
Abstract
Purpose
This study aimed to evaluate the quality of dry eye disease (DED) treatment–related short videos on popular Chinese platforms.
Methods
To better evaluate the quality of short videos related to DED treatment, the Dry-eye-related Short Videos Standardization Score (DSVSS), a preliminary disease-specific checklist, was developed tailored to DED clinical guidelines. On May 17, 2025, 305 videos (150 from Douyin, 155 from Bilibili) were retrieved using the keyword “dry eye treatment”, and their quality and guideline consistency were evaluated with the Global Quality Score (GQS) and the DSVSS checklist. Basic data, including duration, likes, comments, collections, and shares were recorded. Statistical analysis was performed using the Mann–Whitney U test, Kruskal–Wallis H test, and Spearman’s rank correlation to assess group differences and correlations.
Results
Videos from Douyin were generally shorter but achieved higher user engagement, while videos from Bilibili were longer with lower interaction (both P<0.001). Median GQS was 3 for Douyin and 2 for Bilibili (P=0.041), and median DSVSS was 3 for both (P=0.116). Videos performed poorly in DSVSS checklist in definition and classification [0.05 (IQR 0.03–0.07)], emphasizing chronicity [0.07 (0.05–0.10)], and individualized treatment [0.08 (0.03–0.10)], but performed well in avoiding exaggeration [0.84 (0.63–0.91)], absence of advertising [0.78 (0.66–0.88)], and in providing warnings for special populations [0.91 (0.87–0.96)] (P<0.001).
Conclusions
This study effectively identified critical deficiencies of current short-videos on DED treatment, underscoring the necessity for more professional, guideline-based content and stricter platform supervision to improve the quality of online health information.
Introduction
With the development of social media and mobile internet, video platforms such as TikTok, Instagram, YouTube, Douyin (TikTok in China), and Bilibili have exerted substantial influence on the presentation and dissemination of health-related information because of their concise format, intuitive delivery, and strong visual appeal.1–3 Compared with traditional print media, online health information is more accessible and can be disseminated more efficiently. However, the relatively low barriers to content production, together with heterogeneity in information sources and uploader backgrounds, may result in substantial variation in the accuracy and completeness of such content. 4 In the absence of authoritative sources or professional review, some videos may convey misleading messages, thereby affecting patients’ understanding of disease, which could interfere with treatment process, and potentially delay appropriate care.
Dry eye disease (DED) is a multifactorial ocular surface disorder characterized by disturbance of tear film homeostasis and ocular discomfort symptoms.5–7 Previous studies have shown that the overall prevalence of DED in China is 17.0%, with women, the elder, and residents of northern and western China representing higher-risk groups.5,8–15 Clinically, patients with DED commonly present with foreign body sensation, irritation, fluctuating vision, while tearing and photophobia are also frequently reported.16–18 In addition, prior studies have reported that Asians tend to exhibit more severe dry eye signs and symptoms related to eyelid structure.19–21 Severe DED shares similar clinical symptoms with several other ocular diseases, including allergic conjunctivitis, blepharitis, conjunctivochalasis, and certain forms of neuropathic ocular pain, which may lead to misdiagnosis and inadequate treatment.5,22 Without timely and standardized intervention, patients may experience persistent ocular discomfort and reduced visual quality.23,24 These findings underscore the importance of emphasizing standardized diagnosis, evidence-based management, and individualized care toward Chinese and other Asian patients.
DED is generally classified as aqueous-deficient, evaporative, or mixed.25,26 Management should be stratified and individualized according to disease subtype, severity of inflammation, and patient-specific risk factors. Current guidelines recommend a stepwise treatment strategy, beginning with patient education, environmental and behavioral modification, warm compresses, and artificial tears, then escalating to anti-inflammatory therapy, autologous serum, or scleral lenses when necessary.26,27 Notably, in the real-world context of health information access in China, traditional Chinese medicine (TCM) is also commonly encountered, with relevant interventions including acupuncture and herbal medicine.28–30 Experimental evidence suggests that acupuncture therapies, including manual acupuncture and electro-acupuncture, may offer unique neuromodulatory advantages. These interventions have been reported to modulate the neuro-immune-endocrine network, potentially activating the VIP/cAMP/PKA signaling pathway and upregulating aquaporin 5 (AQP5) expression, which may in turn enhance lacrimal gland secretory function and alleviate ocular pain. Concurrently, preclinical studies indicate that Chinese medicine monomers, such as polydatin, astaxanthin, and paeoniflorin, show potential in attenuating the vicious cycle of inflammation in DED by mitigating oxidative stress, cell apoptosis, and key inflammatory pathways such as NF-κB and MAPK.31–33
Recent studies have used DISCERN 34 and the Patient Education Materials Assessment Tool for Audiovisual Materials (PEMAT-A/V) to evaluate ophthalmic health information on short-video platforms. 35 However, these instruments were developed primarily for general health communication materials, and their emphasis is placed more on overall quality than on disease-specific content. 36 To address this gap, we developed a novel, disease-specific checklist — the Dry-eye-related Short Videos Standardization Score (DSVSS) — to specifically focus on dry eye disease–related content. Later we utilized the Global Quality Score (GQS),36–39 which has been used in prior ophthalmology video studies as a concise tool for evaluating overall video quality. In this research, we used DSVSS in combination with GQS to systematically evaluate DED treatment-related videos on Douyin and Bilibili. By comparing differences in overall quality and guideline consistency across platforms, content classifications, and uploader types, this study aimed to characterize the current landscape of DED treatment-related videos on major Chinese short-video platforms and explore their potential value and limitations in patient education.
