sample was composed of a group of 35 PwMS diagnosed according to the revised McDonald criteria, 13 without any depression- or anxiety-related diagnosis, and free of exacerbation or steroid treatment in the 3 months prior to enrollment of the study (for a more detailed description of the inclusion and exclusion criteria see Esbrí et al. 8 ). Of this sample, 25 patients were classified as relapsing-remitting, 5 as having a secondary progressive form, and 5 as primary progressive. All participants were under disease-modifying pharmacotherapy (but none of them was under corticosteroid treatment or other medications that could interfere with cognition).
Neuropsychological assessment
As described in Esbrí et al., 8 PwMS were neuropsychologically assessed before (D1) and after the n-back training (D10) using the Spanish version of the Brief Repeatable Battery of Neuropsychological Tests (BRB-N). 14 To explore possible effects of baseline cognitive performance on the effectiveness of training, normative data were used to transform individuals’ pre-training scores in the BRB-N tests into their Z scores for verbal memory (ZV), visual memory (ZvI), WM/IP (ZWM/IP), and fluency (ZF) as described in Sepulcre et al. 14 Because our training program and main hypotheses focused on WM/IP capabilities, the ZWM/IP scores were employed to split the original sample into the two groups of main interest for the present study: “WM/IP-impaired” (those individuals exhibiting ZWM/IP scores equal to or smaller than −1.5) and “WM/IP-preserved” (individuals exhibiting ZWM/IP scores higher than −1.5). Yet, we also split our sample according to other relevant variables and assessed to which extent they account for the observed training-induced WM/IP improvements.
The neuropsychological assessment also included the LNST as another measure of WM and the Matrix Reasoning subtest to assess the intelligence quotient (IQ), both of them in the WAIS III 15 ; the Modified Fatigue Impact Scale (MFIS) derived from the original Fatigue Impact Scale 16 ; and the Spanish version of the Beck Depression Inventory (BDI-II). 17
N-back training protocol
The adaptive and intensive n-back training protocol (described in the Supplementary Material and study by Esbrí et al. 8 ) consisted of 10 sessions, with a total duration of 60 min/per session. Within each session, participants first completed three practice runs, each composed of eight blocks that varied the WM load (1-back, 2-back, and 3-back) according to the participant's performance. Thereafter, four 2-back blocks and four 3-back blocks were randomly displayed. The number of correct responses (CRs) was registered and used to calculate the 2- and 3-back net scores (CR-false positives). Reaction times (RT) were also recorded, but given that they were less consistently improved after training (see Esbrí et al. 8 ) and that, as in other studies, 18 we observed dissociated improvements of RT and WM scores, the present study focuses on CR-related improvements (whereas RT-related analyses are reported in the supplementary material).
Two complementary individualized improvement indexes were calculated to assess the effects of the n-back training on WM/IP capabilities: the net score improvement (NSI) index and the percent of maximum possible individualized (PMPI) improvement. The NSI was calculated as the raw difference between the post-training (D10) and pre-training (D1) net scores. This improvement index was also calculated for non-trained WM/IP tasks (PASAT, SDMT, and LNST). The PMPI can only be calculated for tasks having a reachable maximum score (i.e., the 2- and 3-back tasks) and is therefore calculated with the formula: 100*{(D10 net score-D1 net score)/(max net score-D1 net score)} (see Esbrí et al. 8 for further details).
Magnetic resonance imaging (MRI) acquisition
Anatomical 3D MPRAGE volumes were acquired in all participants with a 3 T (General Electric Medical System) using a T1-weighted gradient echo pulse sequence (TR = 2200 ms; TE = 3 ms; flip angle = 15; matrix = 256 × 256 × 160; voxel = 1 × 1 × 1 mm) and a FLAIR sequence to evaluate white matter lesions (TR = 6000 ms; TE = 354 ms; flip angle = 180; matrix = 196 × 256 × 160; voxel = 1.05 × 1.05 × 1 mm).
MRI preprocessing
Regarding the MRI data of PwMS, the lesion Segmentation Tool toolbox (https://www.applied-statistics.de/lst.html) was used via Statistical Parametric Mapping software (SPM12) to segment T2 hyperintense lesions in FLAIR images by implementing a lesion growth algorithm (LGA) described in Schmidt et al. 19 The obtained lesion probability maps were used to develop the subsequent preprocessing images obtained for PwMS.
