
Abstract
Objective
Depression is a prevalent mental disorder associated with substantial social and familial burdens, and exercise is increasingly recognized as a promising non-pharmacological intervention; however, research is hindered by heterogeneous approaches, safety concerns, and individual variability. A structured knowledge framework may support the development of more personalized exercise prescription. This study aimed to construct PEPRKD-Depression (Personalized Exercise Prescription Recommendation Knowledge Database for Depression), a structured knowledge database of exercise interventions for depression, to systematically integrate existing literature and provide a knowledge foundation for personalized exercise prescription.
Methods
Data were sourced from PubMed and included original studies on exercise interventions for depression published between 1960 and 2023. Relevant data including structured exercise programs, patient information, fitness and risk assessments, adverse events, and outcomes, were extracted, standardized, and organized. The knowledge database was developed with Vue3, hosted on Nginx, and uses MySQL for data storage.
Results
PEPRKD-Depression includes 567 studies with 769 exercise intervention protocols involving 100,794 subjects across 49 countries. It extracted 662 depression-related items (e.g., symptoms, disorders, perinatal and subthreshold depression). Exercise regimens followed the “FITT-VPP” principle: Frequency, Intensity, Time, Type, Volume, Progression, Periods of time. The knowledge database is publicly available at: https://dpa.bioinf.org.cn/.
Conclusion
PEPRKD-Depression is a comprehensive exercise therapy knowledge database for depression that provides a structured repository of exercise intervention information that may serve as a preliminary knowledge resource for future personalized exercise recommendation research and decision-support applications.

Keywords
1 Introduction
Depression is a common and serious mental disorder that poses significant threats to the physical and mental health of individuals while also having profound impacts on families, society, and economic development.1,2 According to estimates from the World Health Organization (WHO), depression has become one of the leading contributors to global disease burden and is closely associated with high suicide rates. However, current treatments for depression face several limitations, including long treatment duration, poor medication adherence, and low remission rates.3,4
The etiology of depression is complex and multifaceted, involving biological, psychological, and social factors. Current mainstream treatments include pharmacotherapy, psychotherapy, and non-pharmacological interventions. Among these, exercise intervention has gained widespread attention as a safe and effective non-pharmacological treatment with relatively few adverse effects.5–8 Numerous studies have demonstrated that appropriate exercise can improve emotional well-being, enhance cognitive function, and reduce depressive symptoms,9–12 and relevant guidelines also recommend exercise as an adjunct treatment for depression.13–15 Due to the heterogeneity of depression and the diverse needs of patients, the effectiveness of different exercise interventions varies significantly.16–20 For example, when developing personalized exercise prescriptions for individuals with depression who have comorbidities such as cancer, chronic renal failure, diabetes, or stroke, clinicians must comprehensively consider patients’ health status, exercise tolerance, and the risks and benefits of various exercises. In addition, patient preferences directly influence exercise adherence and outcomes. Thus, formulating appropriate exercise prescriptions for individuals with depression requires consideration of factors such as age, comorbidities, exercise risks, and preferences. However, a systematic and standardized framework for implementing exercise interventions in depression remains lacking.
The core of the precision medicine initiative is to deliver the right treatments to the right patients at the right time. 21 Personalized exercise prescription recommendations tailored to individual patients may become an important direction in depression management. As healthcare undergoes rapid digitalization, digital therapeutics have emerged as an important component of digital health technologies.22,23 The integration of a clinical decision support system (grounded in a knowledge database) with digital technologies (e.g., mobile health applications capable of collecting real-time user data from wearable devices and smartphones and providing algorithm-based feedback) 21 may facilitate the future development of personalized exercise recommendation systems.
In this context, developing a comprehensive knowledge database for exercise interventions in depression is of significant importance. To address this, we synthesized existing relevant research and, in light of the clinical characteristics of depression, compiled 769 research-derived exercise intervention protocols. From this, we constructed the Personalized Exercise Prescription Recommendation Knowledge Database for Depression (PEPRKD-Depression), designed to systematically organize heterogeneous exercise intervention protocols reported in the literature. Traditional exercise prescriptions adhere to the “FITT-VP” principle, encompassing Frequency, Intensity, Time, Type, Volume, and Progression. 13 Building on this framework and tailored to the specific demands of exercise therapy for depression, we propose an expanded “FITT-VPP” principle. The additional “P” denotes limited exercise periods, such as morning sessions,24,25 afternoon routines,26,27 exercise during dialysis, 28 or non-consecutive day regimens.29,30 This inclusion may support future individualized exercise intervention strategies. Furthermore, unlike prior databases, our knowledge repository places greater emphasis on the structured organization and practical characterization of exercise intervention protocols. Its primary objective is to support future research on personalized exercise therapy in depression.
