
Abstract
Background
Autoimmune thyroid disease (AITD) occurs in 40%–50% of alemtuzumab-treated persons with multiple sclerosis (pwMS), most of whom will develop Graves’ Disease (GD).
Objective
To explore contributory factors for alemtuzumab-related AITD in pwMS.
Methods
A retrospective patient chart review was performed.
Results
Sixteen out of 52 (30.8%) pwMS developed AITD. GD occurred in 56.3% (n = 9), the majority (n = 7, 77.8%) symptomatic. All but one (85.7%) pwMS with symptomatic GD developed atypical, large and rapid fluctuations in thyroid hormone levels unexplained by effect of anti-thyroid medication alone. All symptomatic GD cases were age ≤32 years when starting alemtuzumab (ɸ = 0.60, p = 0.03). PwMS who started alemtuzumab at a younger age developed thyroid disease earlier (r = 0.51, p = 0.04). PwMS with clinical and radiological evidence of brainstem involvement at onset of multiple sclerosis were 11 times more likely to develop symptomatic GD compared with those with other phenotypes (p < 0.01).
Conclusion
Alemtuzumab-induced reconstitution GD may result from early and increased cross-reactivity between antigens common to the brainstem and thyroid, or presence of shared Human Leukocyte Antigen (HLA) alleles that determine brainstem and thyroid involvement. We suggest cautious use of alemtuzumab in younger (≤32 years) pwMS with early brainstem involvement, especially those actively planning pregnancy, where alternative therapies are readily available.
Introduction
Alemtuzumab, an anti-CD52 humanised monoclonal antibody, is one of the most efficacious drugs currently available for the treatment of highly active relapsing multiple sclerosis (MS). 1 Alemtuzumab induces antibody- and complement-mediated cytolysis and apoptosis of circulating B- and T-lymphocytes, resulting in a profound depletion of these cells 2 ; this is followed by a slower phase of lymphocyte recovery with unique lymphocyte subset repopulation kinetics; while this confers the therapeutic efficacy of alemtuzumab, it potentially contributes to the development of secondary autoimmune disease.3,4 Autoimmune thyroid disease (AITD) is the most common secondary autoimmune disease observed in alemtuzumab-treated pwMS, affecting up to 40%–50% of cases, the majority of whom will develop Graves’ Disease (GD).5–9 Contributory factors for alemtuzumab-related AITD include smoking, 8 family history of autoimmune disease, 8 female gender 6 and younger age. 6
Importantly, use of alemtuzumab should be carefully considered for female pwMS of childbearing age for several reasons. While alemtuzumab has the potential to offer disease stability during pregnancy in women with highly active relapsing MS, onset of alemtuzumab-related AITD may occur unpredictably years after the last alemtuzumab infusion,2,5–8 and its occurrence during pregnancy raises concerns both for mother and foetus of adverse prenatal and neonatal outcomes that may result not just from maternal thyroid disease but also from use of anti-thyroid drugs. 10 Alternative MS therapies with similar efficacy but lower pregnancy risk could be considered.11–15
Identification of contributory factors for development of alemtuzumab-related AITD may help to optimise patient selection for alemtuzumab therapy. The aim of this study was to explore the clinical manifestations and contributory factors for development of alemtuzumab-related AITD in pwMS.
Methods
A retrospective patient chart review was performed in an MS tertiary referral centre. Patients were included if they had had at least two standard cycles of alemtuzumab therapy and at least two years’ follow-up since alemtuzumab commencement. GD is defined as hyperthyroidism with positive thyroid stimulating hormone (TSH) receptor antibodies (TRAb).16,17 Age at alemtuzumab commencement and onset of AITD were normally distributed when assessed by the Shapiro–Wilk test for normality. The independent samples t-test was used to compare mean age at alemtuzumab commencement, and mean onset of AITD, between patients with and without symptomatic GD. Fisher’s exact test was used to determine any association between symptomatic GD and age dichotomised to ≤32 years and >32 years; symptomatic GD and brainstem syndrome at onset of MS; symptomatic GD and clinical outcomes; brainstem syndrome at onset of MS and clinical outcomes. Pearson correlation was used to assess the association between age at alemtuzumab commencement and onset of AITD. Statistical analysis was performed using SPSS version 24 (IBM Corp, Armonk, NY, USA). A significance level of 0.05 was used. Study approval was obtained from the Research Ethics Committee of the St. Vincent’s Healthcare Group and patient informed consent was obtained for use of non-identifiable retrospectively obtained data.