MRI data from 35 healthy controls (HC) previously acquired in our laboratory with the same MRI protocol were aggregated to examine between-group differences in gray matter volume (GMVOL). These participants were selected to not significantly differ from our PwMS sample regarding gender, age, educational level, and total intracranial volume.
All the MRI data (HC and PwMS) were preprocessed with CAT12 included in the SPM12, following the standard procedure including: (1) normalization and segmentation of the images into gray matter, white matter, and cerebrospinal fluid; (2) data quality check after preprocessing by analyzing the sample homogeneity using covariance; and (3) smoothing using an 8-mm FWHM Gaussian kernel. Finally, the Automated Anatomical Labeling (AAL3 https://www.oxcns.org/aal3.html) was used to obtain the parcellation of GM regions of interest (ROIs) for each participant.
Statistical analyses
All statistical analyses were conducted in R (R Development Core Team, 2019) using robust methods 20 in 5000 bootstrapped samples and all data were FDR-corrected at a significance level of 0.05.
Median comparisons between WM/IP-impaired and WM/IP-preserved PwMS in demographic, clinical, radiological, and cognitive (including WM/IP improvement indexes) variables were conducted with the qcomhd function of the WRS2 package, 21 which provides a robust analogous of the Student's t-test. The non-standardized bootstrap estimate of the medians’ difference (and their 95% confidence intervals) served to quantify the effect size.
The robust Spearman's correlation index was employed to build up the network of relationships between each training-induced WM/IP improvement index and all the variables with significant differences between WM/IP-impaired and WM/IP-preserved PwMS. The results of this correlational analysis provided the departing hypotheses for a series of exploratory, robust, regression-based mediation analyses assessing whether pre-training WM/IP capabilities mediate the possible effects of these other variables on training-induced WM/IP improvement indexes. These analyses were carried out with the robmed package. 22 The mediated proportion was employed to quantify the effect sizes.
To assess the expected loss of local GMVOL in PwMS, the amount of GMVOL in the brain areas defined by the AAL3 atlas was compared between WM/IP-impaired, WM/IP-preserved, and HC using the med1way (which provides an ANOVA-like omnibus test) and the medpb (which provides dyadic post hoc median comparisons) functions of the WRS2 package.
To assess the predictive value of local GMVOL for training-induced WM/IP improvements in PwMS and whether these relationships were direct or mediated by their pre-training WM/IP capabilities, exploratory mediation analyses were conducted again.
Results
Demographic, clinical, cognitive, and conventional radiological variables in WM/IP-preserved and WM/IP-impaired PwMS and their relationship with training-improving effects
As shown in Table 1, the WM/IP-preserved and WM/IP-impaired groups did not significantly differ in terms of gender, age, educational level, disease evolution years, fatigue, depressive symptoms, or total lesion volume. Conversely, WM/IP-impaired PwMS were more physically impaired (EDDS scores, p = 0.005), and exhibited lower Brain Parenchymal Fraction (BPF) values (p = 0.003) than WM/IP-preserved PwMS. At the cognitive level, besides their differences in ZWM/IP, WM/IP-impaired had lower IQ (p = 0.003), Zvi (p = 0.003) but did not significantly differ from WM/IP-preserved PwMS regarding verbal memory (Zv) or fluency Z scores (ZF).
Comparison between WM/IP-preserved and WM/IP-impaired PwMS in demographic, clinical, radiological, and cognitive variables before starting their cognitive training program.

Data are reported as the sample medians and interquartile range (between brackets), except in the case of gender (for which the percentage of females is provided). The estimated median difference in 5000 bootstrap samples and its 95%CI (between brackets) are reported in the third column. Uncorrected and FDR-adjusted p-values are reported in the fourth and fifth columns, respectively. EDSS, Expanded Disability Status Scale; MFIS, Modified Fatigue Impact Scale; BDI, Beck Depression Inventory-II; BPF, Brain Parenchymal Fraction; IQ, Intellectual Quotient; BRB-N, Brief Repeatable Battery of Neuropsychological Tests; ZV, verbal memory z-score; Zvi, visual memory z-score; ZWM/IP, working memory/ information processing z-score; ZF, fluency z-score.
