
Abstract
A critical step in the diagnosis of multiple sclerosis is to rule out a heterogeneous variety of multiple sclerosis mimickers, which is crucial in the era of powerful immune-modulator treatments. In this review, we discuss the background of toxocariasis in general, present central nervous system Toxocara infection as one of the multiple sclerosis mimickers in the Middle East, and share our experience about the diagnosis and management of this condition. This entity seems very relevant in a region such as the Middle East, where displacement of populations and conflict can result in non-hygienic food and water management bundles. The diagnosis should be entertained, especially when assessing patients with myelopathy. The presence of a single lesion in the spinal cord with inflammatory features should prompt serological testing for Toxocara IgG and IgM in serum and the cerebrospinal fluid. This infection is treatable, with the regimen of high-dose albendazole being one of the most accepted treatments. Although most cases exhibit a good prognosis, some have residual deficits localized to the affected spinal cord level.
Introduction
With the advances in magnetic resonance imaging (MRI) and serological testing, the ability to reach a correct diagnosis of multiple sclerosis (MS) has improved, especially when used appropriately to rule out alternative diagnoses (MS mimickers). In the era of advanced disease-modifying treatments (DMTs), it is critical to avoid a misdiagnosis of MS, because of its psychosocial/financial consequences to the patients, 1 as well as the immune biological effects resulting from the use of DMTs. Therefore, the diagnosis of MS in the correct context requires demonstration of dissemination in space and time of demyelinating lesions in the central nervous system (CNS), after exclusion of alternative diagnoses. 2 In addition to the classical “red flags” in the diagnosis of MS, physicians should consider regional risk factors and epidemiology. 3 In this review, we shed light on CNS Toxocara infection as one of the MS mimickers that we have seen in the Middle East and describe its clinical features, diagnosis, and treatment.
Illustrative case report
A 73-year-old woman, known to have psoriasis, presented to the American University of Beirut Multiple Sclerosis Center in March 2019 with a chief complaint of bilateral lower extremity numbness and urinary retention with incontinence.
Her history goes back to October 2018, when she developed bilateral lower extremity numbness starting at the toes and progressing up to mid-chest level (around T5) over 1 month. She also reported burning pain and decreased temperature discrimination in the left lower extremity, accompanied by bilateral knee buckling and difficulty climbing stairs. At that time, she also had urinary retention with incontinence. She was seen by several physicians with no definite workup and was mostly treated for presumed urinary tract infections.
In January 2019, she underwent brain MRI, which showed several subcortical and periventricular hyperintense lesions on FLAIR imaging, and spine MRI, which showed a fusiform lesion in the right posterolateral aspect of the spinal cord at the level of T5–T6, with mild cord enlargement and small peripheral focal nodular enhancement on post-contrast images (Figure 1). Blood tests for thyroid stimulating hormone level, folate, vitamin B12, Brucella titers, anti-cyclic citrullinated peptide, C3, C4, and C-reactive protein were normal. Pelvic ultrasound with post-void residue was normal, with a bladder residue of 55 cc. However, urine analysis was positive with >50 white blood cells (WBCs), nitrites, leukocyte esterase, and bacteria seen. She did not receive any diagnosis or treatment and presented to our clinic in March 2019 for further evaluation.

Sagittal T2-weighted image (a) T1 with Gd (b) and T2 fat-suppressed (c) of the dorsal spine showing hyperintense fusiform lesion at T5–T6 level with focal peripheral nodular enhancement (circle) and mild enlargement of the cord at the same level. Axial T2-weighted images of the spine at T5 level showing the lateral (d) and postero-lateral (e) predominant location of the lesion. Post-contrast axial T1 image of the spine at T5 level (f) showing peripheral focal nodular enhancement of the lesion (circle).
