
Abstract
Background
Although recovery from relapses in MS appears to contribute to disability, it has largely been ignored as a treatment endpoint and disability predictor.
Objective
To identify demographic and clinical predictors of relapse recovery in the first 3 years and examine its contribution to 10-year disability and MRI outcomes.
Methods
Relapse recovery was retrospectively assessed in 360 patients with MS using the return of the Expanded Disability Status Scale (EDSS), Functional System Scale and neurologic signs to baseline at least 6 months after onset. Univariate and multivariable models were used to associate recovery with demographic and clinical factors and predict 10-year outcomes.
Results
Recovery from relapses in the first 3 years was better in patients who were younger, on disease-modifying treatment, with a longer disease duration and without bowel or bladder symptoms. For every incomplete recovery, 10-year EDSS increased by 0.6 and 10-year timed 25-foot walk increased by 0.5 s. These outcomes were also higher with older age and higher baseline BMI. Ten-year MRI brain atrophy was associated only with older age, and MRI lesion volume was only associated with smoking.
Conclusions
Early initiation of disease-modifying treatment in MS was associated with improved relapse recovery, which in turn prevented long-term disability.
Introduction
The clinical course of multiple sclerosis (MS) is largely determined by the varying frequency, severity and recovery of relapses. 1 A high frequency and severity of relapses, particularly in the first two years, have been established as unequivocal indicators of higher disease burden.2–4 However, the third determinant, relapse recovery, remains the least explored. Although its contribution to disability has been shown in a small number of studies,5–7 it has not been included as a treatment endpoint in clinical trials. 8
Incomplete recovery, defined by the persistence of neurologic deficits after a relapse, can be observed in 34–59% of relapses.9,10 The degree of recovery varies significantly among patients, 11 and appears to be influenced by relapse severity. 5 However, other demographic and clinical predictors of recovery have only been found in isolated studies and remain equivocal. Interestingly, a small number of studies has shown that the degree of recovery from the first relapses in a patient’s course can predict the time to disability progression2,3,12 and the time to transition into secondary progressive MS. 13
There is a need to better understand the risk factors for incomplete relapse recovery, the potential effects of disease-modifying treatments and the contribution of incomplete recovery to long-term disability. In this study, we examined the determinants of relapse recovery in the first three years, as well as its contribution to 10-year outcomes.
Materials and methods
Patient cohort and inclusion criteria
We studied a retrospective, clinic-based patient cohort enrolled in the
Patients enrolled in CLIMB were included in the present study if they met all of the following criteria: at least 8.5 years had elapsed since their first symptom, their first visit was within one year of their first documented symptom, they were aged at least 18 years at their first visit and had been diagnosed with relapsing remitting MS according to the McDonald criteria 2010 or 2017.16,17 The first symptom date was determined from the initial note, and demographic, relapse and treatment data were extracted for the first 3 years from the first symptom (Figure 1). Patients were not required to have had additional relapses after their first attack.

Study timeline. Schematic representation of the inclusion criteria, early disease features and long-term outcomes included in the analysis.
Assessment of relapse recovery
Recovery from each patient’s initial attack and subsequent relapses within 3 years was determined by an investigator blinded to 10-year disability outcomes. A binary label of “Complete Recovery” or “Incomplete Recovery” was assigned to each relapse by comparing neurologic examinations from visits before and after. Complete Recovery denotes a complete return to baseline, whereas Incomplete Recovery signifies persistence of signs or symptoms associated with the relapse after at least 6 months of recovery. For each initial episode, the baseline neurologic examination was assumed to have been normal. For subsequent relapses, the latest visit at least 5 days before relapse onset was used to determine the baseline disability before the relapse. Residual disability after 6 months was derived from the earliest visit at least 6 months after onset.
