
Abstract
Background
The relation between ABO/Rh groups and multiple sclerosis (MS) has been proposed in several studies, however there is a controversy about the role of these groups in the disease. Although it has been reported that some groups can be protective or risk factors, there is no consensus and discordant reports can be found in the literature.
Objectives and methodology
In this short report, we analyze the ABO/Rh distribution in a MS cohort of 265 patients and compare these frequencies with the results obtained from the Basque Blood Donors bank (17,796 individuals) of the same region.
Results and conclusions
From our data, the absence of immune antigens (A, B or Rhesus +) defined by the group O- seems to be protective in the MS group with an odds ratio of 0.49 (95% confidence interval 0.309–0.796), while the presence of Rh+ plus A or B seems to be a risk in developing multiple sclerosis.
Introduction
The ABO blood group system was discovered in 1901 by Karl Landsteiner (for which he won the Nobel prize in 1930). 1 This system categorizes the blood group into three main alleles; the alleles A and B that are co-dominant and the allele O that is recessive. These groups are genetically determined by different single nucleotide polymorphisms in the ABO gene, located in the long arm of chromosome 9 (ABO; 9q34.2, ID: 28). A and B alleles encode for slightly different glycosyltransferases that add N-acetylgalatosamine and D-galactose to the H substance (a precursor side chain that is ultimately transformed into A- or B- antigen). Therefore, groups are characterized by the presence or absence of the carbohydrate antigens A and B on the erythrocyte membrane and by the presence of anti-A and anti-B antibodies in blood plasma. The combination of these three alleles produces the four known major genotypes: A, B, AB, and O. 2 These genotypes can be combined with Rh status (positive or negative) giving eight possible combinations.
Although they were discovered more than 100 years ago, the clinical and biological implication of these groups is still not fully understood. Recent evidence suggests that the ABO system is clinically important not only from a hematology, transfusion and transplantation point of view, but also plays a role in the pathogenesis and understanding of several diseases. 3 In this context, blood groups are known to play a direct role in the immune response to infections by serving as pathogen receptors, signal transducers or adhesion molecules. 2 Some phenotypes have also been associated with host resistance to certain infections, however their implication in autoimmune diseases remains unclear.
Multiple sclerosis (MS) is an autoimmune disease whose etiopathology remains unknown although it is widely accepted that genetic and environmental factors interplay to produce the disease. In the 1980s and 1990s several studies examined the relationship between the ABO groups and MS. Despite some contradictory results, they proposed that A+ and/or B+ alleles seem to be a risk factor for MS while O group seems to be a protective factor. However, several of these studies were performed in small-size cohorts and, moreover, the different origin of the patients in each study makes difficult to compare the results.4–8
In this context, we decided to analyze the distribution of ABO and Rh blood groups in MS-cohort patients from Hospital Universitario Donostia. Our health area covered an estimated population of 800 MS patients from Gipuzkoa, located in the Basque Country, Spain. In this short report, we analyze the ABO distribution in an MS cohort of 265 patients and compare these frequencies with the results obtained from the Basque Blood Donors bank (17,796 individuals) of the same region.
Methodology
All patients were recruited at the Neurology Department of the Hospital Universitario Donostia. All of them had been diagnosed with definitive MS by the McDonald 2010 criteria. Blood was extracted using a routine process for biochemical studies and the blood group was included in the biochemical request. Anonymized data was obtained from the 265 patients. Data from the Basque blood bank was obtained from the database preserving the anonymization of all the participants.
Data was analyzed using SPSS 20. Distribution was analyzed using Pearson’s chi-squared test and Student’s t-test. Correlation studies were done by R-3.4.3 using MVA package.
Results
Our cohort included 265 patients and 17,796 anonymous blood donors. The distribution of the data can be seen in Figure 1 and Table 1. The average age of the patients was 47.90 years (from 22 to 88 years), 183 out of the 265 patients were women (69.06%) and the average Expanded Disability Status Scale (EDSS) score was 2.18 (from 0 to 7) (Table 2).

(a) Histogram of the percentage of each ABO (±) category in each group. Blue: Blood donors from Gipuzkoa (n = 17,796), Red: multiple sclerosis cohort (n = 256). (b) Correspondence analysis between the ABO (±) variables, the MS (multiple sclerosis) groups and Gipuzkoa (blood donors form Gipuzkoa). (c) Odds ratios (blood donors versus MS). CI, confidence interval; OR, odds ratio.
Distribution of the blood groups.
