
Abstract
Multiple sclerosis (MS) is a chronic, degenerative autoimmune inflammatory disease of the central nervous system. The prevalence is different in every continent, changing according to geographical and environmental characteristics. The areas with the highest prevalence in the world are Europe and North America. In Latin America, the prevalence is higher in areas where there was greater European migration, as in the case of Argentina, Chile, Brazil, Uruguay and Mexico, and there have been no identified cases amongst native Indian populations. It should be considered that environmental factors may influence the prevalence of MS in Latin America, and it seems as if there are protective factors such as exposure to ultraviolet radiation and the presence of parasitosis.
Introduction
Multiple sclerosis (MS) is a chronic, degenerative autoimmune inflammatory disease that affects the central nervous system (CNS) leading to demyelination and axonal damage of the brain and spinal cord.1,2 This disease is more common in females and mainly affects young people between the ages of 20 and 40. 3 MS is common in Europe, USA, Canada, New Zealand and southern Australia. It is rare in Asia and for a long time was considered a rare neurological disease in areas such as the American Tropics and the southern latitudes of the Americas, known today as Latin America (LA).4-6 However, in recent years there has been an increase in the frequency of cases of patients diagnosed with MS in LA. This is due to a number of factors, including increased diagnosis obtained through the advent of magnetic resonance imaging (MRI), an increased number of neurologists and improved modern medical education. 6
The ethno-geographical concept of LA first appeared in the 19th century to identify a Spanish- and Portuguese-speaking region of the American continent. The precise delineation of the region is variable. However, it is considered that, geopolitically, LA extends from the US border with Mexico (latitude 32° North) to the Patagonia region of Argentina and Chile (latitude 56° South). The Spanish-speaking countries of Cuba, the Dominican Republic and Puerto Rico are traditionally considered to be part of Latin America. 4 It is estimated that about 580 million people live in this region.3,7 Because of centuries of intermixing, it is a heterogeneous and genetically complex population, with a mix of Native Amerindian, white European Caucasian and black African cultures, which has resulted in a predominant ethnic Latin American Mestizo. 7 There are few epidemiological, genetic or environmental studies that explain the presence of MS in LA. Therefore, in this review we have conducted a critical analysis of the presence of MS in LA based on evidence from epidemiological, genetic and environmental studies and have established its relationship with European migration.
Epidemiology of multiple sclerosis in Latin America
The prevalence of MS throughout the world is different on every continent, changing according to the geographical, ethnic and environmental characteristics of the region.
3
In LA, the picture is similar. Several epidemiological studies have shown that the prevalence of MS is variable and seems to increase as we move away from the equator to the north or south. Thus, the highest prevalences of MS are found in Mexico, Argentina, Chile and Uruguay.
3
For example, in northern Mexico, in San Pedro Garza Garcia (state of Nuevo Leon), the prevalence of MS is 30 per 100,000 inhabitants.
8
In Monterrey, the prevalence decreases to 7.5 per 100,000 inhabitants.
9
At the equator we see a different picture. In Quito, Ecuador, the estimated prevalence is 5.05 per 100,000 inhabitants, which is very similar to that reported in neighboring countries like Venezuela and Panama (5.26 and 5.24 per 100,000, respectively).10–12 As we move south of the equator, specifically in Lima, Peru, the prevalence increases slightly to 7.6 per 100,000 inhabitants.
13
On the other hand, Cochabamba, Bolivia is the region with the lowest number of MS cases in all of LA and the Caribbean, with 1.5 per 100,000 inhabitants.
14
In Buenos Aires, Argentina, as in northern Mexico, it has been observed that the prevalence increases: two studies have reported between 18 and 25 cases of MS per 100,000 inhabitants in this city.15,16 However, Córdoba, Argentina is the site of the highest prevalence of MS in LA, with 88 cases per 100,000 inhabitants.
17
A prevalence of 5.69 per 100,000 inhabitants has been determined in Chile,
18
but in the city of Punta Arenas, the prevalence increases to 14 per 100,000 inhabitants.