Focusing on WM/IP, the WM/IP-impaired group did not only exhibit lower pre-training scores than the WM/IP-preserved group in the PASAT and SDMT but also in the LNST and in the 2-back and 3-back tasks (Table 2). Of higher interest for the goals of the present study, both groups of PwMS significantly enhanced their 2- and 3-back performance after repeated n-back training but WM/IP-impaired benefitted less from this cognitive training program (Figure 1). Thus, although due to a ceiling effect in the 2-back task (Table 2; see also Esbrí et al. 8 ), these two groups of PwMS did not significantly differ in their 2-back-NSI and 2-back-PMPI scores, WM/IP-impaired exhibited significantly lower 3-back-NSI (p = 0.031) and 3-back-PMPI (p < 0.001) scores than WM/IP-preserved. Moreover, near transfer effects to untrained WM/IP tasks were solely observed in the WM/IP-preserved. In fact, the NSI scores of the WM/IP-preserved group in the PASAT, SDMT, and LNST were not only significantly larger than those of the WM/IP-impaired group (p = 0.003, p = 0.001, and p = 0.045, respectively), they were also the only ones significantly different from zero (WM/IP-preserved, p < 0.001 in all cases; WM/IP-impaired, 0.380, 0.369, and 0.882, respectively). Therefore, it can be concluded that not only do WM/IP-preserved PwMS have higher pre-training WM/IP capabilities but they can also benefit more from a relatively short WM/IP training, obtaining higher post-training 2- and 3-back scores (Table 2) and significantly improving their performance in other untrained WM/IP tasks.

Training-induced improvement in WM/IP tasks in the WM/IP-preserved and WM/IP-impaired groups. Panels depict the distributions (boxplots) of the individual improvement scores observed in the WM/IP-preserved and WM/IP-impaired groups in the 2-back, 3-back, PASAT, SDMT, and LNST tasks. The estimated median values in 5000 bootstrap samples and the FDR-corrected p-values of the group-based median comparisons are reported within the boxes and at the top of each panel, respectively. Note that for those tasks with a reachable upper bound (the 2-back and 3-back tasks) two indices of improvement were calculated, the net score increase (NSI) and the percent of the maximum possible individual increase (PMPI, see the formula in the Methods section). At the bottom of each panel, the FDR-corrected p-values corresponding to comparisons testing whether each group's median improvement was significantly different from zero are also reported.
Comparison between WM/IP-preserved and WM/IP-impaired PwMS in different wm/ip tasks before and after training.
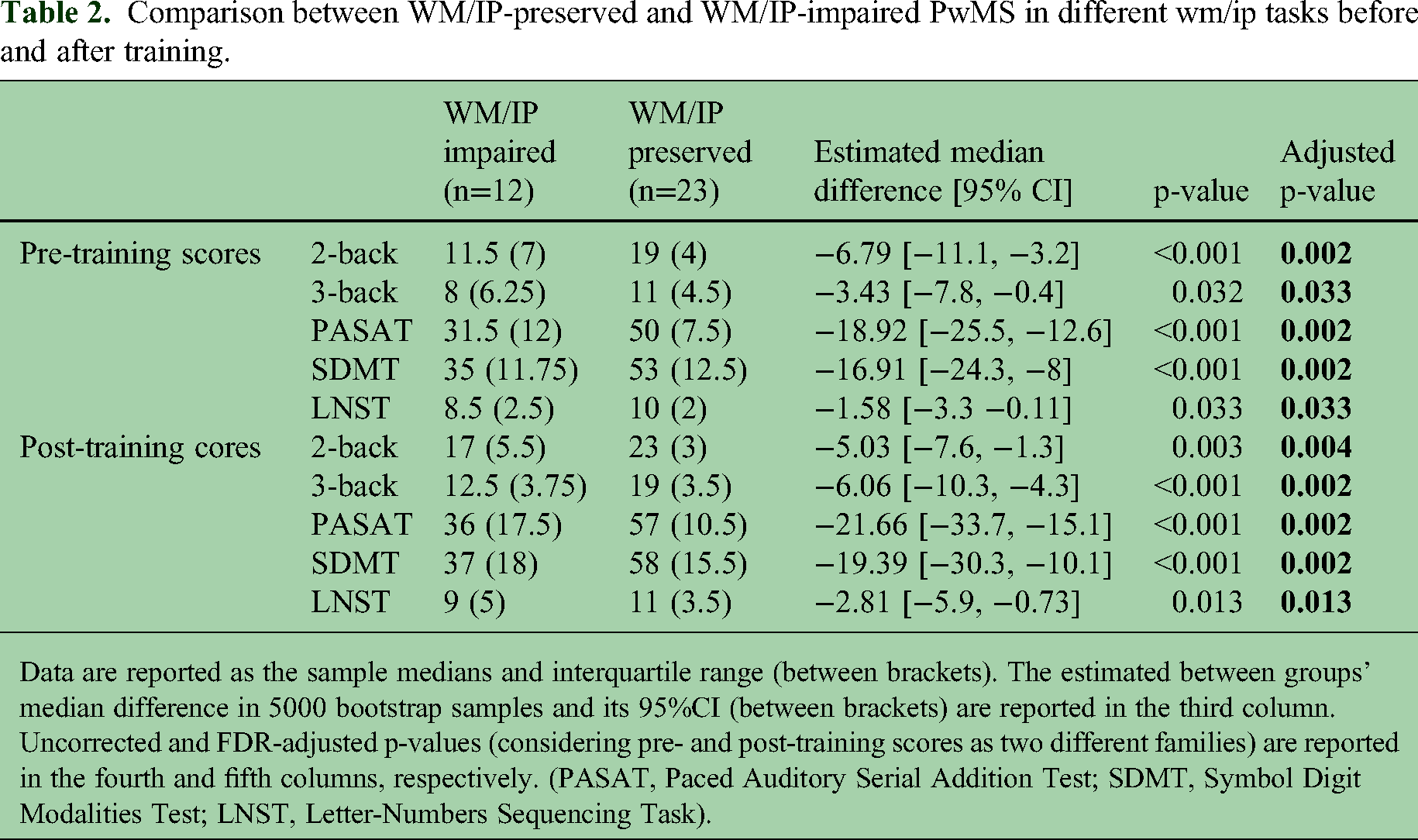