Methods
Search strategy and data collection
On May 17, 2025, the term “dry eye treatment” was searched on Douyin and Bilibili. All retrieved videos were included in the study, comprising 200 videos from Douyin and 192 videos from Bilibili. After exclusion, 150 videos from Douyin and 155 videos from Bilibili were included in the final analysis (Figure 1). For each video, duration, upload date, likes, comments, collections, and shares were extracted. To minimize algorithmic bias introduced by personalized recommendations, all queries were performed in logged-out mode with cleared browser caches. Previous analyses have shown top 100 videos have a stable effect, that the sample of 150 was in align to provide adequate power.13,36–40 Search strategy for short videos on DED treatment.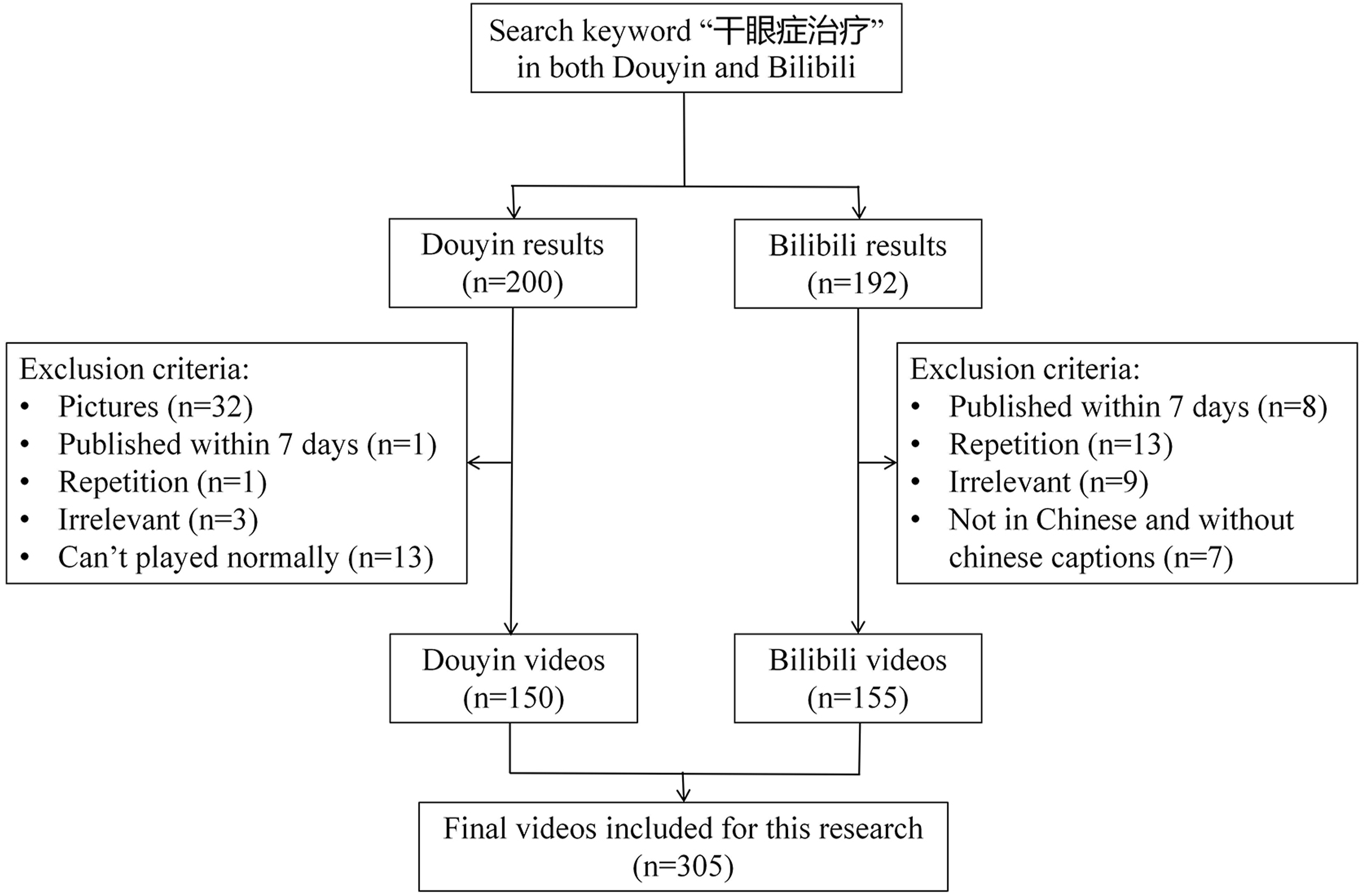
To ensure data validity, platform-specific exclusion criteria were applied. Douyin: (1) image-based works; (2) uploads within 7 days; (3) repetitions; (4) irrelevant content, and (5) unplayable files. Bilibili: (1) uploads within 7 days; (2) repetitions; (3) irrelevant content; and (4) non-Chinese videos without Chinese subtitles.