19
In Montevideo, Uruguay, like in Argentina and Chile, we find one of the highest prevalences in South America with a reported 21 cases per 100,000 inhabitants (see Figure 1).
20
Prevalence of MS in Latin America and the Caribbean.
By analyzing the data presented here, it is clear that the prevalence of MS in LA follows a similar pattern to the rest of the world because, as we can observe, the prevalence increases as we move away from the equator. This observation was confirmed by Risco et al., who showed that for every increase of one degree in latitude there is an increase in the prevalence of MS of 0.33 per 100,000 inhabitants. 21 This study included epidemiological studies carried out in South American countries (from Panama to Argentina). These findings were also found in Europe through a study conducted by Simpson et al., who demonstrated an association between MS prevalence and latitude, through a meta-analysis. 22 However, the increasing prevalence of MS per latitudinal degree in Europe is higher than in LA (1.29 vs 0.33 per 100,000, respectively).21,22 It is clear that in LA none of the prevalences described above equal or exceed those of the United States or Europe. For example, Scotland and Northern Ireland are the countries with the highest number of cases in the British Isles (>200/100,000).22,24 This is followed by countries such as Switzerland, Denmark and Norway (>150 per 100,0000 inhabitants),25–27 which are all very similar to those found in North America (Olmsted County-Minnesota) and Canada (Saskatoon), each with a prevalence greater than 200 cases per 100,000 inhabitants.28,29 In general, the etiology of MS is still unknown. It is thought to be a multifactorial disease with relative contributions of genes and environmental factors, though their influence in the pathogenesis of MS is still a matter of discussion. 30
Environmental factors and their relation to the prevalence of multiple sclerosis in Latin America
25-hydroxyvitamin
The largest source of 25-hydroxyvitamin D (25-[OH] D) comes from the synthesis of vitamin D by the skin when exposed to sunlight (specifically ultraviolet B), 31 whose duration and intensity is dependent on the latitude. 5 It is well known that as the latitude increases (both north and south of the equator), the amount of ultraviolet B radiation (UVB) decreases because the sunlight must travel a longer distance through the earth’s atmosphere before reaching the planet’s surface. 32 At a latitude of 42 degrees during winter UV radiation is absorbed by the atmosphere, thus there is no production of vitamin D in the skin during this time at this latitude. In Europe and North America there is a relationship between levels of 25-(OH) D and the risk of developing MS. This has been demonstrated by Salzer et al., 33 who reported through a case control study in a population from Switzerland that serum levels of 25-(OH) D greater than 75 nmol/l were associated with reduced risk of MS. Munger et al., 34 conducted a prospective longitudinal study involving 257 patients with MS in which two measurements of 25-(OH) D were performed before developing the disease. Three groups of patients were considered for analysis: white, non-Hispanic black, and Hispanics. In the group of non-Hispanic whites, MS risk decreased with increased serum levels of 25-(OH) D, whereas the relationship between levels of 25-(OH) D and MS was not significant within groups of non-Hispanic blacks and Hispanics.
