
Abstract
Background. Ambulation impairment is a major component of physical disability in multiple sclerosis (MS) and a major target of rehabilitation programs. Outcome measures commonly used to evaluate walking capacities suffer from several limitations. Objectives. To define and validate a new test that would overcome the limitations of current gait evaluations in MS and ultimately better correlate with the maximum walking distance (MWD). Methods. The authors developed the Timed 100-Meter Walk Test (T100MW), which was compared with the Timed 25-Foot Walk Test (T25FW). For the T100MW, the subject is invited to walk 100 m as fast as he/she can. In MS patients and healthy control volunteers, the authors measured the test–retest and interrater intraclass correlation coefficient. Spearman rank correlations were obtained between the T25FW, the T100MW, the Expanded Disability Status Scale (EDSS), and the MWD. The coefficient of variation, Bland–Altman plots, the coefficient of determination, and the area under the receiver operator characteristic curve were measured. The mean walking speed (MWS) was compared between the 2 tests. Results. A total of 141 MS patients and 104 healthy control volunteers were assessed. Minor differences favoring the T100MW over the T25FW were observed. Interestingly, the authors demonstrated a paradoxically higher MWS on a long (T100MW) rather than on a short distance walk test (T25FW). Conclusion. The T25FW and T100MW displayed subtle differences of reproducibility, variability, and correlation with MWD favoring the T100MW. The maximum walking speed of MS patients may be poorly estimated by the T25FW since MS patients were shown to walk faster over a longer distance.
Introduction
Although all neurological deficits caused by multiple sclerosis (MS) contribute to a patient’s overall disability, ambulation is recognized as a key factor in determining a patient’s functional status. 1
In therapeutic and rehabilitation clinical trials, the Expanded Disability Status Scale (EDSS) 2 and the Multiple Sclerosis Functional Composite (MSFC) 3 score are the most widely used conventional scores for the quantitative assessment of the impact of MS on neurological status. In the EDSS, ambulation is evaluated through patients’ recall of their maximum walking distance (MWD) and by the observation of the gait disturbances. The MSFC is a composite score that was developed in response to the lack of sensitivity and reliability of the EDSS. It is composed of 3 ratio-interval scales of neurological functions: the 3-Second Paced Auditory Serial Addition Test for cognitive function, the 9-Hole Peg Test for upper limb function, and the Timed 25-Foot Walk Test (T25FW) for the evaluation of leg function/ambulation.
Specific therapies targeting ambulation dysfunction are currently emerging, 4 and gait evaluations are increasingly recognized as primary outcome measures in clinical trials and rehabilitation programs, especially in progressive forms of MS. In this context, the T25FW is by far the most widely used ambulation test. However, even though excellent interrater and intrarater reliabilities have been reported for the MSFC as a composite score, the T25FW component can display variable results, 5,6 especially in more disabled patients with slower walking speeds. This has been attributed to practice effect, test-related fatigue, and motivational issues. 7 In addition, the T25FW has been described as being hampered by low responsiveness and marked floor and ceiling effects, 8 mainly because it is assumed to reflect only speed over a short distance. Ambulation fatigue, 9 spasticity, coordination, and balance are not specifically assessed by the T25FW, which is why more refined gait evaluations have been proposed. 8
To study ambulation characteristics of MS patients on a longer distance and to overcome the limitations of the T25FW, we evaluated the Timed 100-Meter Walk Test (T100MW). In MS, 100-, 200-, 300-, and 500-m distances represent the ambulation range of EDSS milestones 5.5, 5.0, 4.5, and 4.0, respectively. We chose the 100-m distance as the threshold in the EDSS beyond which patients require at least unilateral assistances.
Methods
A total of 141 patients with a diagnosis of relapsing–remitting or progressive MS according to the Poser 10 and McDonald 11 criteria and 104 age- and sex-matched healthy volunteers used as a control group were enrolled in the study.
Both MS patients and controls performed the T25FW and the T100MW. The procedures were approved by the local ethics committee of the Medical Faculty of Liège. All the assessments were made by a certified MS nurse (PC) or by a physical therapist in charge of patients’ rehabilitation programs (PG). All EDSS score were collected by a certified EDSS rater (RP or SB).
The MWD was evaluated as follows: control healthy volunteers all reported a MWD superior to 4000 m, which was considered as “unlimited.” MS patients were asked whether they had the feeling that during the past 4 weeks their average walking performance had been unlimited and whether they thought they could walk for more than 4000 m without aid or rest. If so, they were considered to have an “unlimited” MWD. Patients considering themselves unable to walk more than 4000 m were defined as having a “limited” ambulation and were asked to evaluate as accurately as possible their MWD, that is, the maximum distance they thought they could walk without aid or rest, with a high risk of falling if they went on for a few meters more. Patients who evaluated their MWD as being less than 2000 m were considered to be patients with so-called restricted ambulation. The accurate MWD was measured for patients reporting to be unable to walk more than 500 m.
