
Abstract
Background
It is unclear whether EDSS is responsive to disability worsening in advanced MS.
Objective
To explore the dynamics of disability worsening in persons with advanced-stage MS (EDSS ≥5.5) using three disability worsening definitions (EDSS, Rivermead Mobility Index (RMI), 9-Hole Peg Test (9-HPT)).
Methods
EDSS-, RMI- and 9-HPT-based disability worsening were assessed over a minimum of two years in a cohort of 286 persons with advanced MS attending inpatient rehabilitation using Kaplan-Meier Curves and multivariable Cox regression. Furthermore, the correspondence between EDSS-, RMI- and 9-HPT-based disability worsening was analyzed.
Results
Disability progression was observed in 49% (9-HPT), 52% (EDSS) and 53% (RMI), with 9-HPT-based worsening slightly lagging behind. The Multiple Sclerosis Severity Score (MSSS) was the only consistent factor predicting disability worsening based on all three definitions (EDSS: hazard ratio 1.48 [1.30;1.68]; RMI: 1.12 [0.99;1.27]; 9-HPT: 1.36 [1.18;1.57]). Correspondence between EDSS and the other definitions (9-HPT and RMI) was 44.3% and 55.7% at time of EDSS progression and 65.1% and 72.5% overall, respectively.
Conclusion
In persons with advanced-stage MS, half still developed disability worsening in different functional systems over a median of 6 years. MSSS seems a valid predictor for disability worsening in all three outcome measures in advanced MS.
Introduction
MS is known to lead to progressive impairments over time. However, the great variability of disease expression with respect to symptomatology and progression speed hamper individual predictions of the future disease course. This multi-faceted disease presentation also entails the lack of a universally accepted measurement scale to comprehensively describe functionality or disability status. For example, the widely employed Extended Disability Status Scale (EDSS) is heavily geared towards the assessment of gait mobility, thereby ignoring upper limb functions or symptoms such as fatigue or depression. The EDSS is further criticized because it suffers from substantial inter-rater variability.1,2 Moreover, most instruments to measure impairments, including EDSS, were developed in persons with mild to moderate MS, and hence the understanding of disease progression in persons in advanced stages or with a more severe disease course is still partial.3–10
To make further progress in understanding different disease course expressions, it is important to discern how established impairment measurements behave across the full spectrum of disease presentation (i.e. from mild to very severe impairments), which only few studies have attempted so far. 11 This aspect is particularly pertinent for persons with (primary or secondary) progressive multiple sclerosis and is gaining relevance with the advent of new specifically targeted medications. Treatment response monitoring requires outcome measures that are responsive in persons with MS (PwMS) with more advanced impairments. Against this background, this study’s aims were as follows.
First, we aimed to describe and assess the dynamics of disability worsening based on EDSS and two other outcome measures (nine-hole peg test (9-HPT), Rivermead Mobility Index (RMI)) in persons attending a Swiss in-patient neuro-rehabilitation with EDSS ≥5.5. 10
Second, we sought to compare the dynamics and convergence of the two disability assessments relative to EDSS. These analyses were performed at two time-points: at time of EDSS-based disability worsening and at the last available follow-up.