Data are reported as the sample medians and interquartile range (between brackets). The estimated between groups’ median difference in 5000 bootstrap samples and its 95%CI (between brackets) are reported in the third column. Uncorrected and FDR-adjusted p-values (considering pre- and post-training scores as two different families) are reported in the fourth and fifth columns, respectively. (PASAT, Paced Auditory Serial Addition Test; SDMT, Symbol Digit Modalities Test; LNST, Letter-Numbers Sequencing Task).
The differential effects of training in WM/IP-preserved and WM/IP-impaired PwMS were more related to their different pre-training WM/IP capabilities than to other variables in which these two groups also differed (BPF, IQ, EDSS, and Zvi). In fact: (1) only pre-training ZWM/IP scores showed statistically significant correlations with all the WM/IP improvement indexes, except the 2-back-NSI (Figure 2 and Supplemental Table 1); (2) neither “Zvi-impaired/ Zvi-preserved” nor “high/low” BPF, IQ, or EDSS groups reproduces the consistent pattern of differences in WM/IP improvement indexes observed for the WM/IP-preserved and WM/IP-impaired groups (Supplemental Table 2); (3) exploratory mediation analyses revealed that the effects of Zvi and EDSS are completely mediated by pre-training ZWM/IP scores and that, most, but not all of the influence of BPF and IQ on training-induced WM/IP improvement seems to be mediated by pre-training ZWM/IP scores (Supplemental Table 3).

Correlation networks. (A)–(G) depicts the direct (green) and the inverse (red) Spearman's correlations between all the variables significantly differing between WM/IP-preserved and WM/IP-impaired groups (see Table 1). For simplicity, only those correlations remaining statistically significant after multiple comparisons’ correction are included (for the whole correlation matrix and associated p-values, see Supplemental Table 1).
Loss of GMVOL and its relationship with training-improving effects
To explore local brain atrophy in PwMS, the possible differences in GMVOL between WM/IP-preserved, WM/IP-impaired, and a matched control group (see Table 3) in the 166 anatomical regions defined by the AAL3 atlas were assessed. As summarized in Supplemental Figure 1 and Supplemental Table 3, statistically significant between-group differences indicative of atrophy were identified in 41 of the 166 brain regions evaluated (24.7% of total). WM/IP-preserved PwMS had significantly lower amounts of GMVOL than HC in 29 brain regions (Supplemental Figure 1A). WM/IP-impaired PwMS exhibited significantly lower amounts of GMVOL than HC in 41 brain regions (Supplemental Figure 1B). Significant differences between WM/IP-preserved and WM/IP-impaired were identified in 8 brain regions (Figure 3).