2 Methods
2.1 Study design
This study is designed as a knowledge base construction study aiming to systematically compile exercise intervention protocols for depression. Key reporting elements were structured with reference to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Scoping Reviews) framework, including search strategy, eligibility criteria, study selection, and data extraction. The study selection process is illustrated in Figure 1. The corresponding PRISMA-ScR checklist is provided in Supplemental Material S1. The flowchart for the collection of exercise intervention protocols for depression.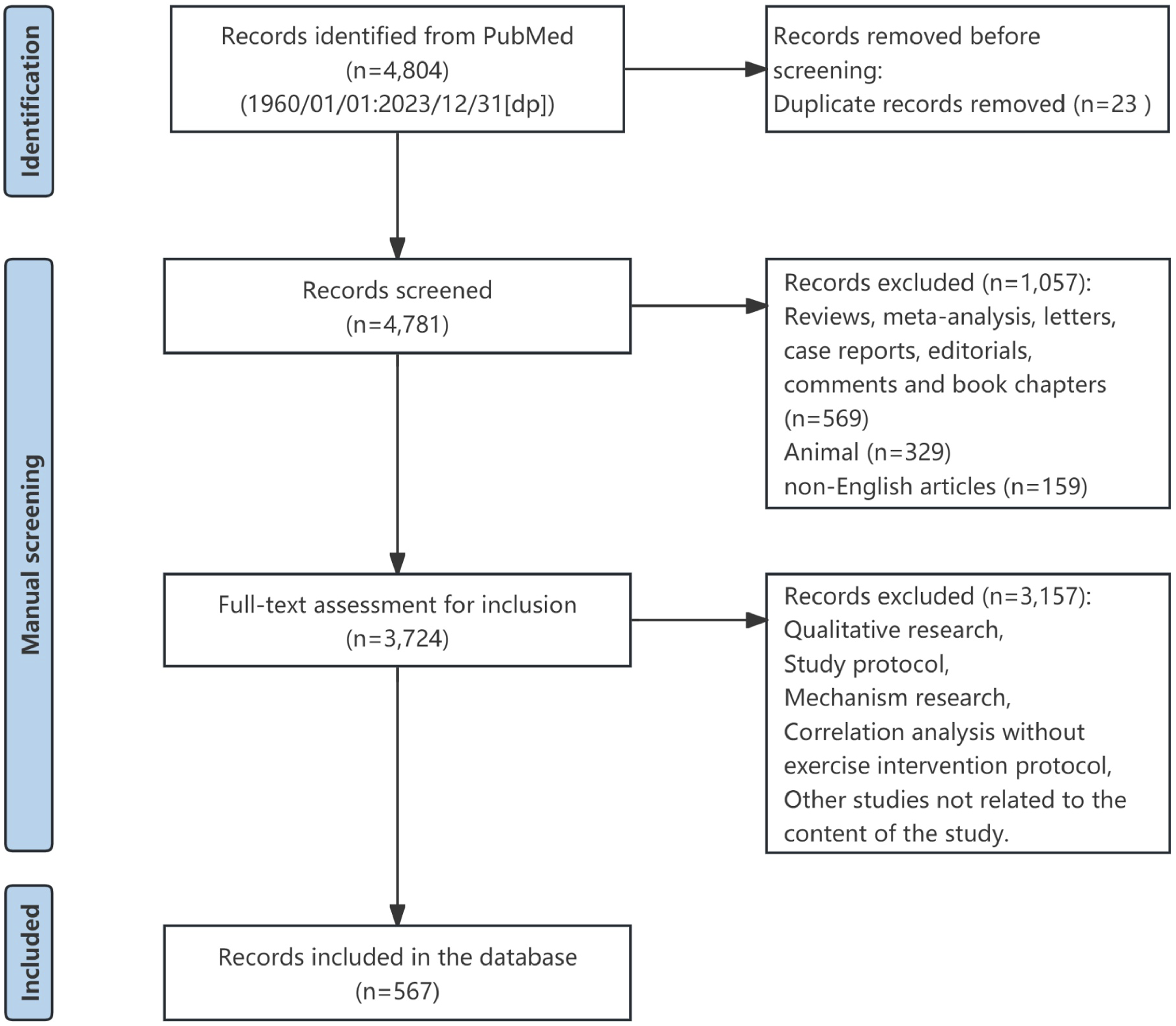
2.2 Data source
Original research articles published between 1960 and 2023 were primarily retrieved from PubMed. PubMed, a literature abstract and citation database managed by the National Institutes of Health (NIH), is one of the world’s largest and most authoritative biomedical literature databases. All articles indexed in PubMed undergo rigorous peer review, earning it widespread recognition in the field. To systematically retrieve literature on exercise interventions for depression, we used “depress*”, “exercise”, “physical”, and “training” as search keywords in PubMed, with filters applied to include only titles containing both “depress*” and exercise-related terms. Due to the concept-specific nature of the topic, the PubMed search was limited to title fields to enhance retrieval specificity. Preliminary searches showed that title-and-abstract searches substantially increased records with peripheral relevance without materially improving the identification of directly eligible studies. Given that standardized assessment scales for depression were first developed in the 1960s, we set the literature inclusion timeframe as January 1, 1960, to December 31, 2023. Specifically, the search strategy was formulated as “(depress*[ti]) AND (exercise[ti] OR physical[ti] OR training[ti] OR aerobic[ti] OR sport[ti] OR athletic*[ti] OR yoga[ti]) AND 1960/01/01:2023/12/31[dp]”.
2.3 Inclusion and exclusion criteria
The knowledge database mainly includes original intervention research, such as randomized controlled trials, quasi-experimental studies, and self-controlled pre-post cohort studies. The scope of depression-related conditions is broad, encompassing depressive disorder/depression, subthreshold depression, depressive symptoms, and perinatal depression. The database excludes reviews, meta-analyses, letters, case reports, editorials, comments, book chapters, animal studies, and non-English publications. Additionally, studies without specific exercise protocols, such as qualitative research, mechanistic studies, and correlation analyses, were excluded.