Methods
Setting of data collection
The data was collected at the Berner Klinik Montana in Crans-Montana, Switzerland from 1992 to 2015. The Berner Klinik is a rehabilitation clinic with around 250 PwMS in in-patient rehabilitation each year. This corresponds to about 35% of all MS-related in-patient rehabilitations in Switzerland. The entire spectrum of PwMS is covered with a preponderance of the progressive forms. The MS neurorehabilitation consists generally of a three-week program with individualized therapy consisting of a combination of physiotherapy, occupational therapy, speech therapy, and nutritional counselling, among others. The Berner Klinik is a member of the rehabilitation in multiple sclerosis (RIMS) which is a European network for best practice and research in the rehabilitation of MS. [REF: Website https://www.eurims.org/]
Outcome measures
The Berner Klinik applies a battery of tests to assess the progress made during the rehabilitation stay. Three outcome measures were selected for the present study because they were systematically assessed in all in-patient rehabilitation stays. The first was the EDSS as the most used progression measure in clinical research. It is responsive towards gait mobility and was assessed by a neurologist.1,2,10 The nine-hole peg test (9-HPT) was the second, a manual dexterity tool executed for both hands individually and part of the MSFC.4,12 The third was the Rivermead Mobility Index (RMI), which assesses whether specific mobility tasks can be performed. While measuring mobility, it is less gait-focused compared to the EDSS and has been validated for use in persons with MS to some extent.13,14 All information was recorded in a systematic fashion by an experienced and well-trained MS team for administrative purposes. A more detailed description of the assessments can be found elsewhere. 10
Inclusion criteria
Inclusion into this study required the availability of at least three complete, concomitant assessments of RMI, 9-HPT, and EDSS, obtained over a period of at least 2 years. Moreover, only persons with an EDSS ≥5.5 at the first in-patient rehabilitation stay were analyzed. As shown in the flowchart in Figure 1, further inclusion criteria pertained to completeness of additional information (other than EDSS, RMI and 9-HPT).

Flowchart of persons with MS included in the study.
Statistical analysis
Baseline characteristics were analyzed descriptively for the full population. The following characteristics were compared at the first in-patient rehabilitation stay (baseline): age, duration since MS diagnosis, gender, type of MS (secondary, primary progressive, unspecified progressive (chronic) form), EDSS, RMI, 9-HPT, Multiple Sclerosis Severity Score (MSSS).15,16 Age was transformed into restricted cubic splines because 1) the exact shape of the relationship between age and the different outcomes of interest is generally unknown and 2) the factor age was not the primary focus of study. Therefore, age splines were just used for confounder adjustment but not interpreted further.
Disability worsening in terms of RMI, 9-HPT, and EDSS was determined according to the following algorithm. 17 Along the established progression cutoffs, EDSS worsening was defined as an increase of 0.5 points from baseline, and confirmed by a second EDSS measurement at least 6 months later for persons with a baseline EDSS ≥6 (and by 1 point for baseline EDSS 5.5). For the 9-HPT, a 20% increase in time (seconds) to complete the task was considered a worsening if confirmed at a second in-patient stay at least 6 months later. 17 As no data on minimal clinically important differences could be found in the literature for RMI, a threshold of 2 units was chosen, corresponding to the standard-deviation of RMI changes over a one-year period found by another observational study.18,19 The RMI increase also needed to be confirmed on the subsequent visit.
Time-to-event methods were utilized to address study goal 1 of describing the disability worsening dynamics. Follow-up time started at the first in-patient rehabilitation stay at the Berner clinic (baseline) and ended at the occurrence of the confirmed disability worsening (depending on the analyzed outcome measure) or the last follow–up, whichever occurred first. Time to worsening was assessed using Kaplan-Meier plots and multivariable Cox regression, investigating the following baseline characteristics (age (splines), duration since MS diagnosis (=disease duration), sex, type of MS, MSSS, EDSS, use of disease-modifying treatment (DMT)). Model selection followed an algorithm described elsewhere, which is based on a selection criterion of an Akaike Information Criterion score reduction of ≥2. 20 Based on this rule, disease duration was eventually not included in the model. The proportional hazards assumption was verified using Schoenfeld residuals.
The second study goal aimed to investigate the overlap between EDSS-based disability worsening (which is currently still considered the clinical gold standard) and 9-HPT- and RMI-based disability worsening. Descriptive statistics were employed to characterize persons with and without EDSS-based disability worsening. Additionally, the overlap of disability worsening based on EDSS and other outcome assessments was assessed in terms of sensitivity, defined as the percentage of persons with disability worsening based on 9-HPT or RMI as a fraction of all persons with EDSS-based disability worsening. Sensitivity was estimated both at time of EDSS worsening and over the complete follow-up period.
Analyses were conducted in Stata 13 (Stata Corp., College Station TX, USA.).
The re-usage of these data was approved by the Ethics Committee Zurich (BASEC. 2017-00077), who also issued a waiver for the retrospective retrieval of informed consent.
Data availability
The data of this study are available from the corresponding author on reasonable request.