When the patient was first seen in our MS center, neurological examination revealed impaired ambulation with the need for unilateral assistance to walk at least 50 meters. Tandem walking was slightly impaired. There was a decrease in touch, pinprick, and temperature sensation in the left-lower extremity with a sensory level at T5. There was a moderate decrease in vibration sense in the right-lower extremity and a mild decrease in vibration sense in the left-lower extremity. Muscle strength in the right hip flexor was 4/5 and in the left hip flexor 4+/5. Plantar flexion was scored as 4+/5 in the left foot. Plantar reflexes were flexor responses bilaterally. Investigation of her urinary symptoms revealed no urge to urinate for the past year, absent bladder sensation, straining and 2–3 episodes of nocturia per night, as well as dysuria. The patient also reported chronic constipation with only one bowel movement every 5 days.
The patient had lived in Venezuela for 20 years, before resettling in Lebanon in a suburban area in the mountains 5 years ago. She did not recall any exposure to pets such as cats or dogs. She also denied having any neurological disturbances during her pregnancies or after delivery of her seven children. She never had blurry vision, weakness, gait problems or bowel symptoms that would last for more than 24 hours. She developed psoriasis in 2014 and was initially treated with methotrexate until 2018, then switched to weekly phototherapy.
Considering the patient’s myelitis presentation, further workup with a dedicated brain MRI, blood studies for autoimmune workup, cerebrospinal fluid (CSF) studies and visual evoked potentials were ordered. The repeat brain MRI showed multiple white matter lesions in the periventricular area, mostly subcortical (Figure 2), but no callosal, juxtacortical, or infratentorial white matter lesions (Figures 3 and 4). Although the MRI findings mimicked MS lesions, they were not suggestive of demyelinating disease. Blood workup for autoimmune diseases mimicking MS, including anti-Sjögren's-syndrome-related antigen A antibodies, anti-Sjögren's-syndrome-related antigen B antibodies, antinuclear antibodies, anti-dsDNA, anti-cardiolipin antibodies was negative. CSF analysis showed 4 WBCs, 0 red blood cells, protein 0.5 g/L, glucose 52 mg/dl, but positive Toxocara IgG by Western blot against several antigens (24, 28, 30 and 35 kD), negative for oligoclonal bands (analyzed by isoelectric focusing) and a normal IgG index of 0.56. The patient was diagnosed with Toxocara myelitis based on the combination of clinical, radiological, and serological findings, with incidental non-specific white matter lesions in the brain most likely related to chronic ischemic small vessel disease considering the patient’s age.