2.4 Data extraction
Study selection was performed independently by two reviewers to minimize bias. A standardized data extraction form with predefined extraction items was developed prior to formal data collection to ensure consistency across studies. Before data extraction, the reviewers discussed and unified the extraction criteria. Data extraction was conducted by one reviewer and independently verified by a second reviewer for accuracy and completeness. Any disagreements were resolved through discussion, and if consensus could not be reached, a third reviewer made the final decision. As illustrated in Figure 2, the entity relationships within PEPRKD-Depression were constructed in accordance with the American College of Sports Medicine’s (ACSM) guidelines
13
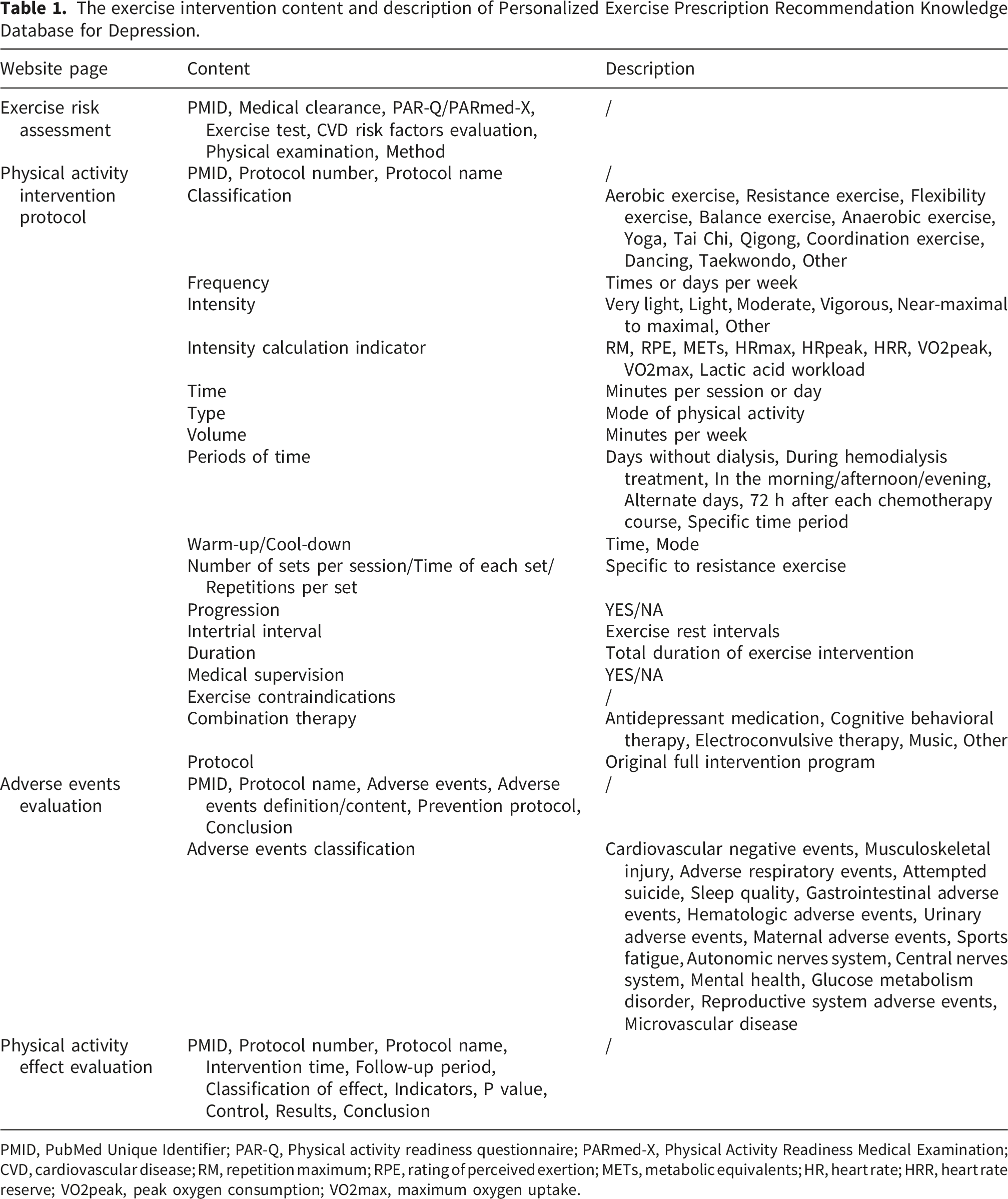
for exercise testing and prescription, as well as recommendations from psychiatrists. Detailed information on exercise interventions for depression was extracted based on the ACSM FITT-VP framework (Frequency, Intensity, Time, Type, Volume, Progression). By integrating data from the included literature, PEPRKD-Depression encompasses information on depression-related details, baseline characteristics, physical fitness assessments, exercise risk evaluations, exercise intervention protocols, adverse event monitoring and prevention, and exercise efficacy evaluations. The specific content of exercise interventions is presented in Table 1. Entity-relationship diagram of the Personalized Exercise Prescription Recommendation Knowledge Database for Depression (PEPRKD-Depression). The diagram illustrates the overall architecture of the knowledge base and how different components are logically connected. At the center is the core knowledge framework of PEPRKD-Depression, which integrates five functional modules. These modules collectively represent the key elements required to build a knowledge base for personalized exercise prescriptions for depression. Building outward from the center, the figure systematically presents the detailed contents of five modules. Among them, the exercise/physical activity module (shown on the left side of the figure) is further expanded into four sub-tables, which provide a comprehensive description of exercise protocol details, as