Results
Out of 1931 persons with MS being treated at the rehabilitation clinic between 1992 and 2015, 286 met all inclusion criteria for this study (Figure 1). Of those, 61% were females and the median age was 51 years (Table 1). Per definition, these persons had an advanced MS disease status: the median baseline EDSS was 6.5, 72% of individuals were classified with a secondary progressive MS, and at baseline the median disease duration was 13 years. The median follow-up duration was 6 years [interquartile range (IQR) 4-10 years], and the median number of in-patient rehabilitation stays was 5 [IQR 3–7], data not shown.
Baseline characteristics of persons with MS included in the study.

Note: Baseline was defined as the first recorded in-patient rehabilitation stay.
EDSS: Expanded Disability Status Scale; DMT: disease-modifying treatment; IQR: inter-quartile range; MSSS: Multiple Sclerosis Severity Score; RMI: Rivermead Mobility Index; 9-HPT: 9-Hole Peg Test.
Dynamics of disability worsening by different outcome measures
In total 149 of 286 (52.1%) persons experienced confirmed disability worsening as measured by EDSS, 141 (49%, 9-HPT) and 153 (53%, RMI) experienced confirmed disability worsening based on the other two respective measurements. The dynamics of worsening are illustrated in Figure 2. Median disability worsening times were 5.2 years for the EDSS, 5.8 years for the RMI, and 6.3 years for the 9-HPT. The Kaplan-Meier curves in Figure 2 underscore these findings: whilst the RMI progresses faster in the beginning and after about four years is matched by the EDSS curve, the curve for 9-HPT lags behind. The patterns in the late follow-up (≥6 years) should not be overestimated however due to the limited sample sizes.

Kaplan-Meier plots of disability worsening as measured by three outcome measures.
Additionally, factors associated with the three types of disability worsening were investigated using multivariable Cox regression models (Table 2, univariable results are displayed in the Appendix, Table S1). For the EDSS-worsening outcome, a higher baseline EDSS was associated with a decrease in worsening probability (Hazard Ratio HR 0.38 95% confidence interval (CI) [0.27; 0.52]), whereas a higher MSSS was associated with an increased risk (HR 1.48, 95%-CI [1.30; 1.68]). Moreover, still receiving DMT at baseline was also associated with a risk decrease (HR 0.62, 95%-CI [0.40; 0.94]). In the RMI analysis, male gender (HR 1.48, 95%-CI [1.06; 2.08]) and higher MSSS (HR 1.12, 95%-CI [0.99; 1.27]) were associated with disability worsening. When modelling disability worsening based on 9-HPT, also male gender (HR 1.64, 95%-CI [1.15; 2.35]) and higher baseline MSSS (HR 1.36, 95%-CI [1.18; 1.57]) were associated with increasing risks for disability worsening.
Multivariable Cox regression of EDSS, RMI or 9-HPT based disability worsening.

Note: All characteristics were assessed at baseline, that is, the first recorded in-patient rehabilitation stay.
DMT: disease-modifying treatments; EDSS: Expanded Disability Status Scale; MSSS: Multiple Sclerosis Severity Score; RMI: Rivermead Mobility Index; 9-HPT: 9-Hole Peg Test.
Concordance of outcome measures with EDSS-based disability worsening
As shown in Table 3, persons with EDSS-based disability worsening differed in several aspects from persons without: they were less frequently female (52% vs. 71%), somewhat younger at baseline (median 51 vs. 53 years) and less frequently had a secondary progressive MS (68% vs 77%). However, median follow-up durations were also markedly different between the two groups, with a median of 5.2 years in the group without and 7.9 years in those with EDSS-based disability worsening.
Comparison of groups who did not experience EDSS-based disability worsening vs. persons who did experience a worsening.