Differences between the HC, WM/IP-preserved, and WM/IP-impaired groups in local GMVOL. Panels depict the distributions (boxplots) of the individual GMVOL Z-scores observed in those brain areas in which post hoc comparisons revealed a statistically significant difference between WM/IP-preserved and WM/IP-impaired PwMS. The p-values of all post hoc comparisons are provided. Moreover, the between-median differences for those comparisons achieving statistical significance are also provided. Because GMVOL scores are standardized as robust and re-scaled z-scores (Wilcox 20 ), these median differences are expressed in standard deviation units and provide an effect size with the same scale and a similar interpretation as Cohen's d. l: left; r: right; ACCsub: anterior cingulate cortex subgenual; MCC: middle cingulate & paracingulate gyrus; PCFventmed: superior frontal gyrus and medial orbital; IFGob: inferior frontal gyrus pars orbitalis; INS: insula; PAL: lenticular nucleus; PoCG: postcentral gyrus; PUT: putamen.
Comparability of healthy controls (HC) and persons with multiple sclerosis (PwMS).

Data are reported as the sample medians and interquartile range (between brackets). The estimated median difference in 5000 bootstrap samples and its 95%CI (between brackets) are reported in the third column. Uncorrected p-values are reported in the fourth column. Because none of these comparisons yielded any significant effect, FDR adjustment is unnecessary and FDR-adjusted p-values are not reported.
Interestingly, most of the 41 brain areas in which atrophy was confirmed were predictive of training-induced improvements of PwMS performance in all WM/IP tasks except the 2-back task (Figure 4A and B, and Supplemental Table 4). The same exploratory mediation analyses also revealed that: (1) GMVOL loss in most brain areas (including those in which GMVOL differences between WM/IP-preserved and WM/IP-impaired had been confirmed; Figure 4C) primarily affected pre-training WM/IP capabilities and indirectly reduced training-improving effects and (2) GMVOL loss in other brain areas (i.e., thalamic) reduced training-improving effects directly or, more often, through a combination of direct and indirect effects (Figure 4D).
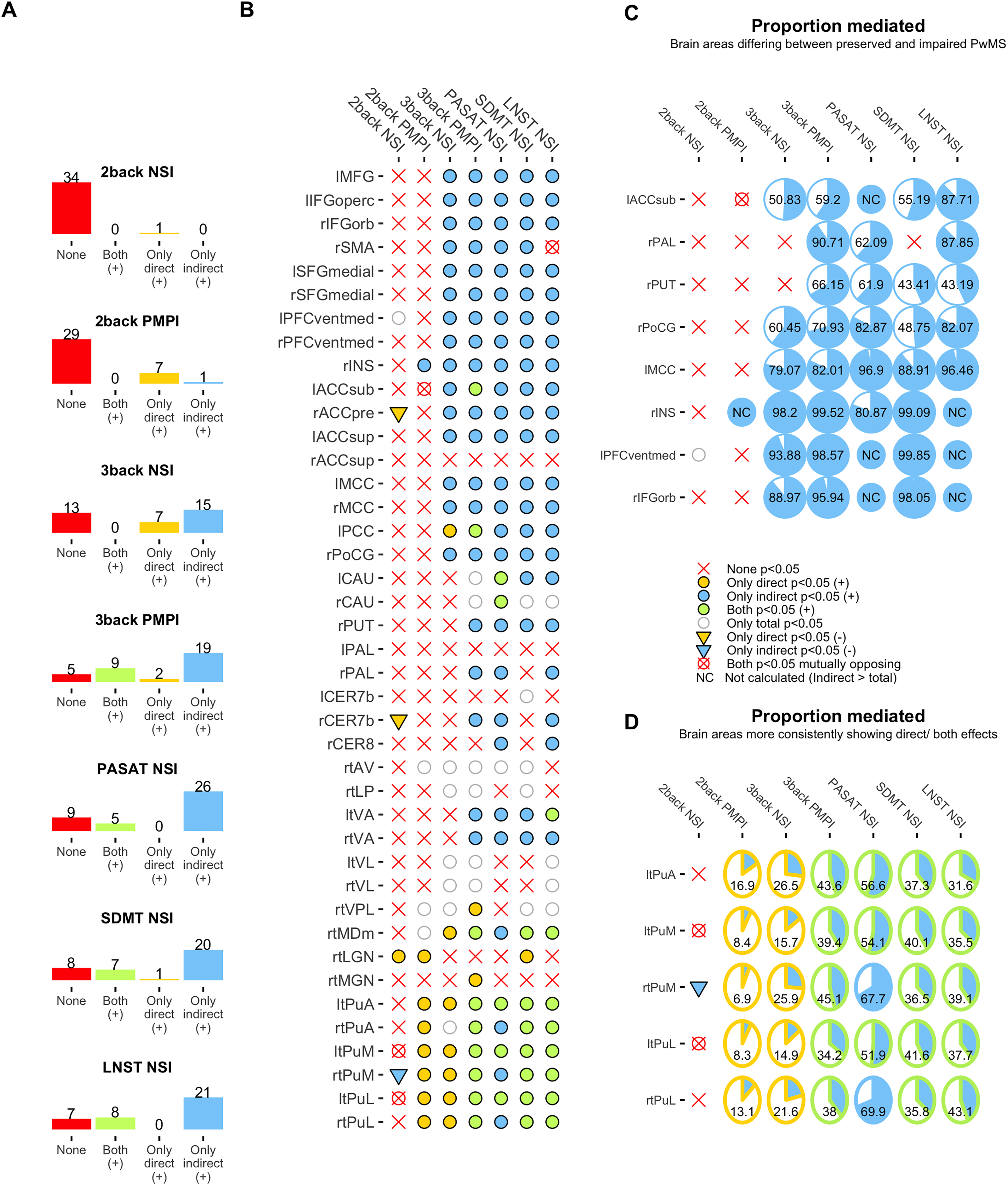
