
Abstract
Background
Rehabilitation is effective for multiple sclerosis, but is it value for money?
Objectives
To evaluate functional outcomes, care needs and cost-efficiency of specialist inpatient rehabilitation for adults with multiple sclerosis (MS).
Methods
A multicentre cohort study of prospectively collected clinical data from the UK Rehabilitation Outcomes Collaborative national clinical database. Data included all adults with MS (n = 1007) admitted for specialist inpatient (Level 1 or 2) rehabilitation in England, 2010–2018.
Outcome measures
Dependency/care needs: Northwick Park Dependency Scale/Care Needs Assessment, Functional independence: UK Functional Assessment Measure (UK FIM+FAM). Cost-efficiency. Patients were analysed in three dependency groups (High/Medium/Low).
Results
All groups showed significant reduction in dependency between admission and discharge on all measures (paired t-tests: p < 0.001). Mean reduction in care costs/week was greatest in the most dependent patients: High: £519 (95% CI: 447–597), Medium: £148 (76–217), Low: £36 (12–83). Despite longer stays, time taken to offset the cost of rehabilitation was shortest in the most dependent patients: High: 12.9 (12.0–14.1) months; Medium: 29.3 (21.3–51.8); Low: 76.8 (0–36.1). Item-level changes corresponded with clinical experience.
Conclusions
Specialist rehabilitation provided good value for money in patients with MS, yielding improved outcomes and substantial savings in ongoing care costs, especially in high-dependency patients.
Introduction
Multiple sclerosis (MS) is estimated to affect 2.2 million people globally 1 and is a major cause of chronic neurological disability in young and middle‐aged adults. People with MS can present with a wide range of functional deficits that result from physical, cognitive, psychosocial, behavioural and environmental problems, which impact on their activity (function) and societal participation. 2
By improving independence and autonomy, rehabilitation has the potential to reduce the burden and costs of care, both for family and society. Specialist rehabilitation is increasingly recognised as an essential component of healthcare for this group of patients, but it can be a costly intervention and systematic evaluation is required to demonstrate that programmes are both effective and cost-efficient.3–5
There is a growing body of evidence for the effectiveness of rehabilitation in MS,6–15 but with ever-increasing financial pressures on healthcare systems it is necessary to demonstrate value for money. Such evidence is required not only in the context of clinical trials but also in real-life clinical practice.16,17 Economic analysis of individual interventions such as home-exercise programmes, functional electrical stimulation, and schemes to keep people in work have been reported,18–24 but there is no published evaluation of the cost-efficiency of holistic multidisciplinary specialist rehabilitation.
Since 2010, the national UK Rehabilitation Outcomes Collaborative (UK ROC) database has collated episode data for all inpatients admitted to specialist rehabilitation services in England, providing national benchmarking on quality, outcomes and cost-efficiency of rehabilitation. Within the UK ROC dataset, functional gain is evaluated using the UK Functional Assessment Measure (UK FIM+FAM),25,26 which provides a global assessment of physical, cognitive, communicative and psychosocial functions. Cost-efficiency is computed as the length of time taken to offset the initial costs of rehabilitation through savings in the ongoing costs of community care, as estimated by the Northwick Park Dependency Care Needs Assessment.27,28
A previously published multicentre analysis using these indices has demonstrated the cost-efficiency of rehabilitation for younger adults with complex needs due to a range of different neurological conditions. 5 The study analysed outcomes in three groups of dependency and showed that, despite their longer lengths of stay and thus higher initial costs of rehabilitation, it was the most dependent patients who generated the greatest savings in care costs. This was true not only for patients with acquired brain and spinal cord injuries, but for patients with long-term progressive neurological conditions. Although this latter group included patients with MS, the analysis did not address outcomes specifically for MS patients.
This study presents the first national prospective cohort analysis to evaluate changes in functional outcomes, care needs and cost-efficiency following specialist inpatient multidisciplinary rehabilitation for patients with MS. The specific research questions were:
What types of functional gain are made during rehabilitation by patients with MS? Can the longer lengths of stay for highly dependent patients be justified by savings in ongoing care costs? Are there important differences in outcome and cost-efficiency between patients at different levels of dependency that clinicians and service planners should be aware of?
