
Abstract
Background and Aims
Guidelines for exercise recommendations are typically designed for the population as a whole and do not account for individual differences, making it challenging to provide personalized exercise training for individuals with complex conditions. To address this issue, this study aimed to develop PAHFKB (Physical Activity-Heart Failure Knowledge Base), a knowledge-based system for personalized exercise prescription (EP) for heart failure (HF), by mining, analyzing, and organizing existing literature and data on the relationship between physical activity (PA) and HF.
Methods
Firstly, 3186 citations on PAHF were gathered from PubMed. Then, the data standards for personalized PAHF were defined with the entity-relationship model. Following data collection in accordance with these standards, PAHFKB was developed using MySQL and ASP.NET, integrating elaborate and diverse PAHF evidence, knowledge-based EP and visualization tools.
Results
PAHFKB (pahfkb.sysbio.org.cn) incorporated 357 studies published between 1989 and 2021, involving over 900,000 subjects from 43 countries. And 1010 PAHF items were extracted, encompassing 357 exercise training protocols, 333 outcomes, and 42 risk factors for HF prevention and intervention. Among all protocols, the most frequently employed regimen consisted of three 60-minute sessions of moderate-intensity aerobic exercise training on a weekly basis.
Conclusion
PAHFKB is an online system designed to support personalized EP in HF management. It incorporates diverse tools and visualization and will promote personalized decision support, establish data standards, and advance interpretable artificial intelligence in digital health. Ultimately, it will enhance clinical practice and digital therapy in the prevention and intervention of HF.
This is a visual representation of the abstract.
Introduction
Heart failure (HF) refers to a group of complex syndromes arising from ventricular dysfunction, characterized by exercise intolerance, fatigue, and dyspnea.1,2 Despite the evolution in medical treatments, the global incidence, burden, and cost of HF continue to persist unabated.3,4 From 1990 to 2017, both the prevalence and years lived with disability of HF have nearly doubled. 3 In addition to population aging, the suboptimal implementation of pharmacological and device-based therapies contributes to the issue, particularly in developing countries. For example, in China, the utilization of beta-blockers and cardiac resynchronization therapy among patients with HF was a mere 25.6% and 0.3%, respectively. 5
In comparison, exercise training offers a more cost-effective and efficient nonpharmacological intervention to managing HF in most cases. 6 Research increasingly shows that systematic and regular physical activity (PA) significantly enhances cardiorespiratory fitness while reducing HF-related morbidity and hospitalization rates.7,8 Given its numerous benefits, exercise training is recognized as a vital preventive and interventional strategy for HF.9–11 Numerous guidelines have been published to promote exercise training, yet, its clinical practice remains suboptimal. On the one hand, these guidelines or related reviews only provide general recommendations for all diseases.9,12 On the other hand, although they focused on the exercise medicine research status of cardiovascular disease (CVD), they only assessed and explained the effectiveness of exercise for patients and provide common knowledge (such as how to conduct exercise tests, and provide standardized exercise protocols), but lack personalized guidance based on evidence.13–16 They neglected individual specificities, such as medication use, comorbidities, and surgical history.9,10 Comorbidities refer to the simultaneous presence of one or more diseases or conditions in a single individual. These diseases or conditions can interact with each other and may exacerbate the severity of a primary disease. For example, patients with HF often have other conditions such as diabetes, hypertension, or chronic kidney disease. These comorbidities can affect the treatment outcomes and prognosis of HF.17–19 When prescribing a personalized exercise regimen, the presence of comorbidities has a significant impact on the design and implementation of the prescription. First, comorbidities may limit the frequency, intensity, and types of exercise that the patient can perform. Second, comorbidities may also increase the risks associated with exercise. Therefore, when designing an exercise prescription (EP), a thorough health assessment is essential to ensure the safety and effectiveness of the exercise program. While growing studies indicate that individual differences, such as genetic factors, physiological and physical characteristics, and lifestyle, can significantly affect the outcomes of exercise training.20,21 Therefore, when prescribing exercise for these individuals, physicians should consider multiple factors, such as age, health status, exercise habits, risk factors, and medical history. Currently, there have been several attempts to develop personalized EPs in the field of CVD.22,23 However, these attempts still have certain limitations. For instance, the exercise protocol is still limited to the FITT (frequency, intensity, time, type) principle; the tools lack public and reliable experimental evidence support; and the reasoning behind the exercise protocol lacks interpretability. Consequently, in clinical practice, prescribing safe and effective exercise regimens for specific patients remains challenging for physicians.24,25 Currently, there is no comprehensive investigation about existing literature on PAHF to support the development of personalized EPs system. 26
To address this issue and enhance clinical practice for exercise training, we developed the Physical Activity-Heart Failure Knowledge Base (PAHFKB) to provide comprehensive, evidence-based support for EP recommendations tailored to individuals with HF and associated risks. First, we summarized existing studies on PAHF and identified potential individual specificities that may influence EP generation. Then we established data standards to describe and collect the personalized PAHF dataset from literature. Finally, we developed a knowledge-based automated system for EP that considers individual specificities and designed a web-based user interface, providing clinicians and researchers with access to data resources, PA recommendation tools, and data analysis tools.