Results
Of 52 pwMS who fulfilled criteria, 16 (30.8%) developed alemtuzumab-related AITD over mean ± SD follow-up of 4.6 ± 2.4 years (range 2.0–10.3). The female:male ratio of the AITD cohort was 7:1, while that of the entire alemtuzumab-treated cohort was 3:1. Three pwMS were excluded from further analysis due to pre-existing AITD. GD was observed in 56.3% (n = 9) of cases, most (n = 7, 77.8%) were symptomatic. Six (85.7%) pwMS with symptomatic GD experienced large and rapid fluctuations in thyroid hormone levels unexplained by effect of anti-thyroid medication alone and not typical of conventional GD (Figure 1(a)); three (42.9%) experienced a recurrence of thyrotoxicosis after a prolonged period (4, 6, 30 months) of normalisation of thyroid function tests; three (42.9%) developed a goitre; two (28.6%) are under consideration for definitive therapy including radioactive iodine or thyroidectomy, of whom one was actively planning pregnancy. Nobody developed thyroid eye disease.
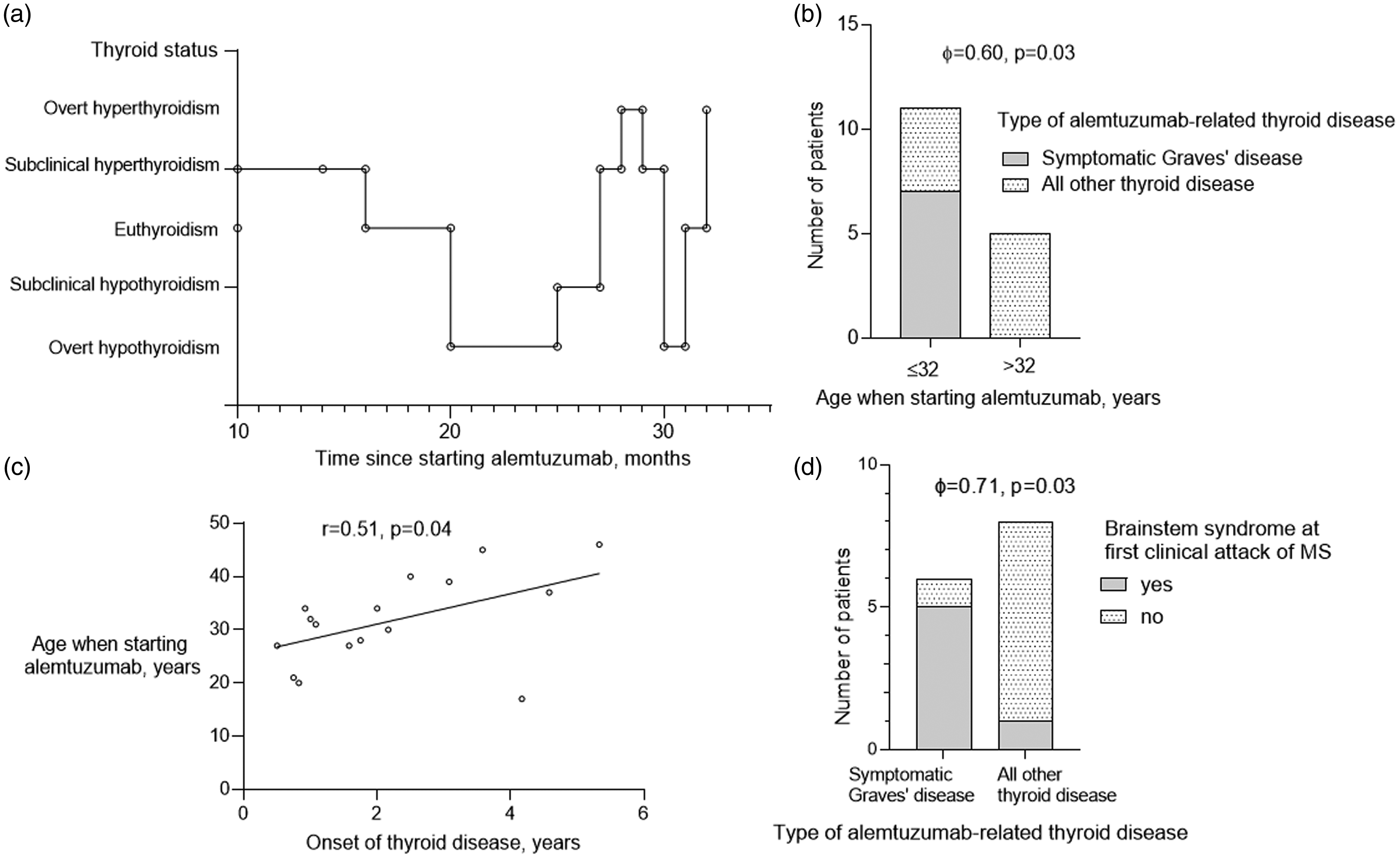
Clinical manifestations of alemtuzumab-related autoimmune thyroid disease: (a) example of atypical fluctuations in thyroid status in a 21-year-old female who developed alemtuzumab-related symptomatic Graves’ disease; (b) proportion of MS patients with symptomatic Graves’ disease, dichotomised to age ≤ and >32 years when starting alemtuzumab; (c) correlation between age when starting alemtuzumab and onset of thyroid disease; and (d) proportion of MS patients with symptomatic Graves’ disease vs all other thyroid disease, who had a brainstem syndrome at onset of MS.
