
Abstract
Background
There are no data on neutralising antibodies to interferon-beta and its clinical implications in Chinese patients with multiple sclerosis (MS).
Objectives
The objectives of this study were to investigate the prevalence of neutralising antibodies among Chinese patients with relapsing MS receiving interferon-beta (1a or 1b) and to study the association between neutralising antibodies and the clinical-radiological response.
Methods
We performed a cross-sectional study on MS patients who received interferon-beta for 9 months or more, and evaluated the clinical response by relapses and magnetic resonance imaging lesions. Blood samples were evaluated for myxovirus resistance protein A (MxA) gene expression by polymerase chain reaction, anti-interferon-beta binding antibodies by enzyme-linked immunosorbent assay, and neutralising antibodies by cell-based MxA protein induction and luciferase reporter gene assays. Assay performances were evaluated by receiver operating characteristic analysis.
Results
Among 78 subjects recruited, 61/77 (79%) had anti-interferon-beta binding antibodies, and 22/78 (28%) had neutralising antibodies by MxA protein induction assay. The presence of high-titre neutralising antibodies was associated with poor clinical outcome (odds ratio 6.1, 95% confidence interval 1.5–25.6, P = 0.013). The sensitivity and specificity for neutralising antibodies using MxA gene expression assay (cut-off 0.20) was 80% and 68%, respectively (area under the curve 0.71).
Conclusions
Neutralising antibodies are associated with poor clinical outcome in Chinese patients with relapsing MS. MxA gene expression and protein induction assays are complimentary assays for neutralising antibody detection.
Keywords
Introduction
Multiple sclerosis (MS) is a disabling neurological disease affecting the central nervous system of young adults, and is the most common autoimmune inflammatory demyelinating disease worldwide. 1 The prevalence in Hong Kong has risen by 40% between year 2008 and 2015, from 4.8 to 6.8 per 100,000 persons.2,3 Interferon-beta (IFN-β) remains an efficacious first-line treatment for relapsing MS, by reducing the relapse rate, disability and magnetic resonance imaging (MRI) disease burden. 4 In Hong Kong, IFN-β became a fully reimbursed medication in public hospitals in 2012. Although IFN-β has excellent long-term safety and efficacy data from prospective studies, evidence suggests that up to 30–40% of MS patients treated with interferon may develop neutralising antibodies (NABs) to IFN-β. NABs are associated with reduced treatment efficacy, disease relapse and progression. 5 Patients with persistent NABs and poor clinical response are usually recommended to switch to other disease-modifying treatments in most practice guidelines.5,6
To date, there are no data on NABs in Chinese MS patients. We performed a cross-sectional study with the aim of developing and validating in-house assays to investigate the prevalence of anti-IFN-β binding antibodies (BABs) and NABs among Chinese patients, and to study the association between NABs and clinical-radiological treatment response. The results can be used to develop pragmatic treatment algorithms to identify MS patients with NABs early in their disease course and to switch them to alternative second-line therapies, which are now becoming available in Hong Kong.
Materials and methods
We recruited relapsing MS patients from neurology outpatient clinics in 11 public hospitals in Hong Kong. All assays were performed at a central immunology laboratory that provides diagnostic services for the territory. The inclusion criteria were: (a) adult patients (≥18 years old) with MS by McDonald criteria 2010 diagnosed by a neurologist; 7 (b) who fulfilled the diagnostic criteria for relapsing MS; and (c) were treated with IFN-β 1a or 1b (1a: rebif or avonex, 1b: betaferon) for 9 months or more. The exclusion criteria were: (a) last dose of IFN-β more than 12 months earlier or duration of treatment less than 9 months; (b) non-MS central nervous system demyelinating disorders, such as neuromyelitis optica; or (iii) other subtypes of MS, such as primary progressive MS. The study was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (CRE-2012.143). All patients gave written informed consent.
