
Abstract
Background
The traditional paper and pencil method for EDSS calculation (pEDSS) is the cornerstone of multiple sclerosis practice; however, it requires an expert for an accurate calculation, and it takes a lot of time to perform the function scores. A new algorithmic approach (aEDSS) has been developed for easier and faster assessment.
Objective
To determine if using aEDSS can achieve good inter-rater agreement and save time compared to pEDSS.
Subjects and methods
This study was conducted on 200 MS patients; EDSS was performed twice for each patient by two neurologists on the same day; one used the pEDSS, and the other used the aEDSS in a random order to test the inter-rater agreement regarding functional system scores and the final EDSS score and to detect the difference in the time needed for calculation between both methods.
Results
The new algorithmic approach achieved excellent agreement with the traditional method (Kappa > 0.81) with a shorter calculation time (16 ± 2.67 min for aEDSS vs 31 ± 4.3 min for pEDSS, P < 0.0001).
Conclusion
The new algorithmic approach could represent a suitable alternative to the traditional method, making EDSS calculation easier and faster.
Introduction
The clinical evaluation of disability in multiple sclerosis (MS) remains the cornerstone outcome measure in everyday practice. Although sophisticated, the traditional paper and pencil method for EDSS calculation (pEDSS) and its functional systems (FS) are the most widely used clinical outcome measures.1,2 It was first introduced by John Kurtzke in 1955 as the Disability Status Scale (DSS), 3 then modified in 1983 as the EDSS, 4 and after that, a set of scoring rules (that depend on the results of a standard neurological examination called Neurostatus) were introduced in 1990. Neurostatus consists of three steps: (a) a standard neurological examination, including the assessment of ambulation (the Neurostatus subscores); (b) the assessment of the FS scores based on these subscores; and (c) the calculation of the EDSS step, depending on the FS scores, and the estimation of walking range and the need for walking support or assistance in everyday activities, evaluated with the ambulation score (AS). It includes detailed definitions and rules to clarify the scoring standards, but it also increases the complexity and time of assessments. 1
A new algorithmic approach (aEDSS) was introduced for easier and faster EDSS practice. It consists of a set of color-coded tables and algorithms that facilitate and accelerate the estimation of neurological examination results, including the neurostatus subscores, FS scores, AS scores, and the final EDSS step. In this prospective study, we test the hypothesis that this new algorithmic approach (aEDSS) could be an easier and faster method and achieve results comparable to those of the traditional paper and pencil EDSS (pEDSS). 5
Materials and methods
The aEDSS algorithm
The aEDSS algorithm is a new method of visualization based on the rules provided in the “Neurostatus” for the standardized assessment of Neurostatus subscores, FS scores, the AS, and the final EDSS step (except for the visual and bowel and bladder subscores, which do not need correction in this new method). It consists of three sets of color-coded tables and algorithms.
The functional subscore algorithms
It consists of six subsets: visual, brainstem, pyramidal, cerebellar, sensory, bowel, and bladder.
Visual
Estimate the best corrected visual acuity in both eyes and follow the diagram in Figure 1 to get the final visual score from 0 to 4 without the need for correction (this is a significant difference from the traditional paper and pencil method, as it is easier and faster to calculate and will yield similar results).

The visual score (corrected).
Brainstem
Calculate the seven subscores as follows: Green is 1, Yellow is 2, Orange is 3, Red is 4, and Brown is 5. The largest of those numbers is the Brainstem Score (Table 1).
The brain stem score (1–5).

Pyramidal
Examine the strength of all muscle groups and determine the lowest grade according to the British Medical Research Council (BMRC) and its distribution (Figure 2).