Two out of 16 (12.5%) pwMS with alemtuzumab-related AITD developed biochemical thyrotoxicosis without symptoms; meanwhile, pwMS who developed TRAb-negative thyroiditis (n = 2, 12.5%) and TRAb-negative, thyroid peroxidase (TPO) antibody-positive hypothyroidism (n = 3, 18.8%) experienced a benign clinical course. However, pwMS with TRAb-positive hypothyroidism (n = 2, 12.5%) initially, later became thyrotoxic and experienced unusual fluctuations in thyroid hormone levels, similar to patients with symptomatic GD.
PwMS who developed symptomatic GD were 9.5 years (95% CI 1.7–17.2, p = 0.02, d = 1.4) younger at time of starting alemtuzumab compared with pwMS who developed any other thyroid disease (26.4 ± 5.7 years versus 36.9 ± 8.1 years). All pwMS who developed symptomatic GD were age ≤32 years when starting alemtuzumab (ɸ = 0.60, p = 0.03) (Figure 1(b)). Mean onset of thyroid dysfunction was 2.2 ± 2.5 (0.5–5.3) years. Patients with MS who started alemtuzumab therapy at a younger age developed thyroid disease earlier (r = 0.51, p = 0.04) (Figure 1(c)). One patient developed thyroid disease four months beyond the recommended safety follow-up period of 48 months from last alemtuzumab infusion.
