
Abstract
Background
Proprioceptive acuity and impairments in proprioceptively guided reaches have not been comprehensively examined in people with multiple sclerosis (MS).
Objective
To examine proprioceptive acuity in people with MS who self-report and who do not self-report upper limb (UL) impairment, and to determine how people with MS reach proprioceptive targets.
Methods
Twenty-four participants with MS were recruited into two groups based on self-reported UL impairment: MS-R (i.e. report UL impairment; n = 12) vs. MS-NR (i.e. do not report UL impairment; n = 12). Proprioception was assessed using ipsilateral and contralateral robotic proprioceptive matching tasks.
Results
Participants in the MS-R group demonstrated worse proprioceptive acuity compared to the MS-NR group on the ipsilateral and contralateral robotic matching tasks. Analyses of reaches to proprioceptive targets further revealed that participants in the MS-R group exhibited deficits in movement planning, as demonstrated by greater errors at peak velocity in the contralateral matching task in comparison to the MS-NR group.
Conclusion
Our findings suggest that people with MS who self-report UL impairment demonstrate worse proprioceptive acuity, as well as poorer movement planning in comparison to people with MS who do not report UL impairment.
Keywords
Introduction
Multiple sclerosis (MS) is an immune-mediated, progressive neurological disorder often associated with sensory impairment, including a decline in one's sense of body position in space (i.e. proprioception). 1 Given proprioception plays an important role in upper limb (UL) function, including one's ability to perform activities of daily living,2–4 identifying deficits in UL proprioception is essential for preventing further deterioration and informing future rehabilitation for people with MS (PwMS). To establish UL proprioceptive acuity in research settings, participants are typically asked to perform proprioceptive matching tasks, in which they are to match the sensed position of their hand using their opposite hand (i.e. contralateral matching task).1,5 Using this contralateral matching task, Simmatis and colleagues 1 found that a small percentage of PwMS (i.e. 8/43 participants) performed worse than control participants. Miehm and colleagues 5 further demonstrated that PwMS diagnosed with primary progressive MS had greater matching errors compared to control participants and individuals with relapsing-remitting MS. In general, these studies discuss their findings of poor proprioceptive function in light of MS disease progression, such that they emphasize differences between clinical courses 5 or correlations with such clinical measures as performance on the nine-hole peg test (9-HPT). 1 Unfortunately, these studies either do not report 1 or assess 5 endpoint errors, which most studies utilize to quantitatively evaluate proprioceptive acuity in people without MS.6,7 Furthermore, these studies do not assess proprioceptive acuity in PwMS via an ipsilateral matching task, in which participants match the sensed position of their reference hand using the same hand, and hence information does not need to be relayed between the two brain hemispheres. 6 Finally, a detailed investigation into how PwMS plan and execute their movements to a proprioceptive target has not been undertaken in previous studies utilizing proprioceptive matching tasks.
To address these limitations, we aimed to establish proprioceptive acuity in PwMS via ipsilateral and contralateral matching tasks. We also aimed to determine how PwMS reach proprioceptive targets. Proprioception was examined in PwMS in light of perceived UL impairment given recent findings in post-stroke research demonstrating the importance of considering perceived impairment when assessing UL performance following neurological pathologies, 8,9 as well as findings from our own work in PwMS. 10 Specifically, proprioception was compared between PwMS who reported UL impairment (MS-R) and PwMS who did not report UL impairment (MS-NR). Data were also collected from a group of age-matched controls as a reference sample. We hypothesized that participants in the MS-R group would demonstrate greater performance deficits on the robotic proprioceptive matching tasks compared to participants in the MS-NR group.