Methods
Data source
To ensure the rigor and validity of our findings, we utilized the PubMed database as our primary data source. PubMed is the preferred literature search tool in the field of medicine, biology, and life sciences, offering rigorously reviewed literature to ensure high-quality academic resources. We employed the search strategy “(Physical activity[ti] OR Exercise[ti] OR Sports[ti]) AND Heart failure[ti]”, which yielded 3186 publications until 31 December 2021 (Figure 1). Given the evidence quality,1,10 we excluded duplicates (2 results), nonhuman studies (223 results), letters (153 results), case reports (18 results), and other unqualified studies (193 results), resulting in 2595 studies for full-text screening. After manual screening, we excluded 2238 articles that lacked conclusive data or conclusions, leaving with 258 original articles and 99 systematic reviews and meta-analyses for data collection.

Flowchart for collection of PAHF studies. HF: heart failure; PA: physical activity.
Data extraction
Data extraction comprises data collection and standardization. Rational and consummate data standards are the pre-requisite for both steps. Therefore, we developed structure and content standards to define and standardize PAHF data drawing upon related studies, state-of-the-art guidelines, professional expert opinions,9,10,27,28 and the functional requirements of PAHFKB.
We formed an entity-relationship model (Figure 2) to depict the main framework of relationships between PA and HF. In this model, a complete PAHF association included four main components: demographical characteristics, HF information, risk factors, PA protocol, and the effects of PA under the above conditions. To provide a more precise description of PA information, in addition to the traditional “FITT” concept,9,10,27 we added the latest parameters from ACSM EP, V(volumn) and P(progression). 28 “Volume” refers to the capacity of exercise. For each exercise protocol, we calculated the exercise minutes required per week, in minutes. “Progression” refers to the process of gradually increasing exercise load or intensity in EP, which can ensure physical adaptation and gradual improvement of exercise performance. We documented details in the exercise protocol on how to progressively increase the exercise load or intensity. At the meantime, we incorporated “modality” and “protocol” to record specific exercise forms (e.g. walking, cycling, and jogging) and detailed exercise training strategies. In addition, we also supplemented information regarding contraindications. Informing about contraindications ensures that the exercise protocol fits to the individual's health condition, avoiding potential worsening situations. To account for specific HF conditions, we used “type,” “stage,” and “etiology.” We also extracted possible factors from available medical evidence to describe demographic characteristics and risk factors. Except for the essential entities, we included study and reference entities to record research information for validation and future updates. As a knowledge base, we aimed to include a wide range of data sources to ensure the comprehensiveness of PAHFKB. Consequently, the data quality might be uneven. Therefore, we used “recommendation classification” and “evidence level” based on the ESC quality criteria to differentiate the different levels of data quality. 10

ER model for PAHF data. ER: entity-relationship; HF: heart failure; PA: physical activity.
The attributes for specific PAHF information in the database were standardized for sharing and analysis, as illustrated in Table 1. Using the established criteria, PAHF data was manually extracted from the relevant literature and systematically stored in the database.
Data content description criteria.