If a relapse was the only relapse in the interval between its baseline and follow-up visits and had a relapse-free interval six months before and six months after symptom onset, recovery was determined based on the return of follow-up Expanded Disability Status Scale and all Functional System Scores to baseline. For the remaining relapses, which had overlapping baseline and recovery assessments, all single or multiple relapses that had a rapid EDSS and FSS return to baseline before 6 months were also classified as recovered. For the remaining relapses, EDSS/FSS increases could not be attributed to a single relapse. These were classified based on residual changes in specific signs and Functional System Scores: if two or more relapses were associated with different deficits, recovery at 6 months was determined for each based on different signs (e.g. an optic neuritis and a motor attack within 2 months were assessed based on the recovery of vision and strength, respectively). The remaining relapses with similar deficits were classified based on providers’ assessments in notes (e.g. “made a full recovery from recent relapse”) or, when those were not available, patient perceptions (residual symptoms). This resulted in a comprehensive assessment of recovery from all attacks within the first 3 years.
MRI and automated pipeline
Brain MRI acquisition was performed on a 3Ta unit (Siemens Skyra) which used a 20‐channel head coil, comprised of 3 high-resolution sequences, and covered the whole head with 1 mm3 isotropic voxel sizes. This included a 3 D T1‐weighted gradient echo (TE/TR = 2.96/2300 msec, TI = 900 msec, flip angle = 9 deg), 3 D T2 spin echo (TE/TR = 300/2500 msec, echo train length = 160), and 3 D T2‐FLAIR (TE/TR = 389/5000 msec, TI = 1800 msec, echo train length = 248). Sequences were optimized in contrast for depicting brain‐cerebrospinal fluid interfaces and white matter lesions. The main steps of the fully automated quantitative analysis pipeline and its validation have been described previously. 18 The output provided brain T2 hyperintense lesion volume (T2LV) and brain parenchymal fraction (BPF), a surrogate of whole brain atrophy. This pipeline has shown high accuracy and reliability. 18
Outcomes and statistical analysis
The first aim was to identify risk factors associated with incomplete relapse recovery. The outcome was the recovery of each relapse, and demographic, clinical and treatment information were used as predictors. In order to overcome the small sample size for some disease-modifying treatments, they were grouped into the following: untreated, interferons (Interferon β-1a, β-1β), glatiramer acetate, and all other DMTs. The same was done for races, which were grouped into Non-White and White (Table 1).
Demographic characteristics of the patient cohort.

For the second aim, prediction of 10-year outcomes, disability and imaging outcomes were extracted from the visit and MRI scan closest to a timepoint 10 years from first symptom, within 8.5 to 11.5 years (Figure 1). The primary outcome was the EDSS score at this visit. Secondary outcomes included timed 25-foot walk at the 10-year visit, T2LV and BPF.
Analyses were conducted using R Language and Environment, v.3.3.2 (Vienna, Austria). They included generalized estimating equations with exchangeable correlation structure for Aim 1, due to repeated outcomes (multiple relapses from the same patient), and linear regressions for Aim 2. Both univariate and multivariable analyses were employed. A level of 0.05 was used to determine statistical significance.
Study approval
This study complied with the Declaration of Helsinki. The CLIMB study is approved by the Mass General Brigham Institutional Review Board. All participants provided written informed consent for the CLIMB study. Additional consent was not required.
Results
Demographics and disease course
A search based on the inclusion criteria yielded 360 patients enrolled in CLIMB, who were all included. The demographics are available in Table 1. Briefly, 89.2% were white and 73.6% were female. The mean age at first symptom onset was 35.8 years. On average, patients had 2.04 relapses, or one initial attack and 1.04 subsequent relapses in the first three years (mean Annualized Relapse Rate: 0.35, Table 1).
