
Abstract
Background
We aimed to determine the proportion of highly active multiple sclerosis patients under high-efficacy therapies (HETs) achieve no evidence of disease activity-3 (NEDA-3) at 1 and 2 years, and to identify factors associated with failing to meet no evidence of disease activity 3 at 2 years.
Methods
This retrospective cohort study based on Argentina Multiple Sclerosis patient registry (RelevarEM), includes highly active multiple sclerosis patients who received HETs.
Results
In total, 254 (78.51%) achieved NEDA-3 at year 1 and 220 (68.12%) achieved NEDA-3 at year 2. Patients who achieved NEDA-3 at 2 years had a shorter duration of multiple sclerosis (p < 0.01) and a shorter time between first treatment and current treatment (p = 0.01). Early high-efficacy strategy patients reached NEDA-3 more frequently (p < 0.01). Being a naïve patient (odds ratio: 3.78, 95% confidence interval 1.50–9.86, p < 0.01) was an independent predictor to reach NEDA-3 at 2 years. No association was found between type of HETs and NEDA-3 at 2 years when adjusted for potential confounders (odds ratio: 1.73; 95% confidence interval 0.51–6.06, p 0.57).
Conclusion
We found a high proportion of patients who achieved NEDA-3 at 1 and 2 years. Early high-efficacy strategy patients had a higher probability of achieving NEDA-3 at 2 years.
Background
Multiple sclerosis (MS) is a chronic disease characterized by inflammatory lesions in the central nervous system. It is regarded as the most common cause of non-traumatic neurological disability in young adults. 1 Data has emerged which shows that both relapses and ongoing focal inflammatory activity on magnetic resonance imaging (MRI) are associated with a worse short- to intermediate-term prognosis. 2 Consequently, in clinical practice, the composite measure of the absence of relapses, confirmed disability progression, and MRI activity—known as “no evidence of disease activity”-3 (NEDA-3)—is increasingly used as the goal of treatment in MS. 3 Achieving the NEDA-3 status in the first 2 years of treatment has shown to hold 80%–90% positive predictive value for the absence of long-term disability accrual in the following years. 4 NEDA-3 is considered a useful strategy for targeting and monitoring treatment response in relapsing-remitting MS, especially when no other measures are available. Furthermore, NEDA-3 has become an important secondary outcome measure in clinical trials with the introduction of more effective types of disease-modifying therapy (DMT) for relapsing forms of the disease.4–6 The proportion of MS patients who maintain NEDA-3 over time may be variable and depend on baseline MS inflammatory activity and different factors associated with treatment, such as early treatment and effectiveness.
Even though there is no universally accepted definition of highly active MS (HAMS), it is considered that patients with HAMS will have frequent relapses and/or an increasing burden of brain MRI lesions. Other features include severity and localization of relapses, clinical or MRI disease activity under treatment, burden of T2 lesions and presence of gadolinium (Gd+) enhancing lesions. Additionally, patients with highly active MS often have factors associated with poor prognosis including ⩾1 spinal cord lesions, incomplete recovery from relapses, accrual of physical or cognitive impairment, and a short inter-attack interval. 7 The availability of more effective DMTs over recent years has increased the complexity of selecting an appropriate treatment for patients with MS. Monoclonal antibodies and cladribine (high-efficacy therapies, HETs) are the most widely used therapies for the treatment of highly active MS. Regarding therapeutic strategies, two treatment pathways were described depending on the early use or not of HETs.1,8
Although there are numerous studies addressing the effectiveness of HETs in real life, the evaluation of NEDA-3 in the subgroup of highly active MS patients has not been widely addressed. The primary aim of our study was to investigate the proportion of NEDA-3 at 1 and 2 years in a cohort of HAMS patients under clinical examinations every 6 months and yearly MRI. The secondary objectives were to evaluate the association between NEDA-3 and (A) therapeutic strategy, escalation strategy (ES) vs. early high efficacy (EHE) and (B) type of treatment (cladribine vs. monoclonal antibodies).
