
Abstract
Background
Benign Paroxysmal Positional Vertigo (BPPV) is common with high recurrence. Social media platforms like TikTok and Bilibili offer health-related content, but their quality and reliability remain unclear.
Objective
This study aims to evaluate the content and quality of BPPV-related videos on TikTok and Bilibili.
Methods
A total of 199 BPPV-related short videos from TikTok and Bilibili were collected between September 25 and 28, 2025. Video characteristics were extracted, and quality was assessed using the Global Quality Score (GQS) and modified DISCERN scale (mDISCERN). Content accuracy was evaluated based on clinical guidelines. Non-parametric tests and Spearman correlation analysis were used to compare uploader groups and explore the relationship between engagement and video quality.
Results
The videos had a median duration of 99 seconds. TikTok videos showed significantly higher interaction metrics than those on Bilibili (all P < 0.001). Content primarily covered clinical presentation, diagnosis, and treatment, while epidemiology and prevention were underrepresented. The median GQS was 3.00, and the median mDISCERN score was 2.00, indicating low quality and reliability. Professional videos had significantly higher mDISCERN scores than individual user videos (P < 0.001), but both groups had low scores. For content accuracy, the lower quartile for professional videos was exceptionally low (Q1 = 0.00), with 25% of these videos containing significant errors or omissions. No significant correlations were found between engagement metrics and quality scores (r = 0.00-0.11, P > 0.05).
Conclusion
BPPV-related short videos on TikTok and Bilibili generally have low quality, reliability, and accuracy. While professional videos are more reliable, they lack evidence-based content and omit key information. Strengthening content moderation and increasing professional involvement is crucial for improving digital health education.
1. Introduction
Benign Paroxysmal Positional Vertigo (BPPV), commonly referred to as “otolithiasis,” is a prevalent vestibular disorder characterized by brief and recurrent episodes of vertigo and positional nystagmus, triggered by specific head movements. 1 This condition is typically caused by the displacement of otoconia in the inner ear, leading to abnormal stimulation of the semicircular canals. 2 It is estimated that BPPV accounts for approximately 20-30% of patients experiencing vertigo, 3 with a lifetime prevalence of up to 2.4%. 4 The recurrence rate is about 5-13.5% within six months, increasing to 15-30% after one year. 5 BPPV significantly impacts patients’ quality of life, raises the risk of falls, and imposes psychological burdens.6–9 Furthermore, it may elevate the risk of ischemic stroke, dementia, and other diseases, resulting in both health and economic challenges.10–13 This situation is exacerbated by the general lack of disease awareness among patient populations. Therefore, enhancing public awareness of BPPV can facilitate early intervention, promote standardized treatment, and improve prognosis, while also reducing associated social and economic burdens.
BPPV rely on specialized procedures. Accurate diagnosis requires positional tests, such as the Dix-Hallpike maneuver, to trigger characteristic nystagmus. 14 The primary treatment involves manual repositioning, like the Epley maneuver, which must be customized based on the affected semicircular canal. This procedure has strict requirements for the angle of head rotation and the duration of position maintenance. 15 Consequently, BPPV cannot be reliably diagnosed remotely. Self-repositioning attempts can lead to otolith displacement, symptom worsening, or the onset of complex BPPV. 16 In elderly patients, improper neck rotation may also cause serious complications, such as cervical spine injury or vertebral artery dissection. 17 Furthermore, misdiagnosing central vertigo as BPPV can delay treatment, potentially missing the critical window for managing severe cerebrovascular events. 18 Therefore, providing the public with accurate and reliable information about BPPV is essential for promoting timely medical intervention and preventing the risks associated with self-treatment.
The rise of digital media has transformed social media platforms into primary channels for disseminating health information. Platforms like TikTok and Bilibili have large user bases, algorithm-driven personalized recommendation systems, and high interactivity, enabling rapid dissemination of medical content worldwide.19,20 Short-video platforms lack robust peer review and content verification processes, leading to significant variability in information quality. Research indicates that health-related videos on TikTok and Bilibili frequently exhibit poor source attribution, limited professional oversight, and weak evidence-based foundations.21–24 These issues contribute to the dissemination of misinformation, potentially delaying accurate diagnoses and timely treatment.
Research on the quality of BPPV-related information on short-video platforms remains limited. Unlike many chronic conditions where misinformation primarily leads to misconceptions, BPPV treatment depends heavily on procedural accuracy, meaning that errors in video content can directly result in physical harm. This unique clinical characteristic makes BPPV a particularly important case for studying digital health misinformation. This study is the first to systematically evaluate BPPV-related short videos on social media platforms. We aim to analyze the distribution, quality, reliability, and accuracy of video content, compare differences among various uploaders, and investigate the relationship between viewer interaction metrics and information quality. The findings are expected to provide evidence-based support for optimizing digital health communication strategies and developing public health intervention measures on social media.
2. Methods
2.1. Study design
This study adopted a cross-sectional design conducted from September 25 to 28, 2025. The objective was to analyze the content, quality, and reliability of videos related to BPPV on TikTok and Bilibili platforms.
2.2. Data source and search strategy
The Chinese versions of TikTok and Bilibili were selected as the data sources. During the study period, the keyword ‘耳石症’ (Otolithiasis) & ‘良性阵发性位置性眩晕’ (Benign Paroxysmal Positional Vertigo) was used in the search. To avoid bias due to personalized recommendation algorithms, all searches were conducted while logged out. Previous studies have indicated that the top 100 videos in search results sufficiently represent the core content of a specific field on a platform.25,26 To improve the robustness of the findings, this study expanded the sample to include the top 150 videos on each platform for preliminary screening.27,28
2.3. Inclusion and exclusion criteria
2.3.1. Inclusion criteria
(1) The video content is related to Benign Paroxysmal Positional Vertigo. (2) The video contains language or textual explanations directly related to the disease.
2.3.2. Exclusion criteria
(1) Videos that are advertisements or promotional in nature. (2) Videos whose primary content is unrelated to Benign Paroxysmal Positional Vertigo, including but not limited to migraines and epilepsy. (3) Duplicate videos. (4) Videos with a duration exceeding 20 minutes. Recent studies suggest that the optimal video length is between 5 and 10 minutes.29,30 In this study, however, the duration was extended to 20 minutes to accommodate viewers who prefer longer videos.31,32
2.4. Data extraction
For each included video, the following features were extracted: video duration (seconds), number of likes, shares, comments, saves, and video source. Topic types (e.g., treatment, symptoms, diagnosis, epidemiology, prevention). Uploader types (e.g., professionals, other specialists, individual users, organizations).
2.4.1. Video classification
2.4.1.1. Uploader characteristics
The uploaders were categorized as: (1) Professionals: Ear, Nose, and Throat doctors, neurologists. (2) Other specialists: Neurosurgeons, cardiologists, dermatologists, etc. (3) Individual Users: Patients, science communicators. (4) Organizations: For-profit and non-profit organizations.
2.4.1.2. Video content
The content topics were classified into epidemiology, etiology, symptoms, diagnosis, treatment, and prevention.
2.5. Quality, reliability and accuracy assessment
The overall quality of the videos was evaluated using the Global Quality Scale (GQS), 33 a 5-point Likert scale assessing the accuracy, usability, coherence, and practical value of online information. A score of 1 indicates poor quality with limited usefulness, whereas a score of 5 denotes excellent quality, characterized by clarity, comprehensiveness, and informativeness. Video reliability was assessed using the modified DISCERN scale (mDISCERN), 34 which includes five criteria: 1) the video is clear, concise, and easy to understand; 2) information sources are reliable; 3) content is balanced and impartial; 4) additional information sources are provided for patients; and 5) uncertainties or controversial topics are appropriately addressed. Each criterion is scored as “yes” (1 point) or “no” (0 points), yielding a total score ranging from 0 to 5. For both GQS and mDISCERN, scores of 1–2 indicate low quality, 3 indicates moderate quality, and 4-5 indicates high quality.