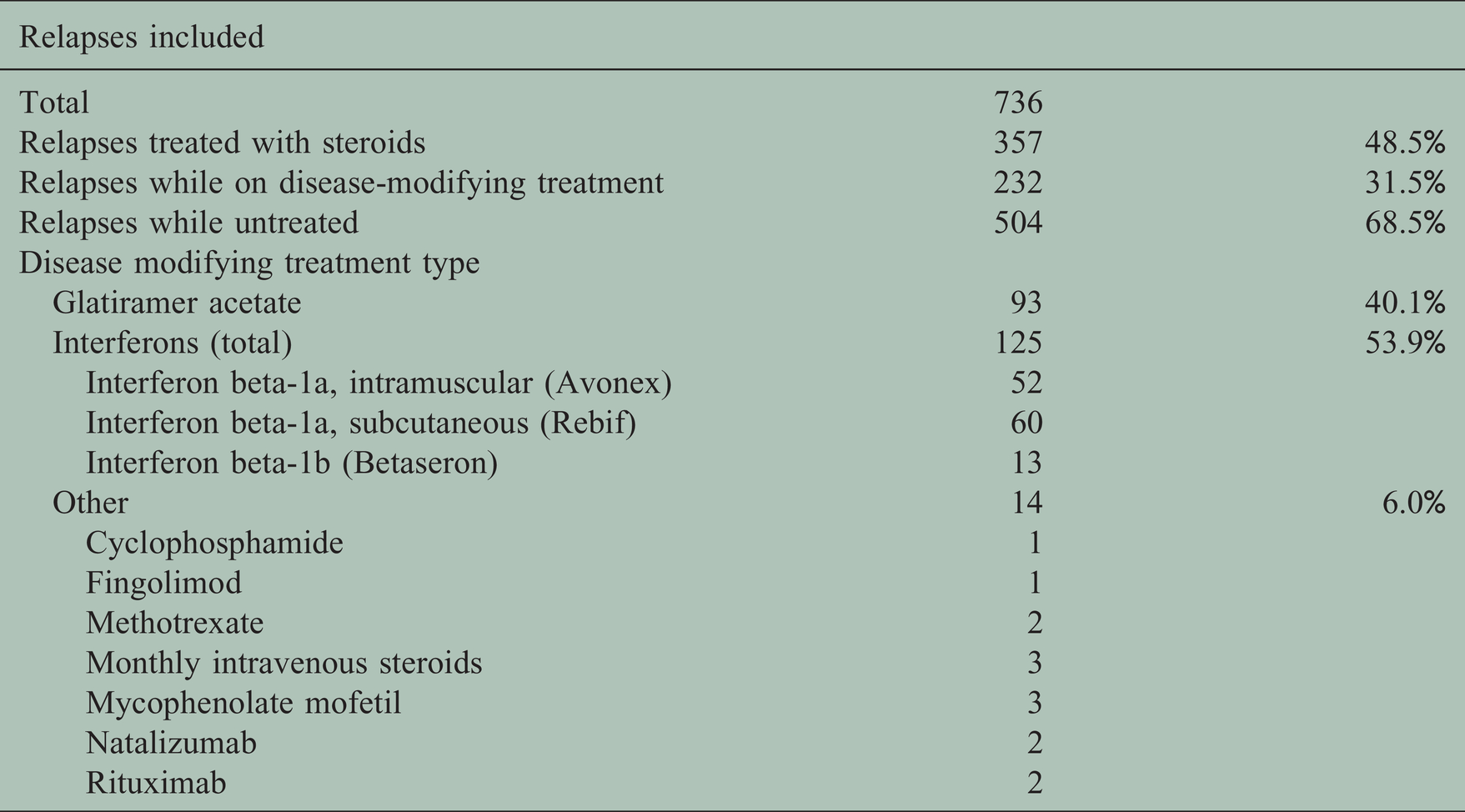
328 relapses (44.6%) had incomplete recovery at 6 months. 232 relapses (31.5%) occurred when the patient was on a disease-modifying treatment and 357 (48.5%) were treated with steroids. Detailed treatment information is available in Table 2. 51.8% of relapses in untreated patients had an incomplete recovery, compared to 28.9% in patients who were treated with a disease-modifying drug (p-value < 0.001) (Figure 2; Table 3).
Treatment status of the included relapses.

Association of treatment status with relapse recovery. Relapses that occurred while the patients were on a disease-modifying treatment (n = 232) had significantly improved recovery compared to relapses that occurred in untreated patients (n = 504).
Demographic and clinical predictors of relapse recovery.

Significance levels:
At the 10-year timepoint, the data available consisted of EDSS scores in 355 patients, timed 25-foot walk in 355 patients, and quantitative MRI data in 196 patients. The mean EDSS was 1.655 (SD:1.51). 24.5% of patients had a normal examination (EDSS = 0), and 34.4% had abnormal signs without overt disability (EDSS = 1–1.5, Supplemental Figure S1).
Demographic and clinical factors associated with relapse recovery
In univariate analyses, relapses in the first three years were more likely to recover completely in patients who were younger at their first symptom, had lower BMI, higher disease duration and were on a disease-modifying treatment at the onset of the attack, specifically interferons or glatiramer acetate. Complete recovery was also more likely in relapses that were treated with steroids, had no bladder, bowel or cognitive symptoms on history or exam and were classified by clinicians as mild.