The T25FW was performed according to the published standardized instructions. 2,6
For the T100MW, a 25-m walk (to be performed 4 times with 3 U-turns) was accurately measured in a corridor of at least 3 m width, devoid of obstacles. Running was prohibited. Patients could use assistive devices if absolutely necessary to perform the test. Ankle–foot orthosis was permitted if worn from onset for all evaluations throughout the trial. The subject was directed to the end of a clearly marked 25-m course (clearly defined on the floor) and instructed to stand just behind the starting line. We pointed out where the 25-m course ended and then instructed the patient as follows: “I’d like you to walk this 25-meter distance 4 times as quickly as possible, but safely. Do not slow down until after you’ve passed the finish line. Ready? Go.” Timing started when the lead foot crossed the starting line. The examiner could not walk along with the patient as he/she completed the task. Timing was stopped when the lead foot crossed the finish line (4 × 25 m). The examiner then recorded the subject’s walking time to within 0.1 second, rounding up or down as necessary. We rounded up to the next tenth if the hundredth of a second’s place was ≥.05, rounded down if the hundredth of a second’s place was <.05 (eg, 55.45″ would round up to 55.5″ but 55.44″ would round down to 55.4″). On the day of the clinical evaluations, rehabilitation sessions or other demanding physical activities did not take place prior to the testing. The 2 sessions of the T25FW were always performed prior to the T100MW. Control healthy volunteers performed the T25FW and the T100MW twice to establish the test–retest intraclass correlation coefficient (ICC).
To evaluate the interrater reliability of the tests, 50 healthy volunteers and 40 MS patients underwent a second evaluation for the T100MW and the T25FW by another rater after a 15-minute resting time.
The mean walking speed (MWS) expressed in meters per second for both tests were obviously calculated by dividing 100 m by the time to perform the T100MW and 7.62 m by the time to perform the T25FW.
A Wilcoxon rank sum test was performed to compare walking test scores in healthy controls and MS patients. Test–retest and interrater reliabilities were evaluated using ICC. 12 The coefficient of variation (standard deviation divided by mean, expressed as a percentage) was used to compare relative variation between the 2 walking tests overall, by limited/restricted ambulation, and within each step of EDSS. The results from the 2 methods were also compared in accordance with the principles described by Altman and Bland. 13 Spearman rank analyses were used to assess the strength of the correlation between walking tests, EDSS, and MWD, and the coefficient of determination was obtained from a linear regression excluding outliers. The area under the receiver operator characteristic (ROC) curve provided an overall measure of the accuracy of each walking test in predicting limited ambulation. Last, a t test was used for between-groups comparisons, whereas a paired t test was used for within-group comparisons of the MWS on the T100MW with the MWS on the T25FW. All statistical tests were applied with a 2-tailed analysis and .05 as a level of significance.
Results
A total of 141 MS patients with a mean age of 40.0 ± 12.4 years and an EDSS score ranging from 0 to 5.5 (median = 2.5) and 104 control healthy volunteers with a mean age of 35.4 ± 13.0 years participated in the study (Table 1). We observed that 53 out of the 141 (37.6%) MS patients had a “limited” ambulation defined by an MWD ≤ 4000 m. Forty-four subjects (31.2% of the whole population) had a so-called restricted ambulation, defined by an MWD ≤ 2000 m. The subgroup of MS patients who underwent a second analysis for the interrater ICC calculation and the whole MS patient population had comparable baseline characteristics (data not shown).