well as exercise-related risk assessment, effect evaluation, and adverse events. Different colors are used to distinguish modules and substructures, helping to clarify the hierarchical organization and relationships within the knowledge base. The exercise intervention content and description of Personalized Exercise Prescription Recommendation Knowledge Database for Depression. PMID, PubMed Unique Identifier; PAR-Q, Physical activity readiness questionnaire; PARmed-X, Physical Activity Readiness Medical Examination; CVD, cardiovascular disease; RM, repetition maximum; RPE, rating of perceived exertion; METs, metabolic equivalents; HR, heart rate; HRR, heart rate reserve; VO2peak, peak oxygen consumption; VO2max, maximum oxygen uptake.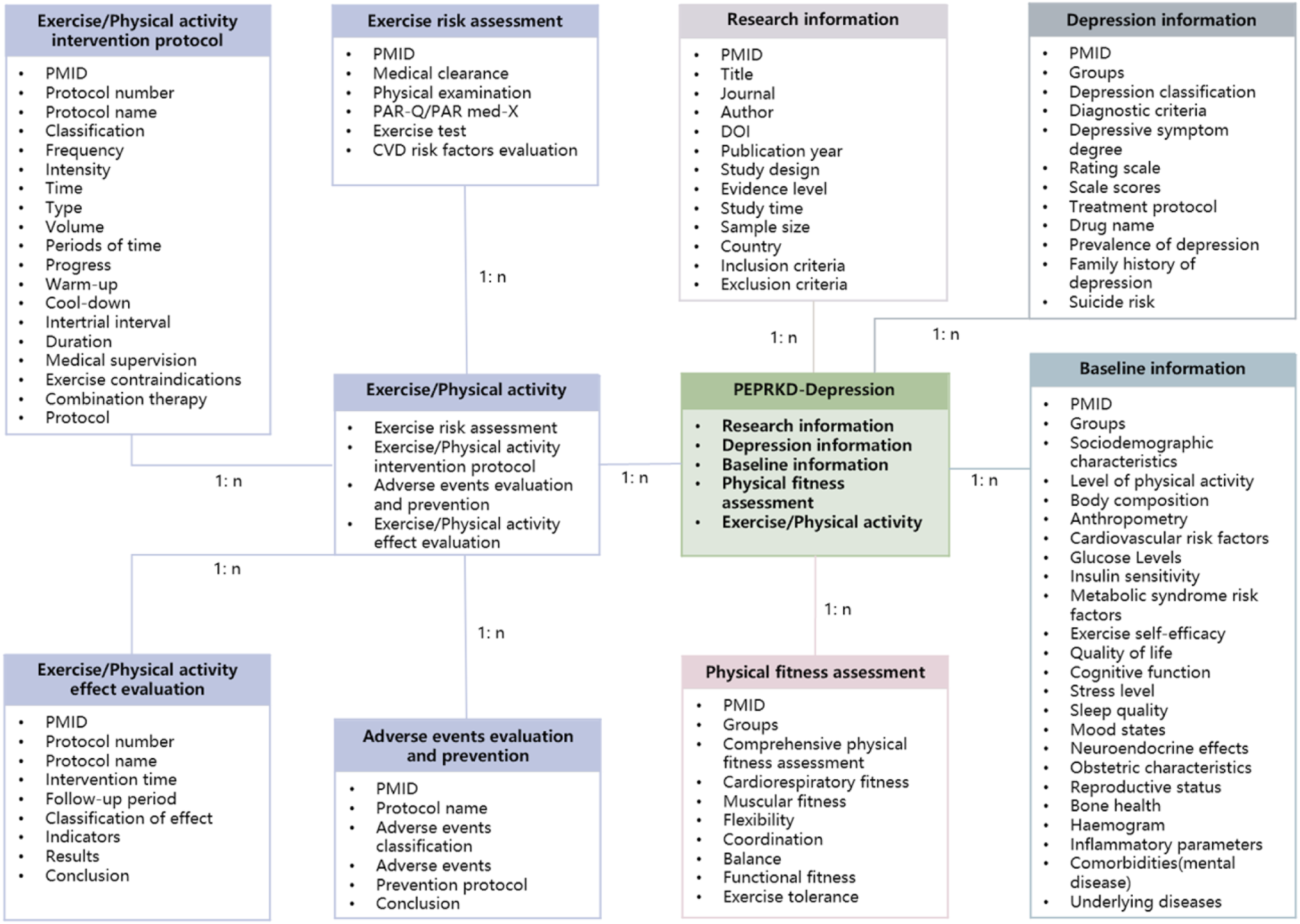
2.5 Evidence classification
Included studies were categorized according to the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (2009) 31 to provide a general indication of study design hierarchy. Because the primary aim of this study was to construct a structured knowledge database of exercise intervention protocols rather than to synthesize intervention effectiveness, a formal risk-of-bias assessment was not conducted. This classification did not influence study selection or the overall exercise recommendation, but was considered as one of several factors in protocol ranking rather than the sole determinant.
2.6 Knowledge database implementation
PEPRKD-Depression employs Vue3 (https://cn.vuejs.org/) as the web development framework and Nginx as the web server, with data stored in a MySQL database. Additionally, several JavaScript plugins—including ECharts.js (https://echarts.apache.org), Sigma.js (https://www.sigmajs.org/), and Gephi (https://gephi.org/)—were utilized to generate visual data charts.
3 Results
3.1 The landscape of PEPRKD-Depression
Characteristics of personalized exercise prescription recommendation knowledge database for depression.
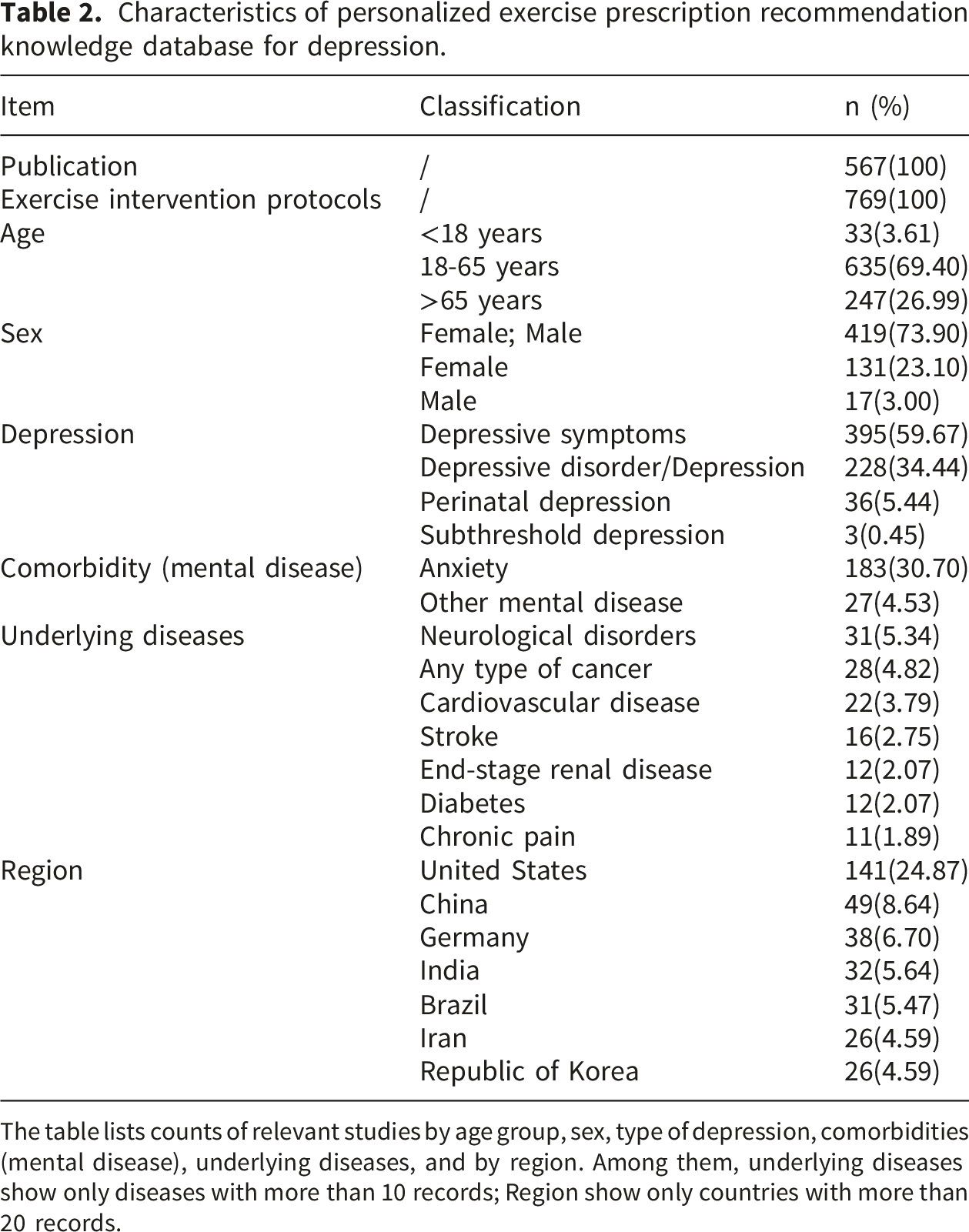
The table lists counts of relevant studies by age group, sex, type of depression, comorbidities (mental disease), underlying diseases, and by region. Among them, underlying diseases show only diseases with more than 10 records; Region show only countries with more than 20 records.
