
Abstract
Novel epidemiological data have appeared in recent years in Latin America (LATAM). The objective of this study was to perform an updated systematic review of the epidemiology of the disease reported in LATAM.
Methods
We conducted a systematic review of published epidemiological articles from January 1995 to December 2016.
Results
Incidence data were found in four studies and ranged from 0.3 to 3 annual cases per 100,000 person-years. Prevalence was reported in 13 studies and ranged from 0.83 to 38.2 cases per 100,000 inhabitants. Two studies showed an increase in prevalence and incidence in the last five years in specific regions.
Conclusion
The study provides updated information on epidemiological features of MS in the region. The frequency reported is lower compared with some European and North American countries; however, due to recent observations, studies including follow-up assessment of prevalence and incidence should be conducted in the region.
Introduction
Systematic study of multiple sclerosis (MS) in populations started in 1929 when 40 cases in North Wales were ascertained, estimating a point prevalence of 13 per 100,000 inhabitants. 1 Today, there are several publications that deal with prevalence and incidence of MS throughout the world; nonetheless, despite this wealth of data, current knowledge of MS epidemiology in Latin America (LATAM) is limited.2–5
An uneven distribution of MS in LATAM was described. 3 LATAM presents different population genetics and environmental aspects around the region, with European and African immigrants resulted in a concentration of the Caucasian population in the southern regions of the continent whereas in the northern region, the population is predominately Mestizo. 6 In terms of epidemiological observations in the region,3,7 information regarding incidence, prevalence and other aspects were described and allowed us to understand and compare the disease in LATAM with other regions of the world; however, novel data have appeared over the last few years that make the updating of the information about the frequency of the disease in our region relevant in order to better understand the distribution of the disease.
Considering that the distribution of MS has substantial differences in LATAM regarding other world regions and that novel epidemiological data emerged during the last years, the objectives of the present study were to perform an updated systematic review of the epidemiology of the disease reported in LATAM and discuss the findings.
Material and methods
Search strategy and selection criteria
We conducted a systematic non-language-restricted literature search of LATAM MS reports from January 1995 to December 2016 using electronic databases included in Cochrane CENTRAL, MEDLINE, EMBASE, and LILACS with the following search terms:
multiple sclerosis and Latin America multiple sclerosis and population* multiple sclerosis and epidemiology multiple sclerosis and prevalence multiple sclerosis and incidence multiple sclerosis and etiology*
Selection criteria
The review was restricted to published research articles in order to perform a complete evaluation of the quality of the studies included in our review (setting, type of study, study population, definition of MS, prevalence and incidence rate, and 95% confidence interval). Population-based studies were included if data were collected through standardized questionnaires, if raw population numbers were available for data confirmation and if MS was diagnosed, based on validated diagnostic criteria.8–11 We also included studies involving a network of hospitals that fulfilled previous criteria. Studies that were based in a single institution or did not involve a network of hospitals serving a well-defined general population were excluded.
Data extraction and assessment of study quality
Two of the authors agreed on the data to be extracted. Data included the study period, details of the study population and diagnostic selection criteria. One of the reviewers (JIR) extracted data using a data extraction form, while a second reviewer (EC) confirmed the data. Each study was evaluated on the following items: type of study design; description of study population; and adequacy of case definition based on validated criteria.8–11 Those studies in which the items were not reported or unclear were excluded.
Assessment of risk of bias
Methodological quality used in the reviewed studies and risk of bias was assessed by two reviewers using a modified checklist available in Strengthening the Reporting of Observational studies in Epidemiology (STROBE) 12 and in Fowkes and Fulton. 13 We estimated a bias risk summary considering six criteria: methods for selecting study participants, methods for measuring exposure and outcome variables, methods to control confounding, design-specific sources of bias, comparability among groups and statistical methods and declaration of conflicts of interest.