Video classification
Videos were classified based on their content and uploader identity.
Content classification: ①System of medicine: videos were labelled as either modern medicine (MM) or TCM. TCM is a holistic medical system based on syndrome differentiation and individualized treatment, emphasizing overall body regulation, which differs fundamentally from MM’s evidence-based and standardized diagnostic and therapeutic approaches.41–43 Videos citing TCM definitions, aetiology, or management of DED were assigned to the TCM category; all others were classified as MM. ②Primary focus: treatment, disease knowledge, dry-eye care, pathogenesis, or synthesis.
Uploader classification: ①Uploader: Uploaders were categorized into four categories: Professional individuals (PI), Non-professional individuals (NPI), Professional institutions (PIn), and Non-professional institutions (NPIn). ②Subtype of uploader: PI included ophthalmologists, physicians from other specialties, and other licensed healthcare professionals, whereas non-professional individuals included patients and lay users.
Content categories were determined by one reviewer after complete video review; uploader identities were extracted from platform verification badges. When verification was absent, identity was inferred from self-reported credentials within the video.
Assessments of video quality and guideline consistency
Three independent raters assessed all videos, including two ophthalmology postgraduates and one attending ophthalmologist. Consensus between the first two raters was adopted; disagreement triggered use of the third rater’s score. Inter-rater reliability was tested using intraclass correlation coefficient (ICC) based on a two-way random-effects model with absolute agreement for single measurements (ICC (2,1)), and Kendall’s coefficient of concordance (W), representing score agreement and rank agreement respectively. ICC(2,1) values > 0.40 were considered indicative of acceptable agreement,44,45 and W scores range between 0 and 1, where 0 signifies no agreement and 1 signifies complete agreement. 46
Dye-eye-related Short Videos Standardization Score (DSVSS).
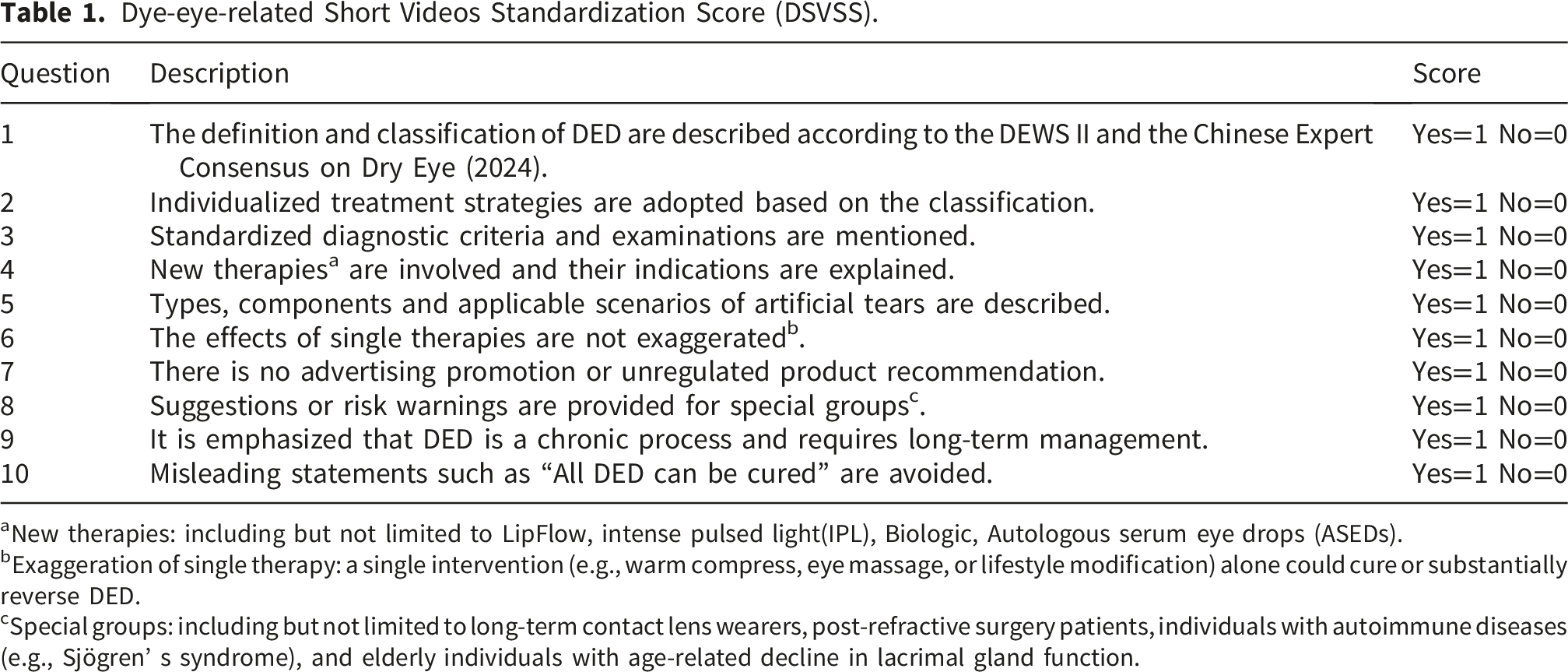
aNew therapies: including but not limited to LipFlow, intense pulsed light(IPL), Biologic, Autologous serum eye drops (ASEDs).