Method
Study population
This retrospective cohort study was done using the Argentina MS patient registry (RelevarEM), (Clinical Trials registry number NCTNCT03375177). 9 The database was recorded prospectively from 1 August 2018 but retrieved data retrospectively from the disease beginning of each included patient. Detailed information on the database and data collection has been previously published. 9 For this cohort study, the database lock occurred in April 2021. The inclusion criteria for this study were age ≥18 years at study inclusion, patients diagnosed with RRMS according to validated diagnostic criteria, 10 patients currently treated with natalizumab, alemtuzumab, cladribine, rituximab or ocrelizumab. Presence of at least 1 clinical relapse in the previous 12 months and at least 1 of the HAMS risk factors prior to the initiation of current HETs proposed by Sorensen et al. 7 Only patients with Expanded Disability Status Scale (EDSS) assessment every 6 months and yearly MRI were included. Patients with missing or incomplete information and patients with incomplete information precluding the determination of NEDA-3 were excluded.
Definitions and data collection
Data were obtained from the anonymized registry following all relevant local regulations. The following sociodemographic variables were collected from the registry: age, sex. Clinical variables: MS duration, MS phenotype, EDSS score at diagnosis and before starting HET, current and past DMTs. The NEDA-3 status was identified by the absence of the following parameters: clinical relapses, 6-month confirmed increase in EDSS score, and MRI activity at 12 or 24 months (NEDA at 1 year or 2 years, respectively). 11 A confirmed disability increase was defined as 1.5-point increase (if the baseline EDSS score was 0), 1.0-point increase (if the baseline EDSS score was <5.5), or 0.5-point increase (if the baseline EDSS score was ≥5.5) confirmed 6 months apart. 12 Clinical relapse was defined as any new neurological symptom not associated with fever or infection lasting for at least 24 h and accompanied by new neurologic signs or symptoms. 12 MRI activity included the presence of contrast-enhancing lesions and/or new or enlarging T2-hyperintense lesions on brain and/or spinal cord. 12 For NEDA-3 at year 1, we included all patients who had been on the drug for at least 12 months, including those with treatment interruption due to lack of efficacy. We did not include patients with treatment interruption due to side effects or pregnancy planning. For NEDA-3 at year 2, we included all patients who had been on the drug for at least 24 months, including those with treatment interruption due to lack of efficacy. We did not include patients with treatment interruption due to side effects or pregnancy planning. For cladribine and alemtuzumab, the evaluation after the end of the first treatment cycle was considered a baseline measure. After this assessment, NEDA-3 was evaluated at one year and at 2 years. Escalation strategy (ES) refers to the initiation of treatment in newly diagnosed patients with less effective but relatively safer agents, as opposed to EHE strategy, in which HETs are initiated early to control disease activity.1,8
To address the secondary objective (A), patients were categorized into ES or EHE according to the therapeutic strategy, based on previous research. Patients were classified as follows: EHE if they received natalizumab, ocrelizumab, rituximab, alemtuzumab or cladribine as initial treatment and ES if they received interferon β, glatiramer acetate, teriflunomide, dimethyl fumarate, or fingolimod as initial treatment. For this analysis, those patients who had received a HET prior to the current HET were eliminated (n = 31).
Statistical analysis
Data analysis was conducted using RStudio 2022.02. 0. 13 Descriptive analyses of all variables were conducted. Results were presented as frequencies, percentages, ranges, mean, and standard deviation values. Comparisons between the two groups were analyzed using Chi-square or Fisher's exact tests for categorical variables. Continuous variables were analyzed using Student t-test or Wilcoxon's tests as appropriate and analysis of variance (ANOVA) with Bonferroni post hoc comparisons or Kruskal–Wallis test with Dunn post hoc analysis was used to compare three or more groups.
Two binary logistic regression analysis models were performed: first, to assess the association between NEDA at 2 years (dependent variable) and therapeutic strategy (independent variable), and second, to evaluate the association between NEDA at 2 years (dependent variable) and the HET type (independent variable). In both models, the adjustment was made for clinical and demographic variables considered biologically important or possible confounders. The independent covariables were included as a continuous variable: age at diagnosis, age at HET, EDSS score at diagnosis, and before HET, number of relapses in 12 months pre-HETs, number of prior DMT, time to HET, time between first treatment and current treatment and dichotomous variables: sex, new brain MRI lesions (new T1-weighted gadolinium enhancement and newT2 lesions), type of HET (for the first model) and therapeutic strategy (for the second model). Those variables with p < 0.20 in the bivariate analysis or those variables that produce a confounding effect were introduced in the final model. For all analyses, p-values < 0.05 were considered statistically significant.