Results
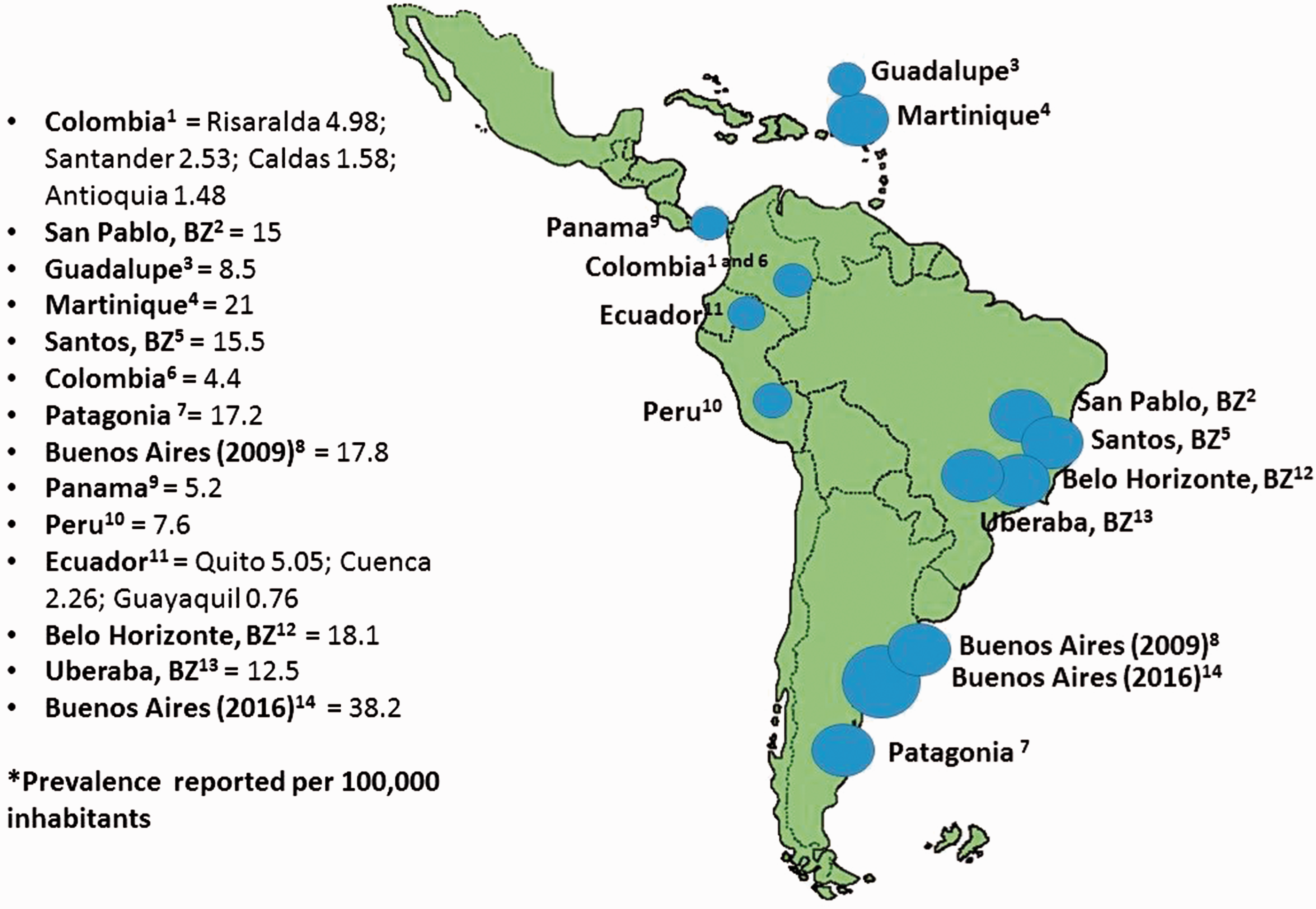
A total of 645 citations were identified. After reviewing titles and abstracts, 65 studies were considered eligible. After full-text review, 14 met inclusion criteria and were selected for data abstraction and analysis of incidence-prevalence (Figure 1).14–37 Information was obtained from nine countries (Figure 2). Regarding incidence, we found five studies (French West Indies, Argentina and Panama) that evaluated this issue.16,19,24,38 Of these five studies, one reported incidence from a period of 16 years that was later extended to 22 years. This study identified an increase in incidence during the follow-up period.
38
Incidence values ranged from 0.15 to 3 annual cases per 100,000 person-years (Table 1). Regarding prevalence rates, 13 identified studies assessed prevalence in the region (Table 2). Reported prevalence ranged from 0.75 to 38.2 cases per 100,000 inhabitants (Table 2). The reported prevalence was lower in Ecuador, Colombia and Panama (range = 0.75 to 6.5 cases per 100,000 inhabitants) while Brazil and Argentina reported 12 to 38.2 cases per 100,000 inhabitants.
