
Abstract
Background
While magnetic resonance imaging contrast-enhancing lesions represent an excellent screening tool for disease-modifying treatments in relapsing–remitting multiple sclerosis (RRMS), this biomarker is insensitive for testing therapies against compartmentalized inflammation in progressive multiple sclerosis (MS). Therefore, alternative sensitive outcomes are needed. Using machine learning, clinician-acquired disability scales can be combined with timed measures of neurological functions such as walking speed (e.g. 25-foot walk; 25FW) or fine finger movements (e.g. 9-hole peg test; 9HPT) into sensitive composite clinical scales, such as the recently developed combinatorial, weight-adjusted disability scale (CombiWISE). Ideally, these complementary simplified measurements of certain neurological functions could be performed regularly at patients’ homes using smartphones.
Objectives
We asked whether tests amenable to adaptation to smartphone technology, such as finger and foot tapping have comparable sensitivity and specificity to current non-clinician-acquired disability measures.
Results
We observed that finger and foot tapping can differentiate RRMS and progressive MS in a cross-sectional study and can also measure yearly and two-year disease progression in the latter, with better power (based on z-scores) in comparison to currently utilized 9HPT and 25FW.
Conclusions
Replacing the 9HPT and 25FW with simplified tests broadly adaptable to smartphone technology may enhance the power of composite scales for progressive MS.
Keywords
Introduction
Neurological disability is a loss of acquired functions caused by damage to the central or peripheral nervous system(s). Many clinical scales estimate disability, but none entirely captures all aspects of a complex disease process. Disability scales differ in their sensitivity (i.e. ability to detect minor changes reliably over time) and specificity (i.e. ability to differentiate changes caused by damage to the nervous system from random fluctuations in performance). Because the usefulness of a scale is determined by the balance between specificity/sensitivity characteristics and ease of administration, disability scales are usually tailored to a specific disease, capturing those functions that are most likely to be affected by the disease process.
In this regard, multiple sclerosis (MS), an inflammatory/demyelination condition of the central nervous system (CNS) is unique, because it affects any location in the neuraxis, but does so more or less randomly in individual patients. Consequently, measuring disability in MS has been a challenge. Historically, the most successful MS scale, the Expanded Disability Status Scale (EDSS) 1 is relatively insensitive in more advanced stages of the disease called progressive multiple sclerosis (PMS). As an alternative, the National MS Society task force developed a composite scale called the multiple sclerosis functional composite (MSFC), 2 consisting of measurements of hand functions (i.e. 9-hole peg test; 9HPT), walking speed (i.e. 25-foot walk; 25FW) and cognition (i.e. paced serial addition test). Unfortunately, the MSFC did not outperform the EDSS. 3 We have recently subjected the EDSS, MSFC components and two additional scales, Scripps neurological rating scale (SNRS) 4 and a cognitive symbol digit modalities test, 5 to thorough statistical analysis and combined scales with an independent cohort-validated sensitivity to detect yearly clinical worsening in PMS into the combinatorial weight-adjusted disability scale (CombiWISE), using genetic algorithm-based statistical learning6. CombiWISE combines four afore-mentioned scales using coefficients proportional to the sensitivity/specificity of validated components (i.e. SNRS > EDSS > 25FW > non-dominant hand 9HPT).
In view of the cumbersome nature of 25FW and 9HPT, combined with ever-increasing abilities of smartphone-based apps to measure certain neurological functions such as finger tapping, which were shown to be a useful outcome in other neurological diseases such as primary lateral sclerosis, 7 the goal of this study was to compare the utility of finger and foot tapping as alternatives to 25FW and 9HPT in MS disability scales.
Methods
Patient population
Patient demographics.

Average of ages at initial visit.
IPPoMS and RIVITALISE 8 clinical trials have an adaptive design, in which a total of 58 prospectively acquired candidate outcomes (i.e. eight clinical, one electrophysiological, one optical coherence tomography, seven magnetic resonance imaging (MRI) volumetric, nine quantitative T1 MRI outcomes and 32 diffusion tensor imaging MRI outcomes) during the one year pretreatment period were subjected to predetermined statistical analyses to select the most sensitive of these outcomes as the primary outcome for the treatment phase of the trials. The result of this undertaking was the development and validation of the CombiWISE scale, as the most sensitive and reliable outcome for measuring disability progression in PMS.