Furthermore, additional statistical information from the knowledge database is available on our website (https://dpa.bioinf.org.cn/), including regional distribution maps of all studies, statistics on comorbidities, and statistical charts illustrating improvements in efficacy evaluation indicators following exercise. The relationships between exercise effects and corresponding exercise types, frequencies, intensities, and volumes are visualized using Sankey diagrams. Trends in key exercise variables, data completeness, and annual publication distribution are presented in Supplementary Table S2.
3.2 Applications of PEPRKD-Depression
3.2.1 A preliminary decision-support tool for exercise recommendation
PEPRKD-Depression provides basic functions such as knowledge browsing, information retrieval, and original study information downloading. In addition, it serves as a preliminary decision-support tool for exercise recommendation. When users provide baseline characteristics, clinical information related to depression and comorbidities, suicide risk assessment results, responses to exercise preparticipation health screening questionnaires, and desired exercise goals, the tool applies the established matching logic to identify potentially relevant exercise protocols (Figure 3 and Supplemental Table S3). Users may review the recommended exercise protocols and select preferred options, while clinicians may refer to the information when considering exercise interventions for individual patients. Physical activity protocol recommendation tool of PEPRKD-Depression. The exercise program recommendation process consists of five steps: users provide baseline information and details on depression and comorbidities, complete a suicide risk assessment and a pre-exercise health screening questionnaire, and define exercise goals, after which the system generates personalized exercise plans for selection. For users at high suicide risk, the system terminates the recommendation process and advises seeking professional help. In Step 4, if any symptoms (e.g., chest discomfort with exertion) or medical conditions (e.g., heart attack) are reported, the system also discontinues recommendations for safety reasons and advises obtaining medical clearance before exercise. Users who already engage in regular physical activity and have medical conditions may continue light- to moderate-intensity exercise without clearance, but vigorous-intensity exercise requires prior approval from a healthcare professional.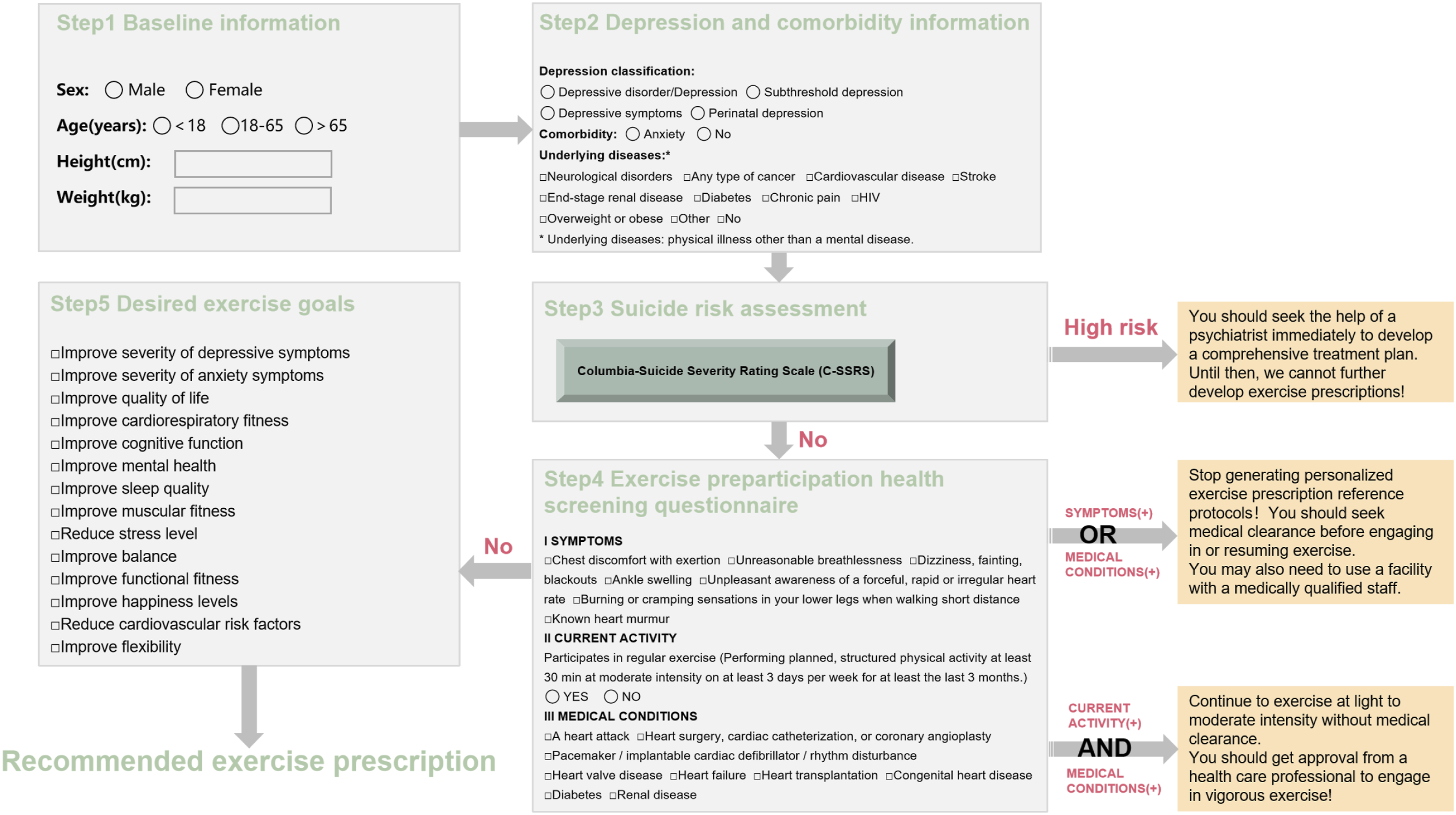
The exercise protocols displayed on the website are ranked based on the level of literature evidence, the completeness of the exercise intervention protocol, and whether an exercise risk assessment is included. In the scoring system, evidence level contributed 20% of the total score, whereas protocol completeness accounted for the largest proportion (70%), followed by risk assessment (10%). Detailed scoring criteria are provided in Supplemental Table S4. Greater weight was assigned to the completeness of the exercise protocol, as an effective exercise prescription requires clear and comprehensive reporting of its core elements. Therefore, protocols with lower levels of evidence could rank higher if they provided more detailed and implementable exercise information, while high-quality studies could rank lower if key elements were insufficiently reported.