To evaluate the accuracy of medical information in BPPV-related videos, we applied the Accuracy Digital Health Instrument (ANDI) framework, 27 adapted in accordance with the 2017 AAO-HNSF BPPV Clinical Practice Guidelines 14 and the Bárány Society diagnostic criteria. 4 A structured checklist was developed comprising three dimensions: treatment accuracy, guideline consistency, and misinformation. Each item was rated on a 5-point scale following the ANDI scoring system, where 4 indicates complete accuracy or compliance, 3 indicates minimal flaws, 2 indicates partial accuracy, 1 indicates major errors, and 0 indicates that the item was not addressed. Scores were summed within each dimension, yielding ranges of 0-12 for treatment accuracy and 0-8 for both guideline consistency and misinformation, with higher misinformation scores indicating fewer errors. Quality levels were subsequently classified based on these scores, with treatment accuracy categorized as low (0-4), moderate (5-8), or high (9-12), and guideline consistency and misinformation categorized as low (0-2), moderate (3-5), or high (6-8). Details of these scales are presented in Supplementary File Tables S1-S3.
The three assessors were licensed emergency physicians with extensive clinical experience in diagnosing and managing dizziness, particularly in the identification, diagnosis, and emergency treatment of BPPV. To ensure a standardized and consistent evaluation, all assessors underwent formal training prior to the assessment. Following the training, two physicians independently rated the videos, and any discrepancies were resolved through discussion with a third physician. To guarantee that the evaluation adhered to established clinical standards, it strictly followed the 2017 AAO-HNSF guidelines and Bárány Society recommendations. Inter-assessor reliability was then assessed using Cohen’s κ coefficient. According to Landis and Koch’s classification, a κ value greater than 0.80 indicates excellent agreement, 0.61-0.80 indicates substantial agreement, 0.41-0.60 indicates moderate agreement, and below 0.40 indicates poor agreement.
2.6. Statistical analysis
Descriptive statistics were used to summarize video characteristics. Continuous variables are reported as medians with first and third quartiles (Q1, Q3), and categorical variables are reported as counts and percentages. Differences in platform distribution were assessed using chi-square or Fisher’s exact tests, as appropriate, while the Mann-Whitney U test was applied to compare two groups. The Kruskal–Wallis H test was used for comparisons