The prospective collection of finger and foot taps as exploratory outcomes started only two and a half years after the initiation of the IPPOMS trial and therefore these outcomes could not be included in the afore-mentioned comparative analysis. Instead, the present study (Table 1) includes cross-sectional data of HVs, untreated relapsing–remitting multiple sclerosis (RRMS) and PMS patients and longitudinal data on PMS patients, in which the first year is untreated and for the second year, one half of the cohort is randomly assigned to placebo, whereas another half of the cohort is randomly assigned either to oral idebenone (IPPoMS trial) or intravenous and intrathecal rituximab (RIVITaLISe trial).
Neurological scales
All clinical scales were collected within 24 hours of each other; MS-trained clinicians determined the EDSS 1 (from 0 to 10 in increments of 0.5) and SNRS 4 (from 100 to 0 in increments of 1). A different group of trained investigators, blinded to clinician’s rating collected 9HPT 9 (measured as time in seconds required for test completion by each hand; averaging two trials per hand), 25FW (measured as time in seconds required for walking 25 feet with or without the use of an assistive device; averaging two trials), finger and foot tapping (described below).
Finger tapping test
Patients tap a circular button (1 inch diameter) on an in-house developed apparatus (Figure 1(a)) with their index finger as fast as they can without moving the rest of their hand or arm. A 10-second trial is performed three times with each hand and the result is averaged. Results and handedness are prospectively recorded in a database. Analogously to 9HPT, the average number of taps obtained by the dominant hand (DH) and non-dominant hand (NDH) are added together to produce the finger taps outcome.
Finger tapping platform (a) and foot tapping platform (b).
Foot tapping test
Patients tap a 2 × 2 × 1 inch button elevated on a platform of an in-house developed apparatus (Figure 1(b)) with the ball of their foot while keeping their heel in contact with the platform. A 10-second trial is repeated three times averaged for each foot. The sum of these foot-specific averages produces the foot taps outcome.
Data collection and statistical analysis
All scores underwent weekly quality control (QC) before locking inputted values. The database automatically calculates CombiWISE (continuous scale 0 to 100) using the following formula:

A total of 289 patients was analyzed (35 HV, 94 primary progressive, 59 secondary progressive and 101 RRMS). The two progressive disease subtypes were combined because they showed no differences in the tapping results or the rate of progression.
Patients unable to perform the finger or foot taps tests received a score of 0. Patients unable to perform the 9HPT were scored 300 (max time in seconds allotted). Patients unable to perform the 25FW were scored 179.9 (max time in seconds allotted). If tapping data were missing due to technical reasons (e.g. malfunctioning of the apparatus), the time point was removed from the analysis.
Differences between cohorts were evaluated by analysis of variance with pair-wise differences based on the Student–Newman–Keuls method (if distribution passed normality test) and Dunn’s test (if failed normality test). Group differences between DH and NDH (from all collected data points) were calculated using the paired-parametric t-test (if distribution passed normality test) or Wilcoxon sign-rank test (if failed normality test).
Cross-sectional and longitudinal correlations used the Spearman test because the majority of data were not normally distributed. The significance of change over time was calculated with the one-sample t-test with null hypothesis of 0% change. In the longitudinal analysis, 48 patients had tapping outcomes collected one year apart in the pretreatment period; of these, 31 (65%) patients had tapping outcome results two years apart, spanning one year of pretreatment and one year of treatment (active treatment or placebo; cohort remains blinded).
To compare sensitivity between different outcomes, z-scores were calculated as an average of longitudinal change divided by variance of that change (i.e. ratio of mean change/standard deviation (SD)), as this measure is directly related to the statistical power to detect change in the outcome(s).
The arbitrary P value of 0.05 was used as a cut-off of statistical significance.
Results
Finger and foot tapping reproducibly differentiates between RRMS and progressive MS patients in cross-sectional analysis
First we compared the sensitivity of tap outcomes in identifying differences in disability among diagnostic categories and compared this to traditional MS scales and the optimized CombiWISE scale.
Analyzing test results from initial visits only, finger taps, foot taps and total taps (i.e. sum of finger and foot taps) had comparable values in HV and RRMS patients, while patients with PMS had a significantly (P < 0.0001) reduced ability to tap, both with their fingers and feet (Figure 2(a)). HV, RRMS, and PMS patients averaged 184 (SD 28), 185 (SD 32) and 121 (SD 33) total taps, respectively. A similar relationship is seen with both 9HPT and 25FW, which discriminate RRMS from PMS, but not RRMS from HV (Figure 2(b)).
Differentiating subgroups of multiple sclerosis and healthy volunteers with results of tapping tests and other neurological tests and clinical scales of disability. Foot taps and total taps passed the normality test and the Student–Newman–Keuls method was used. All other comparisons were made using Dunn’s test, which only returns whether P < 0.05 or P > 0.05, and not an exact P value. (*P < 0.05, **P < 0.01, ***P < 0.001).