Methods
Design
A large multicentre national cohort analysis of prospectively collected clinical data from the UK ROC national clinical database. Participants were adults with MS admitted to specialist inpatient rehabilitation between 2010 and 2018.
Setting and data source
In England, Level 1 rehabilitation units are tertiary services serving a regionally based catchment population and taking a caseload of patients with very complex needs. Level 2 services take a mixed caseload serving a more local population, divided into 2a (supra-district) and 2b (local district) specialist rehabilitation services.
The UK ROC database was established in 2009 and data reporting was initially voluntary, however since 2013/14, it has provided the national commissioning dataset for NHS England. 29 All Level 1 and 2 specialist rehabilitation services in England are now required to be registered with UK ROC and to submit data for each admitted episode of care. However, data-reporting requirements have evolved over time and vary somewhat between the different levels of service. 30 Governance arrangements are described elsewhere. 5
Measurements
The dataset comprises socio-demographic and process data (waiting times, discharge destination, etc.) as well as clinical information on rehabilitation needs, inputs and outcomes. Full details can be found on the UK ROC website (www.kcl.ac.uk/cicelysaunders/research/studies/uk-roc/index).
The UK FIM+FAM
The UK FIM+FAM (version 12) is a global measure of disability.25, 26 It includes the 18-item FIM (version 4) and adds a further 12 items (FAM), mainly addressing psychosocial function giving a total of 30 items (16 motor and 14 cognitive items). A six-item additional module capturing extended activities of daily living (EADL) such as shopping, finance, household tasks and work 31 is also available for optional completion where these activities are included in the goals for treatment. Each item is scored on a seven-point ordinal scale from 1 (total dependence) to 7 (complete independence). Further details are published elsewhere.25,26
The Northwick Park Dependency Score (NPDS)
The Northwick Park Dependency Score (NPDS) is an ordinal scale of dependency on nursing staff time (number of helpers and time taken to assist with each task) designed to assess needs for care and nursing in clinical rehabilitation settings.
27
It has a total range of 0–100 (a higher score indicates high dependency) and has been shown to be a valid and reliable measure of needs for care and nursing in rehabilitation settings.
32
It supports categorisation of patients into three dependency groups based on their NPDS scores at admission
3
:
Low-dependency (NPDS <10): patients are largely independent for basic self-care, Medium (NPDS 10–24): patients generally require help from one person for most self-care tasks, High (NPDS ≥25): patients require help from two or more persons for most care tasks and often also have special nursing needs.
The NPDS also translates via a computerised algorithm to the Northwick Park Care Needs Assessment (NPCNA), 28 which estimates the total care hours per week and the approximate weekly cost of care (pound sterling (£) per week) in the community, based on the UK care agency costs. The NPCNA provides a generic assessment of care needs, regardless of who provides and pays for them. The estimated cost of care is therefore independent of individual circumstances or local policy for the provision of continuing care, which varies widely across the UK. The algorithm is embedded within the UK ROC software and generates this information.
Cost-efficiency
Within the UK ROC dataset, the cost-efficiency of rehabilitation is calculated as the time taken to offset the cost of rehabilitation by the resultant savings in the cost of ongoing care in the community. 5 This is calculated from the population means and 95% confidence intervals (CIs) as ‘episode-cost of rehabilitation’ divided by ‘reduction in cost of care/month’ from admission to discharge, as estimated by the NPCNA. The episode-cost was calculated per patient as ‘bed-day cost × length of stay’. The cost per bed-day was calculated using the NHS England complexity-weighted bed-day currency based on the indicative tariff costs published for 2013/14 (which remained current up until April 2019). For comparison with other series, we also report FIM-efficiency, as change in total FIM score (FIM gain)/length of stay (LOS) in days, and the equivalent for the UK FIM+FAM (FAM-efficiency).
Valid length of stay
To identify plausible admissions for rehabilitation (as opposed to brief inpatient assessment or long-term care) we selected patients with LOS between 8 and 180 days.
Data extraction
De-identified data were extracted for all recorded inpatient episodes for adults with MS (aged 16+) who were admitted for restorative goal-orientated rehabilitation in a Level 1 or 2 specialist service for between 8 and 180 days, 30 and discharged during the 8-year period (01 April 2010–31 October 2018). Patients were included in the analysed dataset if they had valid UK FIM+FAM and NPDS ratings completed on both admission and discharge from the programme. Data were analysed using STATA v15.1 and SPSS v24.