bExaggeration of single therapy: a single intervention (e.g., warm compress, eye massage, or lifestyle modification) alone could cure or substantially reverse DED.
cSpecial groups: including but not limited to long-term contact lens wearers, post-refractive surgery patients, individuals with autoimmune diseases (e.g., Sjögren’ s syndrome), and elderly individuals with age-related decline in lacrimal gland function.
Statistical analyses
All data were tested for normality and found to be non-normally distributed. Therefore, results were expressed as medians with interquartile ranges. The Mann–Whitney U test was used for two-group comparisons, while the Kruskal–Wallis H test was applied for multi-group comparisons. Spearman’s rank correlation was used to analyze the relationships between video basic data and evaluation scores separately for the two platforms. Specifically, the Benjamini–Hochberg (BH) p-value adjustment was applied to all pairwise correlations within the matrix containing video metadata (Duration, Like, Comment, Collection, Share) and evaluation scores (GQS, DSVSS). Correlation strength was interpreted as very weak (0.00–0.19), weak (0.20–0.39), moderate (0.40–0.59), strong (0.60–0.79), and very strong (0.80–1.00).47,48 Statistical analyses were performed using R, and data visualizations were created with GraphPad Prism and R. A P<0.05 was considered statistically significant.
Result
Inter-rater reliability
For videos from Douyin, the intraclass correlation coefficient
Basic information characteristics
Basic information on characteristics.

Z: Mann-Whitney test, M: Median, Q₁: 1st Quartile, Q₃: 3st Quartile, DSVSS: Dye-eye-related Short Videos Standardization Score, GQS: Global Quality Score.
In terms of quality, median GQS was higher for Douyin [3 (IQR 2–3)] than for Bilibili [2 (IQR 2–3)] (P=0.041). Median DSVSS was 3 on both platforms, with no statistically significant difference between them (P=0.116).
Content and uploader distributions
Figure 2 illustrates the distribution of content domains and uploader identities. On Douyin, 74% (n=111) of videos were categorized as MM and 26% (n=39) as TCM, the corresponding proportions on Bilibili were 77% (n =120) and 23% (n=35). Regarding primary focus, Douyin predominantly featured treatment-focused videos (80%, n=120), followed by disease knowledge (12.7%, n = 19), pathogenesis (3.3%, n = 5), dry eye care (2.0%, n = 3), and synthesis (2.0%, n = 3). Whereas Bilibili demonstrated more diversity, including treatment (73%, n=113), disease knowledge (10%, n=15), dry eye care (9%, n=14), and synthesis (6%, n=9). The distribution of primary focus categories differed significantly between Douyin and Bilibili videos (Fisher–Freeman–Halton exact test, P = 0.025). Proportion of videos focusing on traditional Chinese medicine and modern medicine on douyin (a) proportion of videos focusing on traditional Chinese medicine and modern medicine on Bilibili (b) distribution of uploader identity on Douyin (c) distribution of uploader identity on Bilibili (d).
Uploader identity also differed across platforms. On Douyin, 80% (n=120) of videos were produced by medical professionals, of whom 74% (n=111) were ophthalmologists; only 11% (n=17) originated from non-professionals. In contrast, Bilibili had a higher proportion of non-professional uploaders (44%, n=68), including patients (26%, n=40).
Supplementary Table 1 summarizes the basic data of videos from Douyin, categorized by content domain and uploader identity. In terms of medical system, no statistically significant differences were found between MM and TCM videos in duration, likes, comments, collections, or shares (P=0.441, P=0.512, P=0.271, P=0.113, and P=0.665, respectively). Likewise, Videos’ primary focus showed no significant variation in any metrics (P=0.087, P=0.578, P=0.657, P=0.384, P=0.058, respectively).
In contrast, stratification by uploader revealed marked differences across NPI, NPIn, PI, and PIn for all five aspects (respectively P<0.001, P=0.007, P=0.006, P=0.018, and P=0.018). Further analysis of the subtype of uploader also revealed significant differences across duration, likes, comments, collections, and shares (respectively P<0.001, P=0.002, P=0.016, P<0.001, P=0.001).
Supplementary Table 2 presents the corresponding analyses for Bilibili. In terms of medical system, MM and TCM videos differed only in the number of comments (P=0.050), while no significant differences were observed for duration, likes, collections, or shares (P=0.480, P=0.066, P=0.234, and P=0.301). Videos’ primary focus differed in duration (P=0.007) but not in the remaining aspects (P=0.123, P=0.149, P=0.118, and P=0.203).
When assessed by uploader, videos from Bilibili differed significantly in duration, likes, comments, and collections (P=0.001, P<0.001, P<0.001, and P=0.002), but not in shares (P=0.085). Further analysis under uploaders’ subtypes confirmed significant differences across all five dimensions (P=0.001, P<0.001, P<0.001, P<0.001, and P<0.001).