across multiple groups. When significant differences were detected, pairwise post hoc comparisons were performed using Bonferroni-adjusted significance levels for parametric tests or Dunn’s test with Bonferroni correction for nonparametric data. Spearman’s rank correlation coefficients were calculated to evaluate relationships between video engagement metrics and quality or reliability scores. Correlation strength was classified as negligible (|ρ| < 0.2), weak (0.2 ≤ |ρ| < 0.4), moderate (0.4 ≤ |ρ| < 0.6), strong (0.6 ≤ |ρ| < 0.8), or very strong (|ρ| ≥ 0.8). Two-sided p-values less than 0.05 were considered statistically significant. All analyses were conducted using R software (version 4.4.2), with significance set at P < 0.05.
3. Results
3.1. General characteristics of BPPV-Related videos
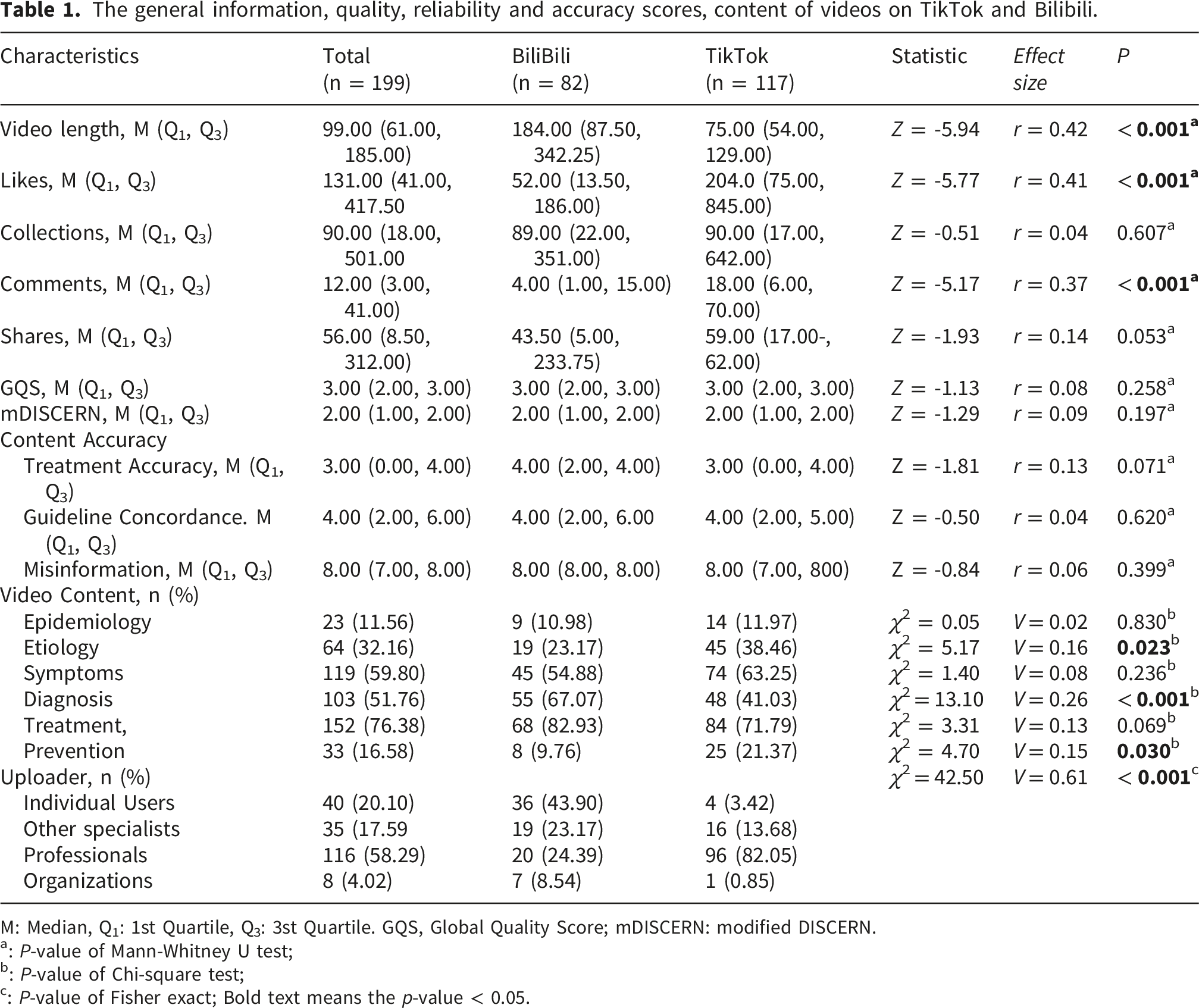
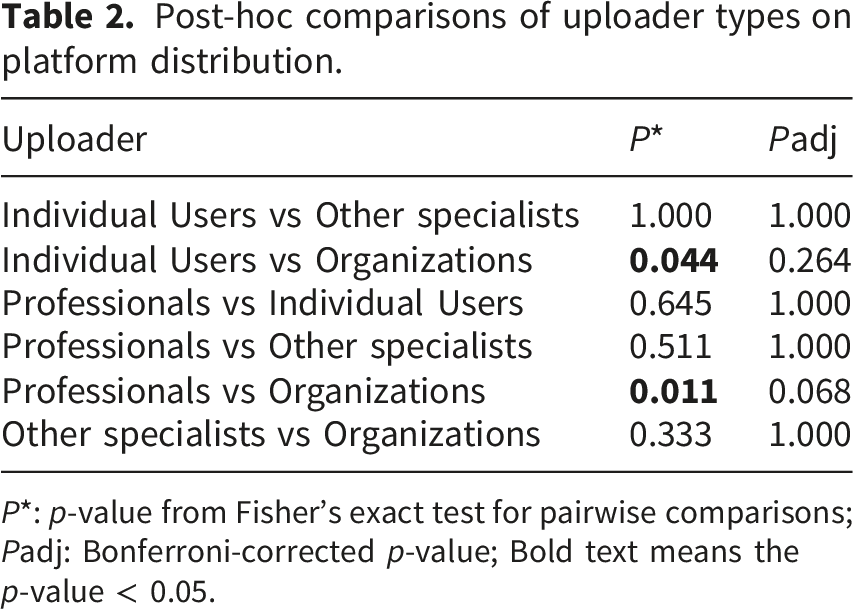
As shown in Figure 1, 199 videos were included in the study based on the exclusion criteria, with 117 videos from TikTok and 82 from Bilibili. The baseline characteristics of the study sample are summarized in Table 1. Videos on TikTok had significantly higher engagement metrics compared to those on Bilibili, with a median of 204 likes (75.00, 845.00) (r = 0.41, P < 0.001), 90 collections (17.00, 642.00) (r = 0.04), 18 comments (6.00, 70.00) (r = 0.37, P < 0.001), and 59 shares (17.00, 462.00) (r = 0.14). In contrast, Bilibili videos had longer durations with a median of 184.00 seconds (87.50, 342.25) (r = 0.42, P < 0.001) but showed lower engagement across all interaction metrics. Significant differences were observed in the overall distribution of uploader types across platforms (V = 0.61, P < 0.001). However, pairwise post hoc comparisons using Bonferroni correction showed no statistically significant differences between groups (adjusted P > 0.05) (see Table 2). Flowchart of video search, screening, and inclusion for analysis. The general information, quality, reliability and accuracy scores, content of videos on TikTok and Bilibili. M: Median, Q1: 1st Quartile, Q3: 3st Quartile. GQS, Global Quality Score; mDISCERN: modified DISCERN. a: P-value of Mann-Whitney U test; b: P-value of Chi-square test; c: P-value of Fisher exact; Bold text means the p-value < 0.05. Post-hoc comparisons of uploader types on platform distribution. P*: p-value from Fisher’s exact test for pairwise comparisons; Padj: Bonferroni-corrected p-value; Bold text means the p-value < 0.05.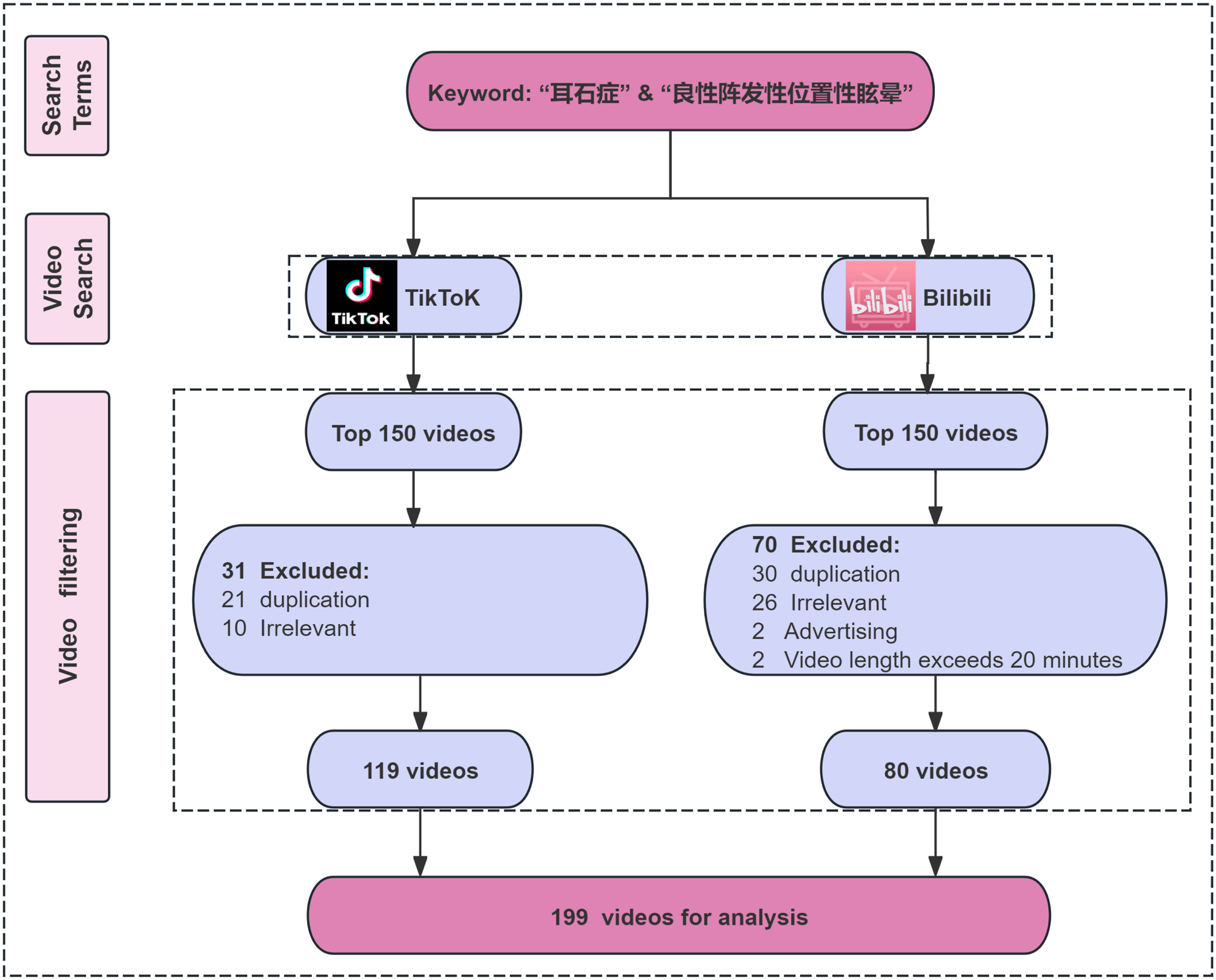
Characteristics of video uploaders about BPPV treatment on TikTok and Bilibili.