While transverse myelitis was the most common phenotype at onset of MS among the entire alemtuzumab-treated cohort, of the patients who developed alemtuzumab-related AITD, brainstem syndrome (i.e. diplopia, ataxia, vertigo, dysarthria, facial numbness) was instead the most common phenotype at onset of MS. Where information was available, brainstem lesions were observed on magnetic resonance imaging (MRI) brain obtained at onset of MS in these cases. Of the symptomatic GD cohort, 83.3% were found to have brainstem involvement at onset of MS, compared with only 12.5% of pwMS with any other AITD (ɸ = 0.71, p = 0.03) (Figure 1(d)). Patients with brainstem involvement at onset of MS were 11 times more likely to develop symptomatic GD (relative risk (RR) 11.1, 95% CI 1.4–86.2, p < 0.01) and three times more likely to develop TRAb (RR 3.3, 95% CI 1.1–9.9, p = 0.05) with alemtuzumab therapy, compared with patients with any other phenotype at onset of MS.
In relation to post-alemtuzumab disease activity, there were no statistically significant differences in the proportion of pwMS who relapsed (28.6% vs 22.2%), remained neurologically stable (57.1% vs 33.3%) or developed non-active secondary progressive disease (14.3% vs 44.4%) between thyroid cases with and without symptomatic GD respectively. Of the thyroid disease cohort with brainstem involvement at MS onset, 50% relapsed while 50% remained neurologically stable; of those without brainstem involvement at MS onset, 12.5% relapsed, 37.5% remained stable and 50% developed non-active secondary progressive disease; however, there were no statistically significant differences between these two groups.
Discussion
We report a potential association between brainstem phenotype at onset of MS and development of alemtuzumab-related symptomatic GD. We hypothesise that use of alemtuzumab in pwMS induces immune reconstitution that can manifest with increased T-cell cross-reactivity between antigens or epitopes common to both the brainstem and the thyroid. 18 This concept of ‘spreading’ autoimmunity between the central nervous system (CNS) and extra-CNS locations is not new, 18 and may be seen in other clinical settings, the best example of which is the pathogenicity of anti-glutamic acid decarboxylase (GAD) antibodies in the development of type 1 diabetes and stiff person syndrome, due to recognition of different epitopes of the GAD65 isoform between patients with these two clinically distinct diseases. 19 Immune-mediated links between other pairings of neurological and thyroid disease have been reported.20–22
Interestingly, localisation of MS lesions in the brainstem may be determined by genetic (HLA-DR4, -DR7, -DR13) and immune-related factors, 23 and these factors were present in high frequency in MS patients with comorbid psoriasis. 24 Furthermore, a systematic review found that GD and psoriasis were the two most prevalent comorbid autoimmune diseases in people with MS. 25 These findings reveal a potentially unforeseen and essential role of the brainstem in the development of comorbid autoimmune disease in association with MS, and supports our unprecedented finding of a significant association between early MS brainstem involvement and alemtuzumab-induced reconstitution GD.
However, 57.1% of MS patients with early brainstem involvement did not develop symptomatic GD with alemtuzumab therapy, likely because a strategic combination of additional contributory factors6,8 is necessary for its manifestation. Furthermore, both MS and GD are associated with HLA-DRB*03, 18 and polymorphisms in T-cell-related genes CD226 and IL2RA. 26 Notably, timing of MS brainstem involvement may be an important contributory factor: while almost all alemtuzumab-treated pwMS in our cohort eventually developed brainstem lesions with subsequent MS relapses, only pwMS with early brainstem involvement, specifically at first clinical attack of MS, developed symptomatic GD. Moreover, while baseline anti-thyroid antibodies were not performed in our alemtuzumab-treated cohort, emerging evidence suggests its potentially valuable role as a biomarker for alemtuzumab-related AITD.27,28
Younger patients developing thyroid disease earlier and with a more severe clinical course may be explained by the physiologic phenomenon of immunosenescence, that is, ageing of the immune system, whereby age-related reduced capacity of the thymus to generate new T-cells causes a compensatory increase in protective regulatory T-cells, resulting in a lower prevalence of, and milder, autoimmune disease in older individuals. 29 Notably, while there were no statistically significant differences in clinical outcomes in the thyroid disease cohort between pwMS with and without symptomatic GD, and pwMS with and without early brainstem involvement, the results suggested a consistent pattern of higher MS disease activity in pwMS with symptomatic GD or early brainstem involvement compared to those without. This is likely explained by the well-established effects of age and disease duration in the natural history of MS: analysis of data from nearly 15,000 patients in the MSBase registry showed that brainstem relapses were more frequent in younger patients and early disease 30 ; furthermore, relapse rate decreased with increasing age and disease duration. 31 This evidence strengthens our hypothesis of increased immunoreactivity in pwMS who are younger/at an earlier stage of the disease who may be predisposed to increased cross-reactivity between brainstem and thyroid antigens when alemtuzumab therapy is administered.