3.2.2 Suicide risk assessment tool
Given that patients with depression may be at increased risk of suicide, screening for suicide risk prior to exercise is particularly important. PEPRKD-Depression incorporates the Columbia-Suicide Severity Rating Scale (C-SSRS) as a suicide risk assessment tool, as shown in Step 3 of Figure 3. The C-SSRS assesses suicide risk through a series of simple and plain-language questions to determine the severity and immediacy of suicide risk and evaluate the level of support required. It is widely recognized as a commonly used screening instrument for suicide risk assessment. 32 If a user is identified as being at high suicide risk, further exercise recommendations will not be provided, and consultation with a psychiatrist is recommended.
3.2.3 Exercise preparticipation health screening tool
Exercise preparticipation health screening is important for identifying individuals at increased risk of exercise-related adverse cardiovascular events and for guiding recommendations regarding exercise intensity. 13 In accordance with ACSM guidelines, PEPRKD-Depression incorporates an exercise preparticipation health screening questionnaire (Step 4 of Figure 3) as a screening tool. 13 This questionnaire consists of a simple three-step process that assists exercise professionals in determining whether medical clearance is required before initiating exercise for patients with depression. 33 If medical clearance is deemed necessary, further exercise recommendations will not be provided.
3.3 The extension of the FITT-VP principle
In line with ACSM guidelines, PEPRKD-Depression not only compiles exercise intervention protocols but also incorporates pre-exercise fitness and risk assessments, exercise-related adverse events, and evaluations of intervention efficacy. The intervention protocols are structured according to the “FITT-VP” principle, including exercise classification, weekly frequency, intensity, session duration, exercise modality, weekly volume, progression during the intervention (e.g., changes in intensity or duration), total intervention duration, availability of medical supervision, combination therapies, and detailed program descriptions.
Furthermore, we found that “Periods of time” (i.e., specific periods for exercise) are also critical in designing exercise programs. Currently, 15.61% of the exercise protocols in the database include descriptions of “Periods of time”. Consequently, we innovatively expanded the “FITT-VP” principle to “FITT-VPP” by incorporating this additional dimension of timing. Based on the data collected so far, we have made a preliminary definition and classification of “Periods of time”.
The specific time periods during which exercise is restricted, as opposed to exercise that can occur at any time or during any phase of a disease.
Classification: (a) By different stages of the disease: before dialysis, during dialysis, non-dialysis days, 72 hours after chemotherapy. (b) By interval between exercise sessions: alternate days, daily, non-consecutive days. (c) By specific time of day: morning, midday, afternoon, evening, or a specific point in time.
4 Discussion
In recent years, a growing body of research has focused on the effects of exercise interventions for depression. This study systematically synthesizes knowledge on exercise interventions for depression through the development of the first personalized exercise prescription recommendation knowledge database for depression (PEPRKD-Depression). As a knowledge-based resource designed to support preliminary exercise recommendation processes, PEPRKD-Depression provides users with exercise program options matched to individual characteristics. Unlike prior databases, it places greater emphasis on the structured organization and practical usability of exercise intervention information, and may serve as a reference resource for healthcare providers, patients, and researchers in addressing real-world clinical challenges.
4.1 Potential applications of PEPRKD-Depression
The comparison with current guidelines related to depression.