Flow of studies through the review. City-country multiple sclerosis prevalence reported in the studies included in the review. Reported multiple sclerosis (MS) incidence in Latin America and the Caribbean. CI: confidence interval; N: north; S: south. Reported multiple sclerosis (MS) prevalence in Latin America and the Caribbean. Studies used capture-recapture method to estimate global prevalence. Cases included were adjusted cases. 95% CI not reported in the original publication. CI: confidence interval.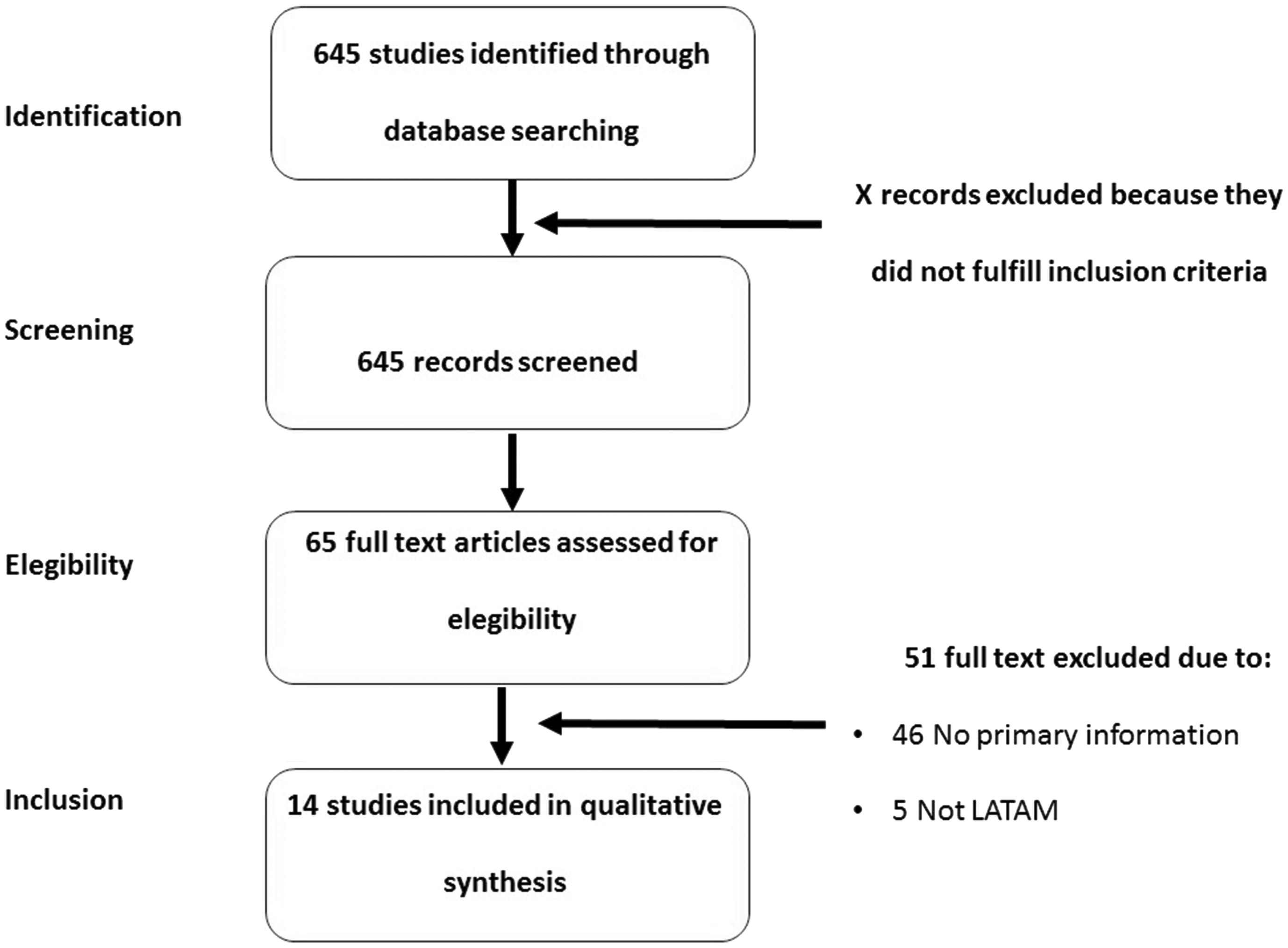


Discussion
During the last decade, there has been a surge of interest in the epidemiology of MS in LATAM, and several investigations have begun to provide a reasonable estimate of the disease in the region. In this updated review of the frequency of MS in LATAM, we found that the incidence reported ranged from 0.15 to 3 cases per 100,000 person-years. Prevalence ranged from 0.75 to 38.2 cases per 100,000 inhabitants in 13 studies analyzed.