Data handling and analysis
In this non-interventional observational study, size was not predetermined but dictated by the accruals to the national dataset over the 8-year period that met the inclusion criteria. Missing data were expected as data reporting was initially voluntary, and reporting requirements also vary between service levels. No data were imputed for missing values. Given the large size of the dataset and long-ordinal nature of the measures (i.e. many possible data points) parametric statistics were used for the main analysis.
95% CIs were calculated using bootstrapping with replications of n = 1000, to minimise the effect of any skewed data. Paired t-tests were used to compare significant changes from admission to discharge. One-way analyses of variance (ANOVAs) with post hoc analysis were used to compare differences between the different levels of dependency. Bonferroni corrections were applied to correct for multiple comparisons.
Because item scores yield short-ordinal data (few data points), item-level changes were analysed using non-parametric techniques (Wlicoxon signed-rank tests) and these analyses are included as supplementary files.
Results
Figure 1 illustrates the data extraction process. From a total of 2814 registered episodes, 1592 were admitted for rehabilitation with a LOS of 8–180 days (‘rehabilitation dataset’), of which 1007 (64%) had complete UK FIM+FAM and NPDS data at admission and discharge, and were included in the analysis.

Illustration of the data extraction process to derive the dataset used for analysis.
Study demographics
Demographics for both the analysed and rehabilitation datasets are presented in Table 1. They were generally similar but the analysed sample had slightly longer admissions and so had higher episode costs.
Demographics of the total analysed sample and for the three dependency groups.

M:F ratio = male/female ratio; SD = standard deviation.
*Significant differences were seen between the full and the analysed datasets.