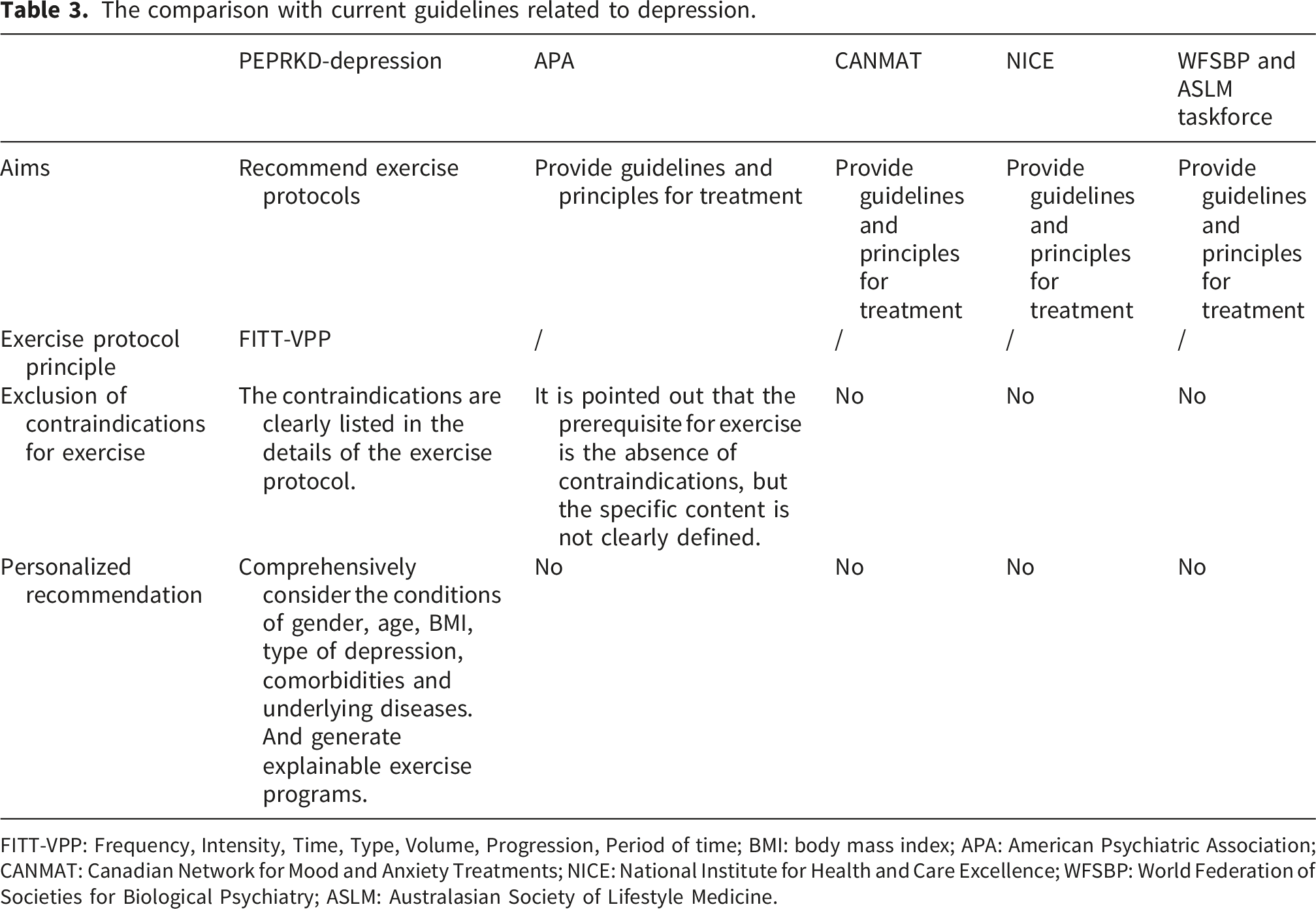
FITT-VPP: Frequency, Intensity, Time, Type, Volume, Progression, Period of time; BMI: body mass index; APA: American Psychiatric Association; CANMAT: Canadian Network for Mood and Anxiety Treatments; NICE: National Institute for Health and Care Excellence; WFSBP: World Federation of Societies for Biological Psychiatry; ASLM: Australasian Society of Lifestyle Medicine.
4.2 The importance of “periods of time”
Exercise prescriptions are typically developed following the “FITT-VP” principle,
13
and we have added “periods of time” as an additional dimension, expanding it to the “FITT-VPP” principle. The specific limitation of exercise time is directly related to the safety and effectiveness of exercise for patients. Next, we will discuss this in detail according to different classifications. (a) “Periods of time” restrictions at different stages of disease may involve exercise safety considerations. For example, for breast cancer patients with depressive symptoms, exercise is recommended to begin 72 hours after chemotherapy to ensure safety.
37
Chemotherapy can cause acute reactions such as fatigue, nausea, bone marrow suppression, and blood pressure fluctuations. Exercising too soon may increase the risk of infection or induce adverse events. For patients with chronic kidney failure who require long-term hemodialysis, exercise can be arranged during dialysis or on non-dialysis days.38–41 However, during dialysis, many types of exercise are difficult to perform due to limitations in position, vascular access, and potential hypotension, posing safety risks. In these cases, exercise is usually limited to lower limb resistance training or stationary bicycle. On non-dialysis days, patients are generally more stable and can engage in a wider variety of exercises. (b) Properly scheduling exercise intervals is crucial for both effectiveness and adherence. Exercising on alternate days or non-consecutive days42–44 allows sufficient recovery and may improve adherence. However, if exercise sessions are scheduled with excessively long intervals between them, the total exercise volume may be insufficient to achieve the desired training effects. Increasing the intensity of individual sessions to compensate for this may, in turn, raise the risk of injury. On the other hand, exercising too frequently, especially with high-intensity training every day, may lead to chronic injuries and fatigue, resulting in interruptions in training and reduced long-term adherence. (c) The “periods of time” for exercise during the day should be based on the patient’s symptoms, preferences, and other factors. For example, patients with depression often experience more severe symptoms in the morning and improved symptoms in the evening. Morning exercise45–47 may be more effective for improving mood, while high-intensity exercise in the evening could potentially affect sleep quality. Of course, further randomized controlled trials are needed to validate the clinical significance of these findings.
4.3 Ethical considerations
The use of automated suicide risk screening tools (C-SSRS) in digital environments raises important ethical considerations. Compared with clinician-administered assessments, automated systems lack contextual judgment and may increase the risk of misinterpretation. Accordingly, the present assessment is intended for preliminary screening rather than clinical diagnosis.
To address safety concerns, the platform incorporates safeguards for high-risk users. When high-risk responses are detected, the platform provides immediate access to crisis support resources (e.g., helplines recommended by the International Association for Suicide Prevention) and encourages users to seek professional help. However, effective referral and follow-up remain challenging in fully automated contexts.
Clinical oversight remains essential, as responsibility for diagnosis and treatment lies with licensed professionals. Institutions adopting the platform should ensure appropriate oversight and risk management. The platform is intended for both clinician-guided and patient self-directed use; however, self-use does not constitute a diagnosis or treatment.
4.4 Limitations
This study has several limitations. First, the literature search was limited to the PubMed database and English-language publications, which may have introduced selection bias and restricted the comprehensiveness of the evidence base. Additionally, the search strategy focused on title terms only, potentially missing relevant studies in which key concepts are described in the abstract but not in the titles. This approach may have also biased the results toward well-represented regions and populations, while neglecting studies from underrepresented regions or different demographic groups. Future studies may consider broader search strategies to minimize potential selection bias.