Characteristics of Patients and Control Subjects
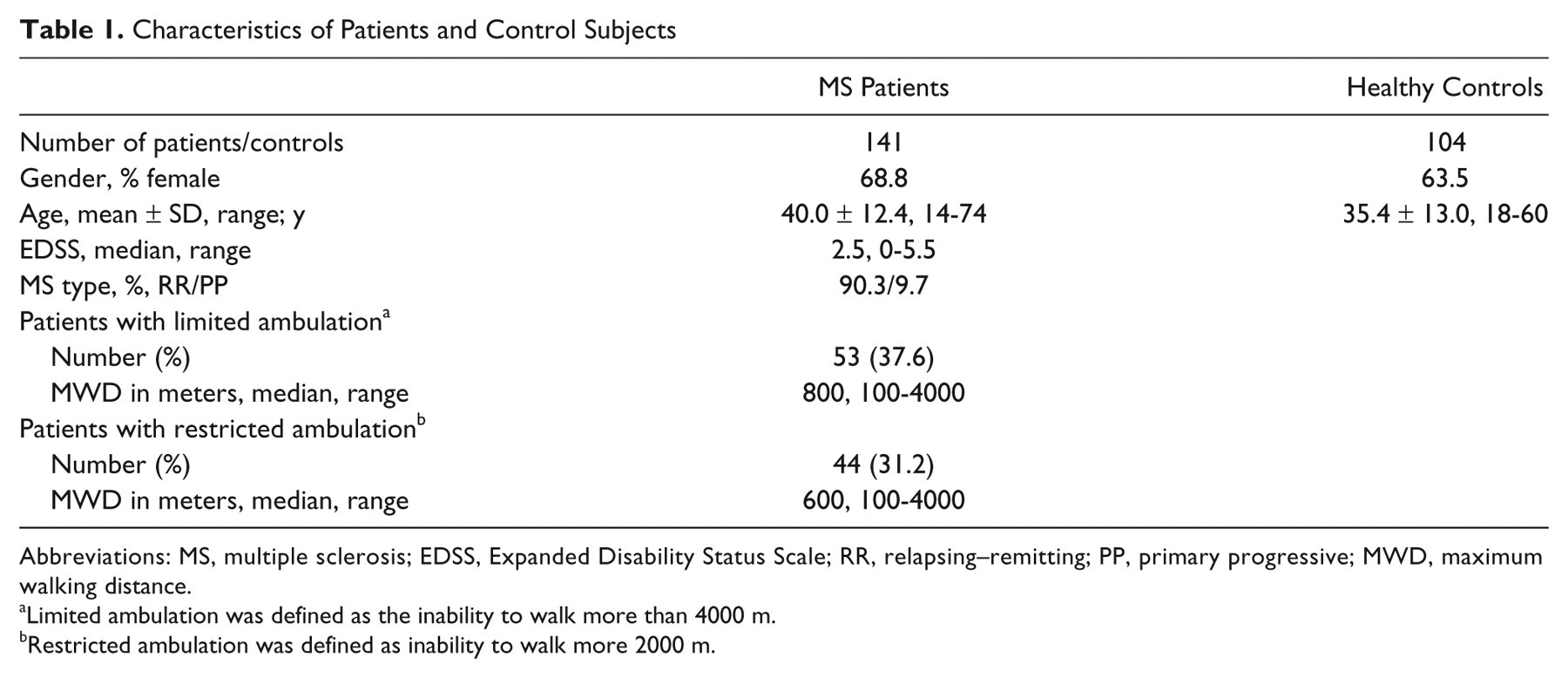
Abbreviations: MS, multiple sclerosis; EDSS, Expanded Disability Status Scale; RR, relapsing–remitting; PP, primary progressive; MWD, maximum walking distance.
Limited ambulation was defined as the inability to walk more than 4000 m.
Restricted ambulation was defined as inability to walk more 2000 m.
In the MS patient population, the time taken to perform the T100MW ranged from 30.6 to 197.9 seconds, with a median of 53.9 seconds, compared with a range of 33.1 to 62.1 seconds in healthy control volunteers with a median of 46.1 seconds (Table 2). The T25FW was performed in a time ranging from 2.9 to 20.7 seconds (median = 4.4 seconds) in MS patients and from 2.8 to 5.2 seconds (median = 3.7 seconds) in healthy control volunteers. Timed performances in both tests were significantly weaker for MS patients when compared with that of healthy control volunteers (both P < .0001). In every subpopulation of MS patients with EDSS scores ranging from 0 to 2.0, 2.5 to 3.5, and 4 to 5.5, both tests were also significantly altered when compared with healthy controls (P = .018, P < .0001, and P < .0001, respectively).
Time Values (Seconds) for the T100MW and the T25FW in Different Population Subsets
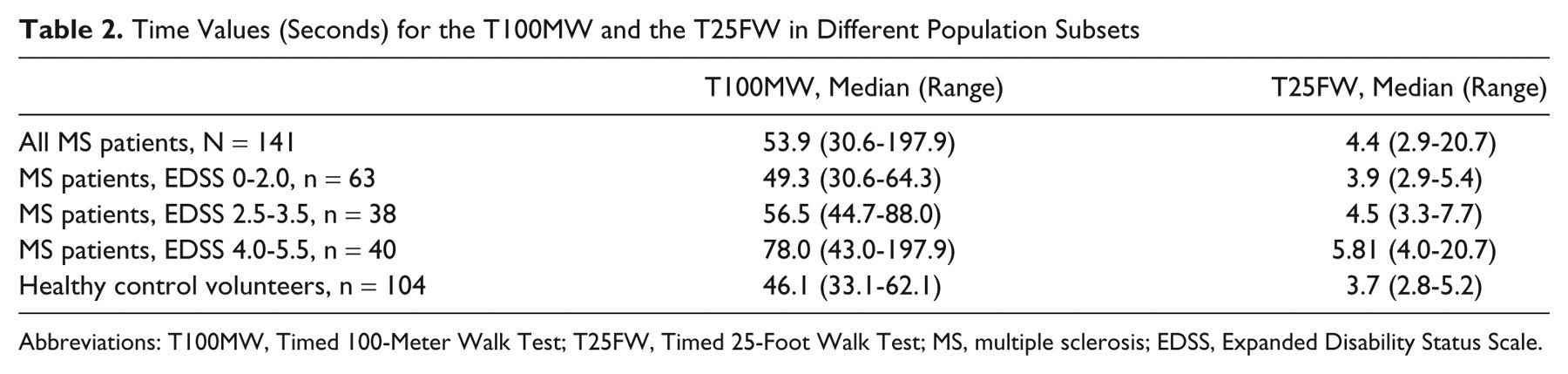
Abbreviations: T100MW, Timed 100-Meter Walk Test; T25FW, Timed 25-Foot Walk Test; MS, multiple sclerosis; EDSS, Expanded Disability Status Scale.