A research nurse collected clinical data including demographics, functional assessment by the Expanded Disability Status Scale (EDSS) by neurologists, type, dosage, route of administration, duration of IFN-β therapy from first prescription and, clinical information related to the diagnosis of MS and relapses. All MRI evaluations for MS before and after the use of IFN-β were recorded, which included the presence of new T2-hyperintense lesions typical of MS, the presence of contrast enhancing lesions (CELs), and the presence of enlarging lesions as reported by radiologists. Study neurologists adjudicated the clinical status of each patient as overall response to IFN-β: ‘doing well’ – no clinical relapse after IFN-β therapy, with no or limited MRI activity (CELs and/or new T2 lesions); ‘intermediate disease activity’ – one clinical relapse during therapy, with no or limited MRI activity (CELs and/or new T2 lesions); ‘doing poorly’ – multiple clinical relapses during therapy or, one relapse with extensive MRI activity (multiple CELs and new T2 lesions). 5 The sample size of 80 subjects was determined by convenience sampling of the number of patients undergoing treatment at the recruiting sites when planning the study. A control group consisted of 20 age-matched healthy subjects recruited for the analysis of assay sensitivity and specificity.
Sample collections
All blood samples were collected within 3 to 12 hours after IFN-β injection and sent to the central laboratory for processing. For each subject, 10 mL clotted blood was collected for isolation of serum, which was aliquoted and stored at –70℃ until analysis. In addition, 5 mL of whole blood was drawn into a PAXgene blood RNA tube (BD Diagnostics) for total RNA extraction. PAXgene samples collected were mixed thoroughly and incubated at room temperature (RT) for 2 hours, then transferred to the central laboratory at RT for processing within 72 hours of collection. Total RNA was extracted by PAXgene blood RNA extraction kit (BD Diagnostics), and stored at –70℃ until analysis.
Serum samples were tested for the presence of BABs by a commercial enzyme-linked immunosorbent assay (ELISA; Bühlmann Laboratories AG). The bioavailability of IFN-β in subjects’ circulation was determined by analysing the gene expression of myxovirus resistance protein A (MxA). 8 We developed a cell-based MxA protein induction assay for NABs in serum samples. 9 A luciferase assay for NABs, luciferase gene reporter assay (Biomonitor Ltd.), was used for internal comparison. 10 MxA protein induction assay performance, including sensitivity and specificity, was analysed with reference to luciferase assay and receiver operating characteristic (ROC) analysis. In addition, 15% of study samples were analysed by an external laboratory (Mayo Clinic) using the cytopathic effect (CPE) assay to provide comparison data.
MxA gene expression analysis
MxA mRNA expression was analysed using total RNA extracted from the PAXgene blood samples. Total RNA was first converted to cDNA using a SuperScript III First-Strand Synthesis SuperMix kit for quantitative (q) reverse transcriptase polymerase chain reaction (PCR; ThermoFisher Scientific). The cDNA was used as a template for the SYBR green real-time PCR analysis using Platinum SYBR Green qPCR SuperMix-UDG ROX kit (Thermo Fisher Scientific) with 10 mM of specific oligonucleotide primer pair sequences for MxA mRNA (forward: 5′–ACCTACAGCTGGCTCCTGAA–3′; reverse: 5′–GCACTCAAGTCGTCAGTCCA–3′). Real-time PCR reactions were carried out with an ABI 7900HT qPCR system (Applied Biosystems). All reactions were performed in triplicate and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used for sample normalisation. The relative MxA mRNA expression levels were expressed as 10 × 2^-delta CT values.