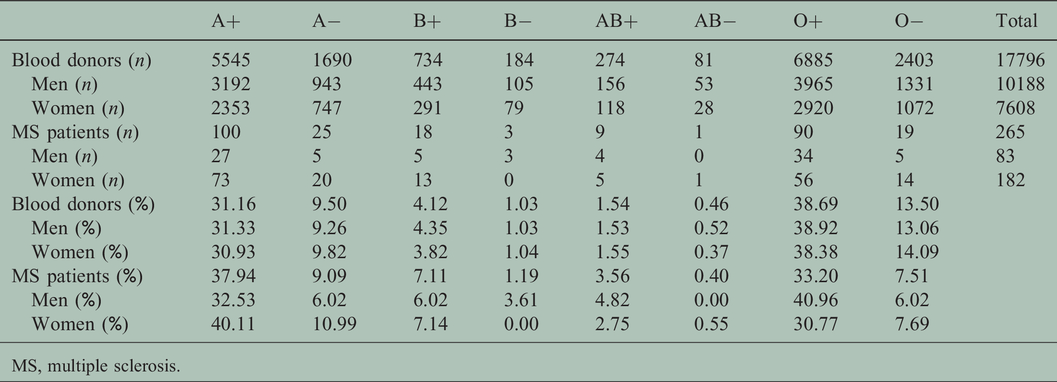
MS, multiple sclerosis.
Demographical data of the MS cohort.
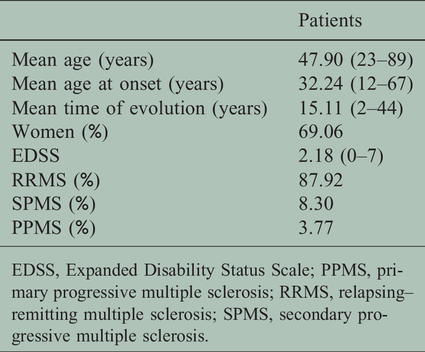
EDSS, Expanded Disability Status Scale; PPMS, primary progressive multiple sclerosis; RRMS, relapsing–remitting multiple sclerosis; SPMS, secondary progressive multiple sclerosis.
Data analysis showed that blood groups were differently distributed among the two populations (p < 0.001). The individual statistical analysis revealed that A+ and B+ were overrepresented while O- was underrepresented in the MS group when compared with the blood donors’ group.
When we conducted a correspondence analysis to better study those differences, the previous results were confirmed adding AB+ as overrepresented in the MS group.
No differences were found in EDSS, age, age at onset, or gender between ABO, Rh- groups or ABO (±) groups.
Discussion
Our data showed a different distribution of ABO (±) groups in the MS cohort but not in any other variable (EDSS, gender, age at onset, age, or disease type). This suggests that ABO (±) groups could be a factor related to the risk of suffering from MS but not to the evolution of the disease. From our data, the absence of immune antigens (A, B or Rhesus+) defined by the group O- seems to be protective against the disease with an odds ratio of 0.49 (95% confidence interval 0.309–0.796), while the presence of Rh+ plus A or B are overrepresented in the MS group (Figure 1). Following this trend, the AB+ group should be considered a risk factor for MS. Although in the classical analysis we do not have enough statistical power owing to the lack of data (just nine patients), in the correspondence analysis the importance of AB+ arises.
ABO groups are related to several diseases and our results underline the possibility that they are also related to MS. 9 In concordance with our findings, the O group has been proposed previously as a protective factor against MS in the Cuban population 10 and in the Croatian population. 5 However, we are far from understanding the relationship between blood groups and MS. The ABO system is known to be related to neurogenesis and neurodegeneration, 11 and has been also related to a risk of progressive multifocal leukoencephalopathy, an undesirable side effect in some treatments used to manage MS. Blood groups have been related to an increased risk for cardiovascular diseases that are associated with higher white matter and whole-brain volume loss.12,13 ABO (±) distribution has been linked to our response to inflammation and even with the microbiome and its role in immune regulation, highlighting their importance in the complex puzzle that is MS.
Our data shows an interesting observational relation between MS status and blood group, therefore ABO (±) may be included in the characterization of patients as another interesting variable.
Our results are limited to a specific region, therefore further studies are needed to validate this relationship in other cohorts. Moreover, the meaning of this relationship and the functional implications should be addressed in further functional studies.
Conflict of interests
The author(s) have no conflicts of interest to declare.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work has been partially supported by the Spanish Network of Multiple Sclerosis (REEM) from Instituto de Salud Carlos III partially covered with FEDER funding.