Methods
Participants and demographics
This manuscript is part of a larger study characterizing UL performance in PwMS across a variety of tasks differing in the engagement of sensory, cognitive, and motor processes. Power analysis using G-Power (Version 3.1.9.7) revealed that 36 participants were required to detect group differences with respect to proprioceptive acuity, which is a similar number of participants used in previous literature that recruited PwMS with mild-to-moderate disability.11–13 The MS sample was recruited from MS-specific community outlets (e.g. the MS Society of Canada outlets and MS support groups). In brief, PwMS required (1) self-reported diagnosis of MS; (2) been relapse-free for 30 days; and (3) experienced no changes to disease-modifying therapies in the past 6 months to be eligible to participate. Additional details can be found in Wijeyaratnam et al., 10 and Table 1 for participant characteristics (24 PwMS and 12 age- and sex-matched controls).
Demographic and clinical characteristics for the three experimental groups. Values are reported as mean (standard deviation), unless specified otherwise.

Note. BMI, body mass index; EDSS, Expanded Disability Status Scale. MS types were not compared statistically between MS-NR and MS-R groups.
Denotes values reported as median (interquartile range).
Denotes significant difference between MS-NR and MS-R (p < 0.05).
Procedures
Upon arriving at the lab, participants provided written informed consent, and hand dominance was established. 14 Height and weight were measured in the lab using a scale with a stadiometer (Detecto, Webb City, MO) and body mass index (BMI) calculated. The Expanded Disability Status Scale (EDSS) 15 was performed by a Neurostatus-certified assessor (TE, Level C) to characterize overall disability and sensory system scores. Participants reported their use of assistive devices/technologies using the Assistive Device Use questionnaire. 16 All ethical standards and safety monitoring procedures were followed according to the University of Ottawa Health Sciences and Science Research Ethics Board. Participants received $40 remuneration for their participation in the study.
Robotic assessments of proprioception
Proprioceptive matching tasks were completed in the lab using a two-joint robot manipulandum (End-Point Lab, Kinarm, Kingston, ON; Figure 1A). Participants sat on height-adjustable chairs and grasped either both handles or a single handle of the two-joint robot manipulandum with their dominant and/or non-dominant hand(s) (Figure 1A). Participants’ view of their hands was obstructed by the reflective surface and a black cloth draped between their shoulders and the experimental apparatus. The location of the robotic handles (i.e. participants’ hands) was tracked at 1000 Hz, with a spatial accuracy of 0.1 mm.

Experimental apparatus, robotic proprioceptive matching tasks, and trial sequence. (a) Experimental apparatus for the robotic proprioceptive matching tasks. Participants were instructed to grasp the robotic handles with their dominant or non-dominant hand (i.e. ipsilateral matching task) or both hands (i.e. contralateral matching task). (b) Top view of the visual display, indicating the three potential reference locations (gray circles) on either side of the workspace. The reference locations were the same for both the ipsilateral and contralateral matching tasks. (c) An example trial sequence that was completed by a participant using their dominant (unshaded region) and non-dominant (shaded region) hands. Tasks outlined by a solid black border indicates trials that were included in our analyses, whereas dotted border represents practice trials that were not analyzed. These tasks were counter-balanced by hand (i.e. dominant vs. non-dominant testing hand first) and task (i.e. ipsilateral matching first vs. contralateral matching first).
Proprioceptive acuity was assessed in ipsilateral and contralateral matching tasks, in which participants were instructed to match the position of the reference hand with their testing hand in the absence of visual feedback. In the ipsilateral matching task, the reference and testing hands were the same, while in the contralateral matching task, the reference and testing hands differed. In general, the robotic handle passively moved the participant's reference hand from a home position to one of three reference locations at a distance of 5 cm (near), 7.7 cm (middle), or 9.4 cm (far) from the home position at an angle of 75°, 65°, and 44° from the horizontal, respectively (see Figure 1B). Participants completed both the ipsilateral and the contralateral matching tasks with both hands (see Figure 1C). Figure 2 provides a breakdown of the timing of events that occurred in each trial.