Cell-based MxA protein-induction assay
For the MxA protein induction assay, 1 × 104/well IFN-responsive adenocarcinomic human alveolar basal epithelial cells, A549 cell line (ATCC), were seeded and grown overnight in a 96-well culture plate at 37℃, 5% carbon dioxide. The cells were stimulated for 24 hours with various concentrations (0 IU/mL to 800 IU/mL) of recombinant human IFN-β (PBL Assay Science) in triplicate, to generate an IFN-β activity standard curve. One laboratory unit (LU) of IFN-β activity in the assay was defined as equal to the IFN-β (IU/mL) value at the midpoint of the standard curve (i.e. 50% MxA protein level of the curve). One LU was approximately equal to 20 IU. On the same plate, another set of cells with the same cell density was incubated with different concentrations of heat-inactivated patient sera (screening at 1:10, 1:100 and 1:1000) in triplicate wells, which were spiked with 10 LU of human IFN-β (i.e. 200 IU/mL), for 30 minutes prior to adding into the A549 cell-containing culture plate for 24 hours. The IFN-β stimulated intracellular gene expression and MxA production in the A549 cells. In the presence of NABs in serum samples, the bioactivity of IFN-β is neutralised and the expression and production of MxA is reduced. After 24 hours of incubation, cells were washed and lysed with 100 µL/well RIPA lysing solution (0.1% sodium dodecyl sulphate (SDS), 1% NP40, 0.5% sodium deoxycholate, 1× proteinase inhibitor). Cell lysates were collected, incubated on ice for 30 minutes and stored at –80℃ until used. The amount of MxA protein in the cell lysates was measured using a commercial MxA ELISA (BioVendor Inc.) according to the manufacturer’s instructions. The titre of the NABs, in tenfold reduction units (TRUs), were determined using the Kawade formula, t = f(n – 1)/9, where f is the reciprocal of the antibody dilution at 1 LU, n is the IFN-β concentration (LU/mL) used in the assay, and t is the titre, expressed in TRUs, 11 of NAB-positive serum that reduces IFN-β activity by 90% (i.e. from 10 to 1.0 LU/mL). This method of reporting NAB titres is recommended by the World Health Organization. 12 Repeated assays for intra-assay and inter-assay precision, and comparison with normal subjects for specificity, were also performed for selected subject samples.
Statistical analysis
We used SPSS 22.0 (IBM) and GraphPad Prism 5.03 for analysis. The Mann–Whitney U test was used for group comparisons of non-parametric variables, and the t-test was used for parametric variables. The chi-square test was used to compare between groups with or without BABs/NABs. The Spearman coefficient was used for correlation analysis. We evaluated the sensitivity and specificity of assays by ROC analysis. Two-tailed P values less than 0.05 were considered statistically significant.
Results
Characteristics of 78 Chinese subjects with relapsing multiple sclerosis receiving IFN-β.

EDSS: Expanded Disability Status Scale; IQR: interquartile range; SC: subcutaneous; IM: intramuscular.
The median age of subjects was 35 years (interquartile range (IQR) 27–45). The majority (62/78, 80%) were women. The mean disease duration was 5.2 ± 4.2 years. The median neurological disability, measured by the EDSS, was 2.0 (1.0– 3.0). The mean duration of IFN-β use was 3.7 ± 2.9 years. Among different preparations of IFN-β, the most commonly used was IFN-β-1a subcutaneously (rebif, n = 52, 67%), followed by IFN-β-1b subcutaneously (betaferon, n = 15, 19%), and IFN-β-1a intramuscularly (avonex, n = 11, 14%). In this cohort, the use of IFN-β was associated with an overall 57% reduction in annualised relapse rate (ARR, 1.12–0.48, P < 0.01) after IFN-β therapy (Wilcoxon ranked test Z score –5.3, P < 0.05). The adjudicated clinical status was ‘doing well’ (n = 48, 62%), ‘intermediate disease activity’ (n = 9, 11%), and ‘doing poorly’ (n = 21, 27%). We recruited 20 healthy subjects as the control group. The median age was 33.0 years (IQR 21–44), and 67% were women; there was no significant difference in baseline characteristics for study subjects (P > 0.05).
Anti-IFN-β binding antibodies
Association between clinical predictors and presence of BABs to IFN-β.

BAB: anti-IFN-β binding antibody; NAB: neutralising antibody; EDSS: Expanded Disability Status Scale; MRI: magnetic resonance imaging; CE: contrast enhancing.
Neutralising antibodies
We evaluated for NABs using the cell-based MxA protein induction assays, and luciferase reporter gene assay for internal comparison. Twelve (15%) samples were sent to an overseas laboratory (Mayo Clinic) using the CPE assay for external comparison.
NABs were present in 22/78 (28.2%) subjects using MxA assay for detection. The titre was between 20 and 100 TRUs in 12 (15.4%) subjects, and more than 100 TRUs in 10 (12.8%) subjects. Among the various types of interferon, NABs were present in 16/52 (31%) subjects using rebif, two of 11(18%) subjects using avonex and four of 15 (27%) subjects using betaferon. A lower proportion of subjects (n = 10, 12.8%) had the presence of NABs using the luciferase assay; one patient (1.3%) had a NAB titre between 20 and 100 TRUs, while nine patients (11.5%) had a NAB titre greater than 100 TRUs.