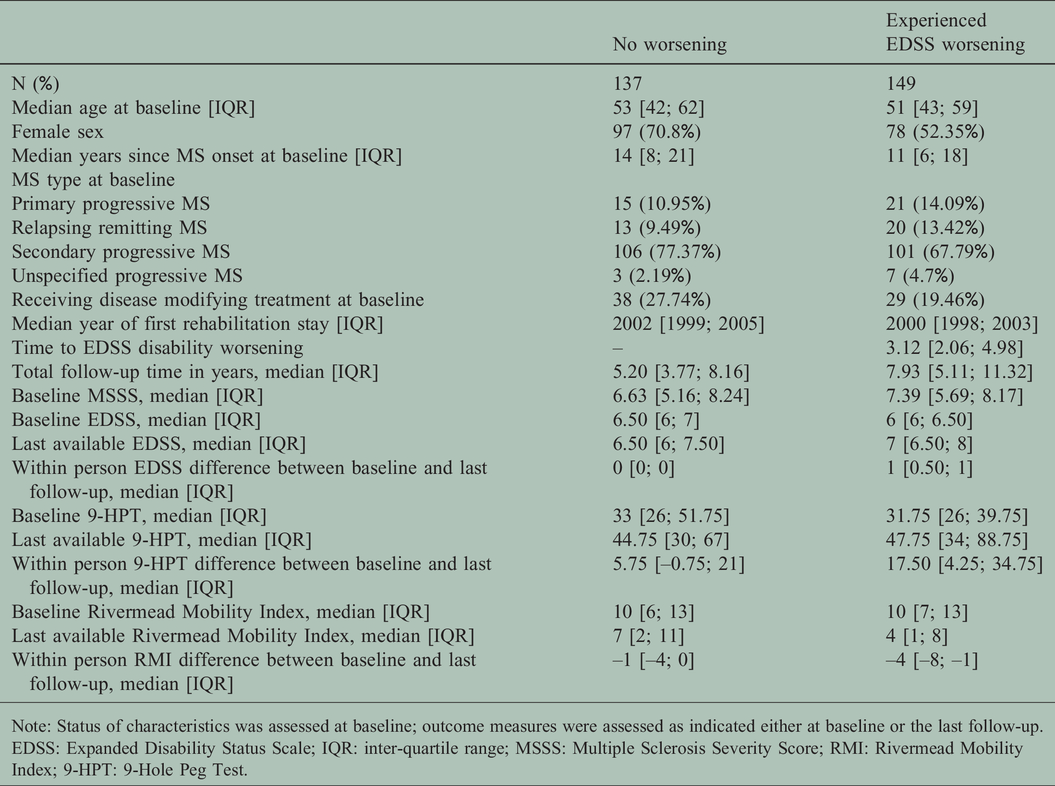
Note: Status of characteristics was assessed at baseline; outcome measures were assessed as indicated either at baseline or the last follow-up.
EDSS: Expanded Disability Status Scale; IQR: inter-quartile range; MSSS: Multiple Sclerosis Severity Score; RMI: Rivermead Mobility Index; 9-HPT: 9-Hole Peg Test.
Further notable, the baseline MSSS was higher in persons with worsening (median 7.39 compared with 6.63 in persons without worsening), thus suggesting an overall faster disease progression already before baseline. Over the full observation period, EDSS-defined disability worsening was also associated with a larger decrease of RMI scores (median loss of 4 scores compared to 1 score among persons without worsening), and a larger worsening of the 9-HPT (median increase of 17.5 s vs 5.75 s).
We further assessed the concordance of 9-HPT and RMI-based disability worsening with EDSS-based worsening. The results are shown in Table 4 and illustrate that of 149 persons with EDSS worsening, only 66 (44.3%) also had a confirmed 9-HPT worsening at the time of EDSS worsening (sensitivity). When assessing progression status at the last follow-up visit, 97 of 149 persons (65.1%) also had a 9-HPT worsening at some point during the observation period. Corresponding numbers for the RMI were higher, namely 83 (55.7%) concordance at time of EDSS-worsening and 108 (72.5%) when considering the full observation period. Furthermore, of 141 persons with 9-HPT progression, 44 (31.2%) showed no EDSS progression. For RMI, 45 (29.4%) showed no EDSS progression.
Correspondence of worsening status between EDSS and different outcome measures (9-HPT and RMI) at time of EDSS worsening and over total follow-up (i.e. ever experienced worsening over total observation period).

Note: Numbers in table reflect the number of individuals by worsening status.