Timeline of events within a trial for the ipsilateral and contralateral matching tasks. (a) The ipsilateral matching task commenced with the reference hand at the home position for 500 ms (box i). The robot then passively moved the reference hand out to the reference position in an MT of 1500 ms, with two or three reversals around the unseen reference location (box ii). The reference hand was held at the reference location for 1000 ms (box iii), before being passively moved back to the home position in an MT of 1500 ms (box iv). Once back at the home position, the hand was held at the home position for 500 ms (box v). Following this time, the home position changed to magenta (box vi), which signaled the participant to actively reproduce the reference location with the same hand (box vii). (b) The contralateral matching task commenced with the two hands held at their corresponding home positions (20 cm apart) for 500 ms (box i). The robot then passively moved the reference hand for 1500 ms to the unseen reference position. The robot moved along a path with two or three reversals around the reference position before it stopped at the final reference location (box ii). The reference hand stayed in the reference position for the duration of the trial. After 1000 ms, the home position of the testing hand changed to magenta (box iv), which signaled the participant to actively reproduce the final position in the opposite testing hand (box v). Once the final position of the testing hand was determined, both hands were brought passively back to the home positions in an MT of 1500 ms (Figure 2A box viii and Figure 2B box vi).
Data analysis
Performance of the active movement portion of each proprioceptive matching trial (i.e. when the participant moved the testing hand into position) was evaluated using custom-written MATLAB scripts (Matlab R2013b (8.2.0.701, The MathWorks, Inc.)). Movement onset of the testing hand was defined as the first increase in velocity greater than 0.01 m/s for 50 consecutive recording samples (i.e. 50 ms). The trial was considered complete when the velocity of the hand fell below 0.01 m/s. A total of 77 trials (5%) were removed from analysis across the entire sample based on outliers as established by start position (>3 cm from the home position) or endpoint position or movement time (MT) (>3 standard deviations away from the respective group means). 17 Performance on the robotic proprioceptive matching tasks was evaluated with respect to (1) overall accuracy to assess proprioceptive acuity and (2) engagement of movement planning and control processes during the goal-directed reach.
The accuracy of the participant's final position was determined based on resultant error and absolute errors in both the horizontal (AEX) and vertical (AEY) directions relative to the reference location. As well, absolute endpoint angular error (|EPAE|) was calculated as the absolute value of the angular difference between the movement vector (i.e. vector joining the home position to the testing hand's end position) and reference vector (i.e. vector joining the home position to the reference location).
Increased engagement of movement planning/preparation processes within a goal-directed reach is reflected by increased reaction time (RT), and time to peak velocity (TTPV),18–23 while a greater engagement of movement control processes during a reach is reflected by a longer time spent after peak velocity (TAPV), a greater number of movement corrections (i.e. a less smooth movement resulting in higher jerk scores), and more accurate movements.19,23,24 We examined the following measures related to movement planning of the testing hand: RT, proportional time to peak velocity (pTTPV), peak velocity (PV) in the resultant direction, and absolute angular error at PV (|PVAE|). The contribution of movement control processes engaged during reaching execution (online) in response to sensory feedback (e.g. proprioception) was evaluated based on MT, path length, proportional time after peak velocity (pTAPV), and jerk score, where jerk score was defined as the change in acceleration over the course of a movement and calculated according to the following formula:
Statistical analysis
We compared performance in the MS sample across self-reports of UL impairment. Similar to the protocol established by Simmatis and colleagues, 1 we first established the number of MS participants within each group who fell outside a 95% confidence interval (CI) established by data from age-matched controls. Dependent variables for the ipsilateral and contralateral matching tasks were then compared in 2 Groups (MS-R vs. MS-NR) × 2 Hand (dominant vs. non-dominant hand) mixed ANOVA with RM on the last factor. Finally, we compared participants’ accuracy (i.e. R-Error and |EPAE|) on the ipsilateral versus contralateral matching tasks within Groups in a 2 Task (ipsilateral vs. contralateral matching task) × 2 Hand (dominant vs. non-dominant hand) RM ANOVA to establish task differences. The significance value for all statistical tests performed was set at p < 0.05, and Bonferonni post-hoc tests corrected for multiple comparisons were used to find the locus of significant effects. Below we discuss the significant effects of Group, and significant Group × Hand interactions for our accuracy, planning, and control measures
Results
Table 1 presents a summary of the sample demographics and clinical characteristics.