In the multivariable analysis, significant predictors of complete recovery included lower age at first symptom, higher disease duration, interferon treatment and absence of bowel or bladder symptoms. There were also nonsignificant trends associating complete recovery with the absence of cognitive symptoms, absence of optic nerve localization and presence of brainstem and/or cerebellar lesions based on history.
Upon excluding each patient’s first attack and examining only the subsequent relapses with a known baseline EDSS (n = 376), 71.5% of relapses on DMT recovered completely, compared to 63.8% of relapses in patients not on DMT (p = 0.11).
Recovery from relapses was not associated with sex, smoking history, family history of MS, race or relapse duration in either model. The univariate and multivariable analyses are presented in Table 3.
Prediction of 10-year outcomes
In the univariate analyses, the EDSS score at 10 years from the first symptom increased by 0.7 points for every relapse in the first 3 years with incomplete recovery (Figure 3), decreased by 0.2 points for every relapse with complete recovery, increased by 0.04 points for every added BMI point and increased by 0.03 points for every added year of age at first symptom. In the multivariable model, 10-year EDSS increased by 0.6 points for every incomplete recovery and by 0.02 points for every added year of age at first symptom. Higher BMI was also associated with higher EDSS, without reaching statistical significance.

Correlation of incomplete recoveries with 10-year disability. Each patient’s Expanded Disability Status Scale score at 10 years (y-axis) was significantly correlated with the number of incomplete recoveries they had had in the first 3 years (x-axis). For each additional incomplete recovery, the mean 10-year EDSS score increased by 0.6 points. The boxplots depict the median EDSS and interquartile range.
The timed 25-foot walk score at 10 years increased by 0.6 and 0.5 seconds for every incomplete recovery in the univariate and multivariable models respectively. It was also higher by 0.08 and 0.07 seconds for every added BMI point, higher by 0.04 and 0.03 seconds for every added year of age at first symptom and lower by 0.6 and 0.6 seconds in males in the two models respectively.
On 10-year MRI, lower brain parenchymal fraction (BPF), indicating brain atrophy, was only associated with increased age at first symptom with a trend for male sex in both models. The total volume of T2-hyperintense lesions was only associated with a positive smoking history in both models.
All univariate and multivariable analyses are available in Table 4.
Predictors of disability and imaging outcomes at 10 years from first symptom.

Significance levels: ∼0.1,
Discussion
In our cohort of patients with MS, relapses in the first three years recovered better in younger patients, who were on disease-modifying treatment at relapse onset, were later in their disease course, had no bowel or bladder symptoms (multivariable and univariate analyses), less severe symptoms, lower BMI and were treated with steroids (univariate analyses). For each incomplete recovery in the first three years, the EDSS score and timed 25-foot walk at 10 years increased by 0.6 points and 0.5 seconds, respectively.
In this cohort, 44.6% of early relapses left a residual deficit after at least 6 months. It has been established that, even in early stages, relapses often leave residual deficits, with the percentage of early relapses with incomplete recovery reported in different cohorts as 34%, 9 42%, 5 49.9%, 7 53.3%, 8 54.5%, 19 and 58.6%. 10
The most common treatments in our cohort, interferons and glatiramer acetate, were associated with improved relapse recovery. Previous post hoc clinical trial analyses have noted improved recovery as an effect of teriflunomide, 20 natalizumab, 21 and peginterferon β-1a, 22 but not fingolimod. 23 More importantly, a follow-up analysis of an interferon beta-1a trial underlined the importance of immediate treatment initiation in patients with incomplete first episode recovery, in order to prevent 10-year disability. 8 Older studies pooling treated patients failed to show an effect.11,19 Whereas previous studies have shown declining recovery with subsequent relapses,7,24 we found improved recovery for later relapses within the three years. This could represent confounding by DMT, which improved recovery in later relapses, decrease in EDSS sensitivity, or underestimation of first episode recovery due to a lack of baseline neurologic examination before the first symptom: all first attacks were assumed to have had a normal baseline examination, possibly resulting in subclinical, preexisting signs being attributed to the first episode. In order to overcome this, we confirmed residual disability associated with the first episode using the follow-up FSS and neurologic examination. Our univariate analysis showed a beneficial effect of steroid treatment on recovery. Previous studies have shown either a lack of effect, 25 or an inconsistent improvement. 24
The observed decline in recovery with increased age at onset has been shown previously in CLIMB 26 and other cohorts,3,9,24 whereas two studies in Italian cohorts found no age effect.9,19 Interestingly, children with MS recover better than adults. 26 Bowel/bladder symptoms were also associated with incomplete recovery. Previous studies have found worse recovery in polysymptomatic relapses9,10 and relapses localizing to the brainstem, cerebellum or spinal cord.13,24 Increased BMI was significantly associated with incomplete recovery in the univariate analysis. This is an interesting finding not reported before. Previous studies have also repeatedly confirmed that more severe relapses recover worse.5,7,9–11,13,19,23,24,26 Our study was not designed to objectively assess relapse severity, as a peak disability assessment was not required. Nevertheless, the univariate analysis showed worse recovery in relapses subjectively classified by clinicians as severe.