In contrast, two clinician-acquired MS scales, the EDSS and SNRS, as well as the composite scale CombiWISE were able to discriminate all three subgroups of patients with high statistical significance (Figure 2(c)).
Age did not correlate with tapping outcomes (only total taps are presented) in diagnostically homogeneous groups (see Supplementary Figure 1).
Effect of handedness on measures of fine finger movements
The machine learning algorithm used for development of the CombiWISE scale revealed significantly greater sensitivity of NDH 9HPT in detecting sustained disability progression in MS in comparison to DH 9HPT6. Therefore, we asked whether such an effect of handedness can also be seen in finger taps.
In both RRMS and PMS cohorts (but not in HV), NDH finger taps was significantly lower (RRMS, P = 0.0002; PMS, P = 0.0056) than DH finger taps (Figure 3(a)). In fact, the handedness effect was statistically more pronounced for finger taps in comparison to 9HPT (Figure 3(b); RRMS, P = 0.0012; PMS, P = 0.0079).
Non-dominant hand performs worse on both tests (fewer taps, longer 9-hole peg test time) in patients with multiple sclerosis, whereas there is no difference between the dominant hand and non-dominant hand in healthy volunteers (*P < 0.05, **P < 0.01, ***P < 0.001).
Correlation between tap outcomes, traditional MS outcomes and CombiWISE composite outcome
In order to assess whether finger and foot taps can substitute for 9HPT and 25FW in composite scales, we evaluated the correlation between finger taps and 9HPT and foot taps and 25FW. For completeness, we also evaluated correlations with other clinical scales.
As we expected, finger taps correlated strongly with 9HPT (Spearman rho 0.708; P < 0.0001) and foot taps correlated strongly with log-transformed 25FW (Spearman rho −0.795; P < 0.0001; Figure 4(a and b). In addition, we observed strong, statistically significant correlations between tap outcomes and all other measures of physical disability (Figure 4(c)).
Cross-sectional correlations of tapping tests with other neurological tests and clinical scales of disability. Analysis is based on results taken from the initial patient visit combining healthy volunteers, relapsing–remitting multiple sclerosis and progressive multiple sclerosis subgroups (*** P < 0.001).
Foot taps and sum of finger and foot taps have slightly enhanced sensitivity to detect yearly accumulation of disability in progressive MS in comparison to 9HPT and 25FW
The sensitivity of the test to detect the development of disability in time was assessed in the longitudinal paradigm. We focused this analysis on the PMS subgroup for two reasons: (a) We identified no significant differences between RRMS and HV in a cross-sectional study, demonstrating that 9HPT, 25FW, finger taps and foot taps are insensitive to detect disability progression in early RRMS. Furthermore, virtually all RRMS patients were treated during longitudinal follow-up, the majority with daclizumab, which has been shown to inhibit disability progression; 10 and (b) the need for the development of a sensitive outcome is greater for progressive MS, in which contrast-enhancing lesions are sparse and in which we could analyze longitudinal data in untreated subjects.
Analysis of yearly change in PMS cohort (N = 48).

Only CombiWISE, EDSS and SNRS had higher sensitivity to change compared to total taps.
Analysis of change over two years in PMS cohort (N = 31).

In the second year, subjects are treated with placebo or trial drug.
Foot taps has the second highest sensitivity to change based on z-score (0.749) compared to all other measures.
When correlated with disability scales, the yearly change in finger taps did not correlate with the yearly change in 9HPT (Spearman rho = −0.251, P = 0.085) while Foot Taps correlated strongly with yearly change in 25FW (Spearman rho = −0.521; P < 0.001). Although finger taps did not detect significant change over one year, it correlated with measured changes in CombiWISE (Spearman rho = −0.407) and SNRS (Spearman rho 0.328), more so than foot taps, 9HPT or 25FW did with these clinical scales. Total taps correlated more strongly with CombiWISE (Spearman rho = −0.417) than finger taps. Finally, only NDH finger taps correlated with EDSS (Spearman rho = −0.340) (Figure 5(a)).