Robotic assessments of proprioception: Ms compared to control participants
Figure 3 displays the percentage of MS-R and MS-NR participants whose proprioceptive acuity or performance measures related to movement planning and control fell outside the 95% CI established based on data from our age-matched controls. As seen in Figure 3, a number of MS-R and MS-NR participants fell outside the established CI, in particular with respect to variability measures (e.g. variability of resultant error and absolute endpoint angular error).

Percentage of MS participants designated as impaired based off 95% confidence intervals established from data from control participants. Performance percentages by PwMS were separated by task type (ipsilateral and contralateral matching tasks), hand (non-dominant hand (NDH) and dominant hand (DH)) and group (MS-R and MS-NR) for dependent variables (i.e. accuracy, planning, and control). Accuracy measures: resultant error mean (R-Error) and variability (V_R-Error), absolute error in the horizontal direction mean (AEX) and variability (V_AEX), absolute error in the vertical direction mean (AEY) and variability (V_AEY) and absolute endpoint angular error mean (|EPAE|) and variability (V_|EPAE|). Planning measures: reaction time mean (RT) and variability (V_RT), proportional time to peak velocity mean (pTTPV) and variability (V_pTTPV), peak velocity mean (PV) and variability (V_PV) and absolute peak velocity angular error mean (|PVAE|) and variability (V_|PVAE|). Control measures: movement time mean (MT) and variability (V_MT), path length mean (PL) and variability (V_PL), proportional time after peak velocity mean (pTAPV) and variability (V_pTAPV) and jerk score mean (Jerk) and variability (V_Jerk).
Robotic assessments of proprioception: Ms-R compared to Ms-Nr
Mean and variability of accuracy and performance measures on the robotic proprioceptive matching tasks for the MS-R and MS-NR groups are reported in Tables S1 and S2 of the Supplementary File.
Ipsilateral matching task