Results
Participants
Of the 3640 registered MS patients, 2450 RRMS patients were under a DMT and 462 (19%) were under HETs. Out of a total of 462 patients treated with HET, 323 (70%) met the inclusion criteria (Figure 1). Demographic characteristics of these patients are summarized in Table 1 and the presence of highly active MS risk factors prior to the initiation of current HETs

Study flowchart of patients’ disposition legend: RRMS: relapsing-remitting multiple sclerosis. HET: high efficacy therapies. HAMS: highly active multiple sclerosis. * The database was recorded prospectively from 1 August 2018 but retrieved data retrospectively from the disease beginning of each included patient for this cohort study, the database lock occurred in April 2021.
Baseline characteristics of the entire cohort.

HET: high-efficacy therapies; EDSS: Expanded Disability Status Scale; SD: standard deviation; EHE: Early high-efficacy; MRI: magnetic resonance imaging; DMT: disease-modifying therapy.
Outcomes
Of the patients included, 254 (78.51%) achieved NEDA-3 at year 1 and 220 (68.12%) achieved NEDA-3 at year 2. Regarding treatments, no significant differences were found to achieve NEDA-3 at year 2: natalizumab 70.2%, alemtuzumab 58.3%, cladribine 73.9%, ocrelizumab 70.6% and rituximab 66.7% (p 0.38). The sensitivity analysis showed that 85.82% of patients who received EHE treatment achieved NEDA-3 at year 1 and 83.21% at year 2 (Figure 2). The superior effect of patients receiving EHE treatment vs. patients with ES on NEDA-3 was highly significant at both year 1 (62.54% vs. 85.82%, p 0.02) and 2 (70.43 vs. 83.21%, p < 0.01). As shown in Table 2, no significant differences were found between patients who achieved NEDA-3 vs. patients with evidence of disease activity (EDA) in demographic characteristics or clinical history of the disease. Among patients receiving EHE treatment (EDA: 22.80%; NEDA-3: 48.40%, p < 0.01), those with shorter disease duration (EDA: 53.86%; NEDA-3: 52.25%, p = 0.01) and shorter time between first treatment and current treatment (EDA: 70.64%; NEDA-3: 55.65%, p < 0.01) achieved significantly more NEDA-3. The adjusted odds ratio (OR) of achieving NEDA-3 at year 2 in patients receiving EHE treatment was 5.58 (95% confidence interval (CI) 2.08–16.29, p < 0.01) compared to patients with ES. No association was found between NEDA-3 at 1 year and EHE. Besides, there was no association between the type of HET (monoclonal antibodies or cladribine) and NEDA-3 at 1 or 2 years (Table 3).

NEDA-3. Achieved NEDA at year 1: (a) in entire cohort (78.51%) and (b) EHE strategy (85.82%). Achieved NEDA at year 2: (c) in the entire cohort (68.12%), and (d) EHE (83.21%). EHE: early high efficacy; NEDA-3: no evidence of disease activity-3.
Demographic and clinical variables between NEDA-3 and EDA at 2 years (N = 292).