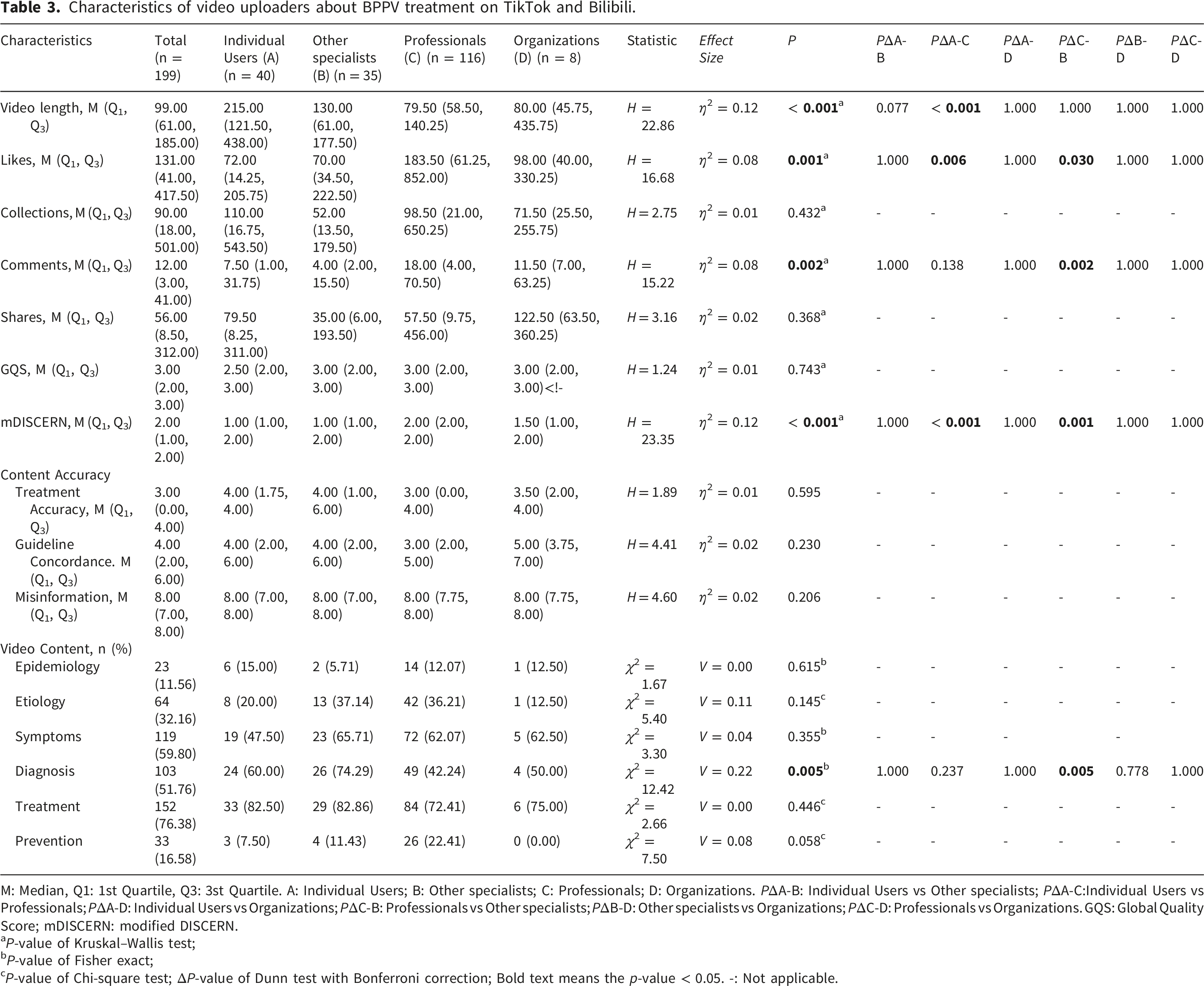
M: Median, Q1: 1st Quartile, Q3: 3st Quartile. A: Individual Users; B: Other specialists; C: Professionals; D: Organizations. PΔA-B: Individual Users vs Other specialists; PΔA-C:Individual Users vs Professionals; PΔA-D: Individual Users vs Organizations; PΔC-B: Professionals vs Other specialists; PΔB-D: Other specialists vs Organizations; PΔC-D: Professionals vs Organizations. GQS: Global Quality Score; mDISCERN: modified DISCERN.
aP-value of Kruskal–Wallis test;
bP-value of Fisher exact;
cP-value of Chi-square test; ΔP-value of Dunn test with Bonferroni correction; Bold text means the p-value < 0.05. -: Not applicable.
3.2. Uploader characteristics
In this study, the uploaders were categorized into professionals (58.29%), other specialists (17.59%), individual users (20.10%), and organizations (4.02%), as shown in Figure 2(a). On Bilibili, individual users were the largest contributors, accounting for 44% of the videos, followed by professionals, with fewer contributions from other specialists and organizations. In contrast, on TikTok, professionals dominated with 82% of the videos, followed by other specialists, while individual users and organizations contributed fewer videos, as depicted in Figure 2(b). Distribution of video uploaders on TikTok and Bilibili. (a) Overall distribution of video uploaders. (b) Distribution of video uploaders on TikTok and Bilibili.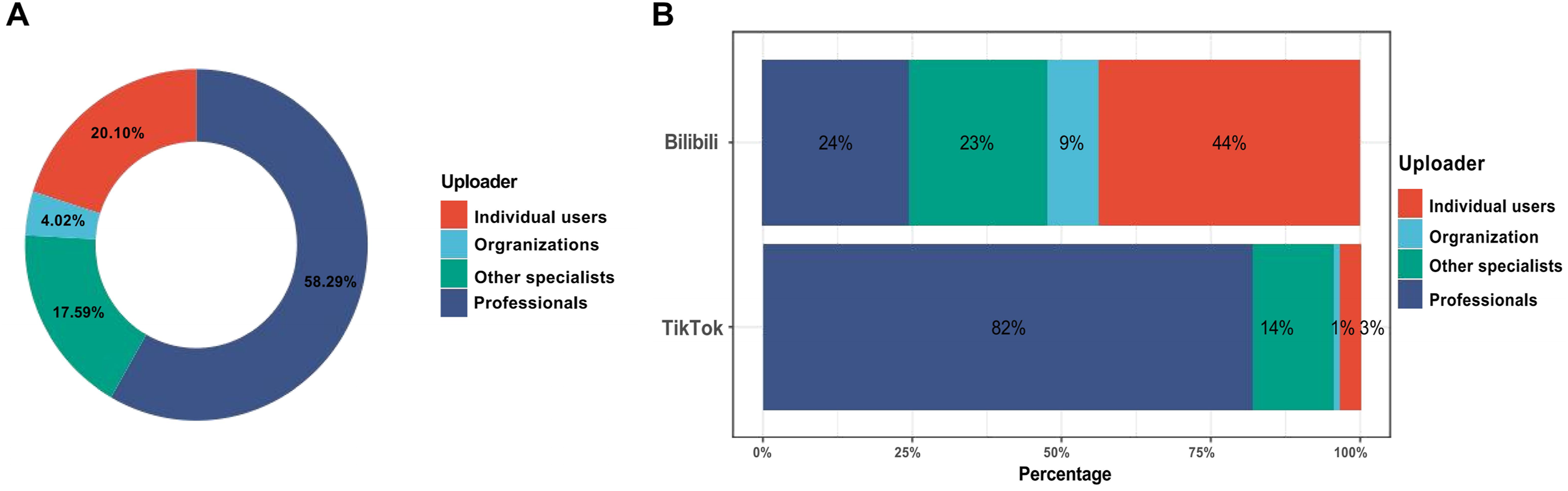
3.3. Content distribution of BPPV-related short videos
As detailed in Table 1 and Figure 3, The video content analysis, as illustrated in Table 1 and Figure 3, reveals that among the 199 videos analyzed, disease treatment emerged as the most frequently discussed topic (76.38%), followed by clinical manifestations (59.80%) and diagnosis (51.76%). Notably, treatment-related content was predominant across both platforms, with Bilibili featuring 82.93% of videos on this topic and TikTok 71.79%. In contrast, discussions on topics such as epidemiology (11.56%) and prevention (16.58%) were significantly less frequent. This pattern suggests a stronger focus on treatment content across both platforms, with relatively less attention paid to broader epidemiological and preventive measures. Significant differences in content distribution across platforms were observed for etiology (V = 0.16, P = 0.023), diagnosis (V = 0.26, P < 0.001), and prevention (V = 0.15, P = 0.030), indicating small to moderate effect sizes. Distribution of content themes in BPPV-related videos.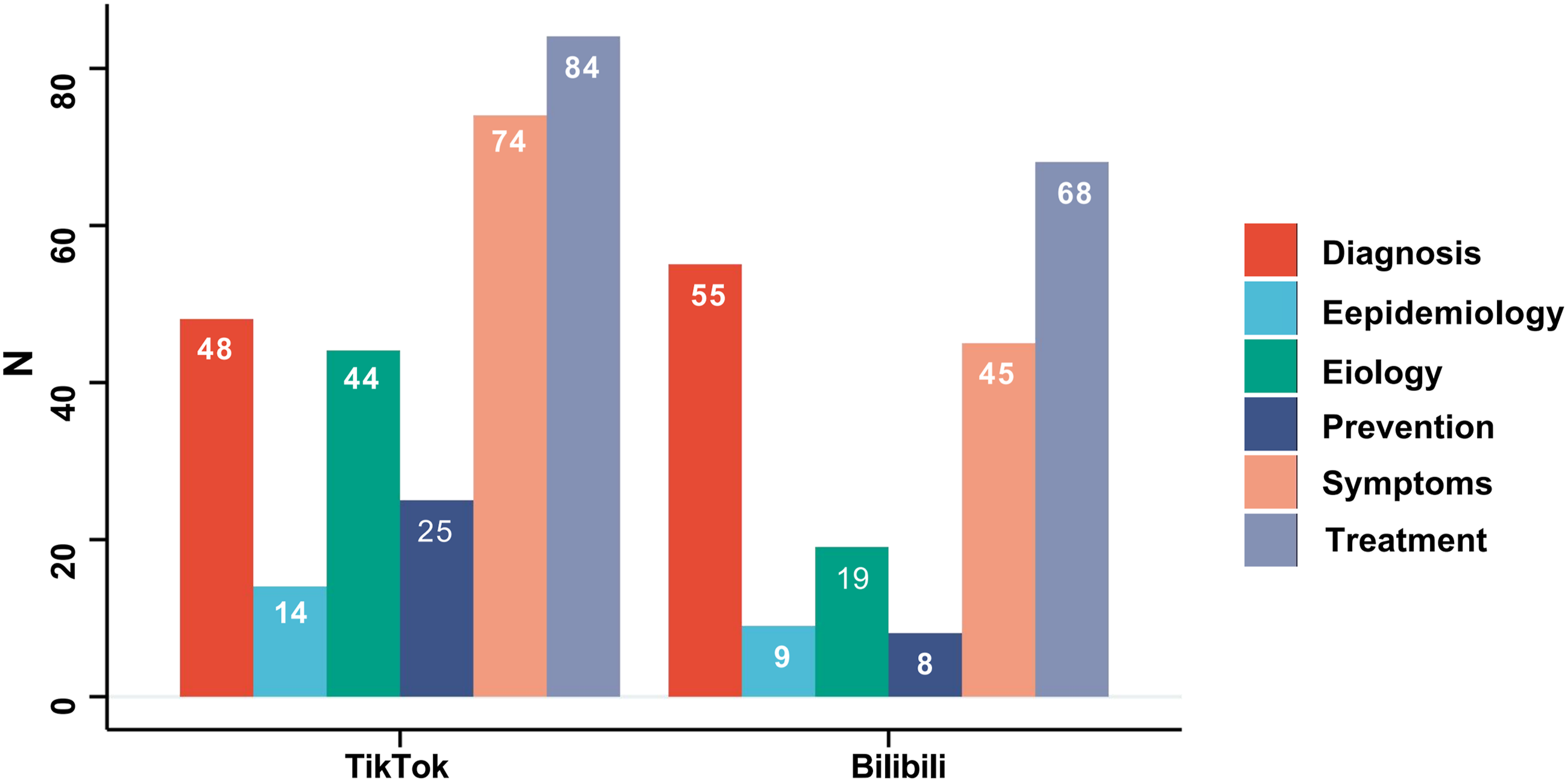
3.4. Comparison of video quality, reliability and accuracy across different uploaders
This study employed Cohen’s κ coefficient to evaluate the interrater reliability of GQS, mDISCERN, and content accuracy scores. The analysis demonstrated κ values of 0.77 for GQS, 0.79 for mDISCERN, 0.85 for Treatment Accuracy, 0.83 for Guideline Concordance, and 0.87 for Misinformation, indicating substantial agreement across all measures.