The findings described above raise a question: if the prevalence of MS in Latin America depends on latitude and the levels of UV radiation and vitamin D, why are there several examples of countries or cities on the same latitude where the prevalences are significantly different? This can be seen in the example of Monterrey (Mexico) and Cuba, the latter being at a lower latitude in relation to Monterrey but with a higher prevalence of MS (7.5 vs 25 per 100,000, respectively).6,14,35 Citing another example to the south, we see a similar phenomenon with Punta Arenas located at latitude 53°, which has a lower prevalence of MS than Montevideo and Buenos Aires, both located at latitude 34°. 6 Therefore, it appears that in LA, latitude and vitamin D levels do not influence MS prevalence to the same extent as in other regions of the world. In this regard, a study conducted in Mexico by Rito J et al., 36 which included 50 patients with MS, showed that serum levels of 25-(OH) D in MS patients were similar to a control group (22.3 ng/L vs 23.3 ng/L, respectively (p = 0.2)). A study conducted in Quito, Ecuador, found similar results − no significant difference between serum levels of 25-(OH) D in patients with MS and the control group (31.89 vs 30.38 ng/L, respectively (p > 0.05)). 37 From what is described above, it is clear that unlike Caucasian populations where there is an effect of latitude and vitamin D on the prevalence of this disease, in LA the effect is minor and due partly to the genetic distribution of populations. A complex mixture of the Native-Andean peoples with European and African immigrants has resulted in a concentration of Caucasian populations in the south of LA. For example, in Argentina the population is predominantly Caucasian, while in Ecuador the population is predominantly Mestizo. It is possible that the Argentinian population has a higher risk of MS than the Ecuadorian population because of their genetic background. 36
Vitamin D acts by binding its receptor (VDR) located on the surface of cells throughout the body. Once binding occurs, the receptor-ligand complex is internalized and forms a heterodimer with the retinoid X receptor. Subsequently, this heterodimer translocates to the cell nucleus where it binds to the vitamin D response element (VDRE) located in the promoter region adjacent to the allele human leukocyte antigen (HLA) DRB1*1501 (dominant in northern European populations). 32 Ramagopalan et al., conducted a study that identified a VDRE motif within the HLADR-B1*15:01 promoter region that enhances gene expression in response to vitamin D stimulus, while other HLADRB1*15 alleles studied were found to carry an alternative promoter sequence that is nonresponsive to vitamin D. 37 This study indicated vitamin D levels as a strongly possible environmental candidate in the development of MS in European populations.
Hygiene hypothesis in multiple sclerosis
During last century in delevoped world, it has been an epidemic of autoimmune and allergic diseases (3 and 50% respectively). The increase is too rapid for significant genomic alterations to occur and therefore implies that there has been a critical environment change in this period. 30 On this matter there is a theory (the hygiene hypothesis) that the prevalence of MS is rare in regions where the prevalence of parasitoses such as T. trichuria are greater than 10%, as is the case in LA countries. Thus, in areas where the frequency of parasitosis is low, MS prevalence increases, as is the case in industrialized countries. 39 Correale et al., showed that in MS patients infected with helminths, the disease activity was lower compared to patients who were not infected with them.40,41 This environmental factor could be taken into account in order to explain the lower prevalence of MS in Latin America compared to countries in Europe or North America. However, besides possible environmental factors, it is important to consider the presence of exogenous factors, such as migration of European populations to LA.
Caucasian and/or European migrations around the world
Poser raised a hypothesis that MS was the result of a series of genetic mutations that occurred in Scandinavia during the first millennium, with a subsequent spread to the rest of Europe through Viking migrations and invasions. 42 Once the disease was established in Europe, it was spread throughout LA and other continents through European migration before and after the 18th century.
In Figure 2, we can see the migratory flow of European populations to other continents before and after the 18th century. The territory of North America was one of the regions that Louis XIV claimed for England in the struggle for colonial supremacy. After Columbus’s voyages, only a handful of Spaniards continued in the conquest of the northern lands, while the bulk of Spanish conquistadors headed south to Mexico.
43
Around the year 1600, before the English established their first settlement, the Spaniards had approximately 200,000 people living in established settlements in the present-day states of California, Texas and Arizona (southwestern North America).
44
By 1621, the Dutch West India Company founded the colony of New Holland, which included trading posts along the Hudson River with settlements in Albany and New Amsterdam (present-day New York City).
43
However, there were expeditions organized by the British Crown and later by the French, which truly colonized the region. The first English expeditions went to Virginia in 1607. By 1626, the English had founded a trading post on Manhattan Island in New Amsterdam. In short, the British founded 12 colonies over 80 years. Other territories under British influence were those of Australia and New Zealand. Although originally discovered by the Portuguese in 1600, James Cook, took possession of these territories under the name of Great Britain in 1700.
44
European migration before and after the 18th century.