For samples sent for external comparison, 11/12 (91.7%) of the results by luciferase assay were concordant. The non-concordant subject had a low titre (23 TRUs) by luciferase assay and was reported as negative by CPE assay. For the MxA assay, eight of 12 (66.7%) concordant results were noted (using 20 TRUs as the cut-off), and 100% concordant when using 100 TRUs as the cut-off.
NABs and clinical radiological outcomes
Association between clinical predictors and presence of NABs by MxA protein induction assay and luciferase assay.

NAB: neutralising antibody; EDSS: Expanded Disability Status Scale; MRI: magnetic resonance imaging; CE: contrast enhancing.
Univariate analysis for predictors of ‘poor’ clinical response.
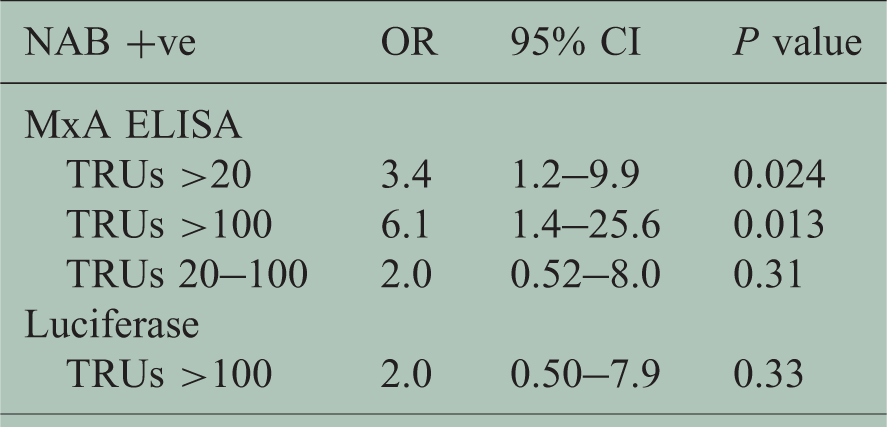
NAB: neutralising antibody; OR: odds ratio; CI: confidence interval; TRU: tenfold reduction unit; ELISA: enzyme-linked immunosorbent assay.
The relative MxA gene expression was lower in NAB-positive subjects than in NAB-negative subjects using a high titre cut-off value greater than 100 TRUs (0.13 ± 0.18 vs. 0.40 ± 0.52, P < 0.01) (Figure 1). However, there was no significant association between relative MxA gene expression and BAB assay in both positive and negative patients (Spearman test P = 1.0 and 0.61, respectively). For subjects with high NAB titres (>100 TRUs), the BAB level (BTU) was significantly higher than those without NABs (812 ± 780 vs. 139 ± 290, P < 0.01). For normal subjects, the BAB level was significantly lower than that of both NAB-positive and negative patients tested by MxA protein induction assay.
Relative MxA gene expression levels in whole blood from subjects with and without neutralizing antibodies, and in normal controls, as determined by the MxA protein induction assay. NAB-positive and NAB-negative groups refers to the presence of NAB titre >100 TRUs (n = 10) and ≤100 TRUs (n = 68), respectively. The box and whiskers plots of each group represent the median level of MxA gene expression, second and third quartile values (box), and the minimum and maximum gene expression levels (whiskers) of the three studied groups.
ROC analysis
ROC curve analysis was performed for BAB results, relative MxA gene expression levels, and NAB results obtained by MxA protein induction assay. For BABs and NABs tested by MxA assay (titre >100 TRUs as the cut-off), the area under the curve (AUC) was 0.73 (Figure 2). At the clinical cut-off of 30 BTUs, the sensitivity was 100% and specificity was 27%. For relative MxA gene expression levels and NABs (MxA assay at cut-off >100 TRUs), the AUC was 0.71 (Figure 3). At a cut-off of 0.20 for MxA gene expression assay, the sensitivity was 80% and the specificity was 62%. MxA gene expression assay appeared to have a better performance, in terms of a higher specificity, when compared with the commercial BAB ELISA.