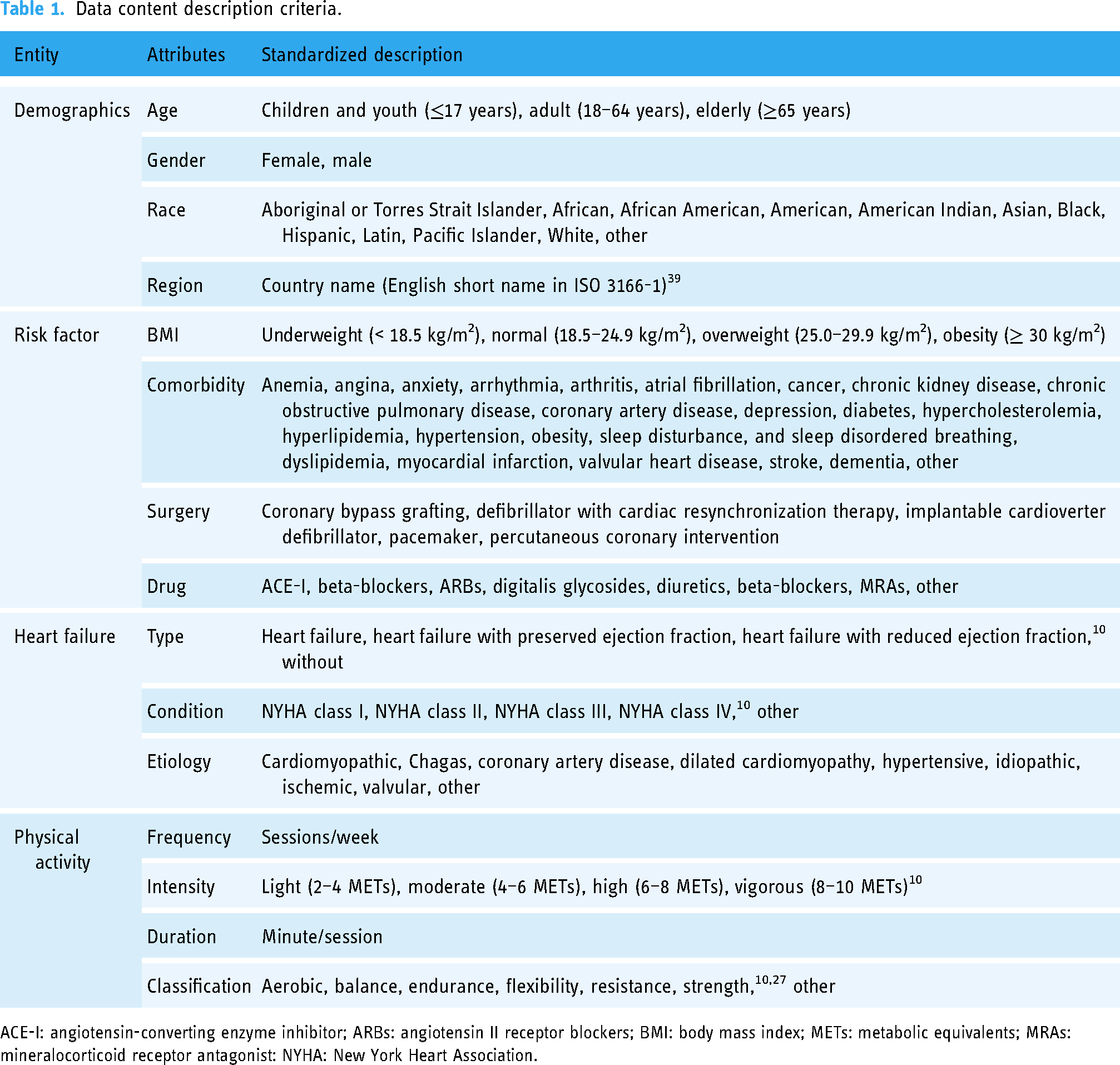
ACE-I: angiotensin-converting enzyme inhibitor; ARBs: angiotensin II receptor blockers; BMI: body mass index; METs: metabolic equivalents; MRAs: mineralocorticoid receptor antagonist: NYHA: New York Heart Association.
Knowledge base implementation
The Browser/Server architecture and the WIMA (Windows, IIS, MySQL, ASP.NET) web stack were adopted to construct the web-based platform. This architecture consisted of three layers: data, business, and presentation. In the data layer, the MySQL database management system was utilized to store and retrieve data. In the business layer, the ASP.NET MVC framework, coded in C#, was employed to develop the algorithms for all system functions (e.g. search engine, data visualization, and EP recommendation tools). Lastly, the presentation layer was implemented using the Bootstrap and Echarts frameworks, programmed with HTML and JavaScript, to provide a user-friendly interface. 29
Results
Data statistics
PAHFKB contains 357 studies published from 1989 to 2021 (Supplemental Figure 1), including 258 original articles and 99 systematic reviews/meta-analyses. Most of these studies were conducted in developed countries, with the United States contributing 62, followed by Germany and Australia with 33 and 30, respectively (Figure 3(a)). These included more than 900,000 subjects aged 18 to 88, with 47% females and 53% males. Notably, New York Heart Association (NYHA) classification was the most frequently used in those studies. After standardizing other classifications according to the NYHA classification, HF subjects in classes I to IV were distributed as follows: 12%, 39%, 39%, and 5%, respectively.