Comparing our study findings with those of two larger cohorts of alemtuzumab-treated pwMS,6,7 the proportion of GD patients who experienced unusual thyroid hormone fluctuations was 67% (our cohort), 30% (Daniels et al. 6 ) and 16% (Pariani et al. 7 ), not typical of conventional GD; meanwhile the frequency of TRAb-positivity among hypothyroidism cases was 40%, 67% and 20% respectively, much higher than the proposed figure of 10% of spontaneous autoimmune hypothyroidism cases. 32 The proposed mechanism underlying these findings is that of a spontaneous switch, or alteration in ratio, between TSH-receptor stimulating and blocking antibodies, the predominant antibody of which dictates the type of thyroid disease (hyperthyroidism or hypothyroidism) that will manifest.6,7,33 While it is believed that hypothyroidism resulting from this ‘switch’ is an extremely rare occurrence in general endocrine practice, 33 the co-existence of TSH-receptor stimulating and blocking antibodies has been demonstrated in the serum of pwMS with alemtuzumab-related AITD. 7
This study was limited by the retrospective nature of data collection, as well as the small sample size, reflected by the wide confidence intervals in the data. Recommendations for further work include HLA typing of our thyroid disease cohort, as well as data collection and analyses on the associations between alemtuzumab-related AITD and smoking history, personal and family history of autoimmune disease, and location of MRI brainstem lesions.
Conclusion
In conclusion, these results warrant cautious use of alemtuzumab in younger (age ≤32 years) female pwMS with early brainstem involvement, especially in those actively planning pregnancy, where potentially safer alternative therapies, such as natalizumab, rituximab and ocrelizumab, are readily available. Of pwMS who developed symptomatic GD, initial normalisation of thyrotoxicosis should not be taken as a reassuring expectation of prolonged remission, given the high (42.9%) rate of recurrence of thyrotoxicosis in these cases and likely necessity for more definitive treatment, although our cohort will require a longer period of follow-up to assess eventual thyroid-related outcomes. Alemtuzumab-related AITD may present beyond the recommended safety follow-up period of 48 months from last alemtuzumab infusion – one European taskforce has recommended lifelong annual TSH measurement as minimal follow-up for these patients. 17 Guidelines on the management of thyroid dysfunction following immune reconstitution therapy have been published and should prove useful.17,32 Meanwhile, further evidence from larger cohorts of alemtuzumab-treated patients is necessary to validate our study findings.
Author contributions
SMY collected, analysed and interpreted the data, and drafted and revised the manuscript for intellectual content. MD collected the data, and revised the manuscript for intellectual content. RKC analysed and interpreted the data, and revised the manuscript for intellectual content. CMcG collected, analysed and interpreted the data, and revised the manuscript for intellectual content.
Conflict of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SMY received personal compensation for conference activities with Roche and received research support from Novartis. MD received personal compensation for education and conferences by Sanofi Genzyme and Roche. RKC received personal compensation from Ipsen for clinical activities and research support from Kyowa Kirin. CMcG has received research support and/or honoraria from Bayer, Biogen, Sanofi Genzyme, Novartis, Roche and Teva.
Data sharing statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.