Video quality and guideline consistency scores
MM videos scored significantly higher than TCM videos in both GQS and DSVSS (P<0.0001). Synthesis videos achieved the highest GQS and DSVSS among all content types (both P<0.001). Treatment videos exceeded disease knowledge or pathogenesis videos in DSVSS (P<0.05).
Videos from PI and PIn scored higher than those from NPI and NPIn (P<0.05). No difference was detected between PI and PIn. Further subgroup analysis revealed that, among PI, physicians from other specialties scored lower than ophthalmologists and other PI. Among NPI, patient-uploaded videos showed higher DSVSS than those from other NPI (P<0.05) (Figure 3). Violin plots showing the comparison of GQS between modern medicine and traditional Chinese medicine (a) the comparison of DSVSS between modern medicine and traditional Chinese medicine (b) the comparison of GQS among uploader categories (c) the comparison of DSVSS among uploader categories (d) (*P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001).
Correlation analyses
On both Douyin (Figure 4) and Bilibili (Figure 5), a correlation heatmap demonstrated strong positive correlations among video popularity metrics (likes, comments, collections, and shares) (all r > 0.7, P<0.001). Correlation heatmap of relationships between duration, video popularity metrics (likes, comments, collections, and shares) and evaluation scores (GQS and DSVSS) on Douyin. The color gradient indicates the direction and strength of the Spearman’s rank correlation, ranging from 1.0 (strong positive correlation) to -1.0 (strong negative correlation). Each cell displays the exact Spearman’s correlation coefficient (r) and its corresponding adjusted p-value (p_adj). Correlation heatmap of relationships between duration, video popularity metrics (likes, comments, collections, and shares) and evaluation scores (GQS and DSVSS) on Bilibili. The color gradient indicates the direction and strength of the Spearman’s rank correlation, ranging from 1.0 (strong positive correlation) to -1.0 (strong negative correlation). Each cell displays the exact Spearman’s correlation coefficient (r) and its corresponding adjusted p-value (p_adj).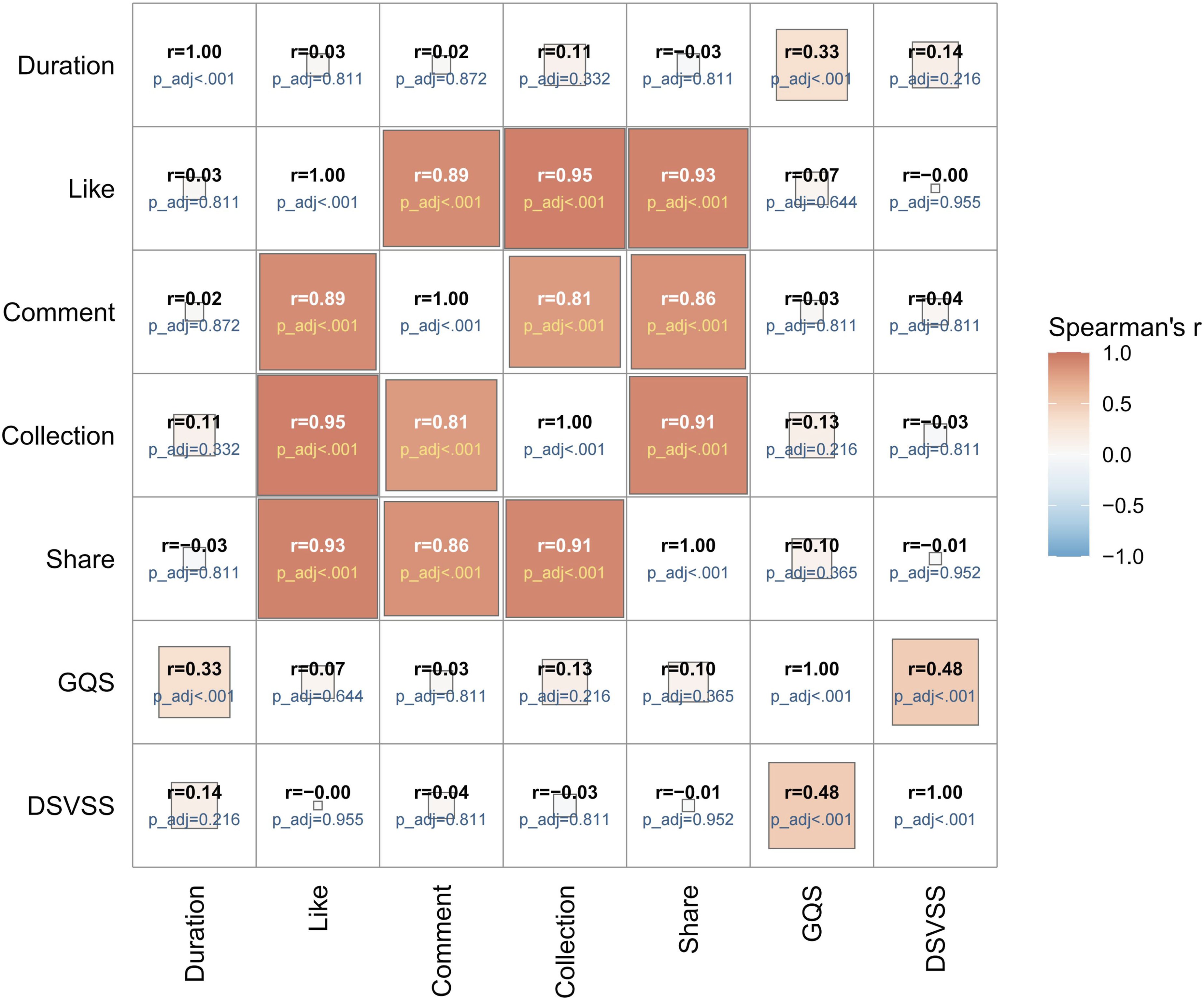

For Douyin, video duration was weakly positively correlated with GQS (r = 0.33, P < 0.001), whereas GQS showed a moderate correlation with DSVSS (r = 0.48, P < 0.001).