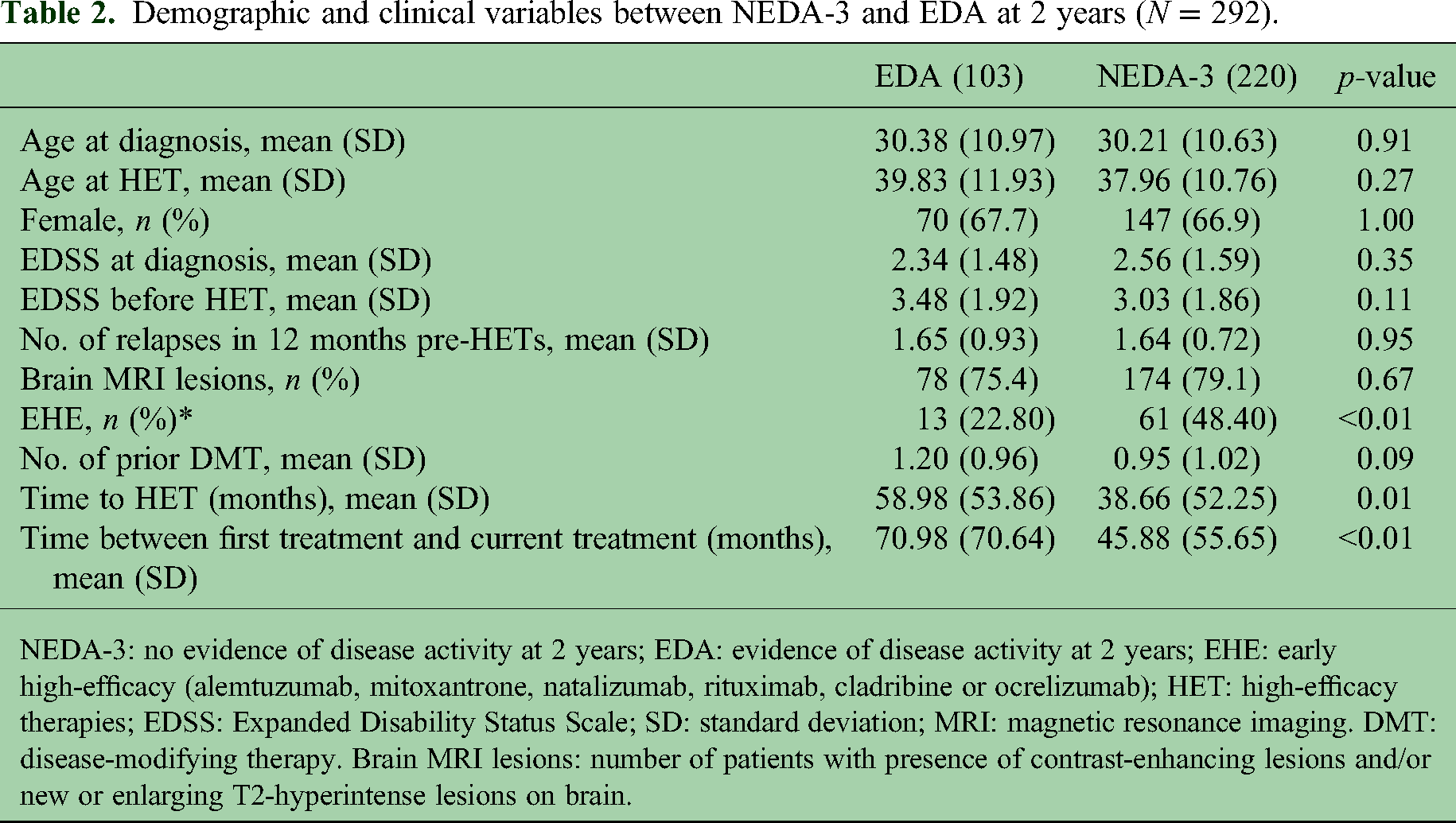
NEDA-3: no evidence of disease activity at 2 years; EDA: evidence of disease activity at 2 years; EHE: early high-efficacy (alemtuzumab, mitoxantrone, natalizumab, rituximab, cladribine or ocrelizumab); HET: high-efficacy therapies; EDSS: Expanded Disability Status Scale; SD: standard deviation; MRI: magnetic resonance imaging. DMT: disease-modifying therapy. Brain MRI lesions: number of patients with presence of contrast-enhancing lesions and/or new or enlarging T2-hyperintense lesions on brain.
OR analyzed by binary logistics for NEDA-3 year 1 (n = 254) and 2 (n = 220).