ROC curve of BABs and NABs using ELISA-based MxA protein induction assay. ROC curve of relative MxA gene expression and NABs by MxA protein induction assay (ELISA-based).

Using the luciferase assay as an internal reference benchmark for the presence of NABs, the ROC curve of NAB titre as measured by the MxA protein induction assay and the luciferase assay had an AUC of 0.91 (Figure 4). At a cut-off of 20 TRUs, the sensitivity was 90% and specificity was 81%. At a cut-off of 100 TRUs, the sensitivity was 90% and specificity was 92%.
ROC curve of NAB titres by ELISA-based MxA protein induction assay and luciferase assay.
Discussion
In this study, we evaluated the performance of assays for BABs and NABs to IFN-β in a cohort of 78 Chinese MS patients. We found BABs in 78% of subjects, and NABs in 28% of subjects. Subjects with high titres of NABs were six times more likely to have a poor clinical outcome, as suggested by multiple clinical relapses or extensive MRI lesions. This was the first study to identify the prevalence of NABs to IFN-β in Chinese patients and to substantiate the need for routine clinical testing of NABs in patients who are using IFN-β for the treatment of relapsing MS.
Increasing evidence supported that there were significant correlations between BABs, NABs and MxA gene expression in Caucasian MS patients. 13 The detection of BABs was suggested as a first-line screening test for NABs. Recent studies suggested that BAB titres are generally correlated with NAB titres, and BAB-negative samples reliably predicted NAB negativity.13,14 We have also identified an excellent negative predictive value of BABs for NABs (94%). The low-titre group had weaker correlations between BABs and NABs than the high-titre group. We found a similar relationship in our Chinese patients. Subjects with low titres (20–100 TRUs) of NABs were not strongly associated with a poor clinical response. For patients with low titres of BABs, MxA gene expression analysis of patients’ blood cells could act as a complimentary test for the bioavailability of IFN-β in the blood. 15
Our data suggests that NABs also developed in Chinese patients with MS using IFN-β regularly. The prevalence rates of both BABs (78%) and NABs (28%) were comparable to those published elsewhere. 16 Among subjects with high titres of NABs, we also observed differences in clinical and MRI responses. This is consistent with the proposed detrimental effect of NABs on treatment efficacy, and a recommendation to switch therapy should be made. The subcutaneous preparations of IFN-β had higher proportions (27–31%) as compared to the intramuscular preparation (18%), although the difference did not reach statistical significance. High titres of BABs or very low levels of MxA relative gene expression were strongly associated with the presence of NABs. 14 The immunological–clinical correlation was less pronounced for subjects with low titres of NABs (20–100 TRUs). However, as this is a cross-sectional study, we were unable to evaluate the changes of NABs over time, as low-titre NABs may disappear over time.17,18 Nevertheless, our data suggests the importance of monitoring for NABs in MS patients receiving IFN-β, as the presence of NABs strongly increased the risk of poor clinical response, and recommendation to switch therapy should be considered.
The generalisability of this study is limited by the relatively small sample size and cross-sectional study design. The relatively higher rates of NABs among users of rebif (31%) and avonex (18%) could be due to the use of the older preparation of rebif and very small number of avonex users (n = 11). The limitations of the Kawade equation used to calculate NAB titres may also account for the higher positive rates of NABs. 19 We cannot evaluate the serological change in study subjects in a prospective manner. 20 An important goal achieved in our project was to develop in-house assays for BAB and NAB assays; more samples are needed in the future to optimise the cut-off values for clinical interpretation. A prospective study to evaluate the sero status changes in subjects using interferon continuously is warranted.
Conclusions
In a cohort of Chinese patients with relapsing MS who used IFN-β for 9 months or more, we found 78% of subjects developed BABs, and 28% of subjects developed NABs to IFN-β. The presence of NABs was associated with poorer clinical outcomes with multiple relapses and extensive MRI lesions.
Footnotes
Acknowledgements
The authors would like to thank Ms Sumei Zhang and Ms Angel Ng for their contributions to the laboratory work and secretarial support for the manuscript, respectively.
Conflicts of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was funded by the Health and Medical Research Fund (01120486) of the Food and Health Bureau of the Government of the Hong Kong Special Administrative Region.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.