In healthy control volunteers (n = 104 patients), the test–retest ICC was slightly better for the T100MW (0.930) than for the T25FW (0.880). To compare the interrater reliability of both tests, a subgroup of 50 controls and 40 MS patients underwent a second testing by a different rater, and the interrater ICC was calculated. The interrater ICC of the T100MW and T25FW were not substantially different between controls (0.886 vs 0.884, respectively) and MS patients (0.953 vs 0.942, respectively).
The coefficient of variation (CV) was calculated to measure the dispersion of results obtained by both tests. Overall, the T100MW demonstrated less variability with a CV of 41% when compared with a CV of 45% for the T25FW. In patients with limited ambulation, the CVs for the T100MW and T25FW were 41% and 46%, respectively. The same was true for patients with restricted ambulation (T100MW CV = 40% vs T25FW CV = 46%). On examination of CVs by EDSS score, differences between the 2 walking tests were observed among patients with mid-range EDSS scores (2.5-3.5). The T100MW displayed less relative variability in this range of EDSS than the T25FW, with CVs ranging from 5% to 18% for the T100MW (Figure 1A) and from 14% to 25% for the T25FW (Figure 1B). It is important to emphasize that in this particular mid-range EDSS interval from 2.5 to 3.5, considered by definition to be fully ambulatory according to EDSS rules, 42.1% (16/38) of patients had a limited ambulation and 26.3% (10/38) had a restricted ambulation according to our aforementioned criteria.
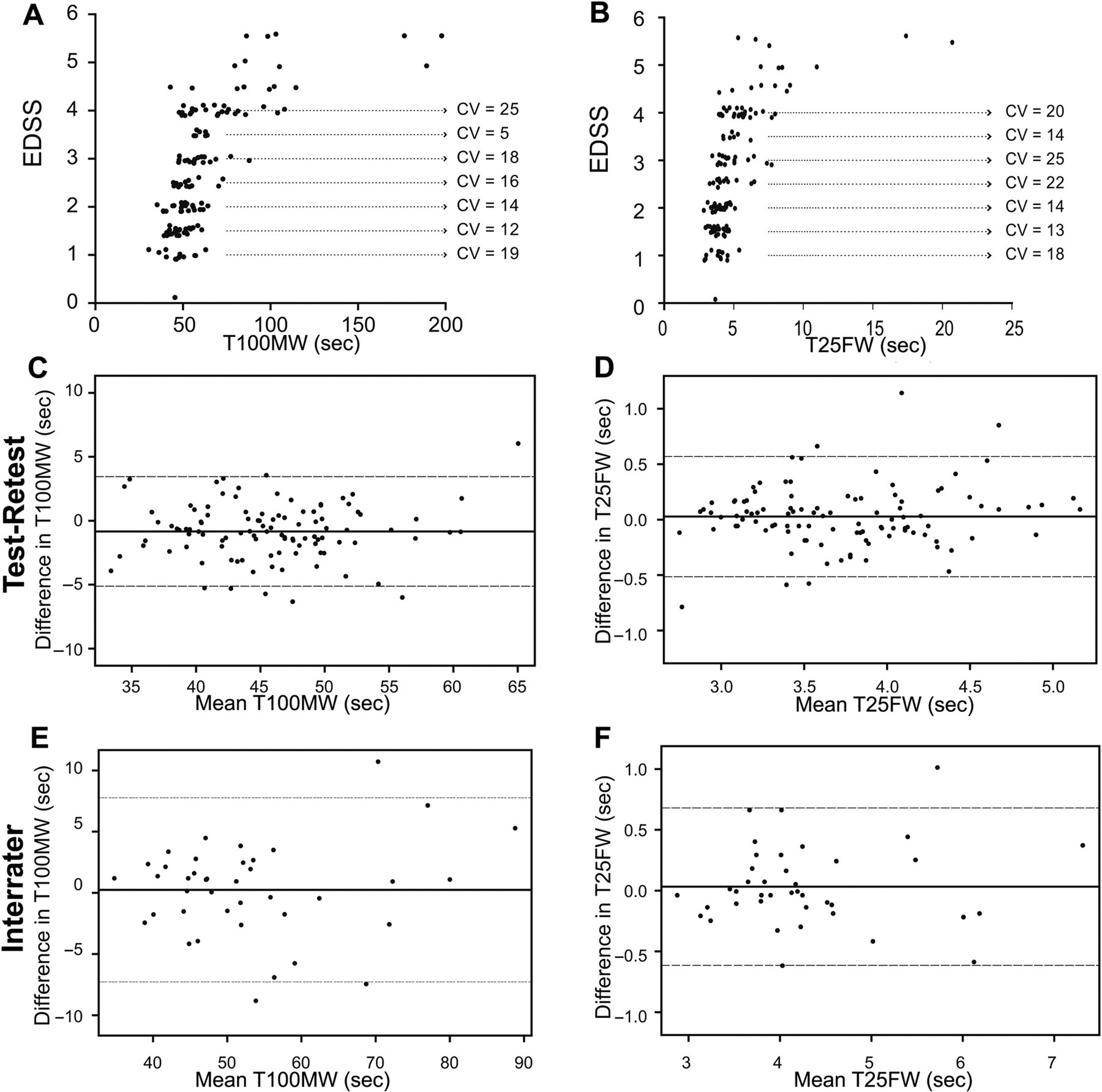