A total of 53 rehabilitation units (10 × Level 1, 11 × Level 2a and 32 × Level 2b services) contributed to the analysed dataset, with good representation across all four health regions in England. Approximately 90% of episodes were in Level 2 (district-based) services. The study sample comprised 63% females with a mean age of 51.7 years at admission. The mean time since onset of MS was 11.2 years. The mean LOS in rehabilitation was 53 days at a mean episode-cost of £22,898.
Table 2 summarises the overall changes in functional independence, dependency and care costs between admission and discharge. Significant gains were seen across all parameters. The mean change in total FIM+FAM score was 17.1 (95% CI 15.8–18.2) (mean change in total FIM score = 12.1). The mean savings in the NPCNA-estimated cost of ongoing care in the community was £319/week, providing annual savings of £16,599, which would offset the initial episode costs of rehabilitation in just 16.6 months.
Overall dependency, functional, and cost-efficiency outcomes on admission and discharge (n = 1007).
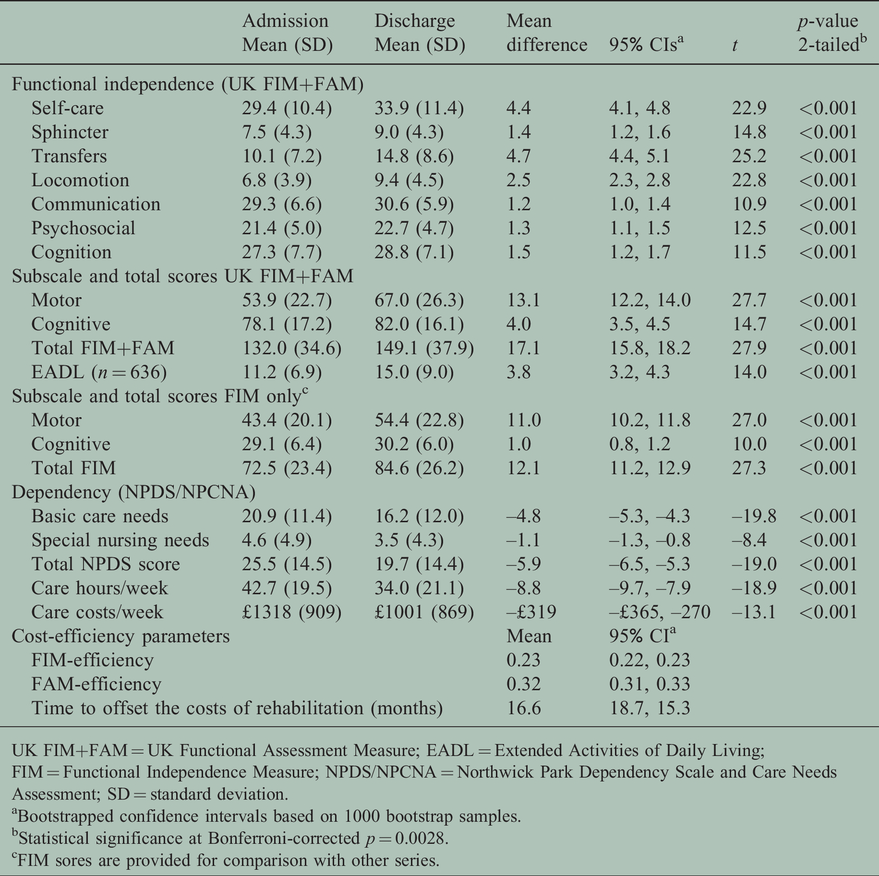
UK FIM+FAM = UK Functional Assessment Measure; EADL = Extended Activities of Daily Living; FIM = Functional Independence Measure; NPDS/NPCNA = Northwick Park Dependency Scale and Care Needs Assessment; SD = standard deviation.
aBootstrapped confidence intervals based on 1000 bootstrap samples.
bStatistical significance at Bonferroni-corrected p = 0.0028.
cFIM sores are provided for comparison with other series.
Differences between between patients at different levels of dependency
Patients in the low-dependency group were younger than both the other dependency groups by a mean of 6–8 years (p < 0.001) and presented at an earlier stage in their disease, averaging 8.8 years since onset (Table 1). The differences in dependency, care needs and cost-efficiency are summarised in Table 3. ANOVA tests showed significant between-group differences and non-overlapping 95% CIs confirm significant differences between each of the groups (see also post hoc multiple comparisons in Supplementary File 1).
Comparison of costs and efficiency between dependency groups (n = 1007).
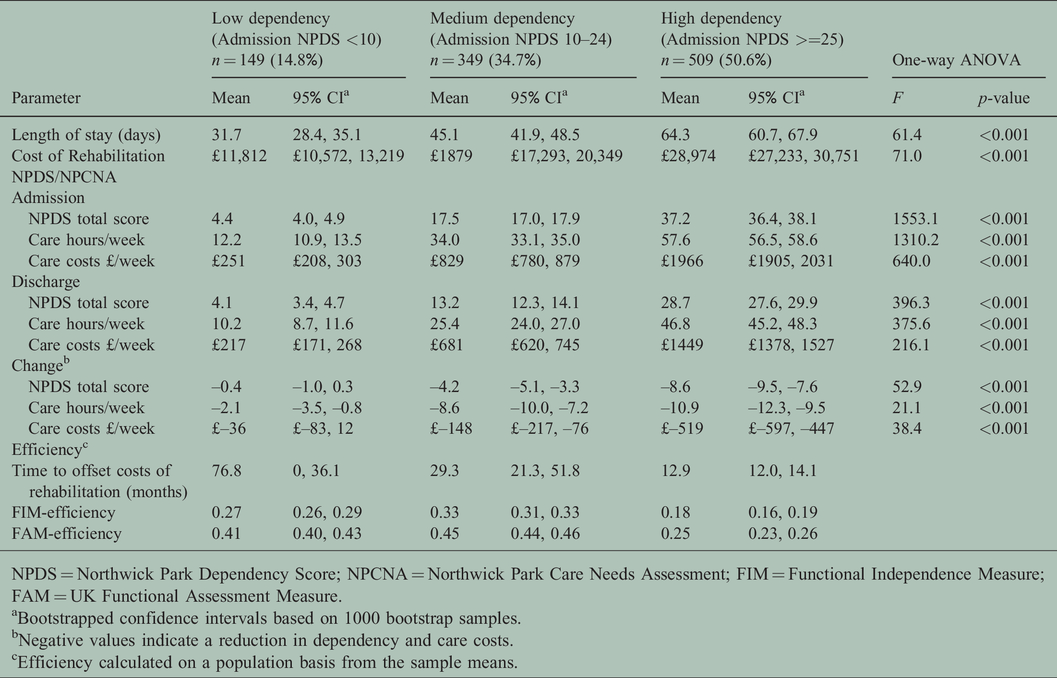
NPDS = Northwick Park Dependency Score; NPCNA = Northwick Park Care Needs Assessment; FIM = Functional Independence Measure; FAM = UK Functional Assessment Measure.