As presented in Table 3 and Figure 4(a) and (b), significant differences in mDISCERN scores were observed among various types of video uploaders. Videos produced by professionals and institutions exhibited higher mDISCERN scores (medians of 2 and 1.5, respectively) compared to those created by individual users (P < 0.0001, P < 0.001, respectively). No significant differences were found between other uploader categories. The median GQS score for individual users was 2.5, while other uploaders had a median score of 3, reflecting a generally moderate to low content quality. The median mDISCERN score of 2 for professional videos suggests a lack of clear sources and evidence-based support, thereby reducing their reliability. Although professionals’ scores were slightly higher, the overall quality remains subpar and insufficient to indicate that their information is inherently more reliable. Comparison of quality, reliability and and accuracy scores between TikTok and Bilibili videos.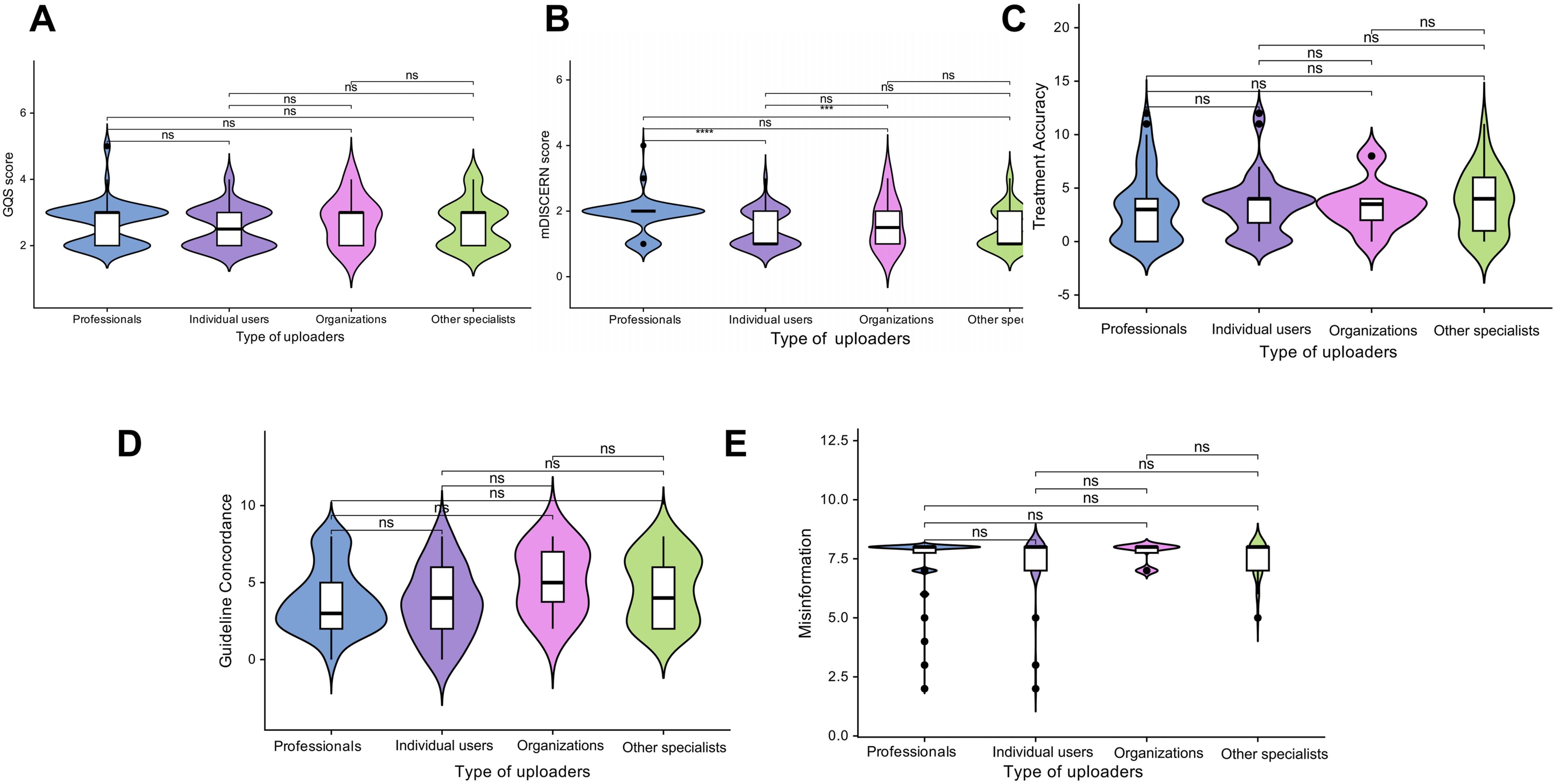
The median content accuracy score for videos uploaded by individual users and other experts was 4, higher than the scores of professionals and institutions, which had medians of 3 and 3.5, respectively. For professionals, the lower quartile was notably low (Q1 = 0.00), indicating a considerable proportion of videos containing critical errors or missing content. In contrast, the interquartile range for other experts was relatively broad (Q1, Q3: 1.00, 6.00), suggesting substantial variability in video quality within this group. In terms of guideline adherence, institutions had a median score of 5, while individual users and other experts both had medians of 4, higher than the score for professionals (median = 3). This suggests that institutional videos generally align with current guidelines, while professional videos tend to exhibit moderate to low quality. Regarding misinformation, the median score for all groups was 8.00, indicating that most videos did not contain significant misinformation. Professionals and institutions showed greater consistency (Q1 = 7.75), remaining in the high-quality range, whereas individual users and other experts exhibited slightly lower lower quartiles (Q1 = 7.00), but still within the high-quality range, reflecting generally reliable content accuracy. No statistically significant differences were found between the groups (P > 0.05). Figure 5 illustrates the overall distribution of GQS, mDISCERN, and content accuracy scores across different types of uploaders. Distribution of quality, reliability and and accuracy scores across different types of uploader groups.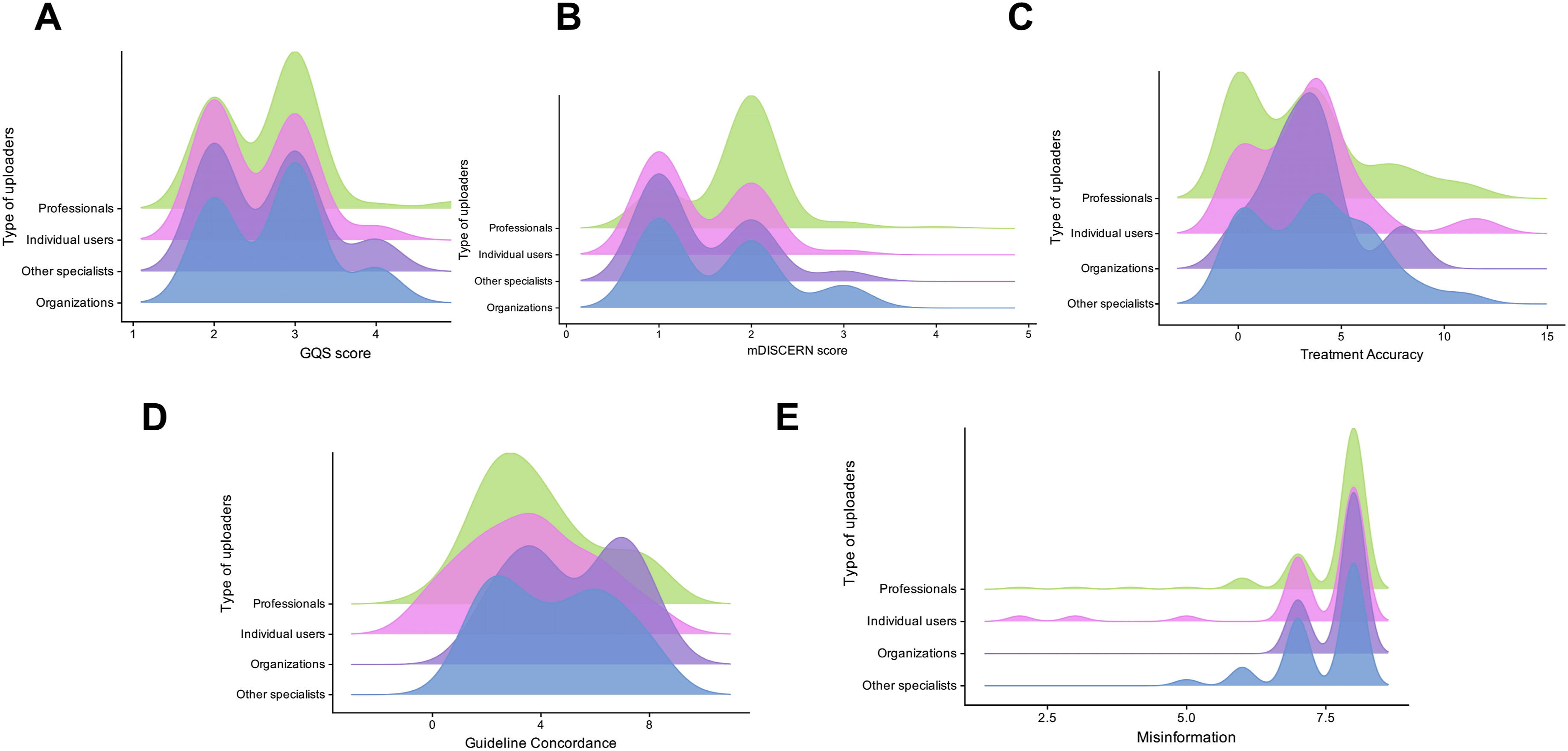
3.5. Association between engagement metrics and information quality, reliability and accuracy