In Europe, MS is more common in southern Scandinavia, northern Germany, the United Kingdom, and Italy, and is less frequent in northern Scandinavia, France, Spain and in eastern Mediterranean countries. In the United Kingdom, the regions of highest prevalence are northeast Scotland and the Orkney and Shetland Islands. In Italy, there is a marked difference in the prevalence of MS between regions and islands that are geographically close, but different in genetics and culture. In North America, MS frequency is the highest in the Midwest and is lower in the Mississippi Delta region. A latitudinal gradient exists in the white population in Australia, with the highest gradients in the south relative to the north.45,46
If we compare the historical record with the prevalence of this disease in various regions of the world, we can see that MS is common in areas that were populated by people from northern Europe and infrequent in regions where the native population is present (Africa and Asia) (Figures 2 and 3).28,45 To cite an example in South Africa, MS is more common in immigrants from southern Europe, lower in African populations, and occasional in the Mestizo populations of the Cape region, which has African and European ancestry.
45
Another example (though controversial) is what happened in the Faroe Islands before the Second World War. There were no reported cases of MS on the island, yet 48 cases have been reported between 1943 and 1989. It is thought that this is related to the settlement of 8000 British troops on the islands during the war, suggesting the transmission of the disease by carriers from a high-incidence population.
47
However, this is simply an intriguing hypothesis, as there may be other explanations, such as exposure to environmental factors or the presence of a recessive allele with reduced penetrance.
48
Map of MS prevalence worldwide.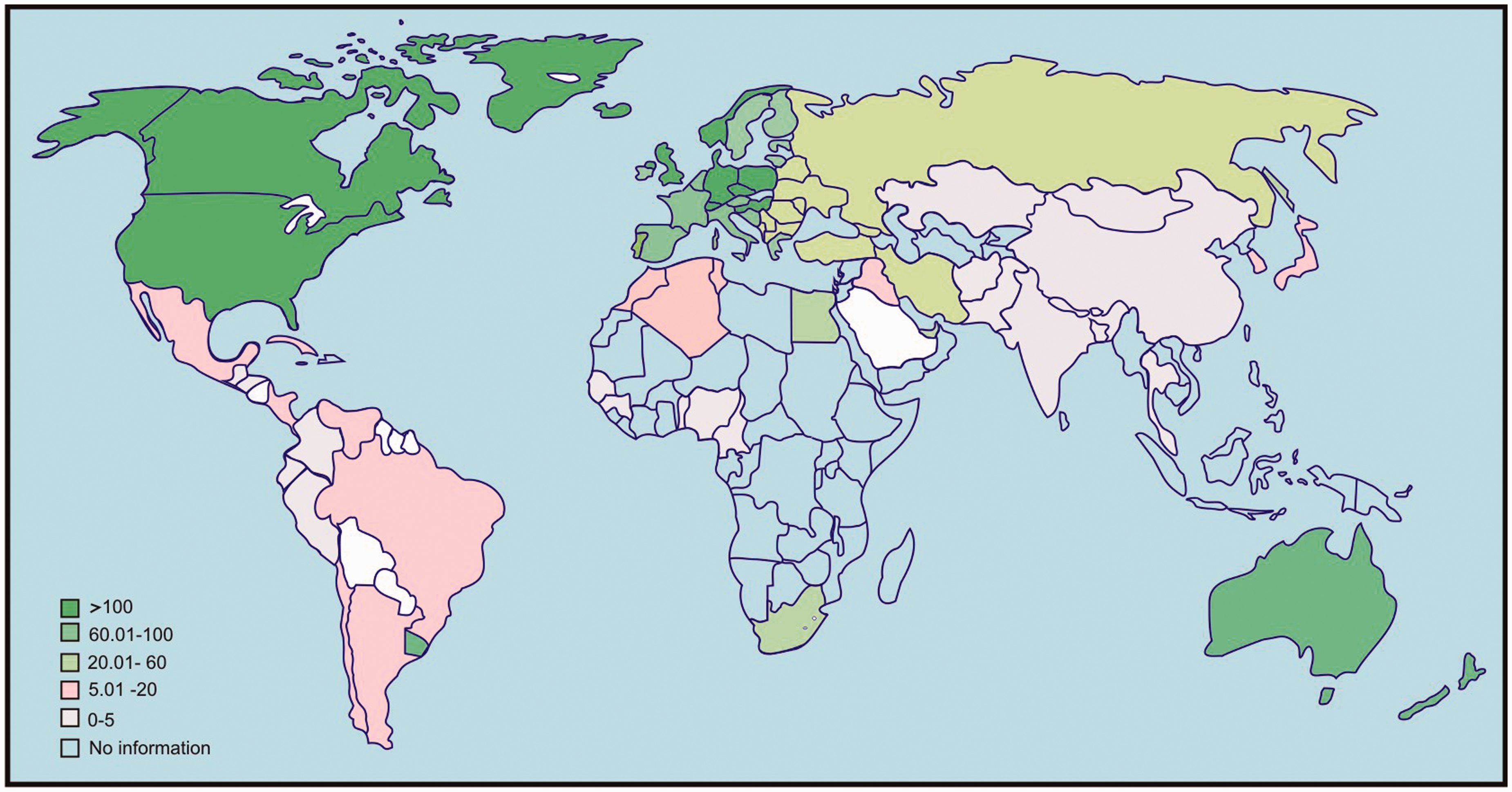
Caucasian and/or European migrations to Latin America
European emigration to LA has resulted in a considerable number of Europeans living in Argentina, Brazil, Uruguay, Venezuela, Cuba, Mexico and Chile, where the largest number of people with European ancestry are concentrated. The principal European migrations into LA were: Spaniards into Argentina, Venezuela, Brazil, Cuba and Mexico; Italians into Argentina, Brazil and Uruguay; Germans into Argentina, Brazil and Chile; French into Argentina, Brazil and Uruguay; English into Argentina and Chile.49,50