Logistic regression models to estimate the OR of EHE (reference in model 1) and Mabs (reference in model 2) for NEDA at years 1 and 2. EHE: Early high-efficacy; Mabs: monoclonal antibodies; OR: odds ratio; Unad OR: Unadjusted OR; Adj. OR: Adjusted OR; CI: confidence interval; MRI: magnetic resonance imaging; EDSS: Expanded Disability Status Scale.
Adjusting for MS duration prior HET, type of HET, age at HET, EDSS before HET, number of relapses in 12 months pre-HETs, new brain MRI lesions and sex.
Adjusting for MS duration prior HET, age at HET, EDSS before HET, number of treatments before HET, number of relapses in 12 months pre-HETs, new brain MRI lesions and sex.
Discussion
NEDA-3 is a relevant composite outcome and therapeutic target for neurologists managing patients with MS. In this Argentinian study, we found that HAMS patients treated with HETs had a high probability of achieving NEDA-3 at year 1 and at year 2. Note that, unlike other investigations, this study included only patients with highly active disease, contributing with specific novel information. The frequency distribution of NEDA-3 was similar to those reported with HETs, both in randomized clinical trials as well as in observational studies.14,15 On the other hand, we found that patients who started their treatment with high-efficacy therapies had a significantly higher probability of achieving NEDA-3 at year 2 compared to patients who started moderate-efficacy therapies. Our findings are in line with recent communications suggesting a better control of the disease in the early stages when a more aggressive therapeutic strategy is used for the treatment of MS. 16
Although NEDA should not be considered the only outcome measure for treatment response in MS, 17 it is considered a useful marker of controlled inflammatory activity. Neurological damage occurs from the earliest stages of the disease, and control of inflammatory activity within the first few years from diagnosis is widely considered to be a good prognostic sign. 8 A recently published Argentinian study showed that patients treated with HET from the beginning (EHE) showed a significantly lower risk of EDSS progression, new relapses, and new MRI lesions compared to those with ES. The authors also reported a lower risk of achieving an EDSS score of 6 in the EHE group. 18 A multicenter study from a tertiary MS outpatient clinic in Italy, compared EHE treatment versus ES on the risk of reaching EDSS ≥ 6.0 over 10 years in previously untreated patients with relapsing-remitting MS. The authors found a lower proportion of patients reaching the outcome after EHE (28.0%) vs. ES (38.7%) (Hazard ratio = 0.48; p = 0.024). 19 Our findings are in line with studies supporting EHE therapy.18,22 There is evidence that the risk of progression at 10 years is strongly associated with the evolution of the disease in the first 5 years and that the disability progression accelerates more rapidly after an EDSS score of 4. 21 An observational multicenter study from the international MSBase registry and the Swedish MS registry evaluated disability in patients who started treatment with highly effective therapies (rituximab, ocrelizumab, mitoxantrone, alemtuzumab, or natalizumab) in the first 2 years (early-onset group) compared to that of those starting HET between 4 and 6 years. The early-onset group showed significantly lower EDSS scores at 6 years compared to the late group (p < 0.01), and this difference persisted through each year of follow-up until the tenth year. 20 Although there is robust evidence supporting early initiation of highly effective DMTs in MS, ES is still the most frequently used. 3 The choice of treatment might be influenced by limitations in access to HETs, among other reasons. Difficulties and inequalities in access to DMT in Argentina have been previously reported and continue to be an unmet need in our community.23,24 In this sense, Argentine MS patients receiving care from the private sector reported greater access to DMT and fewer problems accessing treatment compared to those cared for in public institutions. In addition, lack of coverage, longer MS duration, lower educational level, and unemployment were independently associated with inadequate DMT administration.23,24
We found no differences between the association between achieving NEDA-3 and the type of HET (cladribine vs. monoclonals antibodies). Although these findings lack methodological robustness, they support previously reported data on the efficacy and effectiveness of cladribine. 14
We acknowledge several limitations in our research. First, our observational study does not meet the methodological rigor that randomized controlled trials for the comparison of interventions.