(a) Spearman correlation table of percentage change over one year. (*P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001). Only progressive multiple sclerosis (PMS) patients are included (N = 48). Total taps has the strongest correlation with CombiWISE while finger taps has the strongest correlation with SNRS among neurological scales. (b) Spearman correlation table of percentage change over two years. (*P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001). Only PMS patients are included (N = 31). Finger taps has the strongest correlation with all clinical and composite scales (CombiWISE, SNRS and EDSS).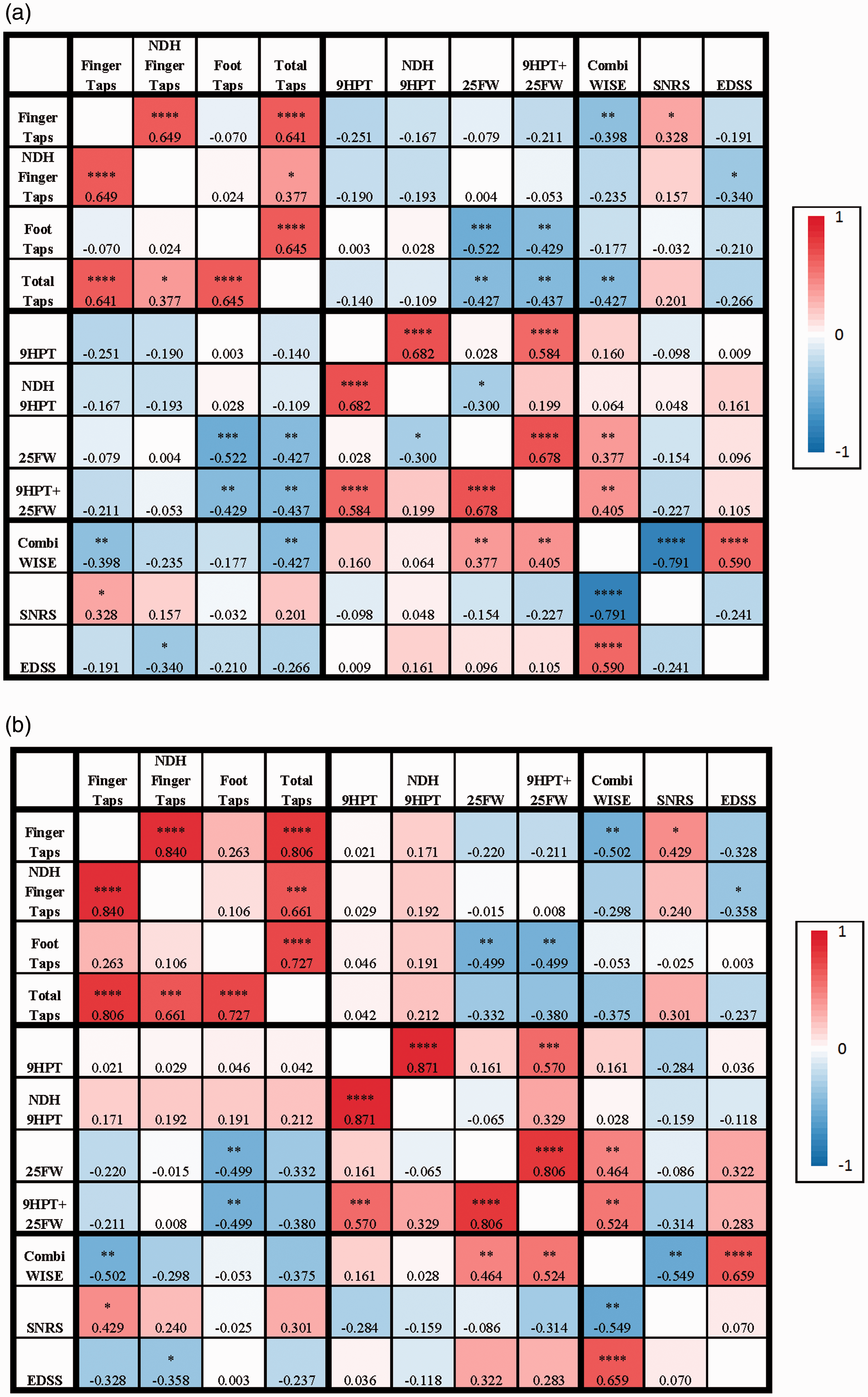
When percentage changes over two years were correlated, similar results were observed (Figure 5(b)). Finger taps outperformed foot taps, total taps, 9HPT, 25FW and the combined 9HPT plus 25FW measure in correlation with EDSS (Spearman rho −0.328); SNRS (Spearman rho = −0.429) and the CombiWISE (Spearman rho = −0.501) (see Supplementary Figure 2).
Extended sensitivity of finger taps, but not foot taps in patients with severe disability
The major problem with 9HPT and 25FW in progressive MS trials is the ceiling effect: i.e. patients reach the state when they are unable to perform either test. Therefore, we asked whether finger and foot taps have an extended sensitivity range in comparison to these traditional MS outcomes.