Proportional genetic admixture of EUR, AFR and AMR populations in Latin American countries and its relationship to MS.

AFR: African ancestry; AMR: Amerindian ancestry; EUR: European ancestry; MS: multiple sclerosis.
Caucasian and/or European migrations to Latin America and the relationship to multiple sclerosis
A multicenter cross-sectional study involving 22 MS centers in Brazil, Venezuela, Paraguay and Argentina studied the spectrum of demyelinating diseases, identifying a cohort of 1474 patients with MS. In this group of patients, a differentiation according to skin color/ethnicity was made and found that 66.7% of MS patients were white, 26.3% black and only 5.7% Mestizos. The demographic and clinical characteristics of the disease in this cohort were not different from what was published in European or American studies. Only 1% of patients with MS who came from Argentina were non-white (Asian). In Brazil, 36.8% of MS patients were African and Mestizo (484 African and 13 Mestizo). The remaining patients were white. An important finding of this study was that native Indians were not affected by MS. 49 Brum et al., showed through ancestry informative markers applied to 128 MS patients from Brazil that the contribution of European ancestry to the development of MS in this cohort was 78.5%. 58 As in the previous study, they did not identify Amerindian genes in patients with MS. Flores et al. conducted an epidemiological study with the objective to determine whether the Lacandon population (a pure Amerindian ethnic group of Mexico) had signs or symptoms consistent with MS or other demyelinating diseases. 4 The study included 5372 Lacandonians. No evidence of MS or other demyelinating diseases was found in this cohort. Abad et al., in their population-based study conducted in Ecuador, identified 103 patients with MS. These patients lived in cities where the population is predominantly white and Mestizo (Quito, Guayaquil and Cuenca). No MS cases were identified in cities where there was native Indian population. 10 Despite the implications of the works described above, more epidemiological studies are needed to support this relationship between MS and European and/or Caucasian migration.