The pyramidal score.
Cerebellar
Follow the diagram in Figure 3 to get the final cerebellar score.
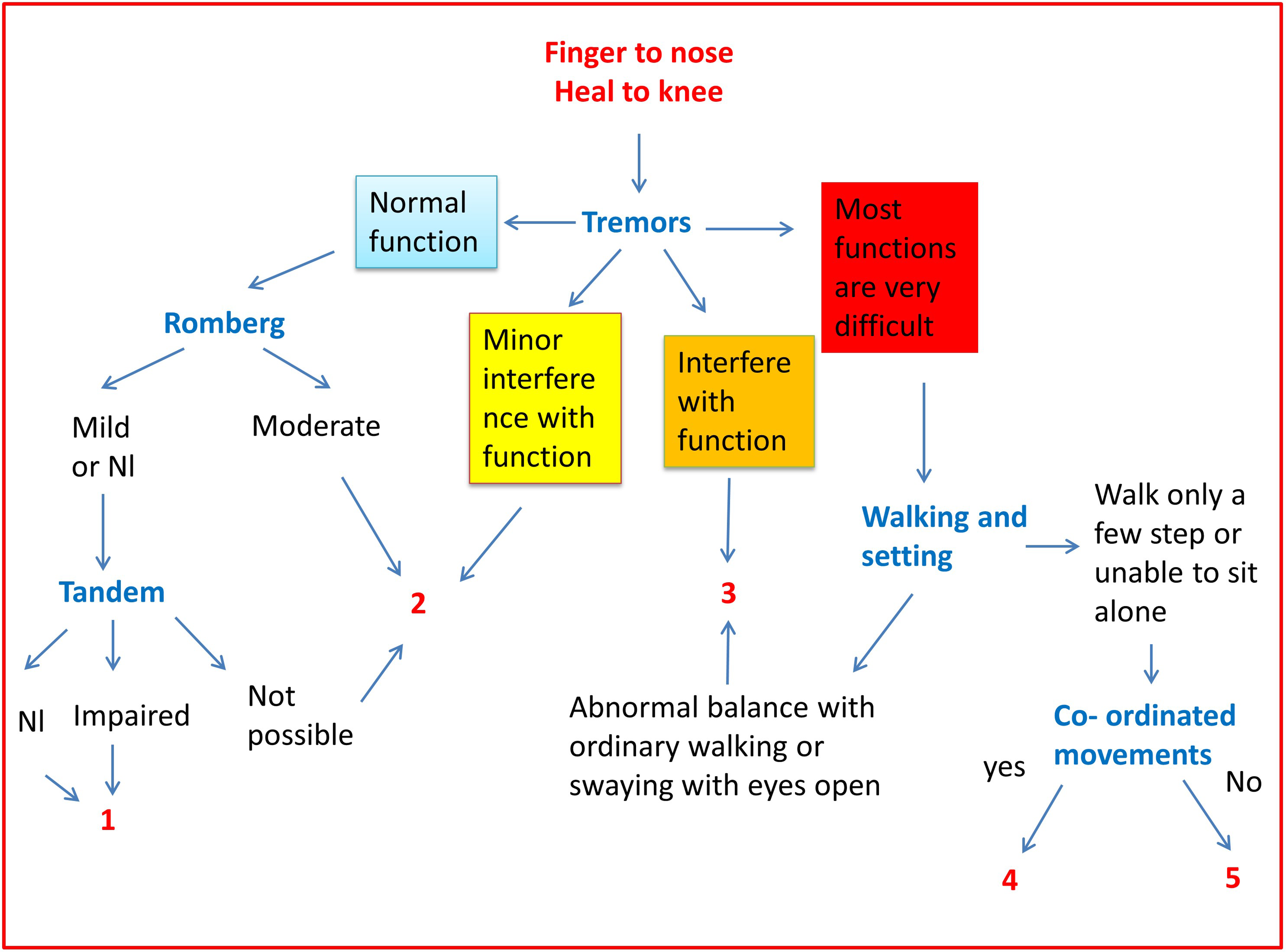
The cerebellar score.
Sensory
The sensory score is divided into superficial and deep sensations, as illustrated in Figures 4 and 5. The final sensory score is the higher of the two subscores; however, if the superficial sensation subscore is 4 and the deep sensation subscore is 4, the final score is 5, and if the superficial sensation subscore is 5 and the deep sensation subscore is 5, the final score is 6.

Superficial sensation algorithm.

Deep sensation algorithm.
Bowel and bladder (corrected from 1 to 5)
Calculate the four subscores as follows: green is 1, yellow is 2, orange is 3, and red is 4. The largest of those numbers is the bowel and bladder score. If the patient scores 4 in urinary urgency, incontinence, and bowel dysfunction, the score is 5. The final bowel and bladder score ranges from 0 to 5, without the need for correction (this is another difference from the traditional paper and pencil method, making it easier and faster to calculate and yielding almost the same results) (Table 2).
The bowel and bladder score corrected (1–5).

Cerebral FS and ambulation
Cerebral FS and ambulation were done in the same manner as in pEDSS.
Interpretation of the EDSS steps based on the seven FS scores
We can complete this task in three steps: first, determine the largest number of the seven FS scores and denote it with the symbol N; the final score will be N, N + 0.5, or N + 1. The second step is to identify how often the largest number is repeated (1, 2, or ≥ 3). The last step is to determine if the other FS scores (other than those taking the largest number) are 0, 1, or more than 1, as shown in Figures 6 and 7.

Interpretation of the 7 FS to get the final function score.

Examples of interpretation of the 7 FS to get the final function score.
One exception to the above rules is that if I have five FS scores of grade 2, the final score will be 5, not 3.5.
The final EDSS steps algorithm (based on the seven FS scores and the AS)
EDSS steps 1.0 to 5 are based on measures of impairment in seven FS, while EDSS steps 4.5 to 9.5 are based on walking and activities of daily living. If the patient is ambulant for less than 500 m but more than 300 m (score 4.5–5 on walking), we assess the seven FSs, and the higher number is the final EDSS score (see Figure 8).