Coefficient of variation (CV, standard deviation divided by mean, expressed as a percentage) showing the distribution of the T100MW (A) and the T25FW (B) values by EDSS step, demonstrating less relative variability for the T100MW in the mid-range EDSS steps (2.5-3.5). Bland and Altman plots showing similar agreement across test and retest between the T100MW (C) and the T25FW (D). Equivalent agreements for the T100MW (E) and the T25FW (F) were also observed between raters.
Bland and Altman (BA) plots with limits of agreement were calculated to assess test–retest and interrater agreements. Between test and retest, the BA plots showed an equally good agreement for each of the walking tests (Figure 1C and D), with a similar number of patients beyond the limits of agreement. Between the raters, mean differences were also near 0 for both tests, with nearly all points falling within the limits of agreement (Figure 1E and F).
Spearman rank correlations (Table 3) showed that the T100MW and the T25FW correlated equally well with the EDSS, with r values of .67 (P < .0001) and .67 (P < .0001), respectively. The overall correlation between the 2 tests was excellent (r = .92, P < .0001). In patients with “limited” or “restricted” ambulation range for whom the MWD could be approximated, the T100MW correlated better with estimated MWD than the T25FW (r = −0.79 vs r = −.71 in the “limited” ambulation population and r = −.77 vs r = −.69 in the “restricted” ambulation population).
Spearman Rank Correlations Between Walking Tests, EDSS, and Walking Distance in Different MS Population Subsets
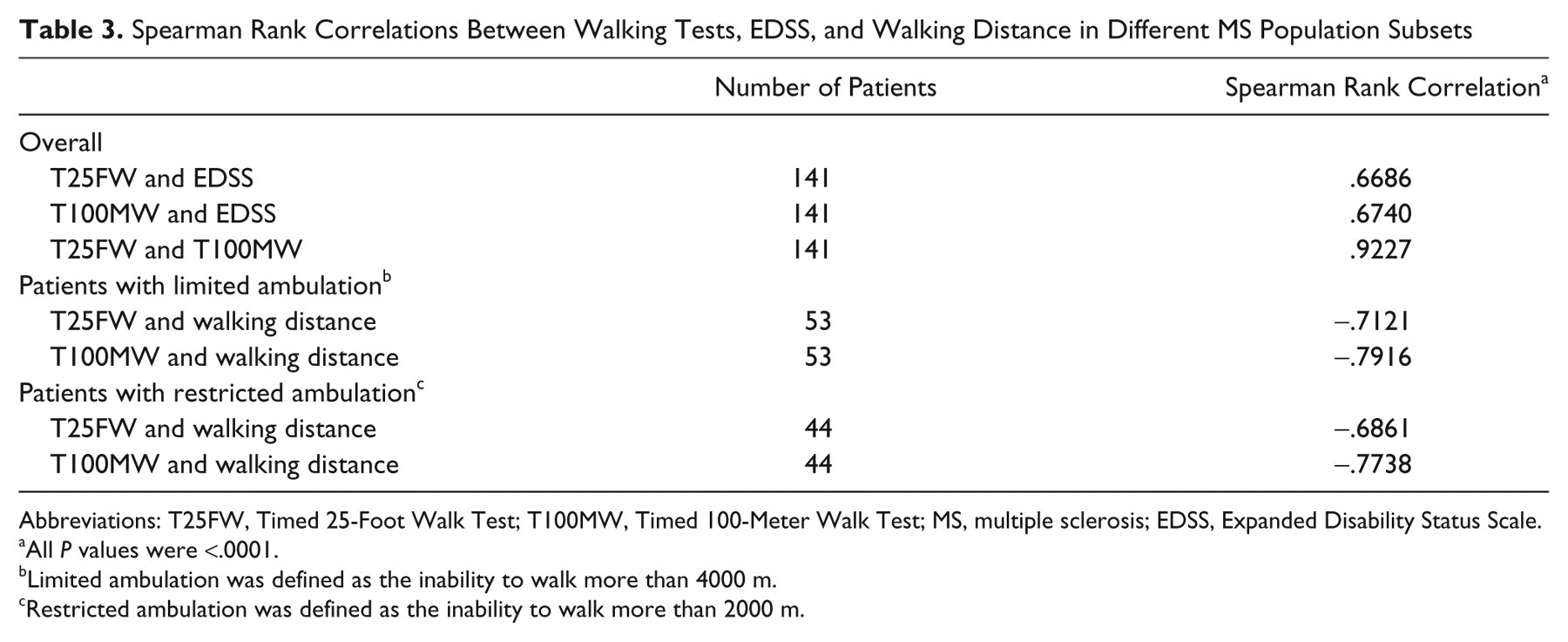
Abbreviations: T25FW, Timed 25-Foot Walk Test; T100MW, Timed 100-Meter Walk Test; MS, multiple sclerosis; EDSS, Expanded Disability Status Scale.