Data statistics for PAHFKB: (a) heat map of country distribution; (b) classification of risk factors; (c) classification of outcomes; (d) outcomes with conflict conclusions; (e) classification of FITT. ACE-I: angiotensin-converting enzyme inhibitor; ARBs: angiotensin II receptor blockers; BMI: body mass index; E/A: mean ratio of early to late mitral inflow velocities; E/E’: the ratio of early diastolic transmitral velocity to early diastolic tissue velocity; FITT: frequency, intensity, time, type; HF: heart failure; IL-6: interleukin-6; LVEDV: left-ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; MHC I: myosin heavy chain class I; MRAs: mineralocorticoid receptor antagonist; NT-pro BNP: N-terminal pro-B-type natriuretic peptide; PA: physical activity; PAHFKB: Physical Activity-Heart Failure Knowledge Base; PWV: pulse wave velocity; ; RVSP: right ventricular systolic pressure; VE: minute ventilation; VE/VCO2: the slope of the minute ventilation to carbon dioxide production.
From these studies, 1010 items were extracted, comprising 357 exercise training protocols, 333 outcomes, and 42 risk factors for PA in the prevention and intervention of HF. As illustrated in Figure 3(b), risk factors in PAHFKEB are categorized into four types: body mass index, drug intake, comorbidity, and surgery history. Overweight (40%), diabetes (29%), angiotensin-converting enzyme inhibitor (ACE-I) (20%), and coronary bypass grafting (51%) represent the most prevalent risk factors for each type. Figure 3(c) displayed the outcomes which can be divided into physical fitness-related (n = 313) and psychological fitness-related (n = 20). Physical fitness-related outcomes can be further subdivided into cardiorespiratory fitness (n = 151), metabolic fitness (n = 6), morphological fitness (n = 6), motor fitness (n = 2), muscular fitness (n = 29), and other physical fitness (n = 119). 30 Among these, 13 PA outcomes were identified with conflicting conclusions (Figure 3(d)). Subsequent studies can use this statistical analysis to assess the consistency of conclusions regarding specific PA.
Furthermore, we summarized all the EPs according to the HF conditions and general risk factors (Figure 3(e) and Supplemental Table 1) and analyzed the data flow between different exercise FITT, and outcomes (Supplemental Figure 2). Overall, frequency ranges from daily to weekly, intensity varies from light to vigorous, duration spans from 1 to 240 minutes per session, and types include aerobic, balance, endurance, resistance, and strength. The most common features are 3 sessions per week (47%), moderate intensity (40%), 60 minutes per session (21%), and aerobic exercise (38%).
User interface and applications
PAHFKB consists of six parts: “Home”, “PAHF Libraries”, “Exercise Prescription Tools”, “Analysis Tools”, “Contact Us”, and “Help”. The “Home”, “Contact Us”, and “Help” pages give a general introduction to the system, including basic information, data and tools portals, links to related guidelines, a user's manual, as well as contact information.
PAHF libraries
PAHF libraries (Figure 4(a)) provide users with a multifunctional search engine including keyword retrieve, datasets download, and detailed browse functions. By inputting keywords in the search box, users will get results from the database with matched parts highlighted. Then, by clicking the download button, users are allowed to save the results in multiple formats: JSON, XML, CSV, TXT, SQL, and MS Excel. Card and full-screen views, as well as customizable column choices, are available in the right-side toolbar for users to flexibly adjust the datasets table. The detail button also provides users with more information about specific PAHF items, such as the primary data and study design.

User interface of PAHFKB: (a) PAHF libraries; (b) exercise risk assessment tool; and (c) analysis tools. HF: heart failure; PA: physical activity; PAHFKB: Physical Activity-Heart Failure Knowledge Base.