For Bilibili, video duration showed weak positive correlations with all video popularity metrics, including likes, comments, collections, and shares (r = 0.26, 0.35, 0.32, and 0.22, respectively; P < 0.001). Duration was also weakly positively correlated with GQS (r = 0.26, P < 0.001), while GQS demonstrated a strong positive correlation with DSVSS (r = 0.71, P < 0.001).
Analysis of DSVSS sub-items
When examining the individual components of the DSVSS, videos showed lower score for items related to definition and classification [0.05 (IQR 0.03–0.07), DSVSS-1], individualized treatment strategies [0.08 (0.03, 0.10), DSVSS-2], diagnostic criteria [0.08 (0.05, 0.15), DSVSS-3], artificial tear specifications [0.08 (0.07, 0.09), DSVSS-5], and emphasis the chronic nature of DED [0.07 (0.05, 0.10), DSVSS-9]. In contrast, videos performed relatively well in avoiding exaggerated efficacy claims [0.84 (0.63, 0.91), DSVSS-6], minimizing advertising [0.78 (0.66, 0.88), DSVSS-7], and providing warnings for special populations [0.91 (0.87, 0.96), DSVSS-8] (all P<0.001). (Supplementary table 3).
Platforms (Figure 6), content categories (Supplementary table 4), and uploader types (Supplementary table 5) revealed no significant differences in any single DSVSS dimensions (all P>0.05). Comparison of the ten sub-items of DSVSS between Douyin and Bilibili. Data are presented as the median of the mean scores from three independent raters, and error bars represent the interquartile range (IQR).
Discussion
This study systematically evaluated DED-treatment short videos on Douyin and Bilibili using the generic GQS and the newly developed, disease-specific checklist DSVSS. By combining a generic and a targeted approach, our findings may help evaluate the quality of short videos on DED treatment, inform future content regulation and improvement, and promote public access to reliable medical information. Nevertheless, as DSVSS is a newly developed exploratory checklist, these findings should be interpreted cautiously until further validation studies are conducted.
Comparison between platforms
Our findings showed clear differences between the two platforms. Videos from Bilibili were significantly longer, whereas videos from Douyin were shorter but achieved much higher levels of audience engagement (likes, comments, collections, and shares). This discrepancy likely reflects differences in platform positioning: Douyin prioritises rapid, entertainment-driven consumption, whereas Bilibili accommodates longer, more diverse content. 49 This may also be explained by the substantially larger user base of Douyin compared with Bilibili. As reflected by GQS, the quality of short videos related to treatment on Douyin is slightly higher, which might also be due to this difference. Moreover, the higher GQS scores observed on Douyin may be partly attributed to the greater proportion of professional uploaders on this platform. In contrast, uploader identities on Bilibili were more heterogeneous, with a considerable proportion of videos contributed by patients. This inclusivity fosters diverse voices but may compromise content accuracy and control.
Differences across content and uploaders
By content type, MM videos achieved higher GQS and DSVSS scores than TCM videos. However, this finding should be interpreted cautiously, as the DSVSS was primarily developed based on evidence-based modern medicine guidelines for dry eye disease. Therefore, higher scores may reflect closer alignment with guideline-based MM recommendations rather than an overall superiority in content quality. Comprehensive videos covering multiple aspects of DED achieved the highest scores on both evaluation metrics, suggesting that broader, multi-dimensional content is more likely to align with quality and guideline standards.
Uploader identity significantly influenced video metrics. Videos created by professionals and institutions were generally of higher quality and showed better guideline consistency than those made by non-professionals. Nevertheless, these professional videos did not always gain more attention, revealing a gap between audience preferences and scientifically reliable content. Subgroup analyses showed patient-uploaded videos achieved marginally higher scores than other lay content, likely reflecting their focus on practical experience.