Our results demonstrated that the number of early relapses with incomplete recovery is a significant predictor of a patient’s 10-year disability, as measured by both EDSS and timed 25-foot walk, two valid, clinically relevant tools.27,28 Incomplete recovery from initial relapses has previously been shown to predict faster accrual of disability, 2 5-year disability, 3 and the duration of EDSS progression from 0 to 3, and from 3 to 6. 12 Importantly, incomplete recovery can also predict earlier transition to secondary progressive disease. 13 Finally, later EDSS increases correlate with the EDSS score 15 years later. 29 We now provide evidence that the recovery at the earliest clinical stages -sometimes before diagnosis of MS is established- is an important predictor of 10-year disability. The number of complete recoveries was associated with lower 10-year EDSS in the univariate model only. Age at first symptom was also a predictor of 10-year EDSS and timed 25-foot walk, validating a well-known age effect on long-term disability.2,3 Higher BMI was associated with higher EDSS and timed 25-foot walk. There is preliminary evidence that BMI is associated with disease progression and disability.30,31 The timed 25-foot walk was lower in males, likely a physiological effect. With regard to neuroimaging, BPF was negatively associated with age, indicating age played a role in predicting subsequent brain atrophy. 32 Male sex also approached statistical significance in predicting a risk for atrophy (p = 0.058). There is evidence that age-related atrophy may be more prominent in men, 33 although this interaction between sex and age is complex and could be explained by differences in brain size. 34 T2-hyperintense lesion volume was associated only with smoking history, validating a number of previous studies. 35 There was no association between relapse recovery and subsequent risk for development of brain atrophy and MRI lesion progression. This finding has not been reported before.
The increase in 10-year disability with every incomplete recovery in the first three years indicates that incomplete recoveries predispose to worse long-term outcomes, either due to accumulating disability or a common, aggressive pathophysiology. The growing evidence on the association between recovery and long-term disability should inform clinical decision-making: patients with incomplete recovery may require closer follow-up and more aggressive treatment. More importantly, early initiation of disease-modifying treatment can improve recovery, preventing long-term disability. These findings should also inform the design of clinical trials, which should include relapse recovery as an endpoint and account for it as a possible confounder. 8 Moreover, basic and translational research on the pathophysiology underlying recovery could lead to the discovery of recovery biomarkers and the development of therapies improving recovery.