All P values were <.0001.
Limited ambulation was defined as the inability to walk more than 4000 m.
Restricted ambulation was defined as the inability to walk more than 2000 m.
We also calculated the coefficient of determination (R 2) to estimate the proportion of variation in MWD explained by the walking tests in patients with “restricted” ambulation. The variation in MWD was explained for 44.1% with the T100MW (Figure 2A) versus 29.6% for the T25FW (Figure 2B). The area under the ROC curve (AUC) was estimated to compare the trade-off between sensitivity and specificity and the value of both tests in predicting limited ambulation (Figure 2C). We did not find a meaningful difference between the AUC of the T100MW (0.884) and the T25FW (0.881) in the overall population.
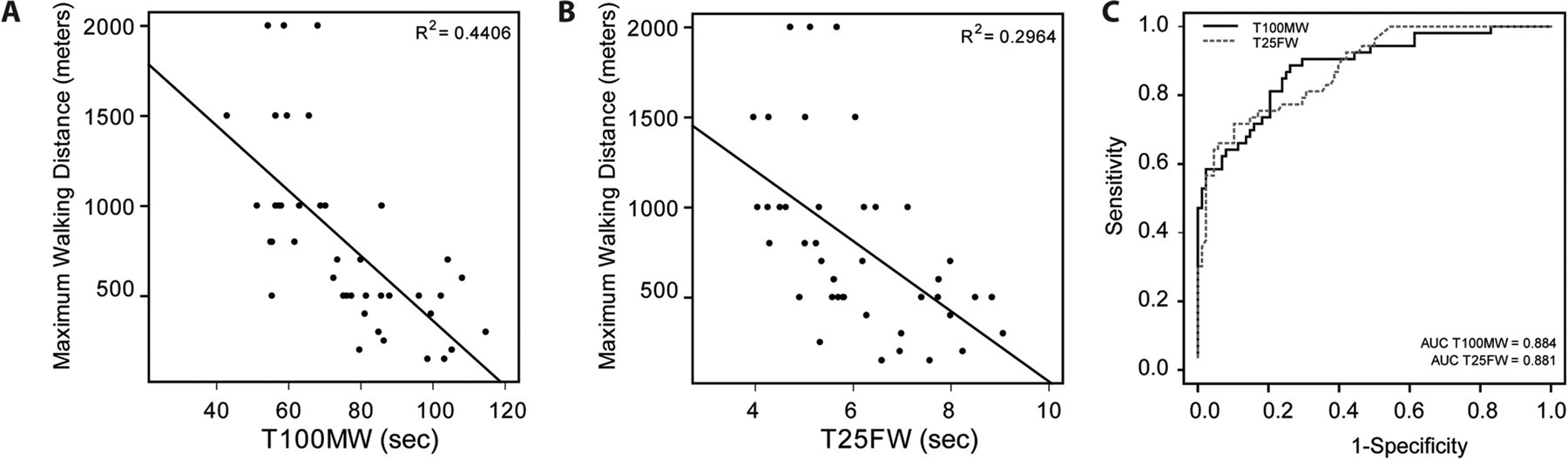
Correlation between the T100MW (A) and the T25FW (B) values and the maximum walking distance (MWD) and corresponding coefficient of determination (R 2). Receiver operator characteristic curve analysis of the T100MW (black line) and the T25FW (dashed grey line) and corresponding area under the curve (AUC) values (C).