aBootstrapped confidence intervals based on 1000 bootstrap samples.
bNegative values indicate a reduction in dependency and care costs.
cEfficiency calculated on a population basis from the sample means.
LOS and the total cost of the rehabilitation episode varied according to dependency with significant differences between all three groups (p < 0.001) and a greater than twofold difference between the high- and the low-dependency groups.
Care costs on admission and discharge also varied with dependency. The mean reduction in care costs was £519/week in the high-dependency group (compared with £148 and £36/week for the medium- and low-dependency groups respectively). Thus, despite their higher episode costs, the time taken for savings in the ongoing cost of care to offset the initial cost of rehabilitation in the high-dependency group was just 13 months, compared with 29 months and 77 months for the medium- and low-dependency groups.
Functional independence
The differences in functional independence across the three groups are summarised in Table 4 and Supplementary File 2. All three groups made significant gains in both motor and cognitive domains of the FIM+FAM, the total gains being greatest in the medium-dependency group. FIM-efficiency was highest in the medium-dependency group at 0.33 (all between-group differences reaching signficance (non-overlapping 95% CIs)). FAM-efficiency showed a similar pattern.
Comparison of functional independence between dependency groups (n = 1007).

NPDS = Northwick Park Dependency Score; UK FIM+FAM = UK Functional Assessment Measure; EADL = Extended Activities of Daily Living.
aBootstrapped confidence intervals based on 1000 bootstrap samples.
bEADL scores are optional and only normally collected in those patients for whom they are goals for treatment.
We also examined the different areas of functional change for the three groups of patients. The UK ROC software generates ‘FAM-splats’ in the form of radar charts that provide an ‘at-a-glance’ view of the disability profile and patterns of change during rehabilitation for the 30 FIM+FAM items. Figure 2 shows the composite FAM-splats based on median item-scores at admission and discharge for the whole sample and each NPDS dependency group. Paired item-level changes from admission to discharge are given in Supplementary File 3.
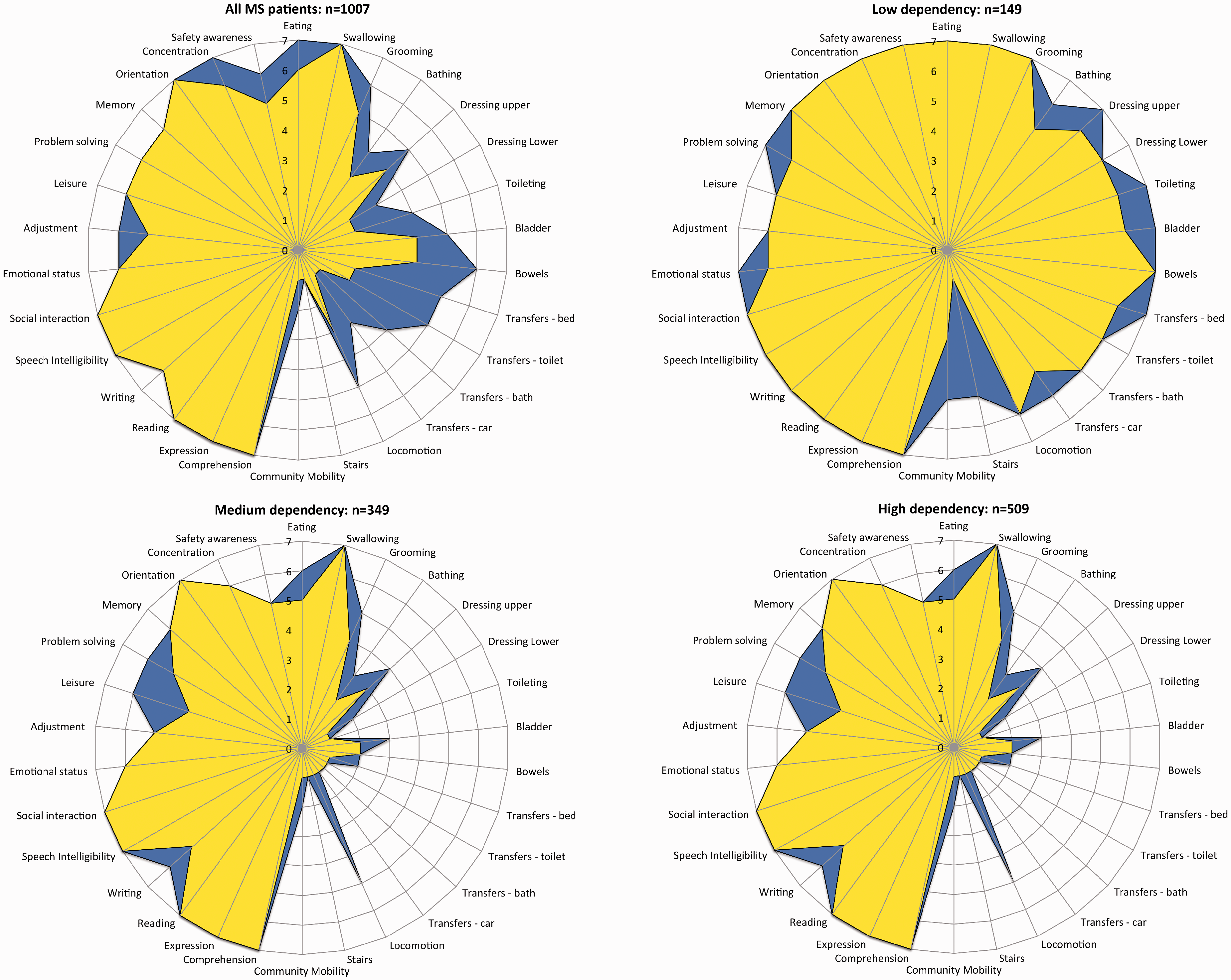