Axial T2 FLAIR images of the brain showing subcortical and periventricular lesions (a, b, c, d, e). Sagittal T2 FLAIR images of the brain showing subcortical lesions (f), some of which are perpendicular to the lateral ventricles but not located in the corpus callosum (g).
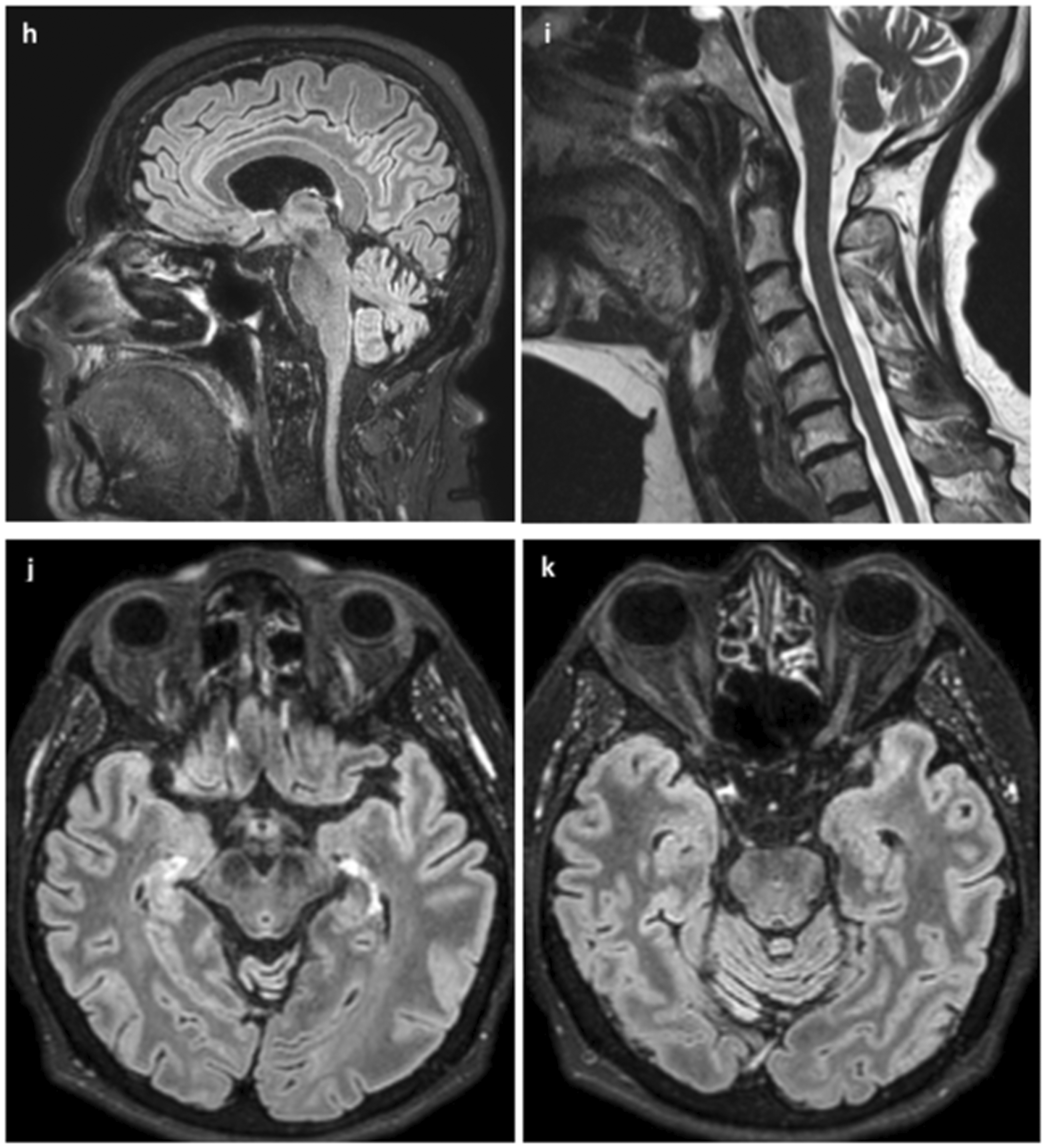
Sagittal T2 FLAIR image of the corpus callosum (h) and cervical spine (i) showing these structures are not involved. Axial T2 FLAIR images of the upper midbrain (j), pons and optic nerves (k) showing there are no lesions in those structures.

Axial T2 FLAIR images of the lower pons (l), and cerebellum (m) also showing there are no lesions in the posterior fossa.
The patient was treated with 1 g intravenous (IV) methylprednisolone for 5 days and albendazole 400 mg twice daily for 3 weeks. She also received treatment for urinary tract infection with E. coli multidrug resistance, as well as symptomatic treatment with pregabalin 75 mg orally twice daily for her left lower extremity burning pain. She was referred to a urologist and was found to have 800 cc of post-void residue on an ultrasound of the bladder. She was diagnosed with neurogenic bladder due to myelitis and was advised to perform intermittent catheterization. The patient presented for follow up 1 month after initiation of treatment. She did not have any improvement in her sensory or bladder symptoms after completing the 5 days cycle of IV steroids. After 3 weeks of anti-helminthic treatment, the paresthesia in the chest and abdomen completely resolved and she was left with residual lower extremities paresthesia, dysesthesia in the left-lower extremity, and severe urinary retention. This is concordant with reports in the literature, which show that residual deficits remain localized at the spinal level of the infection. She denied any adverse effects from her medications. Because in our experience with Toxocara myelitis in Lebanon treatment duration varied between 2 weeks to 3 months, we opted to give her another 3 weeks of treatment with albendazole in hopes of further improving her symptoms. She was also advised to repeat MRI in 3 months to follow up the improvement of the Toxocara lesion, which should accompany the improvement in symptoms.