Finally, the MWS derived from the T100MW and the T25FW was significantly lower in MS patients (1.8 ± 0.5 and 1.7 ± 0.4 m/s, mean ± SD, respectively) compared with healthy control volunteers (2.2 ± 0.3 and 2.1 ± 0.3 m/s, mean ± SD, respectively); both P < .0001. The evaluation of ambulation impairment through the calculated MWS confirmed that performances were significantly altered for the 2 tests (T25FW and T100MW) in the global MS patient population compared with healthy control volunteers and in subsets of MS patients either with high (4.5-5.5) or low (≤3.5) levels of EDSS status (Figure 3A). Furthermore, we observed in individual performances that the T100MW MWS was very frequently faster than the T25FW MWS in healthy controls (data not shown) and in the MS population, as displayed by a positive absolute difference between both tests in a majority of MS patients (109/141 patients, 77.3% of the MS population, Figure 3B). In agreement with this finding, the mean T100MW MWS was found to be significantly higher than the T25FW MWS, both in healthy controls and in each subgroup of MS patients, defined by an EDSS ≤3.5 or ≥4.0 (P < .0001, P < .0001, and P = .009, respectively; Figure 3A). Consistently, in healthy controls as well as in different subsets of MS patients, the MWS over a 100-m distance was paradoxically ∼7% higher than the MWS over 25 feet, as demonstrated by the mean values of the ratio between respective speeds calculated for each tests in individual subjects (Figure 3C).
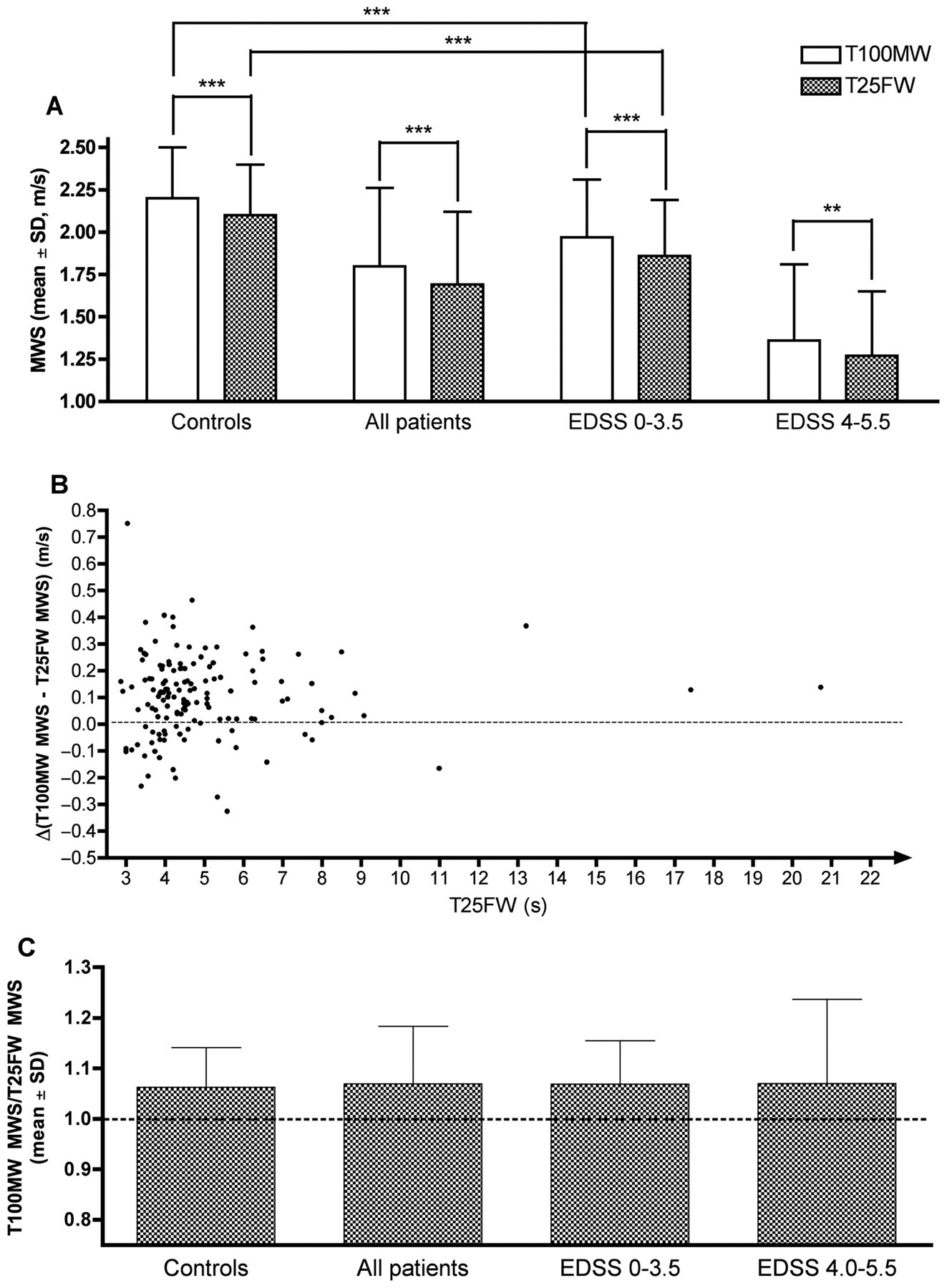
Mean walking speed (MWS) ± standard deviation assessed by the T100MW and the T25FW in healthy control volunteers, in all MS patients and in different subsets of EDSS range in the MS population (A); ***P < .0001; **P = .009; Note that all P values were <.0001 for all respective comparisons of the 2 tests between MS patients and controls but only significant differences between controls and the low EDSS score group were highlighted. Absolute differences between the T100MW and the T25FW MWS in individual MS subjects were expressed as a function of T25FW performances (B). Mean ± standard deviation of T100MW MWS/T25FW MWS speed ratio values in healthy control volunteers, in all MS patients and in different subsets of EDSS scores (C).