Further analysis revealed that the proportion of professional uploaders was higher for TCM than for MM on both platforms (Supplementary Table 6), however, TCM videos received lower scores. This discrepancy may be explained by the fact that the DSVSS was developed based on MM expert consensus, whereas the definitions and therapy to DED differ between TCM and MM. Consequently, the checklist may not be directly applicable to TCM content. Future studies may consider developing a dedicated checklist based on existing TCM expert consensuses for a more appropriate evaluation. Recent studies have begun to explore the correlation between TCM syndromes and the MM classification of DED.50,51 These studies may contribute to the development of more standardized and evidence-based approaches to the treatment of DED within the framework of TCM in the future.
Correlation analysis
Popularity metrics were strongly interrelated. Importantly, GQS and DSVSS were moderately correlated, suggesting that higher-quality videos align with guideline-based standards. However, the absence of strong correlations between popularity and evaluation scores underscores that popularity is not a proxy for quality or guideline consistency; relying on engagement alone may mislead viewers.
The significant correlation between duration and evaluation scores on both platforms indicates that longer videos are more likely to contain comprehensive information and achieve higher quality ratings. On Bilibili, video duration showed weak positive correlations with popularity metrics (r > 0.2, P < 0.001). Although these correlations were statistically significant, their modest strength suggests only limited associations between video length and audience engagement, which may partially reflect the platform’s long-form content characteristics.
DSVSS sub-item analysis
Examination of individual DSVSS items revealed widespread omission of guideline-based management elements. Specifically, definition/classification (DSVSS-1), individualized therapy (DSVSS-2), diagnostic criteria (DSVSS-3), artificial-tear specifications (DSVSS-5), and emphasis on chronic disease management (DSVSS-9) were poorly covered.
Most videos offered only a brief overview, omitting physiological or etiological perspective (DSVSS-1). Many videos only mention the use of artificial tears to relieve symptoms, however, DED subtypes demand tailored therapies (DSVSS-2), such as selecting specific types of artificial tears (DSVSS-5).52,53 For example, aqueous-deficient dry eye is typically managed with artificial tears, secretagogues, or autologous serum eye drops, whereas evaporative dry eye caused by meibomian gland dysfunction may benefit from lipid-based artificial tears and adjunctive therapies targeting the lipid layer.6,54 Some uploaders make self-diagnoses of DED based on isolated symptoms, such as occasional ocular dryness, without considering the objective examinations required by current diagnostic criteria (DSVSS-3).5,7,55 Furthermore, diagnosed DED is a chronic and recurrent disorder that requires continuous long-term management, 24 but very few videos explicitly referred to this aspect (DSVSS-9), ultimately reducing therapeutic effectiveness and increasing the risk of secondary ocular complications.
In contrast, videos performed relatively well in avoiding exaggerated single therapeutic claims (DSVSS-6), limiting advertising (DSVSS-7), and providing warnings for special populations (DSVSS-8). Recognizing risk factors and warning susceptible populations are integral to DED prevention and management. Comprehensive knowledge of DED epidemiology and modifiable and non-modifiable risk factors enhances practitioner assessment and management. 56 These findings highlight the strengths and weaknesses of current video content: ethical and cautionary standards are generally respected, yet systematic and standardized clinical information is often neglected.
Implications and future directions
This study emphasizes the importance of developing disease-specific assessment metrics for online health information. The DSVSS, a guideline-based checklist, offers a focused framework for evaluating DED-related videos, ensuring consistency with both international and national guidelines. The adoption of similar disease-specific metrics could elevate health information standards across short-video platforms. Although DSVSS provides a structured framework for assessing DED-related videos, it remains an exploratory checklist and should not yet be regarded as a fully validated assessment tool. Future studies should further confirm the effectiveness of the checklist by assessing its inter-rater reliability, reproducibility, construct validity. External validation across different diseases, languages, cultural settings, and social media platforms is also needed to determine its generalizability and clinical applicability. In addition, prospective studies evaluating whether higher DSVSS scores are associated with improved viewer understanding or health decision-making would further support its practical value.
Likes and shares do not reflect content quality, therefore patients should turn to information from verified professionals and seek medical advice if symptoms persist. Professionals are encouraged to create videos that follow clinical guidelines, emphasize accurate diagnosis, individual-based treatment, and the chronic nature of DED. Video platforms should strengthen recommendation systems and improve content governance strategies. Platforms may consider verifying health content creators based on relevant medical accreditation or professional background and applying content labeling systems to help viewers better assess the reliability of videos.
Limitations
This study has several limitations. First, as a cross-sectional study, causal inferences cannot be drawn, and results may be influenced by temporal or platform-specific factors. Second, we have reviewed all the retrieved videos, while platform algorithms for video ranking and recommendation remain non-explicit, and their potential impact on our findings cannot be ruled out. Third, although DSVSS, a novel but exploratory disease-specific checklist, provides a structured framework for evaluation, it may not fully capture the scientific accuracy or clinical reliability, and has not yet undergone comprehensive psychometric validation. Therefore, its applicability and interpretability should be considered preliminary. In addition, expert consensuses and clinical practice guidelines for TCM management of dry eye disease have also been published in China, but their evaluation domains may not be fully captured by the current DSVSS framework. Future studies may consider incorporating TCM-specific consensus recommendations into complementary assessment tools for a more balanced evaluation of health information quality. Moreover, DSVSS was developed based on Chinese modern medical guidelines and specifically for Chinese short-video platforms, which may limit its generalizability to global populations or media. Finally, evaluations were conducted by three independent reviewers and two types of inter-rater reliability analyses were performed, however, GQS and DSVSS scores may still be influenced by subjective judgment.