Epidemiology
Toxocariasis in humans was first described in 1950 by Wilder 4 and later in 1952 by Beaver et al. 5 Initially it was considered to be a rare pediatric infection, but later it was recognized to be one of the most prevalent helminthic infestation in industrialized countries. 6 Given that most Toxocara infections remain asymptomatic, the exact prevalence of toxocariasis is difficult to ascertain. Some serology studies reported a variable seroprevalence worldwide, from 2.4 to 31% in Europe and 13.9 to 37% in the United States, 7 and a much greater variability (39–93%) in tropical regions.8–11 The variations in these estimates could be partially explained by differences in serology techniques,6,12 rates of infection of pets, their hygiene/access to public places, habits, and humid climate favoring the survival of Toxocara eggs.9,13,14
In the Middle East, few countries have reports on seroprevalence rates for toxocariasis. In 2004, Kanafani et al. performed a pilot seroprevalence study of 150 participants (14 years of age or older) at the American University of Beirut and Medical Center, motivated by several cases of myelitis of unknown etiology in Lebanon between the years 2000 and 2004, which turned out to be due to toxocariasis. 6 They reported a seroprevalence of 19%, with other groups reporting a 23% in Egypt 15 and 19.5% in Jordan. 16
After the first description of “neurotoxocariasis” published by Beautyman and Woolf in 1951, 17 and recognized as such later in 1966, 18 several cases were reported. Until to a systematic review on the matter in February 2016, 100 case reports of neurotoxocariasis have been published in 66 research papers and eight meeting abstracts. 19 The largest series in that review included 17 cases of Toxocara canis myelitis in Lebanon. 11
Biology of Toxocara sp
Infection by the Toxocara parasite, or “toxocariasis”, is caused by the ascarid nematode Toxocara canis, with domestic dogs as the definitive host and aberrant (accidental) infection to humans. 6 Toxocara cati is commonly found in cats, and has been described to cause a similar infection as Toxocara canis. 20 It has been reported as the most prevalent zoonosis in some industrialized countries and not only in rural areas. 10 In the life cycle of this parasite, the domestic dog is the definitive host of the T. canis worm. 21 Female worms may produce up to 200,000 eggs per day in the small bowel of the host, but eggs passed in the feces are not infective and require an incubation period of around 1 week (more in lower temperatures) in the soil to embryonate. 22 Completely embryonated Toxocara eggs contain larvae that can infect animals and humans, and preserve this infective potential in the environment for several years.19,20 When re-ingested by a definitive host, the eggs hatch in the small bowel and some larvae perforate the mucosa to reach the portal and then systemic circulation. Other larvae remain the small bowel of the host, reaching the adult worm phase within 3 weeks, after which they release eggs in the feces of these animals and complete the cycle. 20 Another mode of transmission, especially relevant in cats, is the transplacental and transmammary migration of larvae into the fetuses, with the highest prevalence of Toxocara infection reported in puppies and kittens up to 6 months of age.20,23
Humans can acquire the infection through accidental ingestion of embryonated eggs excreted in dog or cat feces, typically present in the soil or contaminated fomites. 10 It may also be acquired through the consumption of contaminated pork, chicken, duck, rabbit, or beef.22,24,25 After ingestion, the embryonated eggs hatch in the small bowel of humans and release immature larvae, which enter the mucosa and migrate to the liver via the portal bloodstream, and then to the lungs and heart, reaching the systemic circulation. 19 The larvae migrate through the systemic bloodstream and can survive in the circulation for months or several years, 20 until their arrest in small-caliber vessels facilitates their infiltration into surrounding tissues, in organs such as the liver, lungs, eyes, and CNS.25,26 Migrating T. canis larvae can also cause different inflammatory multisystem tissue eosinophilic reactions known as “visceral larva migrans” (VLM) syndrome. 20 Nevertheless, Toxocara larvae cannot develop into adult roundworm in humans.19,20,22
Clinical manifestations of toxocariasis
Clinical manifestations of toxocariasis vary according to the organs involved, as well as the number of ingested larvae, age, and immune status of the patient, previous exposure to larvae, and persistent re-infection.19,27,28 Mortality is usually low, mostly resulting from pulmonary or cardiac involvement and its complications.