Discussion
The present study revealed minor differences favoring the T100MW over the T25FW, and a paradoxically higher MWS on the T100MW, both in control healthy subjects and in distinct subsets of our MS population.
The variability of the T25FW is related to different factors: practice effect, precision of the examining technician, motivational issues, and the level of accelerating capacity during the very first meters of the test. As a matter of fact, it can take half of the test for many patients to reach their maximum walking speed on a 25-foot-long distance, since the patient is asked to begin just behind the starting line. This is in line with the paradoxical finding of a higher MWS calculated on 100 m (T100MW) compared with the 25-foot distance (T25FW). One can assume that the fluctuant phase of acceleration in the first steps of the T25FW makes it a poor indicator of the real maximum walking speed over a short distance. Hence, variations in the T25FW duration are not solely representative of maximum walking speed differences.
The slightly better reliability and lower variability of T100MW indicate that other yet unidentified confounding factors may have less influence on a walking test based on a longer distance.
The T100MW appeared to be better correlated with the ambulation range (MWD) than the T25FW, in patients with “limited” (MWD ≤ 4000 m) or “restricted” (MWD ≤ 2000 m) ambulation. This was also suggested by the coefficient of determination calculation results. It is important to emphasize that the MWD was evaluated on a subjective basis between 500 and 4000 m, but patients’ report of the MWD remains the most widely used approach in trial guidelines and has been shown to be reasonably correlated with values acquired from more sophisticated measures. 14
When performing and comparing several types of gait evaluations, the order of assessment also has to be taken into account. In our study, one may argue that we did not assess the possible effect of the T25FW over the T100MW. However, the T25FW was always performed first. We postulated that the influence of a previous 7.62-m distance performed twice should only be of minor importance over the next 100 m walking speed performed after a 5 minute stop in between.
Beyond the attempts to develop new walking tests more predictive of the accurate MWD and maximum walking speed, there is a need for research efforts to gain more insight into the integrated comprehension of each individual tests with respect to the multiple identified parameters affecting the quality of ambulation, whether related to MS or not. Although diffuse cerebral white matter dysfunction may play a role in early walking disability, its main pathological substratum below an EDSS of 4.0 is likely to reflect mostly spinal cord demyelination and acute relapse–induced and/or chronic relapse–independent axonal loss or dysfunction, especially at the level of the pyramidal tracts. 15 In our study, the T25FW and the T100MW as well as the corresponding MWS displayed abnormal values in the low levels and mid-range EDSS values (EDSS ≤ 3.5), providing evidence of ambulation limitations at early stages of MS evolution. Such early walking limitations are not directly translated in the EDSS status calculation before the 4.0 milestones. The early insidious progression or relapse-driven accumulation of gait disability heavily contributes to the genesis of MS-related physical fatigue and its detection might be a guiding tool for assessing early specific therapeutic interventions. Moreover, in early stages of MS, any increase in the stringency of our analyses of walking performances may allow us to better delineate the spectrum of clinical improvement under highly active disease-modifying treatments. 16
New walking tests, including a T25FW with a dynamic start (allowing a run-up of a few meters before the starting line), evaluations based on greater distances or longer time measurements, 17 speed ratios, and interval analysis may ultimately be even more informative in clinical trials and rehabilitation programs. 18 To evaluate walking fatigability and limitations of MWD, distance-based evaluations (such as 100-m or 500-m walking tests) may be more suitable than time-based evaluations (such as 2-, 3-, or 6-minute walking tests) for 2 reasons: (a) walking tests over a defined distance may allow patients to better dose their effort since they start with a concrete visuospatial representation of the length of the test and (b) in duration-based walking tests, the rater has to ask the patient to walk “as fast and as far as he/she can” over a defined time, which may be a confusing dual task in comparison to the more straightforward recommendation to walk “as fast as he/she can” in distance-based testing.
One may ultimately consider integrating multiple modalities of ambulation tests to develop composite walking indices that could be highly sensitive to change to better capture the efficacy of therapeutic interventions, especially in primary and secondary progressive forms of MS.
Footnotes
Rémy Phan-Ba and Amy Pace contributed equally to this study.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.