Recovery from relapses is a difficult parameter to measure. Our retrospective cohort assessed recovery based solely on baseline and follow-up examinations. The residual EDSS increase has been used as a measure of recovery in many studies, including post-hoc treatment analyses,5–7,19,22,23 and has been validated as a surrogate of recovery using the affected system ΔFSS change. 22 In order to assess all relapses without ample relapse-free intervals, we employed a predefined combination of metrics, prioritizing objective outcomes and using subjective perceptions only when needed. We extended the recovery interval to 6 months based on conservative estimates from previous studies.6,7,23
The strengths of this study derive from the extensive data available in CLIMB. The cohort included 360 patients, longitudinally followed for more than 8 years with examinations and MRI. They represent modern day patients who received regular standard of care, with no experimental intervention relevant to this study. The patients’ low EDSS at 10 years is in line with recent reports from CLIMB 36 and other cohorts, 37 indicating a gradual decrease in long-term disability in the treatment era. 38 Our study also presents several limitations. Firstly, it is not a prospective study. The cohort was skewed towards white and female patients, possibly lacking the power to detect a potential race or sex effect. Sample size did not permit validation of our results in a second cohort. Baseline 3 T MRI scans from early disease were not available in order to calculate longitudinal change in MRI metrics. The assessment of recovery was not based on one parameter, possibly introducing classification or observer bias, whereas first episode recovery may have been underestimated as discussed above. Functional recovery was determined based on the neurologic examination and not more nuanced testing such as visual fields or evoked potentials. Given the 10-year longitudinal aspect of the study, most patients were on beta-interferon or glatiramer acetate treatment in their early disease, and we therefore cannot comment on the effects of newer, highly effective therapies on relapse recovery. Finally, challenges relating to the EDSS scale have been extensively discussed in the literature: is not linear, it is affected by inter-rater variability, subjective patient perceptions and symptomatic treatments, and higher disability reduces its sensitivity. 7
Conclusions
Recovery from relapses in the first 3 years of MS was better in younger patients and patients who received disease-modifying treatment and is associated with lower 10-year disability. These findings could directly inform clinical decision making, clinical trial design and translational research.
Supplemental Material
sj-pdf-1-mso-10.1177_20552173211015503 - Supplemental material for Relapse recovery in multiple sclerosis: Effect of treatment and contribution to long-term disability
Supplemental material, sj-pdf-1-mso-10.1177_20552173211015503 for Relapse recovery in multiple sclerosis: Effect of treatment and contribution to long-term disability by Marinos G Sotiropoulos Hrishikesh Lokhande Brian C Healy Rohit Bakshi, Howard L Weiner and Tanuja Chitnis in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
sj-pdf-2-mso-10.1177_20552173211015503 - Supplemental material for Relapse recovery in multiple sclerosis: Effect of treatment and contribution to long-term disability
Supplemental material, sj-pdf-2-mso-10.1177_20552173211015503 for Relapse recovery in multiple sclerosis: Effect of treatment and contribution to long-term disability by Marinos G Sotiropoulos Hrishikesh Lokhande Brian C Healy Rohit Bakshi, Howard L Weiner and Tanuja Chitnis in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors wish to thank Mark Anderson, MS for his role in managing the Brigham MS Center Research Database, as well as Taylor Saraceno, BS for her assistance in manuscript preparation. The authors thank the CLIMB study staff for their efforts in collecting and collating data used in this manuscript.
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marinos G Sotiropoulos has received research support from Mallinckodt. Hrishikesh Lokhande has received research support from Verily Life Sciences. Brian C Healy has received research support from Merck Serono, Verily Life Sciences, Analysis Group, Novartis and Genzyme. Bonnie I Glanz has received grant support from Merck Serono and Verily Life Sciences. Rohit Bakshi has received consulting fees from Bayer, Biogen, BMS/Celgene, EMD Serono, Genentech, and Novartis, and research support from BMS/Celgene, EMD Serono, and Sanofi-Genzyme. Howard L Weiner reports grants from National Institutes of Health, grants from National Multiple Sclerosis Society, Verily Life Sciences, EMD Serono, Teva Pharmaceuticals, Sanofi Genzyme, and Novartis; grants and consulting fees from Biogen, Genentech, Inc, Tilos Therapeutics, and he sits on the advisory boards of Everest Medicines Limited, Magnolia Therapeutics, Tiziana Life Sciences, IM Therapeutics, MedDay Pharmaceuticals, and vTv Therapeutics, outside the submitted work. Tanuja Chitnis has served on advisory boards for Biogen, Novartis, and Sanofi-Genzyme; has participated in clinical trials sponsored by Sanofi-Genzyme and Novartis; has received research support from the Department of Defense, National MS Society, Guthy Jackson Charitable Foundation, Novartis, Octave, Serono and Verily.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank Mallinckrodt Pharmaceuticals (IIR #5163, Chitnis), the National Multiple Sclerosis Society, and the Nancy Davis Center Without Walls for their support of the CLIMB study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.