With respect to accuracy, group differences were observed in |EPAE|, such that MS-R participants (x̄ = 6.0° ± 1.5) were less accurate than MS-NR participants (x̄ = 3.8° ± 0.2) when completing the matching task with either their dominant or non-dominant hands (Group: F(1,22) = 7.356, p = 0.013, η2 = 0.251), see Figure 4. No group differences were observed with respect to movement planning or movement control measures (all p > 0.05).
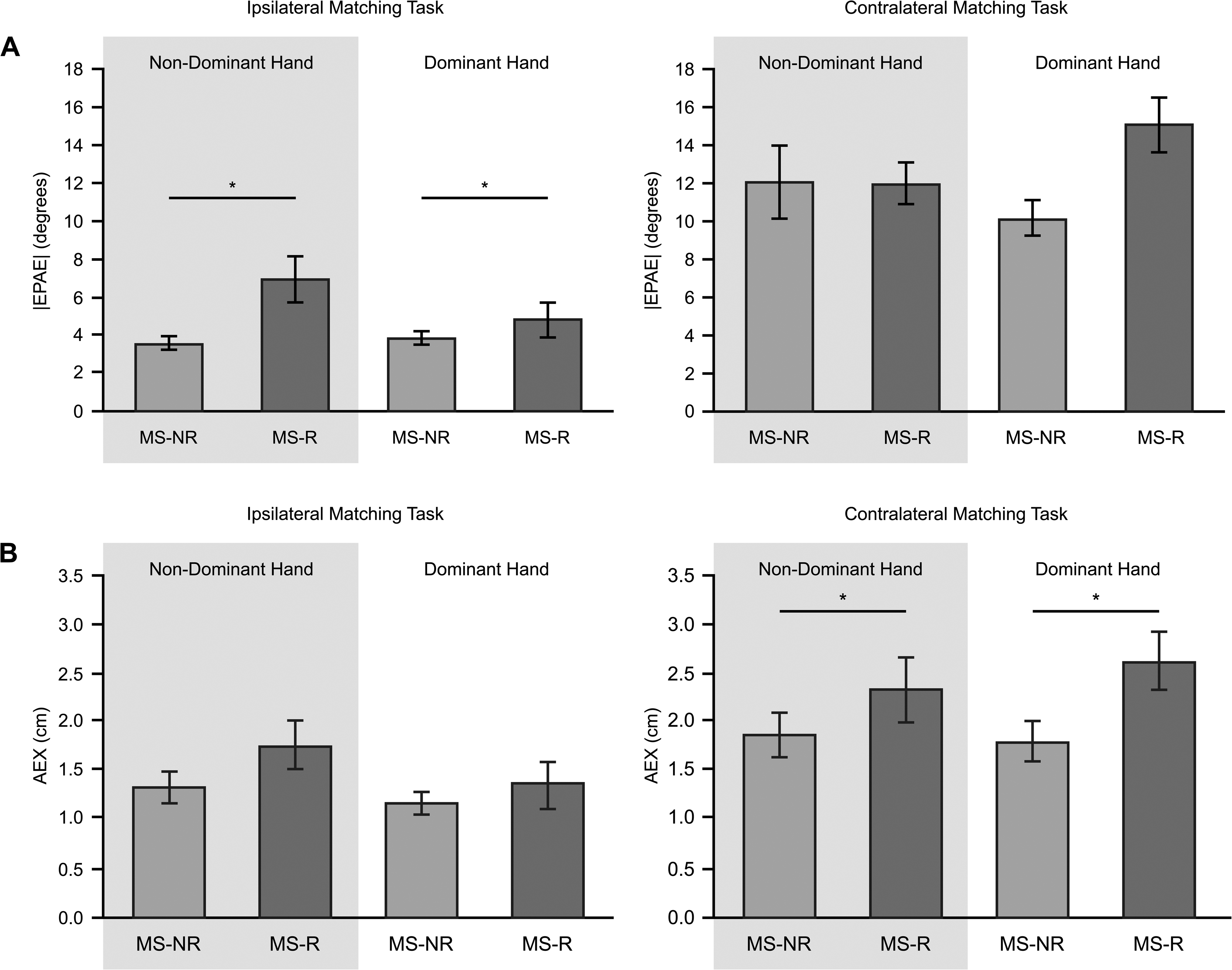
Accuracy measures for PwMS separated by group (MS-NR vs MS-R) when performing the task with their non-dominant and dominant hands. (a) Absolute endpoint angular errors (|EPAE|) measured in degrees for the ipsilateral (left) and contralateral (right) matching tasks. (b) Absolute errors in the horizontal direction (AEX) measured in centimeters for the ipsilateral (left) and contralateral (right) matching tasks. Shaded regions represent trials in which participants’ non-dominant hand was the testing hand. Unshaded regions represent trials in which participants’ dominant hand was the testing hand. Error bars denote the standard error of the mean. * Indicates significance between groups.
Contralateral matching task
We found significantly larger horizontal errors for the MS-R group (AEX: x̄ = 2.5 cm ± 1.1) compared to the MS-NR group (x̄ = 1.9 cm ± 0.8; F(1,22) = 5.227, p = 0.032, η2 = 0.192, see Table S2 and Figure 4(b)). Furthermore, with respect to |EPAE|, analysis revealed a trend for Group differences (F(1,22) = 3.994, p = 0.058, η2 = 0.154), indicating that MS-R (x̄ = 13.6°, ± 2.3) demonstrated greater directional errors than MS-NR (x̄ = 11.1° ± 1.4). Group differences were observed with respect to movement planning in the contralateral matching task. Specifically, there was a main effect of Group with respect to RT variability (F(1,22) = 5.321, p = 0.031, η2 = 0.195). MS-NR participants (x̄ = 288.8 ms ± 4.3) were more variable in the time it took them to initiate their movements compared to MS-R participants (x̄ = 187.4 ms ± 41.4). As well, there was a significant Group × Hand interaction with respect to |PVAE| (F(1,22) = 5.289, p = 0.031, η2 = 0.194). Post-hoc analysis revealed that when matching with the dominant hand, the MS-R group (x̄ = 16.5° ± 1.1) demonstrated greater errors at PV than the MS-NR group (x̄ = 4.2° ± 1.4). There were no group differences with respect to movement control measures (all p > 0.05).