Direct and indirect (ZWM/ip-mediated) predictive value of local GMVOL for training-induced WM/IP improvements. Panel A summarizes the absolute frequencies of statistically significant direct and indirect effects (as well as of the cases in which both or none of these effects were significant) in a series of exploratory mediation analyses using the local amount of GMVOL in the 41 brain areas in which brain atrophy had been confirmed as predictors (see Supplemental Figure 1), pre-training WM/IP capabilities as the putative mediator, and the WM/IP improvement indexes in the 2-back, 3-back, PASAT, SDMT, and LNST tasks as outcomes. Note that this initial summary omits inverse (−) relationships as well as those cases in which only the total effect was statistically significant, so the number of counted effects varies for each outcome and it does not add to 41. These other effects can be found in Panel B, which provides a more detailed (area-by-area) account of the mediation analyses and describes the effects’ direction (for the whole statistical output, see Supplemental Table 5). Panel C depicts the proportion mediated in those brain areas in which statistically significant differences between WM/IP-preserved and WM/IP-impaired had previously been observed (Figure 4). Panel D illustrates the proportion mediated in the brain areas more consistently showing direct or direct and indirect effects. l: left; r: right; ACCsup: anterior cingulate gyrus supracallosal; ACCpre: anterior cingulate gyrus pregenual; ACCsub: anterior cingulate gyrus subgenual; PuL: pulvinar lateral; PuM: pulvinar medial; PuA: pulvinar anterior; tMGN: thalamus medial geniculate nucleus; tLGN: thalamus lateral geniculate nucleus; tMDm: thalamus mediodorsal medial magnocellular; tVPL: thalamus ventral posterolateral; tVL: thalamus ventral lateral; tVA: thalamus ventral anterior; tLP: thalamus ventral lateral; tVA: thalamus ventral anterior; tLP: thalamus lateral posterior; tAV: thalamus anteroventral; CER8: lobule VIII cerebellum; CER 7b: lobule VIIb cerebellum; PAL: lenticular nucleus; PUT: lenticular nucleus putamen; CAU: caudate nucleus; PoCG: postcentral gyrus; PCC: posterior cingulate gyrus; MCC: middle cingulate and paracingulate gyrus; INS: insula; PFC ventmed: superior frontal gyrus medial orbital; SFG medial: superior frontal gyrus medial; SMA: supplementary motor area; IFGorb: inferior frontal gyrus pars orbitalis; IFG operc: inferior frontal gyrus opercular part; MFG: middle frontal gyrus.