Exercise risk assessment tools
Health screening before exercise is crucial to avoid adverse events, especially for patients and individuals with CVD risk factors. 31 Therefore, in accordance with the American College of Sports Medicine's (ACSM) guidelines, PAHFKB provides exercise risk assessment tools (Figure 4(b)) that consist of the PA level assessment questionnaire (PAL-Q) and the PA readiness questionnaire (PAR-Q).9,32 These questionnaires should be completed and used under the guidance of a doctor. Firstly, through the PAL-Q, users can obtain optimal exercise intensity recommendations based on their daily exercise activity under a doctor's supervision. Subsequently, by completing the PAR-Q, users can assess their exercise risk under a doctor's supervision to determine whether medical clearance is needed before initiating exercise. Before using PA recommendation tool, we have emphasized the importance of conducting exercise tests and provided the detail link. Additionally, The Borg Rating of Perceived Exertion (RPE) 33 is provided for individuals to self-report their perceived exertion during physical activities. Using these exercise risk assessment tools under the guidance of a doctor is important in ensuring the safety of patient exercise and monitoring the effectiveness of exercise training.
Analysis tools
This module offers five visualization tools to assist users to analyze PAHF data: publication years, country distribution, classification of risk factors, outcomes, and the data flow between outcomes and PA FITT (Figure 4(c)). Each tool consists of two parts: data selection and result visualization. In the first part, users are prompted to select the data for analysis. The results are subsequently generated and displayed in the second part. The view toggle and result download functions can be accessed through the right toolbar.
Physical activity recommendation tool
The PA recommendation tool consists of two parts (Figure 5):
automated medical history-taking module and PA recommendations module.

Physical activity recommendation tool of PAHFKB. PAHFKB: Physical Activity-Heart Failure Knowledge Base.
Initially, users are required to answer questions in the first module. Based on the user's responses, this module predicts potential PA protocols in the PAHF libraries. Then, considering feedback from the libraries and the prioritization of EP decision factors (HF condition, risk factors, and demographic characteristics), the module automatically generates the next question and relevant options. To ensure accurate and personalized recommendations, this automated medical history-taking process continues looping to collect the user's physical conditions until the knowledge base infers the optimal PA recommendations.
Subsequently, the second module presents the final recommendations. Each recommendation is extracted from an evidence-based study and includes basic information along with the standardized PA protocol (statistical results, classification of recommendations, and reference information). Additionally, this module offers a view toggle, data filter, customizable columns, and recommendation download functions to assist users in comparing and analyzing recommendations flexibly.
Figure 5 illustrates the process of PA recommendation. First, the automated medical history-taking module sequentially generates six questions to collect information about the user's HF type, status, comorbidities, surgery history, drug intake, and age. Then, based on the answers (“heart failure”, “NYHA class II”, “diabetes”, “coronary bypass grafting”, “ACE-I”, and “elderly”), the second module recommends six optimal PA protocols and relevant special cautions. In this case, the most frequently recommended FITT for PA is “2 times/week”, “moderate”, “60 minutes/session”, and “aerobic”.
Discussion
To facilitate the clinical translation and scientific investigation of exercise training for the prevention and intervention of HF, we developed the automated knowledge-based system on EP in HF, termed the PAHFKB. In contrast to the prevailing clinical and health practice guidelines, this work provides comprehensive, diverse, and informative collection of PAHF resources, rather than relying on “averaged” evidence. Additionally, the PAHFKB system incorporates search engines, EP recommendation tools, and visualized analysis tools. Driven by data, facts, and knowledge, these tools deliver timely and up-to-date PAHF support for future research in personalized and digital health management. 34 During data extraction, we established the primary framework to characterize PAHF data, marking an initial step towards standardizing personalized EP for HF rehabilitation.
Specifically, existing guidelines offer exercise recommendations for patients with a single disease but fail to address exercise training for those with multiple conditions. Capitalizing on its benefits, the PAHFKB can assist healthcare professionals in offering more personalized and diverse EPs tailored to the unique needs of each patient. As depicted in Figure 5, the PA recommendation tool provided 6 evidence-based exercise training recommendations for an individual with both HF and diabetes after fully considering HF conditions, the main comorbidity, and important risk factors (“heart failure”, “NYHA class II”, “diabetes”, “coronary bypass grafting”, “ACE-I”, and “Elderly”), rather than only one broad recommendation for all patients with HF. These evidence-based recommendations not only aid healthcare professionals in making informed decisions about EPs but also offer individuals a broader range of options to enhance the efficiency and adherence to their exercise programs. Although previous efforts have been made to develop relevant health guidelines or EP systems in CVDs, such as Life's Simple 7 of AHA, the P3-EX, and the EPAC EXPERT tool, their underlying logic remains reliant on guidelines or non-evidence-based prescription recommendation processes.23,35–37 Comparatively, our manually curated and standardized PAHF resources can provide more robust data support and knowledge-driven foundations for the development of personalized clinical decision support system in the future. Table 2 provides a detailed comparison of these guidelines or tools in various aspects, demonstrating the advantages of PAHFKB.