Ipsilateral vs contralateral matching task
The resultant error did not differ between tasks (ipsilateral vs contralateral matching task), but both Groups (i.e. MS-R and MS-NR) demonstrated greater absolute endpoint angular errors in the contralateral matching task in comparison to the ipsilateral matching task (all p < 0.05).
Discussion
The current study aimed to describe proprioceptive acuity in PwMS who report UL impairment (MS-R) and those who do not report UL impairment (MS-NR). Further, this study aimed to characterize differences in how PwMS reach proprioceptive targets depending on self-reported UL impairment. While self-reporting UL impairment could be considered a limitation, self-reports were corroborated with clinical assessments. As a group, participants in the MS-R group had a higher EDSS score compared to participants in the MS-NR group.
Proprioceptive acuity in PwMS
Recently, differences in proprioceptive acuity have been reported in PwMS based on clinical course, such that people with primary progressive MS have demonstrated lower vibration sensitivity, poorer elbow matching, and overall reduced position sense across ULs when compared to people with relapsing-remitting MS. 5 Moreover, a small percentage of PwMS (i.e. approximately 20%) demonstrate greater matching errors compared to control participants. 1 We found that, similar to Simmatis et al., 1 we had several participants with MS whose proprioceptive acuity and performance measures related to movement planning and control fell outside a 95% CI established based on data from our age-matched controls. In fact, as shown in Figure 3, variability related to proprioceptive acuity and performance measures indicated that approximately 20% of PwMS fell outside the 95% CI when the ipsilateral and contralateral tasks were performed by the dominant and non-dominant hands. These results suggest individual differences in how PwMS perform and complete proprioceptive matching tasks.
Recent work on people post-stroke has demonstrated the importance of considering perceived impairment when assessing UL performance.8,9 Taking perceived impairment into account, previous work from our group examining visually guided reaching performance has shown that PwMS with perceived UL impairment tend to be more variable with respect to the time it takes to initiate their movements relative to controls. 10 In contrast, PwMS that do not report UL impairment did not differ from controls with respect to RT variability. Using the same participants, we show differences in proprioceptive acuity depending on the perceived impairment, such that the MS-R group was less accurate than the MS-NR group on the robotic proprioceptive matching tasks. Specifically, the MS-R group were less accurate at matching their final hand position in the ipsilateral matching task (demonstrating significantly greater absolute angular errors) and contralateral matching task (demonstrating significantly greater errors in the horizontal direction and a trend for greater absolute angular errors) compared to the MS-NR group. Such deficits could feasibly translate into challenges in accomplishing daily tasks that require UL movements to moving and/or stationary targets in the absence of vision (e.g. bringing a cup of water to one's mouth to drink). 27
We recognize that robotic equipment is specialized, and hence may not be a practical option for the assessment of proprioception in clinical settings. However, these matching tasks can be performed with other motion-tracking technology or by having an experimenter move a subject's arm to a specific position and then having the subject replicate that position to determine accuracy in matching performance.11,28 Utilizing these adapted proprioceptive matching tasks that are more reflective of everyday movement compared to typical clinical assessments of UL performance, which often assess proprioception when the limb is stationary or completing fine movements, can ensure a more accurate and relevant assessment of proprioceptive acuity.