Discussion
The results of this study suggest that pre-training WM/IP status is the main moderator of the positive effects of training. Although all PwMS showed improvements in WM/IP after training, these gains were more notable in the participants with WM/IP-preserved functions compared to patients with impaired WM/IP. These results are similar to previous studies which report that participants with initial higher WM ability obtain more benefits from WM training.10–12 Likewise, only WM/IP preserved showed near transfer effects to other tests designed to assess WM/IP functions such as PASAT and SDMT.
Preserved and impaired PwMS also differed in EDSS, IQ, and Zvi scores or BPF. Therefore, we used correlation and mediation analyses to determine the influence of these variables in training-induced WM/IP gains. Correlation results revealed that post-training gains (observed in 2 -PMPI-3 back -NSI- and -PMPI-) and other WM/IP tasks (PASAT, SDMT, and LNST-NSI scores in all cases) were directly and significantly associated with WM/IP baseline capabilities. We also noted that IQ scores were positively correlated with the 3-back gains and transfer effects observed in the PASAT and SDMT, although exploratory mediation analysis revealed that the effects of IQ were indirect and mostly mediated through baseline WM/IP capabilities. These findings are in line with previous studies wherein cognitive reserve has been linked with less cognitive impairment in PwMS, including WM/IP functions, and also with better performance on the n-back task.23,24
Brain atrophy is a relevant marker of the disease process in MS and cognitive impairment is strongly associated with a GMVOL reduction.25,26 In this regard, and as suggested by previous studies, the degree of atrophy can play an important role in the effectiveness of any cognitive therapy.27,28 Different results of this study emphasize the role that lower integrity of cerebral GM plays in the effectiveness of WM training. First, we observed differences in BPF between the two groups of patients; second, correlation analyses showed a positive association between BPF and baseline WM/IP status, but again, our exploratory mediation analyses revealed that BPF effects were indirect and mediated by the WM/IP pre-training baseline abilities. To better characterize the role of GMVOL integrity we decided to explore the distribution pattern of atrophy and its possible influence on training effects in more detail. As expected, the WM/IP impaired group presented less GMVOL when compared to those preserved in cortical frontal areas (including the superior medial and inferior and postcentral frontal gyrus), anterior and middle cingulate gyrus, insula, and subcortical areas as the putamen and the lenticular nucleus of the thalamus. It is worth noting that exploratory mediation analyses revealed the association between the amount of GMVOL in these brain areas and the effects of training to be largely indirect and dependent on the contribution of GMVOL preservation on pre-training WM/IP capabilities. This observation is in alignment with those of previous studies describing an association between the loss of GMVOL in these cortical and subcortical structures and the cognitive status of PwMS.26,29,30 To complement these findings, GM integrity in other brain areas (i.e., thalamic pulvinar nucleus) seems to be related to training-induced WM/IP gains in a more direct (i.e., largely independent of baseline WM/IP capabilities) manner. Thus, severe structural damage in the thalamus reduces the effectiveness of training. These results are not unexpected given that the atrophy of the thalamus has been associated with the evolution and severity of cognitive impairment in PwMS, including WM/IP functions.31–33
The results of this study indicate that all PwMS respond to the restorative WM training, but those with higher WM/IP baseline performance, who also have greater GMVOL in relevant areas (especially in the thalamus) obtain a greater benefit. Ideally, these studies should be conducted with larger samples to attain statistical power and uncover possible small-sized effects that could have gone unnoticed in the present study. This aspect might be especially important when aiming to detect direct effects in mediation analyses, as it is well known that tests for direct and total effects have less power than those for indirect effects. 34 Future work should study the clinical, radiological, and also methodological variables (total duration of the treatment/sessions per week, etc.) associated with the effectiveness of training to help clinicians offer the best treatment programs to PwMS.
Supplemental Material
sj-docx-1-mso-10.1177_20552173231196990 - Supplemental material for Pre-training working memory/information processing capabilities and brain atrophy limit the improving effects of cognitive training
Supplemental material, sj-docx-1-mso-10.1177_20552173231196990 for Pre-training working memory/information processing capabilities and brain atrophy limit the improving effects of cognitive training by Sónia Félix Esbrí, Alba Sebastián Tirado, Maria Zaragoza Mezquita, Carla Sanchis Segura and Cristina Forn in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
We appreciate the collaboration of the Associació Esclerosis Múltiple de Castelló (AEMC).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Universitat Jaume I, Ministerio Ciencia e innovación, (grant number PREDOC/2020/22, UJI B2020-02, MCI/AEI 10.13039/501100011033).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.