The radar chart (or ‘FAM-splat’) provides a graphic representation of the disability profile from the FIM+FAM data. The 30-scale items are arranged as spokes of a wheel. Scoring levels from 1 (total dependence) to 7 (total independence) run from the centre outwards. Thus a perfect score would be demonstrated as a large circle. This composite radar chart illustrates the median scores on admission and discharge. The yellow-shaded (lighter) portion represents the median score on admission for each item. The blue-shaded (darker) area represents the change in median score from admission to discharge. Clear differences in the pattern of disability can be seen between the three groups.
In the low-dependency group, the majority of patients were already functioning largely independently for most of the items (item scores 6–7). The only substantial area of change was in higher-level mobility, such as managing stairs and getting around in the community, which are therefore key goals for this group of patients. In the medium-dependency group, there was more substantial change in independence for self-care activities such as bathing, dressing, toileting and so forth, and changes in mobility were at the level of improving the ease of transfers and indoor walking. In the high-dependency group, patients were substantially dependent for all self-care activities. They achieved some modest change in indoor locomotion (which may include getting around in a wheelchair) and also in psychosocial activities such as leisure and problem-solving.
Figure 3 shows the equivalent profiles for the six EADL items. While the low- and medium-dependency groups showed a change in median score for all items but work, the high-dependency group made modest gains only in shopping and managing finances

Equivalent radar charts for the extended activities of daily living module. Smaller numbers were expected as this module is optional and typically only completed where the goals for treatment address these extended activities.
Discussion
This multicentre prospective cohort analysis of the UK national clinical dataset has demonstrated that patients with MS benefit from specialist rehabilitation on multiple levels, even many years after the onset of the condition. Although the costs of treatment were considerable (£22,898 on average), this investment was offset by savings in the cost of ongoing care within approximately 16.6 months.