Proprioceptively guided reaches in PwMS
Robotic proprioceptive matching tasks also enable one to examine how PwMS carry out goal-directed movements to proprioceptive targets. In the current study, we evaluated the performance of goal-directed movements with respect to the contribution of movement planning and control processes.29,30 Previous work exploring how PwMS plan and execute their movements to visual targets has demonstrated that PwMS utilize compensatory strategies, such as reaching with a slower speed, spending more time after PV, and reaching with an overall longer movement duration in order to reduce their endpoint errors.10,11,29,31 Employing these strategies enables PwMS to utilize visual feedback for a longer period of time when attempting to reach the desired endpoint.
However, in the current study, participants were unable to see their limbs or targets and thus could not rely on visual feedback throughout the task. We found that at an individual level, a number of PwMS differed from age-matched controls with respect to how their movements were planned and controlled when reaching a proprioceptive target. Moreover, we found that performance with respect to movement planning differed between groups in the contralateral matching task, such that MS-R participants exhibited greater errors at PV (in the dominant hand) compared to MS-NR participants. These increased errors early in the movement demonstrate impaired movement planning which translated to deficits in accuracy, as described above. However, MS-R and MS-NR executed their movements in a similar manner, such that both groups showed similar MTs and jerk scores. Together, these results would suggest that MS-R participants did not utilize compensatory strategies, such as reaching at a slower speed or making more movement corrections (i.e. jerk score) to reduce their endpoint error, relative to MS-NR participants.
Given that MS-R participants demonstrated greater endpoint errors than MS-NR, utilizing compensatory strategies may be beneficial to reduce endpoint errors. PwMS could be encouraged to move at slower speeds during UL rehabilitation, in order to prioritize movement accuracy (i.e. speed-accuracy trade-off).30,32 Previous literature has reported comparable reaching performance in individuals post-stroke who moved at slower speeds as control participants who made faster movements. 33 Moreover, the notion of movement slowing has been put forth in MS rehabilitation for such tasks as walking or (motorized) wheelchair driving, in order to promote safe navigation in and around the environment. 34
Recent work has evaluated proprioceptive acuity and underlying neural correlates in PwMS while performing an ipsilateral and contralateral matching task with the lower limb. 13 In general, results revealed that position sense processing relied on the activation of frontoparietal regions in the ipsilateral matching task, as well as precise communication across the hemispheres in the contralateral matching task. The authors suggest that PwMS engage cognitive resources to reduce endpoint errors in lower limb matching, thus providing support to the notion that utilizing compensatory strategies may be beneficial to improve task accuracy, but more importantly, complete ADLs.
Conclusion
Impairments associated with MS vary greatly across individuals. While some individuals with MS experience sensory disturbances, others may only experience cognitive and/or motor deficits. Our results support this individual variation, as several people with MS performed worse than age-matched controls without MS across multiple dependent measures. When people with MS were separated by UL impairment, participants with self-reported UL impairment demonstrated worse proprioceptive acuity and deficits in movement planning compared to participants who did not self-report UL impairment. Thus, our results emphasize the value of perceived impairment when evaluating UL proprioceptive acuity.
Supplemental Material
sj-docx-1-mso-10.1177_20552173221111761 - Supplemental material for Assessing proprioceptive acuity in people with multiple sclerosis
Supplemental material, sj-docx-1-mso-10.1177_20552173221111761 for Assessing proprioceptive acuity in people with multiple sclerosis by Serena Goldlist, Darrin O Wijeyaratnam, Thomas Edwards, Lara A Pilutti and Erin K Cressman in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgments
The authors thank all the participants for participating in this experiment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported, in part, by an endMS Doctoral Studentship Award from the Multiple Sclerosis Society of Canada awarded to Mr Darrin O. Wijeyaratnam, as well as by funds from the Faculty of Health Sciences at the University of Ottawa awarded to Dr Erin K. Cressman and Dr Lara A. Pilutti.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.