In adults, common toxocariasis consists of generalized weakness, pruritic rash, dyspnea, and abdominal pain.14,19,29 Covert toxocariasis is a syndrome most commonly seen in children, consisting of a systemic immune response to constant challenge by the parasite antigens (fever, headache, behavioral and sleep disturbances, cough, anorexia, abdominal pain, hepatomegaly, nausea and vomiting).29,30 VLM is a syndrome consisting of systemic involvement (hyperthermia, anorexia, body weight loss, malaise). Affected organs include: lungs (productive cough, dyspnea and bronchospasm, recurrent episodes of pneumonia with or without pleural effusions and bronchitis), liver (hepatomegaly), bowel (diarrhea, nausea, and vomiting), skin (angioedema, pruritic rash, hives), and heart (cardiac conduction and muscle abnormalities).19,27,31–33Ocular larva migrans is another well-described syndrome, which typically occurs unilaterally in children and young adults causing vision loss over a period of days to weeks, due to larvae migration to the eye causing uveitis, endophthalmitis, granulomatous retinitis, papillitis, and it can take years before diagnosis.34–36
In neurotoxocariasis, CNS involvement is secondary to visceral larva migrans, and although it is considered a rare and unpredictable complication, experimental animal models showed that Toxocara larvae frequently migrate to the CNS.8,13,14,20,37,38 Several studies have reported a possible and debatable association between neurotoxocariasis and epilepsy, but this is still controversial. The relatively high prevalence of epilepsy and seroprevalence of toxocariasis in children, as well as difficulties to establish the time of exposure in case control studies, impedes any definitive association.19,39
Neurotoxocariasis can occur in the CNS compartment alone. 30 Several autopsy studies in the past showed the presence of Toxocara larvae in the leptomeninges of isolated cases with no clear history of symptoms, in the cerebral, cerebellar, and spinal gray (including the thalamus) and white matter.18,20,40 The spectrum of clinical manifestations of neurotoxocariasis is broad, and includes extramedullary mass, cerebral vasculitis, seizures, and eosinophilic meningitis or meningoencephalitis.11,38,41 In 2005, Eberdhart et al. published a review of 41 cases of neurotoxocariasis, in which Toxocara was considered the cause of the disease either because the larvae were identified by biopsy or autopsy, serology results were compatible with Toxocara infection, and/or responded clinically to anti-helminthic treatment. 42 The median age of the cases was 22 years, 36% presented mostly meningitis, 28% myelitis, and 62% predominant encephalitis. 42 In that study, 12 cases had clinical signs of myelitis, clinically presenting with monoparesis or paraparesis, thoracic or lumbar sensory level, or sphincter dysfunction. 42 Other clinical presentations: optic neuritis,43,44 obstructive hydrocephalus, 37 encephalitis, 45 hemiparesis with multiple white matter lesions,24,46 stroke, 46 and cerebral vasculitis.8,47–50
One of the largest series of Toxocara myelopathy was reported in Lebanon, where the clinical and radiological characteristics of 17 cases were published in 2011. 11 Notably, a clinical presentation of sensory, motor, and autonomic dysfunction, predominantly in the lower extremities, without any systemic symptoms makes Toxocara myelopathy an important MS mimicker. Moreover, the majority of the cases followed a subacute or chronic clinical course, both with a slowly progressive or relapsing–remitting pattern, and with mild to moderate neurological deficits. 11 Other authors reported cases of transverse myelopathy, 51 isolated thoracic meningomyelitis, 52 compressive myelopathy by an epidural abscess, 53 cluster-like headache associated with cervical cord lesion, 54 and isolated lumbosacral involvement. 55
Diagnosis of CNS toxocariasis: Serological (blood and CSF) and radiological features
Certain clinical and radiological features raise suspicion for Toxocara sp. infection, prompting confirmation through serology tests. Serology is important to confirm an active infection and initiate anti-parasitic treatment. It might be difficult to distinguish between early and past toxocariasis infection, as detection of specific IgM/IgA was reported to be not useful as a marker of early infection because it is produced throughout the course of the disease. 56 Hence, clinical suspicion along with the presence of leukocytosis with eosinophilia and the detection of specific IgG (which might remain elevated for more than 5 years) has been suggested to be sufficient for diagnosing toxocariasis.56,57