As in our previous analysis of other neurological conditions, 5 the most dependent patients were the costliest to treat, but generated the greatest savings in ongoing care costs, so that cost-efficiency was greatest in this group. This finding contrasts with an earlier study by Grasso et al. in 2009, which found that rehabilitation produced greater change in MS patients with mild to moderately severe impairment, 13 although their outcome measurements (the Barthel Index and Rivermead Mobility Index) focused only on physical disability. In this study, FAM-splats demonstrated the changing profile of disability and the range of physical, cognitive and psychosocial changes that occurred during rehabilitation across the three groups.
Patients with MS present with a diverse range of needs and goals for rehabilitation, which change over time as the disease progresses. 33 In the early stages, rehabilitation goals may focus on mobility and employment. Later, the focus is on maintaining independence for activities of daily living, and latterly on managing and maintaining their care. A variety of measurement tools is therefore required to capture the changes through the different stages.
Our findings underline this point and resonate with clinical experience. The low-dependency group were younger with a shorter time since onset than the more dependent groups. They had little need for assistance from others and so made little gain in terms of reduction in care costs. Thus, according to the NPCNA, rehabilitation appeared not to be very cost-efficient for this group. However, the UK FIM+FAM demonstrated very significant gains in terms of higher-level function in personal care, mobility and extended activities out in the community, all of which have an impact on autonomy and quality of life for them and their families.
Some countries use FIM-efficiency as a proxy for cost-efficiency of rehabilitation. Several authors have highlighted the limitations of this approach,34,35 which is heavily dependent on LOS and influenced by floor and ceiling effects of the FIM, so that FIM-efficiency typically appears greatest in the medium-dependency group. 36 The current study confirms that a linear trajectory of recovery cannot be assumed, nor can an equal weight of items for estimating the cost of care needs. 5 These findings are important because in countries that rely on FIM-efficiency as the means of patient selection for rehabilitation programmes, highly dependent patients may be denied treatment even though they would actually be the most cost-efficient to treat.
The authors recognise the following limitations to this study:
UK ROC captures all patients admitted to Level 1 and 2 services, but those who progress satisfactorily within their local (Level 3) rehabilitation services (which do not submit data to UK ROC) were not represented in this analysis. This series therefore represents a smaller subgroup of more complex patients in comparison with other international rehabilitation cohorts. However, the rehabilitation dataset from which the analysed sample was drawn represents the total population of patients with complex needs presenting for specialist rehabilitation in England. Because of the variation in reporting requirements over the data collection period, the analysed sample represents only about two-thirds of the full rehabilitation dataset. Comparison of demographic data suggested that the analysed sample was reasonably representative of the total population, but LOS and therefore the cost is rehabilitation was greater in this group. This could have introduced some selection bias leading to under-estimation of cost-efficiency. Due to the general nature of the dataset, no MS-specific tools were captured. Until April 2017, UK ROC collected only de-identified data, so it is not possible to identify how many patients had more than one episode of inpatient rehabilitation between 2010 and 2018. The NPCNA estimates of continuing care costs are not true assessments as applied in traditional health economic studies and the estimations of cost-savings should be interpreted with some caution. However, the instrument has been in use for two decades and has been widely taken up both in clinical practice and in research.
32
Experience has demonstrated it to be neither overly generous nor mean in its estimation of care needs and costs. Moreover, in this study the relative values were of more interest for between-group comparison than the absolute values. The method of evaluating cost-efficiency relies on the assumption that the observed functional improvement is maintained at least for the ‘pay-back’ period of 16.6 months. While this assumption is reasonable in single incident pathology (e.g. traumatic brain injury or stroke), it is less secure in a progressive condition such as MS. Freeman et al. provide some evidence for carryover of benefits from an inpatient rehabilitation programme, but emphasise the important of ongoing services in the community to maintain the gains achieved.
37
While rehabilitation is provided through the health sector, the saving in care costs accrues to those responsible for ongoing care (typically the social care services or the patient and their family). Thus, the actual opportunity for realisation and reinvestment of the savings will depend on the local funding arrangements for health and social care.
The above limitations accepted, this study provides important evidence for the cost benefits of rehabilitation for patients with MS. It also confirms the potential for substantial cost-savings to be made from appropriate provision of specialist rehabilitation services towards the later stages of the disease. Indirectly this provides evidence that rehabilitation is a continuing process in a progressive disorder such as MS in which disability may evolve over several decades. It supports the argument that rehabilitation should continue to be provided periodically in both inpatient and community settings throughout the patient’s lifetime.