The final EDSS algorithm.
Study design and population
The research ethics committee of the faculty of medicine at Cairo University approved this study. Consent was taken from 200 patients attending the MS outpatient clinic for regularly scheduled follow-up visits to undergo the neurological examination twice on the same day. Patients were diagnosed with MS according to the McDonald criteria. The MS patients underwent a full neurological examination twice by two neurologists with experience in MS on the same day to calculate the Neurostatus subscores, FS scores, AS, and the final EDSS step. All done twice, one using the aEDSS and the other using the pEDSS based on the neurostatus definition.6,7
To reduce the fluctuations of symptoms from day to day, the MS patients were examined independently by two neurologists on the same day. Furthermore, to limit errors related to fluctuations in a patient's daily performance or due to fatigue or training effects caused by the preceding examination, the assessments were done consecutively in a random order, and the examining neurologists were unaware of the results and scores of each other's assessments. 5
After documenting the results, the Neurostatus subscores, FS scores, AS, and the final EDSS step were all compared in pairs of assessments of the same patient to determine the inter-rater agreement and time spent on different parts of the neurological examination, whichever the method used (pEDSS or pEDSS).
Statistics
We compare aEDSS and pEDSS regarding the time needed for calculation using a paired t-test. Patients were rated as “identical” for most of the items, with minimal observed disagreement. We then used the unweighted Cohen's
Results
The patient's characteristics are listed in Table 3. The median, range of FS grades, and final EDSS score calculated by pEDSS and aEDSS are all summarized in Table 4. Outstanding agreements were found between pEDSS and aEDSS regarding the total EDSS and FSs (Kappa > 0.81 for all) (Table 5). The mean time needed for calculation of the EDSS by using the aEDSS (16 ± 2.67 min) is significantly shorter than that for the pEDSS (31 ± 4.3 min), P < 0.0001, Figure 9.

Comparison between aEDSS and pEDSS regarding the time (minutes) needed for calculation.
Patient characteristics.

RRMS: relapsing-remitting multiple sclerosis; SPMS: secondary progressive multiple sclerosis; PPMS: primary progressive multiple sclerosis.
The median (range) of FS grades, and total EDSS calculated by pEDSS and aEDSS.

Inter-rater agreements between pEDSS and aEDSS.

A multi-class confusion matrix was created, and the results showed that the overall accuracy (correct classification/total number of classifications) was 0.9 (180/200), or 90%, as shown in Table 6. The parameters sensitivity, specificity, and precision were calculated as true positive/(true positive + false negative), true negative/(true negative + false positive), and true positive/(true positive + false positive), respectively, as shown in Table 7.
The multi-class confusion matrix for pEDSS and aEDSS.

Sensitivity, specificity, and precision of various parameters in the multi-class confusion matrix for pEDSS and aEDSS.

Discussion
EDSS is the cornerstone of the daily practice of MS. Despite this, EDSS is a bit complex and requires expert training to be able to calculate it accurately, as it consumes a lot of time in its calculation.
Several electronic EDSS calculators were developed to overcome these problems and are available as download applications.8–10 Furthermore, some calculators are designed for patients to use directly to monitor their own clinical condition. 11
Little information is known about the basis of these methods and their agreement with the traditional paper and pencil method. Most of them provide little information about the specific rules used to estimate the FS scores and EDSS steps.
Some only provide the EDSS step determination based on given FS scores and ambulation. None of these tools give a clear way to calculate the FS based on a complete neurological assessment. 5
In our new algorithmic approach, we provide an easy and straightforward method that relies on the same specific rules outlined in Neurostatus, but in a much simpler form, allowing for easier and faster calculation of the FS scores and the total EDSS, while simultaneously achieving excellent agreement with the traditional paper and pencil method.
Selection bias and observer bias are two systemic biases that were avoided in our study. 12 To avoid selection bias, which occurs when the sample is not representative of the whole MS population, we attempted to involve patients with all degrees of disability (EDSS from 0 to 9) so as not to focus only on ambulant patients.
Regarding observer bias, it could result from variation between observers in administering pEDSS and aEDSS, or from an observer's reporting bias when one observer tends to underestimate or overestimate the results of either pEDSS or aEDSS. To account for observer variability, all the neurologists involved in this study were certified EDSS readers who were well-versed in administering both the pEDSS and the aEDSS. Concerning observer reporting bias, we had two neurologists on the same day, one for pEDSS and the other for aEDSS, with patients randomly assigned to do either pEDSS first with one neurologist, then shifted to the other for aEDSS, or vice versa, and the two neurologists were blind to each other's results.
Limitations: Our limitations included the difficulty of involving more patients with severe disabilities (EDSS ≥ 5.5) due to their limited mobility and visits to the clinic, so ambulation was calculated in the aEDSS in the same way as in the pEDSS, some inter-rater variability, especially at the lower end of the EDSS spectrum of scores, and presumably a lack of objective assessment of walking distance.
In conclusion, this study found that the new algorithm approach (aEDSS) is a faster, yet simpler way with excellent agreement compared to pEDSS. As a result, it can significantly enhance and facilitate the everyday practice and clinical trials that use the Neurostatus-EDSS as an outcome measure.
Footnotes
Availability of data and material
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The local ethics committee approved this study. Consents were taken from the patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.