Enzyme-linked immunosorbent assays (ELISA) are used in routine evaluations and detect specific anti-Toxocara IgG antibodies directed against T. canis excretory-secretory (TES) antigens. 57 Several authors reported that patients with serology results on the border of the cut-off value might be actually Toxocara-positive. 57 Borderline negative results could be due to a weak immune response to the larvae early in the course of the infection. 57
While studies have shown that TES-based IgG ELISA is sensitive for Toxocara serodiagnosis (97.1%), its specificity is low (36%) in blood. This makes the diagnosis of Toxocara in parasite-endemic regions such as the tropics more difficult to establish because of co-existence with other parasitic infections. In this instance, TES-based IgG ELISA will prove useful for excluding toxocariasis from a differential diagnosis, but when results are positive, interpretation of the test can be difficult. 12 Therefore, it is important to confirm all positive and questionable results using the western blot technique, which detects Toxocara spp. infections using recombinant antigens of low molecular weight (24–35 kDa) that are specific to the genus Toxocara. 57
Although using TES-ELISA/western blot yields satisfactory results with respect to both sensitivity and specificity, this combined diagnostic process is costly. 56 Further investigations into developing improved and less costly serodiagnostic assays for Toxocara infection are an active area of research. In the study by Noordin et al., the use of IgG4 subtype ELISA was found to improve specificity at the cost of sensitivity. They argue this test might be of value for attaining higher diagnostic specificity when investigating positive results in endemic areas. 12 However, to date, the detection of specific IgG4 does not have any routine use. 56
In suspected neurotoxocariasis, CSF studies are important in the diagnosis. In the systematic review by Deshayes et al., CSF abnormalities included pleocytosis (62.5%) with a predominance of eosinophils accompanied by elevated proteins (54.5%). However, anti-Toxocara IgG detection in the CSF by western blot remains the best confirmatory test because it is found in most cases of neurotoxocariasis (93.4%). 19
For the post-treatment follow up of the infection, studies have shown that eosinophil counts decrease within a month of treatment and were the only helpful markers of treatment response. Serum total IgE concentrations and anti-TES IgG ELISA remained unchanged. 19 Post-treatment serial MRIs can also be of great value to confirm the diagnosis and efficacy of treatment. 58
In the 17 cases of Toxocara myelitis reported in Lebanon, the diagnosis was confirmed by positive Toxocara canis antibody titers in the blood and the CSF. White cell counts, peripheral eosinophilia, CSF eosinophilia, and CSF proteins did not reveal a consistent pattern among patients. Glucose levels were normal in all patients. The total white cell count was often within the normal range, except in two cases. Peripheral eosinophilia was common but not universal. Three patients had a mild eosinophilia count and one had moderate eosinophilia as defined above. CSF eosinophilia was much less common. Only two patients had significant eosinophil counts in the CSF, whereas glucose levels were all normal. Most patients had normal CSF protein electrophoresis. 11
As for the radiological features, MRI findings prompting suspicion for CNS toxocariasis include a hyperintense single lesion on T2WI with focal nodular enhancement on contrast-enhanced T1 images.58–60 The posterior and postero-lateral segments of the spinal cord are most commonly involved and are the sites of enhancement, indicating particular vulnerability of those areas to the parasite.58–60 The persistence of residual damage confined to the posterior columns confirms preferential involvement of this area. 58 Enhancement is due to blood-brain barrier disruption, which may be the result of inflammation resulting from the infection or secondary demyelination. 61 Toxocara-infected lesions are seen in the cervical and dorsal spine but not in the lumbar region. 60 Spinal Toxocara lesions can be difficult to differentiate from MS lesions because of the short length of spinal involvement in both conditions. 60 Brain MRI in patients with Toxocara myelitis are often normal; however, hyperintense lesions on T2-weighted images have been reported in the literature in cases of cerebral toxocariasis. 62