Supplemental Material
MSO912789 Supplemental Material1 - Supplemental material for Cost-efficiency of specialist inpatient rehabilitation for adults with multiple sclerosis: A multicentre prospective cohort analysis of the UK Rehabilitation Outcomes Collaborative national clinical dataset for rehabilitation centres in England
Supplemental material, MSO912789 Supplemental Material1 for Cost-efficiency of specialist inpatient rehabilitation for adults with multiple sclerosis: A multicentre prospective cohort analysis of the UK Rehabilitation Outcomes Collaborative national clinical dataset for rehabilitation centres in England by Lynne Turner-Stokes Richard Harding, Peihan Yu, Mendwas Dzingina and Wei Gao in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Supplemental Material
MSO912789 Supplemental Material2 - Supplemental material for Cost-efficiency of specialist inpatient rehabilitation for adults with multiple sclerosis: A multicentre prospective cohort analysis of the UK Rehabilitation Outcomes Collaborative national clinical dataset for rehabilitation centres in England
Supplemental material, MSO912789 Supplemental Material2 for Cost-efficiency of specialist inpatient rehabilitation for adults with multiple sclerosis: A multicentre prospective cohort analysis of the UK Rehabilitation Outcomes Collaborative national clinical dataset for rehabilitation centres in England by Lynne Turner-Stokes Richard Harding, Peihan Yu, Mendwas Dzingina and Wei Gao in Multiple Sclerosis Journal – Experimental, Translational and Clinical
Footnotes
Acknowledgements
The authors are grateful to the patients and clinical team who submit data to UK ROC from the clinical teams in the 53 centres. We would like to thank the UK ROC research team (Heather Williams, Keith Sephton and Alan Bill) for their support with data extraction and preparation for analysis.
Author contribution
Lynne Turner-Stokes leads the development of the UK ROC register and dataset. She took the lead role in planning, design, execution and governance of the study and had overall responsibility for study reporting. She prepared the original grant application to the Multiple Sclerosis Society was responsible for drafting the manuscript. Richard Harding contributed to the design of the study and interpretation of results. Peihan Yu was a research assistant on the study. She assisted with data analysis and drafting the manuscript. Mendwas Dzingina was the lead health economist. Wei Gao was the Principal Investigator. She supervised Peihan Yu to implement the statistical analysis plan. She contributed to the design of the study and interpretation of data. All authors contributed to writing, reviewing and commenting on the article. All authors approved the final submitted version.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Outcome measurement is a specific research interest of our centre. Lynne Turner-Stokes is Director of UK ROC and was the lead developer of the NPDS, NPCNA and the UK FIM+FAM, but neither she nor her employing institution has any financial interest in the tools, which are disseminated free of charge. None of the authors has any personal financial interests in the work undertaken or the findings reported. All authors are employed by Northwick Park Hospital and/or King’s College London, which may cite this article as part of their research evaluation processes, including the UK Research Excellence Framework 2020. Lynne Turner-Stokes has received financial support from the National Institute for Health Research (NIHR) to attend conferences to disseminate the findings from the UK programme. We do not consider that any of these relationships or activities have influenced the submitted work.
Data sharing
As the UK ROC dataset is a live clinical dataset, for reasons of confidentiality and data protection data sharing is not available at the current time.
Ethics approval
Collection and reporting of the UK ROC dataset is a commissioning requirement according to the NHS England service specification for Level 1 and 2 Rehabilitation Services. According to the UK Health Research Authority, the publication of research findings from de-identified data gathered in the course of routine clinical practice does not require research ethics permission. Registration: The programme was registered with the NIHR Comprehensive Local Research Network: ID number 6352
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research from the UK Rehabilitation Outcomes Collaborative Database, the development of which was funded by the NIHR under its Programme Grants for Applied Research programme (RP-PG-0407-10185). This project is also partly supported by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) South London at King’s College Hospital NHS Foundation Trust, and Cicely Saunders International. CLAHRC South London is a research organisation working to improve health and social care services and funded by the NIHR. The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Funding from the Multiple Sclerosis Society in the UK (grant reference: 52) and Dunhill Medical Trust also contributed to support this study.
STROBE checklist
Please see attached.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.