The viewer interaction metrics exhibit strong positive correlations with one another. Specifically, the number of likes shows significant positive correlations with the number of saves (r = 0.84, P < 0.001), comments (r = 0.86, P < 0.001), and shares (r = 0.87, P < 0.001). Similarly, the number of saves, comments, and shares are strongly to very strongly positively correlated with each other (r = 0.72-0.90, P < 0.001). In contrast, the video duration is weakly positively correlated with the number of saves (r = 0.21, P < 0.01), as well as with the global quality score (r = 0.30) and treatment accuracy (r = 0.30), with all p-values below 0.001. However, no significant correlations were found with the number of likes (r = -0.02), comments (r = -0.08), or shares (r = 0.08) (P > 0.05). Additionally, the GQS and mDISCERN scores did not show significant correlations with any of the interaction metrics (r = 0.01-0.11, P > 0.05). Treatment accuracy exhibited a moderate positive correlation with guideline adherence (r = 0.56, P < 0.001), although both variables demonstrated negligible correlations with the interaction metrics (r = 0.00-0.09, P > 0.05). Finally, the misinformation score displayed negligible correlations with all other metrics (r = -0.12 to 0.10, P > 0.05). The correlation coefficients are presented in Figure 6. Correlation matrix of spearman’s correlation analysis between video metrics and quality scores.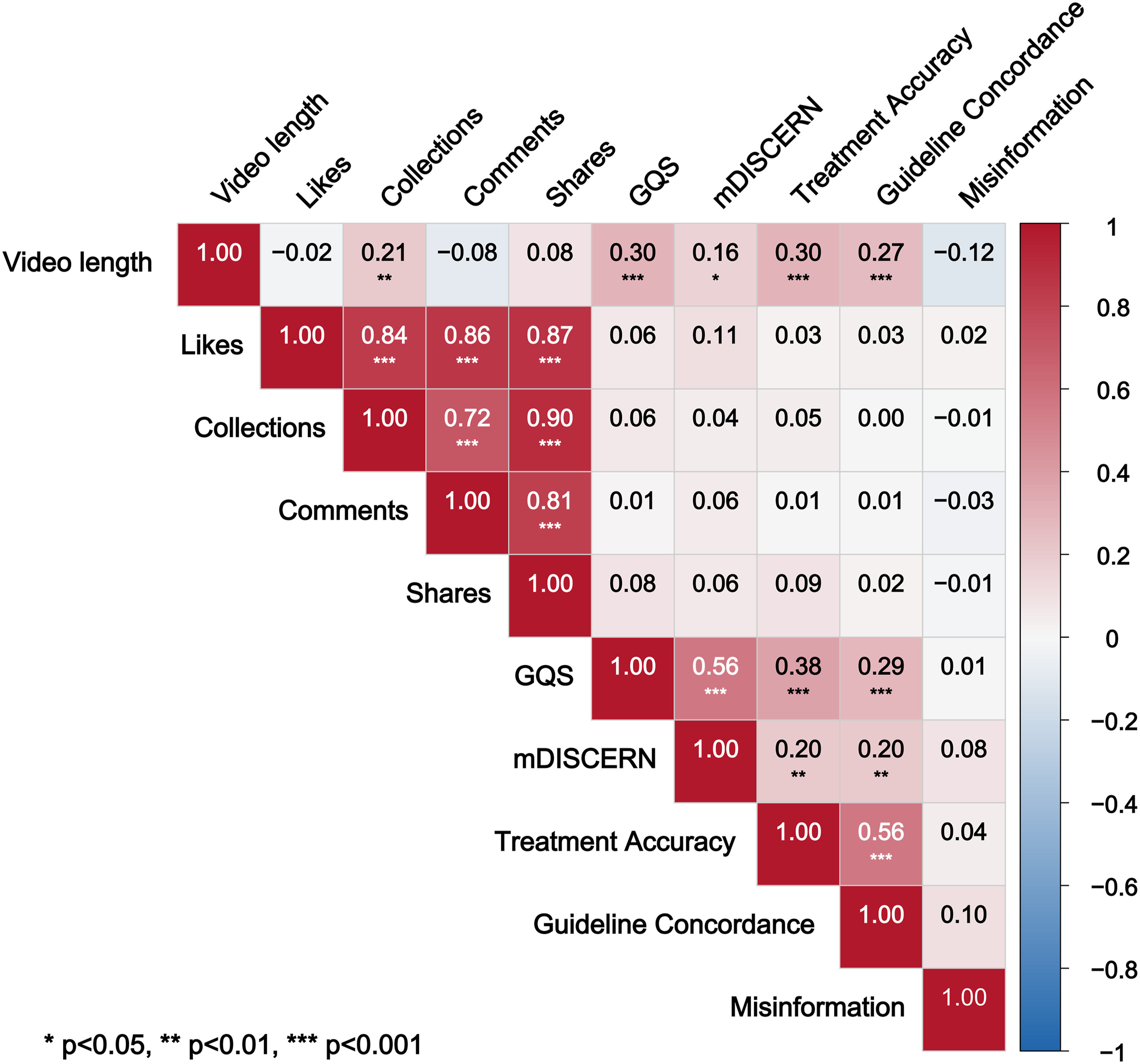
4. Discussion
This study systematically evaluated 199 BPPV-related short videos on TikTok and Bilibili, examining their characteristics, content distribution, quality, reliability, and accuracy. The analysis revealed that the videos predominantly emphasized treatment over prevention, with overall quality and reliability remaining relatively low. While videos uploaded by professionals exhibited slightly higher reliability than those by individual users, both groups demonstrated low reliability, and at least 25% of professional videos contained significant errors, highlighting a gap between professional expertise and effective science communication. Furthermore, no significant relationship was observed between video engagement and information quality, suggesting that high viewership does not necessarily correspond to high educational value. Collectively, these findings provide valuable insights for enhancing the professionalism and comprehensiveness of BPPV health communication on digital platforms and serve as a reference for optimizing quality strategies among healthcare professionals and platform operators.
4.1. Video interaction metrics
Our research shows that BPPV-related videos on TikTok perform exceptionally well in terms of interaction metrics, with users more likely to engage compared to other platforms. This finding aligns with previous studies, 32 suggesting that the short-form nature of TikTok videos plays a significant role. The concise format helps capture users’ attention more effectively, prompting them to like and comment. In contrast, videos on the Bilibili platform tend to be longer, which may impact users’ patience and overall engagement. Therefore, video interactivity is influenced not only by the content’s appeal but also by the specific characteristics of the platform. 35 Correlation analysis revealed a weak positive relationship between video duration and the number of saves, suggesting that although longer videos may garner fewer likes or comments, their greater informational depth prompts users to save them for future reference. Given the nature of BPPV, a condition that requires systematic explanations of diagnostic methods and repositioning techniques, short and long videos likely serve distinct but complementary roles in knowledge dissemination. Short videos are effective in capturing initial attention, while long videos provide a platform for more thorough and detailed knowledge delivery.