From the studies described above, we can observe the absence of MS in Native American populations. It is possible that this population is protected against MS and other autoimmune diseases because of their ancestral genetic profile. 4 However, there is a native population in North America where the presence of MS has been demonstrated, a First Nations community in the province of Alberta, Canada. In this population, Svenson et al. showed a prevalence of MS of 56.3 cases per 100,000 inhabitants.59 The high prevalence in this population could be explained in part by the presence of an environmental factor. However, there are several points that should be taken into consideration with this study. First of all, the prevalence in this population was lower when compared to the prevalence in the rest of the province where the population is mostly white (56.3 vs 262 per 100,000 inhabitants). Also, this study did not establish whether any of the subjects had a European ancestor. Finally, it is known that this population has had increased genetic admixture with the rest of the population of this province. These factors could explain the presence of MS cases in this native population.
Based on the studies presented in this article, we could hypothesize that the variability of the prevalence of MS in LA depends on environmental factors, but that an exogenous factor is also at work (migration of European populations). By comparing Figures 2 and 3 we can see that in LA, as in other regions of the world, there are areas of higher prevalence of MS where there was migration of populations from high-prevalence regions, such as Spain and Italy, and we can see that the frequency of the disease is lower in countries where native populations exist (as in the case of Bolivia, Peru and Ecuador).
Susceptibility genes for developing multiple sclerosis in Latin America
Regions in the short arm of chromosome 6 p 21–23 play a decisive role in the genesis of MS − specifically, the locus of the major histocompatibility complex (MHC), which in humans is called the HLA. It is the largest and most consistent genetic determinant identified in MS. It is well established that the HLA-DRB*1501 allele is associated with susceptibility to developing MS in Caucasian populations. 60 Zhang et al. conducted a meta-analysis of case control studies in Caucasian populations. 61 This meta-analysis included 25 European studies, three Australian, threee Latin American, one Canadian and one English. This study confirmed an increased susceptibility to develop MS in Caucasians who were DRB1*1501-positive. It also found that the DRB1*03 allele was significantly higher in MS patients than in control groups, indicating that this allele can also be a risk factor for developing MS. Conversely, the DRB1*14 and DRB1*07 alleles found in this population were protective. Healy et al. found that the HLA-B*4402 gene can reduce susceptibility to MS and its presence was even related to the preservation of brain volume and a reduction in the number of lesions on T2-weighted MRI sequences. 62
Unlike the large number genetic studies of Caucasian populations, in LA few genetic studies have been carried out in the region. Genetic studies in LA would offer us an opportunity to examine the predisposition to developing MS due to the influence given by the mix between Native Americans, Europeans and blacks that occurred 10 or 20 generations ago. Rojas et al. conducted a systematic review of case control studies from countries such as Argentina, Colombia, Mexico and Brazil. 63 It was found that the DRB1*1503 and DQB1*0602 alleles, as well as the DRB1*15, DQB1*06 and DRB1*1501 alleles, were risk factors for developing MS. In this study, the presence of the DRB1*15 allele was more frequent in Caucasian (33.9%) and white populations (24.7%) who came from Argentina and Brazil.64,65 As we have observed in the works described in this article, genetic factors play a major role in the development of MS in Europe but not in other populations. MS is rare amongst Samis, native Siberians, Chinese, Japanese, Black African and American Indian populations. The presence of the HLA-DRB*15 in all of those ethnic groups is very uncommon or rare. In LA, there is a trend towards an increase in the prevalence of MS due to genetic introduction of European HLA-DRB*15. 66
In conclusion, after the analysis of the information presented in this article, we believe that the prevalence of MS in LA is partly due to the presence of an exogenous factor that came through European migration, which would explain why several regions that are geographically close and exposed to similar environmental factors, nonetheless have variable prevalence of MS. As we saw, in LA environmental factors have a protective effect as in the case of parasitic helminth infections or increased exposure to UVB radiation. Many of the arguments here are hypotheses, so it is imperative to develop genetic, epidemiological and environmental studies that allow us to find an explanation for the existence of MS in LA.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.