Besides, we did not include variables that could influence the result (adherence to treatment, access to treatments, brain atrophy, etc.). Being a retrospective study, clinical outcomes (relapses and EDSS) and MRI analysis could have measurement bias among registry researchers. These limitations could affect the primary objective of this study. On the other hand, the results of the secondary objectives could be influenced by possible treatment selection bias. The cohort exposed to early high-efficacy therapies was younger, with shorter disease duration, and lower EDSS. However, to reduce the influence of these factors (and confounders control), a regression model was performed, we cannot rule out the possibility of hidden confounders that could limiting the results. Regarding the limitations that may affect the external validity of our results, it is important to note that patients with previous exposure to HETs before receiving the current HET (n = 30) were not included in the analysis. Nor were those patients who discontinued treatment for other reasons. Last, this study includes a relatively short follow-up period, long observation periods are needed to establish whether a treatment is effective in reducing relapse rate.
Despite these limitations, the importance of real-world studies in MS and the external validity of these findings, which are in line with other world reports, are highlighted.
In conclusion, our study shows a high frequency of NEDA-3 in HAMS patients treated with HETs. On the other hand, our findings support the importance of early treatment initiation with high-efficacy medications.
Supplemental Material
sj-docx-1-mso-10.1177_20552173231154712 - Supplemental material for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies
Supplemental material, sj-docx-1-mso-10.1177_20552173231154712 for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies by Ricardo Alonso, Magdalena Casas, Luciana Lazaro, Nora Fernandez Liguori, Cecilia Pita, Leila Cohen, Juan Ignacio Rojas, Agustín Pappolla, Liliana Patrucco, Edgardo Cristiano, Marcos Burgos, Carlos Vrech, Raul Piedrabuena, Lopez Pablo, Norma Deri, Geraldine Luetic, Jimena Miguez, Mariela Cabrera, Alejandra Martinez, Gisela Zanga, Verónica Tkachuk, Santiago Tizio, Edgar Carnero Contentti, Eduardo Knorre, Felisa Leguizamon, Carolina Mainella, Pedro Nofal, Susana Liwacki, Javier Hryb, Maria Menichini, Claudia Pestchanker, Marina Alonso, Orlando Garcea and Berenice Silva in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-2-mso-10.1177_20552173231154712 - Supplemental material for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies
Supplemental material, sj-docx-2-mso-10.1177_20552173231154712 for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies by Ricardo Alonso, Magdalena Casas, Luciana Lazaro, Nora Fernandez Liguori, Cecilia Pita, Leila Cohen, Juan Ignacio Rojas, Agustín Pappolla, Liliana Patrucco, Edgardo Cristiano, Marcos Burgos, Carlos Vrech, Raul Piedrabuena, Lopez Pablo, Norma Deri, Geraldine Luetic, Jimena Miguez, Mariela Cabrera, Alejandra Martinez, Gisela Zanga, Verónica Tkachuk, Santiago Tizio, Edgar Carnero Contentti, Eduardo Knorre, Felisa Leguizamon, Carolina Mainella, Pedro Nofal, Susana Liwacki, Javier Hryb, Maria Menichini, Claudia Pestchanker, Marina Alonso, Orlando Garcea and Berenice Silva in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-docx-3-mso-10.1177_20552173231154712 - Supplemental material for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies
Supplemental material, sj-docx-3-mso-10.1177_20552173231154712 for Achieving no evidence of disease activity-3 in highly active multiple sclerosis patients treated with cladribine and monoclonal antibodies by Ricardo Alonso, Magdalena Casas, Luciana Lazaro, Nora Fernandez Liguori, Cecilia Pita, Leila Cohen, Juan Ignacio Rojas, Agustín Pappolla, Liliana Patrucco, Edgardo Cristiano, Marcos Burgos, Carlos Vrech, Raul Piedrabuena, Lopez Pablo, Norma Deri, Geraldine Luetic, Jimena Miguez, Mariela Cabrera, Alejandra Martinez, Gisela Zanga, Verónica Tkachuk, Santiago Tizio, Edgar Carnero Contentti, Eduardo Knorre, Felisa Leguizamon, Carolina Mainella, Pedro Nofal, Susana Liwacki, Javier Hryb, Maria Menichini, Claudia Pestchanker, Marina Alonso, Orlando Garcea and Berenice Silva in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
The authors thank all the patients who contributed to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.