4.2. Uploader characteristics
On TikTok, 82% of BPPV-related videos are uploaded by professionals, compared to only 24% on Bilibili. This variation may reflect the distinct certification and review mechanisms for health content creators on the two platforms. Although post hoc pairwise comparisons did not reach statistical significance, the differences in uploader composition between platforms are still evident at a numerical level. In the case of BPPV, a disorder that requires precise repositioning techniques, such differentiation in content producers could have a substantial impact on the accuracy of the information provided. Non-professional creators may be unable to accurately demonstrate critical procedures, such as the Epley maneuver, thus increasing the risk of improper audience self-application. These findings highlight that the content review processes and creator certification standards of platforms are crucial upstream factors influencing the quality of health science information.
4.3. Video content analysis
This study found that BPPV-related videos on TikTok and Bilibili primarily focus on clinical manifestations and treatment, with limited attention given to epidemiological and preventive aspects. Content creators often prioritize topics that evoke emotional resonance or curiosity, which results in the marginalization of more abstract and less engaging discussions on epidemiology and prevention.
Epidemiological data are critical for improving public understanding of BPPV. Insufficient knowledge of epidemiology may lead high-risk populations, such as the elderly, women, and individuals with a history of head trauma, to underestimate their vulnerability, potentially delaying timely medical consultation. Furthermore, the absence of preventive guidance weakens the effectiveness of health communication and limits public awareness of, and access to, preventive services.
Despite the importance of this epidemiological knowledge, BPPV exhibits a high recurrence rate, and most educational videos primarily focus on risk factors, such as vitamin D deficiency, hypertension, and diabetes, while often overlooking practical daily management strategies. Research suggests that vitamin D supplementation may help reduce recurrence risk 36 ; however, further studies are needed to confirm these findings. In terms of daily management, vestibular rehabilitation exercises like the Brandt-Daroff exercises have proven effective in alleviating residual dizziness in patients with recurrent BPPV. 37 Without proper preventive information, patients may underestimate the risk of recurrence, fail to manage underlying conditions properly, and even increase the likelihood of complications, such as otolith displacement, due to improper self-management.