Reported prevalence and incidence of MS in the region were substantially lower than data found in developed countries, even we observed significant differences between countries from LATAM. 6 Reasons for these differences were attributed to certain environmental and genetic factors.39,40 The distribution of population genetics in LATAM could account for the observed differences. As previously mentioned, a complex mixture between Andean natives with European and African immigrants resulted in a concentration of the Caucasian population in the southern regions of the continent whereas in Colombia and the northern region, the population is predominately Mestizo. 6 It is possible that the Caucasian population has a higher risk of MS than the non-Caucasian population as previously described. Risco et al. found a continental South-North gradient in LATAM between Panama and Argentina; however, they did not find a clear trend of increasing MS prevalence and latitude within Colombia, Ecuador or Argentina, suggesting that other human factors such as ethnicity play an important role in determining the geographic distribution of MS regardless of the impact of latitude. 6 Cabre et al. evaluated the role of migration in the frequency of the disease in French West Indies. 41 They found that the prevalence of MS was twice as high in Caucasian migrants as in non-migrants and that the prevalence was very high if this stay in a temperate region occurred before the age of 15 years. 41 A clear dose-response relationship between the duration of residence out of the French West Indies and the prevalence of MS was also found. A possible explanation provided by authors was that migration of Caucasian genes into the Afro-Caribbean population could serve as a vector for the introduction in the French West Indies of possible infectious environmental factors operating, in particular, before the age of 15 years. These environmental changes may either trigger or protect from the disease. 41 Those findings were in line with other studies of Caucasian populations migrating from high-prevalence areas to low-prevalence areas, suggesting that the risk of acquiring the disease is determined before the age of 15 years (for populations from the United Kingdom who emigrated to South Africa 42 and for Jewish populations emigrating to Israel, for example 43 ). It is important to mention that prevalence is not, however, the best epidemiological instrument for evaluating the change in risk induced by migration.
Interestingly, in the updated information gathered we found two studies that described an increase in prevalence of MS after 20 years as well as an increase in incidence of MS during follow-up, mainly in females. These findings are in line with previous studies performed in other regions of the world that showed an increase in MS incidence and prevalence.44–46 Hirst et al. in South East Wales displays an increase of 45% in the prevalence of MS, from 101 to 146 per 100,000 population over 20 years, 47 while Svenningsson et al. in 2015 published research performed in Vasterbotten County, Sweden, in which a significant increase in the prevalence of MS over a period of 10 years was observed (from 188 to 215 per 100,000 inhabitants). 48 Fernández et al. reported in 2012 a prevalence of MS in Malaga, Spain, by using the capture-recapture method of 125 per 100,000 inhabitants, higher than previously published in the region. 49
The other possible cause related to the low frequency and uneven distribution of the disease in the region could be attributed to environmental factors. As latitude increases, the intensity and duration of sunlight decrease. Many studies have suggested that a lower exposure to sunlight in high latitudes is associated with a greater risk of MS.39,50 This may explain the increased risk observed in areas located at a greater distance from the equator. Also, it has been proposed that improved hygiene, which partially explains the reduced rate of infections in Western countries, might be a starting point to clarify the increased incidence of allergic and autoimmune diseases in a northern hemisphere population. 51 Several factors could contribute to the so-called hygiene hypothesis; 51 however, this social effect is observed in many areas of LATAM and could be a factor involved in the low prevalence of autoimmune diseases observed in the region. 52 Finally, subdiagnosis may contribute to underestimating the MS prevalence found in LATAM. 3 This situation occurs in several regions of the world and may be a factor in LATAM as well.
MS remains a complex disease that is likely caused by the interplay of still unknown genetic and environmental factors. Further efforts are required to determine the exact interplay between environmental factors, lifestyle modifications and genetic susceptibility. 39
In summary, this study provides updated information on epidemiological features of MS in the region, including incidence and prevalence. An increase in frequency should appear in the region, as shown by recent research; however, future studies including follow-up assessment of prevalence and incidence should be conducted in the region.
Footnotes
Conflicts of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.