In Lebanon, the case series describing 17 Toxocara myelitis cases showed a consistent picture with previous literature. In fact, seven patients had cervical lesions and eight patients had dorsal lesions. All lesions were single, showed swelling and enlargement, were isointense on T1 and hyperintense on T2 and FLAIR sequences. Nodular enhancement was observed in the posterior cord. All patients had normal brain MRI. 11
Treatment and prognosis of CNS toxocariasis
There is still no consensus on the treatment of neurotoxocariasis due to lack of randomized clinical trials. Currently, recommendations are based solely on expert opinion. Virtually all anti-helminthic medications can cross the blood-brain barrier; 8 however, albendazole is the most commonly used treatment due to its low toxicity, good penetration in the CNS, and ability to reach high serum concentrations. 19 Albendazole is given at a dose of 800 mg/day divided into two doses per day in adults and 15 mg/kg/day divided into two times per day in the pediatric population. According to the literature, this therapy has been proven to be effective in 47% of patients with toxocariasis. 19 Although thiabendazole and diethylcarbamazine have been shown to induce improvement in 50% and 70% of patients with Toxocara infection respectively, their use is still limited due to their unfavorable and frequent side-effect profile. 19 All other benzimidazoles have poor CNS penetration. 8 Corticosteroids were often used concomitantly with anti-helminthic therapy in an attempt to decrease acute inflammation and immunologic manifestation of the disease;19,63 however, there are no studies supporting this combined treatment rationale. Therapy duration is 21–28 days until complete resolution of clinical symptoms and MRI findings. 19
In the largest case series of Toxocara myelitis reported in Lebanon, all patients were given 400 mg albendazole orally twice daily for 2 weeks to 3 months. Ambulation was improved in all patients but almost half of them had residual sensory, urinary, and erectile disturbances. 11 Treatment with steroids prior to initiating anti-helminthic treatment failed to have an effect both clinically and radiologically. 11 There were no reported side effects from anti-helminthic treatment. 11
Conclusion
In conclusion, toxocariasis should be considered when assessing patients with myelopathy. This can be even more important in patients with white matter lesions presenting for evaluation of possible MS, as in our illustrated case report. This seems very relevant in a region such as the Middle East, where displacement of populations and conflict can result in non-hygienic food and water management bundles. The presence of certain radiological characteristics as described in this review should prompt serological testing for Toxocara IgG and IgM in the CSF. Not all cases have a classic history of exposure to dogs, owning a pet, or ingesting raw food. This infection is treatable, with the regimen of high dose albendazole being one of the most accepted, for 21–28 days at a dose of 400 mg orally twice per day for adults and 15 mg/kg/day in two divided doses for children. Although most cases exhibit a good prognosis, some have residual deficits localized to the spinal cord level of the infection.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
MSO855757 Supplemental Figures - Supplemental material for Toxocara infection in the differential diagnosis of multiple sclerosis in the Middle East
Supplemental material, MSO855757 Supplemental Figures for Toxocara infection in the differential diagnosis of multiple sclerosis in the Middle East by Marwa Baalbaki, Mayssam El Najjar, Samir Atweh and Nabil K. El Ayoubi in Multiple Sclerosis Journal—Experimental, Translational and Clinical
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.