Second, the baseline characteristics used for matching in the database are limited to variables reported in existing studies. However, other patient characteristics, such as preferences, motivation, psychiatric family history, or biological factors like BDNF, 48 may be more predictive of treatment outcomes. To enhance precision, future recommendations for personalized exercise prescriptions should integrate additional personalized or mechanistic factors. Multicenter studies, alongside multidimensional data collection and mechanistic research, will help identify the specific impact of these factors. Additionally, this data-driven matching approach relies entirely on pre-existing study data and lacks adaptive learning capabilities. Future updates could incorporate real-world data and user feedback to refine the matching logic.
Third, although the included studies were categorized according to the OCEBM Levels of Evidence, a formal risk-of-bias assessment was not conducted because the primary aim of this study was to summarize and structure reported exercise intervention protocols rather than to perform comparative effectiveness synthesis. Nevertheless, the absence of standardized quality appraisal may limit interpretation of the relative methodological strength of the included evidence. Future studies may incorporate formal risk of bias tools to support more comprehensive evidence evaluation.
Fourth, this study lacks external validation and has not undergone a formal usability evaluation with clinicians to assess whether the system contains all the necessary information for exercise prescription in real-world clinical practice. Therefore, claims of generalizability and replicability should be considered preliminary until such validation is completed. Future research should incorporate both clinician-based usability testing 49 and external validation 50 to enhance the system’s clinical validity, usability, and generalizability. This should include clinician benchmarking to assess agreement with expert decision-making, user-centered testing to evaluate usability, and real-world implementation studies to assess its feasibility and clinical applicability.
Finally, the current version of the database primarily serves as a platform for summarizing data and offering exercise program recommendations that are tailored to patient characteristics. However, these recommendations should be considered supportive rather than fully personalized exercise prescriptions. Future iterations of the database will be continuously improved through external validation, algorithm optimization, and clinical testing, and may evolve into a more refined decision-support framework for personalized exercise recommendation. To improve the comprehensiveness and timeliness of the database, we plan to update it every two years using a combination of automated literature searches and manual curation from major databases (e.g., PubMed and Web of Science). This update process will be overseen by the corresponding author’s research team, with support from trained research assistants. In parallel, future implementation efforts may focus on clinician training, academic dissemination, Hospital Information System (HIS) integration, and multi-institutional collaboration.
5. Conclusion
PEPRKD-Depression provides a comprehensive and systematic synthesis of exercise therapies for depression, serving as a structured knowledge resource to support preliminary exercise recommendations and future research. By organizing and standardizing relevant evidence, it may facilitate more feasible and individualized exercise planning with potential benefits for safety and long-term adherence. Unlike the generalized guidance of traditional guidelines, PEPRKD-Depression incorporates diverse patient characteristics and complex comorbidities into the organization of exercise intervention information. In summary, PEPRKD-Depression represents an important step toward the development of personalized exercise recommendation systems for depression.
What was already known on this topic. ● Exercise is recognized as a promising non-pharmacological intervention for depression, a prevalent mental illness with significant social and familial burdens, though research in this area is constrained by diverse methodological approaches, safety concerns, and individual variability. ● Traditional exercise prescriptions adhere to the “FITT-VP” principle, encompassing Frequency, Intensity, Time, Type, Volume, and Progression. ● A robust knowledge framework is acknowledged as critical for developing scientific, personalized exercise prescriptions.
What this study added to our knowledge
● This study developed PEPRKD-Depression, the first comprehensive knowledge database of exercise therapies for depression, which includes 567 studies (1960–2023) with 769 exercise intervention protocols (involving 100,794 subjects across 49 countries) extracted and standardized from PubMed. ● PEPRKD-Depression incorporates 662 depression-related items, uses the innovative “FITT-VPP” principle (expanding FITT-VP with “Periods of time”) to structure exercise regimens, and is publicly accessible at https://dpa.bioinf.org.cn/. ● The database provides structured exercise intervention information and serves as a preliminary decision-support resource for exercise recommendations and future research.
Supplemental material
Supplemental material - PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression
Supplemental material for PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression by Danting Li, Jiale Du, Ting Bao, Yingbo Zhang, Jinhua Feng, Xingyun Liu, Rongrong Wu, Cheng Bi, Amin Ullah, Bairong Shen in DIGITAL HEALTH
Supplemental material
Supplemental material - PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression
Supplemental material for PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression by Danting Li, Jiale Du, Ting Bao, Yingbo Zhang, Jinhua Feng, Xingyun Liu, Rongrong Wu, Cheng Bi, Amin Ullah, Bairong Shen in DIGITAL HEALTH
Supplemental material
Supplemental material - PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression
Supplemental material for PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression by Danting Li, Jiale Du, Ting Bao, Yingbo Zhang, Jinhua Feng, Xingyun Liu, Rongrong Wu, Cheng Bi, Amin Ullah, Bairong Shen in DIGITAL HEALTH
Supplemental material
Supplemental material - PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression
Supplemental material for PEPRKD-depression: A knowledge database supporting evidence-based personalized exercise prescription recommendations in depression by Danting Li, Jiale Du, Ting Bao, Yingbo Zhang, Jinhua Feng, Xingyun Liu, Rongrong Wu, Cheng Bi, Amin Ullah, Bairong Shen in DIGITAL HEALTH
Footnotes
Author contributions
Bairong Shen and Danting Li: Conceptualization; Danting Li and Ting Bao Methodology, Investigation; Danting Li, Jiale Du and Xingyun Liu: Data Curation, Resources; Danting Li, Jiale Du, Ting Bao, Yingbo Zhang, Jinhua Feng, Rongrong Wu, Cheng Bi, Amin Ullah, Bairong Shen: Writing, Reviewing and Editing; Bairong Shen: Supervision, Funding acquisition. All the authors completely consented with all the data in the study, critically revised the manuscript for important intellectual content, and approved the final version. All authors contributed to the study’s design and concept.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grants 32270690 and 32070671) and the Sichuan Province Science and Technology Program (grant 2024YFHZ0205, 2024YFHZ0069).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.