EDSS: Expanded Disability Status Scale; OM: Outcome measure; RMI: Rivermead Mobility Index; 9-HPT 9-Hole Peg Test.
Discussion
Using a database of routinely collected rehabilitation outcome measures from 286 persons with at least three in-patient neurorehabilitation stays, this study investigated the dynamics of disability worsening using three different outcome measures, namely EDSS, RMI, and 9-HPT. In particular, over a median follow-up duration of 6 years, more than half of all studied persons with MS had confirmed disability worsening as measured by EDSS, 9-HPT, and RMI. Our analysis further revealed that 44% (9-HPT) and 56% (RMI) of PwMS with confirmed EDSS-based disability worsening also had a worsening in the other respective measure at the time of EDSS-based disability worsening. When considering the full observation period, 65% (9-HPT), resp. 73% of persons with EDSS-based disability worsening also had a worsening in the other outcome measure. Moreover, MSSS at baseline turned out to be a baseline predictor for disability worsening based on any of the three outcome measures, thus confirming the predictive properties of this score.
Overall, these findings provide novel insights into the dynamics of disability worsening, as measured in different outcome domains, in a population that is rarely studied. Comparisons with other databases indicate that the studied population contains a substantial fraction of persons with comparatively fast progressive MS. For example, a study reported only around one quarter of participants with impairments after a disease duration of 10-12 years that are as severe as in the studied population. 21 Along the same lines, a recent analysis also comparing the dynamic of different disability worsening measures included only around one quarter of patients with impairments as severe as in our population at baseline. 22
Our findings fall well in line and extend previous studies assessing the evolution of different outcome assessment methods. The largest analysis performed to date with over 12’000 MS trial participants corroborates our observation that 9-HPT-based disability worsening tends to lag behind EDSS-based disability worsening definitions. 17 Our study adds to these findings by confirming these results in a more impaired study population and over a longer time scale.
Moreover, a different study found – while following 156 patients with a new diagnosis over 10 years – that persons with non-relapsing disease courses exhibited markedly faster deterioration of different functional domains, particularly gait mobility, physical function or motor function. 11 Our study was unable to differentiate findings by MS form potentially due to small numbers. Meanwhile, MSSS – which is also responsive to MS type 15 – emerged as a potential predictor for disability impairments in the time-to-event analysis. This latter finding that MSSS was predictive for EDSS-, 9-HPT- and RMI-defined disability worsening is noteworthy.
Our findings also extend studies of different outcome measures in rehabilitation settings, which confirm the good psychometric properties and responsiveness of RMI.18,19 In particular the study by Baert et al found RMI to be sensitive to changes in moderately to severely impaired patients. Therefore, the changes in outcome measures observed by this study are likely also clinically relevant. 19 Furthermore, because RMI also has a strong gait component, the correspondence between EDSS- and RMI-based disability worsening dynamics was largely expected. 15
Our study has strengths, but also limitations. To our knowledge, our study includes one of the largest samples of more severely impaired persons with MS and one of the longest follow-up durations of a study performed in a rehabilitation setting to date. A further strength is that the population seen at the Berner Clinic – one of the major centers for MS rehabilitation in Switzerland – is largely representative for persons with MS attending in-patient rehabilitation in general, being these treatments covered by the Swiss basic health insurance. One important limitation is that the data were collected mainly for administrative purposes and are dependent on whether and when the clinic was attended. Moreover, certain variables were only partially recorded, such as only whether disease-modifying treatments were used, but not the type nor duration. Further limitations were imposed by changes in recorded outcome measures over the observation period. Because the Functional Independence Measure (FIM), or the 25-Foot Walk Test (25FTW) were not systematically collected over the full study period, they could not be assessed. Additionally, the differing length of follow-up between the persons with confirmed EDSS-progression and those without has to be noted.
To conclude, this study describes long-term disability worsening in persons with already advanced impairments. Furthermore, MSSS seems to be informative for disability worsening risk stratification even in persons with advanced MS and across different dimensions of body functioning.
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Marco Kaufmann https://orcid.org/0000-0002-4810-7734 Laura Barin ![]()
Supplemental material
Supplemental material for this article is available online.