A distinctive feature of BPPV-related content is the critical need for procedural precision. Unlike chronic conditions such as chronic pancreatitis and coronary heart disease, which are primarily managed through medication and long-term self-care,38,39 insufficient operational details in BPPV instructional videos can directly cause physical harm to patients. Therefore, it is essential to integrate preventive guidance and emphasize the risks associated with procedural execution in short videos. Doing so could significantly improve patients’self-management abilities and reduce the healthcare burden linked to recurrence.
4.4. Differences in video quality across uploader types
This study found that GQS scores across different uploader groups were generally moderate to low, with no significant differences between the groups. This raises concerns for BPPV, a condition that relies on precise repositioning techniques, and highlights that a professional background does not guarantee high-quality science communication.
In terms of reliability, professionals’mDISCERN scores were slightly higher than individual users, but both groups scored low overall, indicating that BPPV videos often lack an evidence-based foundation. Accuracy is particularly concerning: the lower quartile of professionals scored extremely low (Q1 = 0.00), meaning at least 25% of videos contained significant errors or omitted crucial information. Examples include videos showing only definitions without repositioning demonstrations, recommending flunarizine inappropriately, misrepresenting vestibular tests, or suggesting practices like “side sleeping” that contradict guidelines. These deficiencies may negatively affect patient care. 40
Such risks include improper techniques leading to abnormal otolith displacement, occurring in up to 8.1%, 16 and complex canal conversions. In elderly patients, incorrect neck rotation may cause severe complications such as vertebral artery dissection. 4 Misconceptions may also delay proper diagnosis and care, with patients averaging 3.4 visits before BPPV diagnosis and often undergoing unnecessary imaging. Poor-quality online content thus poses tangible risks to patient safety and treatment outcomes. 41
4.5. Relationship betweeninteraction metrics and quality and reliability
This study found a significant positive correlation between interaction metrics such as likes, comments, collections, and shares, forming a collaborative interaction cluster, which is consistent with the findings of Huang et al. 42 . However, no correlation was observed between these interaction metrics and the GQS or mDISCERN scores, in line with prior research.43,44 This study highlights a critical issue in health communication on short video platforms. Recommendation algorithms often prioritize videos with high engagement, but these videos are not always accurate or aligned with established guidelines. This gap between high engagement and low quality can foster overconfidence in viewers. Individuals who watch highly liked videos may develop a cognitive bias, assuming that widespread agreement indicates reliability, which can lead to excessive trust in the information presented.
Given that BPPV management relies on precise physical maneuvers, overconfidence may cause patients to mistakenly believe they can perform repositioning techniques correctly and attempt self-treatment. Moreover, they may become less cautious toward misleading claims, such as the view that repositioning is merely an aid, especially when high engagement reduces their skepticism. Over time, patients may continue following advice that contradicts clinical guidelines, including beliefs like side sleeping can prevent BPPV. The primary risk of overconfidence is delayed medical intervention, driven by patients’ strong belief in their own judgment.
This issue is compounded by the fact that these videos rarely contain obvious factual errors. Furthermore, risk information is often presented in a seemingly reasonable manner, making it difficult for viewers to recognize potential hazards. As a result, patients may delay seeking professional medical help, which could lead to worsened outcomes.
In addition to overconfidence, the quality of the videos themselves plays a role in the effectiveness of health communication. A weak positive correlation exists between video length and both GQS and treatment accuracy, suggesting that longer videos may allow for a more systematic explanation of repositioning techniques. However, video length alone does not guarantee quality. Short videos that accurately present key details may provide greater educational value, proving that the focus should be on the clarity and relevance of the information rather than just video duration. 45
4.6. The potential and challenges of social media in health education
While this study highlights several risks associated with short BPPV videos, social media platforms can still serve as a valuable supplement to traditional medical education, particularly when content is developed collaboratively by medical and communication experts. Specifically, platforms could feature vetted videos that teach the recognition of warning symptoms, enabling high-risk individuals to identify issues early and seek prompt medical attention. In addition, professional organizations could produce standardized instructional videos on repositioning techniques, with clear contraindication warnings, to assist patients in home rehabilitation post-diagnosis. Platforms could also collaborate with professional societies to incorporate credible markers on academically reviewed content, which would help users differentiate reliable information from unreliable sources. However, the effectiveness of platforms in fulfilling this role hinges on the professionalism of content design and the credibility of the information sources.
4.7. Limitations
This study has several limitations. First, our research focused only on videos from TikTok and Bilibili, which may limit the generalizability of the findings to other language environments and platforms. Second, sampling bias must be considered. The analysis was restricted to the top 150 search results for each keyword, which are affected by platform ranking algorithms and temporal variations. Consequently, the findings provide only a snapshot of highly visible content and do not constitute a comprehensive survey. Third, this study employed a cross-sectional design, capturing video characteristics at a single time point. Consequently, it cannot account for the dynamic changes in content popularity or user engagement. Fourth, videos longer than 20 minutes were excluded from the study. While this is consistent with the content focus of short video platforms, the weak positive correlation between video length and GQS scores suggests that some in-depth content may have been omitted, which could limit the comprehensiveness of the quality assessment. Finally, although GQS and mDISCERN are widely accepted quality assessment tools, their scoring processes are inherently subjective. The content accuracy checklist used in this study, developed by the research team and based on current clinical guidelines, may still introduce evaluator bias. Future studies should develop specialized assessment tools for vestibular disorder educational videos and incorporate multiple independent evaluators with consistency testing to reduce subjective bias.
5. Conclusion
This cross-sectional study evaluated short videos on TikTok and Bilibili related to BPPV, revealing significant gaps in content related to epidemiology and prevention. The videos' overall quality, reliability, and accuracy were suboptimal. Videos uploaded by professionals were found to be more reliable than those by individual users, although they still lacked evidence-based information and key details. Video duration showed a weak positive correlation with quality, while engagement metrics did not reliably reflect the credibility of the information. As an exploratory analysis, this study offers preliminary evidence regarding the dissemination of BPPV-related health information on social media. Future prospective research is needed to assess the clinical impact of such content on the timeliness of diagnosis, the success rate of repositioning maneuvers, and the recurrence of BPPV.
Supplemental material
Supplemental material for - Analysis of the quality and reliability of benign paroxysmal positional vertigo-related short videos on TikTok and Bilibili: A cross-sectional study
Supplemental material for Analysis of the quality and reliability of benign paroxysmal positional vertigo-related short videos on TikTok and Bilibili: A cross-sectional study by Chunping Zheng, Lijuan Tang, Chunbo Wu, Luan Huang, Runjun Luo in Digital Health.
Footnotes
Author note
Submitted for review and possible publication in Digital Health.
Acknowledgements
All authors have put a lot of effort into this study, and we are very grateful to all the authors.
Ethical considerations
This study did not involve human participants, clinical data, experimental animals, or histological investigations. All data analyzed in this study were obtained from publicly available Tiktok and Bilibili videos, and the data collection process fully complied with the Terms of Service of Tiktok and Bilibili. No private information or personally identifiable information was collected or processed, and no interaction of any kind was conducted with platform users. The use of these data did not require individual informed consent. Therefore, this study did not require formal ethical approval.
Author contributions
CZ: Conceptualisation, methodology, software,validation, formal analysis, investigation, resources, data curation, writing - original draft, writing - review and editing, visualisation, project administration. LT: Validation, formal analysis, investigation, resources, writing - original draft, visualisation. CW: Writing - review and editing, language editing. CZ, CW: Formal analysis, writing - review and editing. LT, LH: writing - review and editing, Supervision. LH, CW: Conceptualisation, methodology, writing - review and editing, supervision. RL: Conceptualisation, methodology, writing - review and editing, supervision, project administration. All authors read and approved the final version of the manuscript. Runjun Luo is the guarantor and takes responsibility for the overall content of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Patient and public involvement
Patients and/or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Guarantor
RJL.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.