Conclusion
Overall, the GQS and DSVSS of DED-related short videos on Douyin and Bilibili were generally unsatisfactory, suggesting that the quality and guideline compliance of these videos require further improvement. While videos generally avoided exaggerated claims and advertising, they failed to adequately emphasize individualized, guideline-based treatment and the chronic nature of DED. The deficiencies identified in our study may suggest potential directions for enhancing the accuracy and educational value of future DED-related treatment videos. Strengthening platform supervision and encouraging professional involvement are essential to improve the quality of health information on short-video platforms.
Supplemental material
Supplemental material - Insights into the quality and guideline consistency of dry eye disease treatment videos on Chinese short-video platforms
Supplemental material for Insights into the quality and guideline consistency of dry eye disease treatment videos on Chinese short-video platforms by Ruoyi Yao, Jiahao Ye, Zhounan Zhu and Chen Li in DIGITAL HEALTH.
Footnotes
Ethical considerations
This study was granted exemption by Medical Ethics Committee of The First Affiliated Hospital of Soochow University (Date of Exemption: February 27, 2026). Because the research exclusively utilized publicly available data, no specific exemption waiver number was issued by the committee for this policy-based waiver. The formal “Explanation on Exemption from Ethical Review” document issued by the committee has been provided as a supplementary file. We certify that the study was performed in accordance with the 1964 declaration of HELSINKI and later amendments.
Author contributions
All authors contributed to the study design. C. Li provided ophthalmological expertise. Z.N. Zhu offered methodological guidance. R.Y. Yao collected the data. R.Y. Yao, J.H. Ye, and C. Li performed the video assessments. R.Y. Yao and J.H. Ye drafted the manuscript. C. Li and Z.N. Zhu revised the manuscript. All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the National Natural Science Foundation of China (No. 82501261) and Medical Research Projects of the Jiangsu Provincial Health Commission (No. M2024041).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Chen Li is the guarantor of this work and accepts full responsibility for the integrity of the data, the accuracy of the analysis, and the conduct of the research. Chen Li had full access to all study data and made the final decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
Appendix
Global quality score (GQS).
37
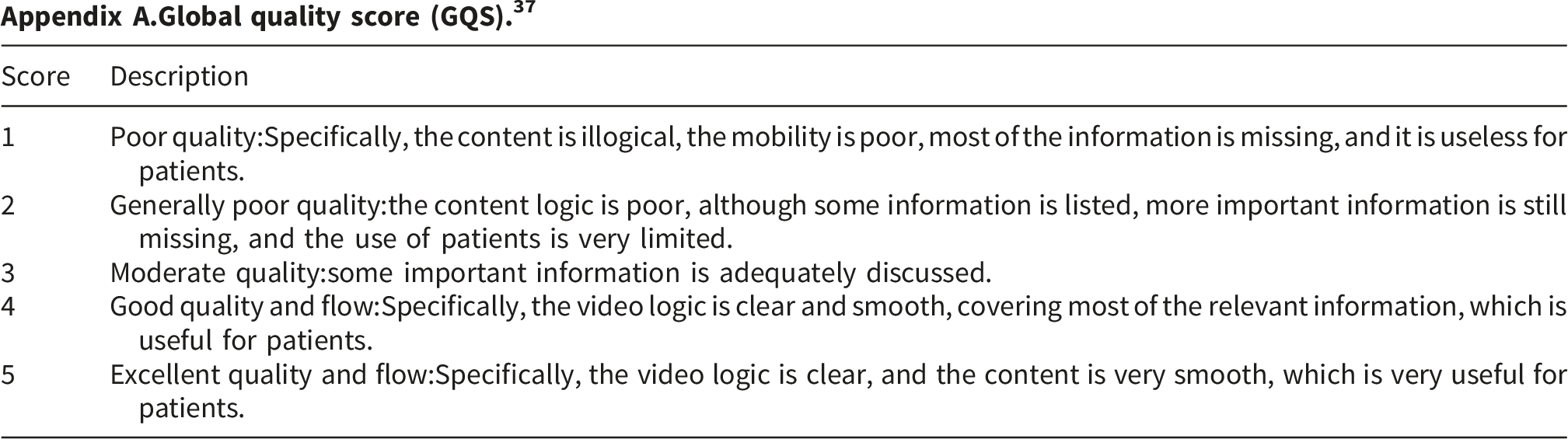
Score
Description
1
Poor quality:Specifically, the content is illogical, the mobility is poor, most of the information is missing, and it is useless for patients.
2
Generally poor quality:the content logic is poor, although some information is listed, more important information is still missing, and the use of patients is very limited.
3
Moderate quality:some important information is adequately discussed.
4
Good quality and flow:Specifically, the video logic is clear and smooth, covering most of the relevant information, which is useful for patients.
5
Excellent quality and flow:Specifically, the video logic is clear, and the content is very smooth, which is very useful for patients.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.