The comparison of current CVD health guidelines/exercise prescription tools.

AHA: American Heart Association; CVD: cardiovascular disease; FITT-VP: frequency, intensity, time, type, volumn and progression; PAHFKB: Physical Activity-Heart Failure Knowledge Base; The EAPC expert tool: The European Association of Preventive Cardiology Exercise Prescription in Everyday Practice and Rehabilitative Training (EXPERT) tool; P3-EX: Prioritize Personalize and Prescribe Exercise.
Despite being the first PAHFKB, this study has some limitations. First, the process of literature reading and data entry is carried out manually, which ensures higher accuracy but results in a low efficiency. To address the increased workload brought by the expansion of data sources, we plan to use natural language processing algorithms for data filtering and reliminary extraction in the next version, thereby improving efficiency. Second, the existing PAHF data standards are relatively simplistic, only considering the primary decision parameters. In the next version, a more systematic and comprehensive data standard (e.g. ontology) will be developed for PAHF, covering as many relevant influencing factors as possible. Third, although the datasets and recommendations in PAHFKB are evidence-based, external validation is necessary to assess the potential medical and economic benefits of this system. Future research will involve prospective studies evaluating the system's impact on clinical practice. Lastly, while the basic PA recommendation tool offers good interpretability and transparency, its capabilities are limited by the data sources. It can only provide answers based on existing evidence and is unable to predict or address complex questions. In subsequent work, deep learning algorithms will be combined to create a more powerful decision support model, while maintaining the overall interpretability of the model.26,38
Conclusion
PAHFKB holds profound significance in advancing the management of HF through personalized EPs. By synthesizing data from a vast array of studies, PAHFKB transcends traditional, one-size-fits-all guidelines, offering a user-friendly tool that tailors exercise recommendations to the unique needs of individual patients. This system not only bridges the gap between research and clinical practice but also sets a new standard for integrating data-driven insights into personalized healthcare. Its ability to accommodate the complexities of comorbid conditions and varying patient profiles ensures that clinicians can make informed decisions that enhance patient outcomes and adherence to exercise regimens. PAHFKB is a transformative platform that has the potential to revolutionize PA management for HF, ultimately leading to more precise, effective, and patient-centered care.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241299083 - Supplemental material for PAHFKB: A knowledge base to support personalized exercise prescription recommendations in prevention and intervention of heart failure
Supplemental material, sj-docx-1-dhj-10.1177_20552076241299083 for PAHFKB: A knowledge base to support personalized exercise prescription recommendations in prevention and intervention of heart failure by Ke Zhang, Shumin Ren, Ting Bao, Rongrong Wu, Erman Wu, Xingyun Liu, Chaoying Zhan, Jinhong Wei, Li Shen, Danting Li and Bairong Shen in DIGITAL HEALTH
Supplemental Material
sj-xlsx-2-dhj-10.1177_20552076241299083 - Supplemental material for PAHFKB: A knowledge base to support personalized exercise prescription recommendations in prevention and intervention of heart failure
Supplemental material, sj-xlsx-2-dhj-10.1177_20552076241299083 for PAHFKB: A knowledge base to support personalized exercise prescription recommendations in prevention and intervention of heart failure by Ke Zhang, Shumin Ren, Ting Bao, Rongrong Wu, Erman Wu, Xingyun Liu, Chaoying Zhan, Jinhong Wei, Li Shen, Danting Li and Bairong Shen in DIGITAL HEALTH
Footnotes
Contributorship
BS and KZ designed the research; BS, KZ, SR, and TB designed the data extraction and standardization criteria; KZ, SR, XL, CZ, EW, and JW conducted data collection, extraction, and standardization; KZ, EW, XL, RW, and LS designed and developed users’ interface; KZ, TB, SR, RW, DL, and EW drafted the edited manuscript; and BS supervised the study and revised the manuscript.
Data availability statement
The raw data and tools are available at pahfkb.sysbio.org.cn.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grant no. 32070671), the COVID-19 research projects of West China Hospital Sichuan University (grant no. HX-2019-nCoV-057) as well as the regional innovation cooperation between Sichuan and Guangxi Provinces (2020YFQ0019).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.