Sixty per cent (9/15) of patients who were unable to walk could perform foot taps. However, 84% (16/19) of patients who could not do foot taps could still walk. Of the patients who could not perform the foot tap test but could still walk, 75% (12/16) used a walker and 25% (4/16) used a cane. Many of these patients used upper body strength and lower body spasticity to walk even with severe disability of their feet/legs.
Extended sensitivity of tests when patients fail to perform other tests.

Asterisks indicate the number of patients that were able to complete that test during one visit, but eventually were unable to perform that test during subsequent visits.
Discussion
The goal of the current study was to compare the utility of finger and foot taps as potential future replacements of 9HPT and 25FT in MS composite scales, especially because such simplified tests can be administered by patients themselves, more frequently than clinic visits, using smartphone technology. We found both tests to have slightly better performance (based on z-scores, which are directly related to power) in one year untreated and two year partially treated longitudinal paradigms, in comparison to 9HPT and 25FW. Therefore, replacing these currently utilized, cumbersome tests with their simplified tapping versions should enhance, rather than decrease, the power of composite clinical scales for drug development in PMS, and it is worthwhile to invest in the further development of such outcomes.
The limitation of the current study is the relatively small cohort sizes (although comparable to a single arm of current, investigator-initiated phase II trials in progressive MS) and the absence of an independent validation cohort. This provides some level of uncertainty when it comes to effect sizes (e.g. foot taps slightly outperformed clinician-measured scales in our two-year longitudinal assessment of PMS patients, which may not happen in a larger cohort). However, we believe that this pilot study provides strong evidence that finger and foot taps are comparable to currently utilized 9HPT and 25FW, and larger confirmatory studies should adopt smartphone-based technology rather than our in-house developed apparatus to investigate the full potential benefit of these simple outcomes, including their more frequent assessments.
We also hypothesized that by simplifying the task, finger and foot taps will plateau later than 9HPT and 25FW. This hypothesis was validated only partially: 73% of patients who fail to do the 9HPT were still able to perform finger taps but not vice versa. However, for foot taps, 60% of patients unable to walk were still able to perform foot taps, but also the inverse was true: 82% patients unable to foot tap were still able to walk. We interpret these data as evidence that while finger taps and 9HPT are measuring completely overlapping domains (i.e. fine finger movements), foot taps and walking are reflecting incompletely overlapping domains, with foot taps measuring distal weakness/coordination, while ability to walk is mostly affected by proximal weakness/coordination. This suggests that rather than replacing 25FW with foot taps, the two measures provide somewhat complementary information.
The major advantage of the finger and foot taps is their potential to be captured via smartphone apps, thus providing denser longitudinal data, e.g. measured multiple times per day, at the convenience of patients’ homes. Apple has recently released the ‘research kit’, an application that allows researchers to create outcomes on an iPhone interface. The mPower 11 study of Parkinson’s disease has successfully monitored 10,000 participants using such an iPhone app interface. One of the utilized tests is a tapping test in which patients tap the screen for 20 seconds. The app calculates and longitudinally tracks daily averages, providing potentially more reliable information than office-based cross-sectional measurement. We can envision this app adapted to foot taps by printing low-cost scaffold on a three-dimensional printer that serves as a foot support and contains indented opening for the specific smartphone.
With today’s smartphones equipped with sensors such as an accelerometer (with shaking meter), gyrometer, inclinometer, light sensor and orientation sensor, the possibilities for devising simple but reliable measurements of varied neurological functions are almost unlimited. However, such measurements should be tested against current clinical scales, as performed in this study, to understand the neurological domains these new measures capture and the clinical relevance of measured changes. Assembling such novel independently validated measures into composite scores using statistical optimizations or other forms of machine learning has the potential to develop highly sensitive, specific and patient-tailored disability measures that can be used in clinical trials, but also in daily clinical practice.
Footnotes
Acknowledgements
The authors acknowledge the clinicians Alison Wichman and Jamie Cherup and nurses Jenifer Dwyer, Laura Kannaian, Fee Pee Ansher, Naomie Gathua for their extraordinary patient care, and Kewonie Pumphrey for patient scheduling. They also thank Brandon Loughridge who was instrumental in setting up the tapping system, as well as present and past post-baccalaureate fellows of Dr Bielekova’s lab for collecting all of the tapping data used in this study. Finally, the authors thank all patients, their caregivers and healthy volunteers, without whom this work could not be possible.
Conflicts of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the intramural research programme of the National Institute of Neurological Disorders and Stroke (NINDS) of the National Institutes of Health (NIH).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.