
Abstract
Objective
Chronic diseases have become a major public health burden globally, and online health information seeking behavior (OHISB) has emerged as a potential tool for improving health literacy and protecting individuals from chronic diseases. Nevertheless, previous studies have shown that OHISB may exacerbate health disparities, and its specific association with chronic disease prevalence remains unclear. This study aims to investigate the relationships between OHISB, chronic disease literacy, and chronic disease prevalence, with a focus on sociodemographic heterogeneity.
Methods
A cross-sectional questionnaire survey was conducted in China, from June to September 2024. Partial correlation analysis and restricted cubic spline (RCS) regression were used to analyze the specific relationships among OHISB engagement, chronic disease literacy and prevalence. Stratified interaction analyses were performed to explore the heterogeneous effects of OHISB across distinct sociodemographic subgroups.
Results
OHISB was positively associated with chronic disease literacy (r = 0.218, P < 0.001), The RCS model revealed a significant nonlinear relationship between OHISB and chronic disease literacy (P nonlinear < 0.001), characterized by an initial significant increase followed by a plateau. Significant interaction effects of OHISB and sociodemographic factors were observed (P interaction < 0.001), OHISB conferred more benefits on vulnerable subgroups, including those aged ≥45, suburban residents, non-college graduates, and low-consumption individuals (≤¥3,000/month). Conversely, while the RCS plot revealed a descriptive risk convergence trend, no significant association was found between OHISB and chronic disease prevalence (r = -0.005, P = 0.855).
Conclusion
OHISB was positively associated with chronic disease literacy, although its benefits were limited by a ceiling effect. Moreover, it was also associated with the narrowing of sociodemographic gaps in chronic disease literacy. However, we did not observe a significant link between OHISB and chronic disease prevalence. Therefore, targeted digital interventions are essential to bridge the knowledge-behavior gap and promote chronic disease prevention among vulnerable populations.
Keywords
Introduction
Chronic diseases have emerged as a significant public health concern and leading cause of mortality worldwide, driven by demographic and environmental shifts. 1 As lifestyle-related diseases, seeking health information and improving health literacy are economical and effective measures for prevention.2,3 In recent decades, with the proliferation of Internet technology, seeking health information online has gained popularity.4,5 According to the Eurostat, around 52% of individuals searched health information online in 2022 and this proportion is still growing. 6 In China, researchers recorded 78.19% of adults sought medical information online, 7 and with the digitally down to the countryside, 47.27% of residents in suburban and remote regions obtained health-related information through the internet. 8
Online health information seeking behavior (OHISB) involves individuals’ retrieval of health information from the Internet for the purpose of obtaining health knowledge and facilitating decision making. 9 Previous studies have noted that using online health information was crucial for promoting health literacy , 10 as it could improve users’ health knowledge, and increase confidence in managing health condition. 11 Moreover, people who are engaged in seeking online health information are more likely to protect themselves from chronic disease. 12 Studies conducted in Poland 13 and China 14 have widely confirmed that online health information facilitates healthy lifestyles and preventative health behaviors. 15 For chronic disease patients, online health information also helps them better adhere to treatment 16 and adopt chronic disease self-management behaviors. In brief, adequate online health information may enhance chronic disease literacy and facilitate the prevention of chronic diseases.
Despite the potential benefits of OHISB, researchers also warned that the increasing reliance on the Internet to seek health information may intensify health inequalities. 17 Vulnerable groups lack the skills to effectively utilize or critically evaluate the content. 18 In particular, rural residents, 19 immigrants or ethnic minorities, 20 elderly individuals with lower education levels, 21 and populations in developing countries 22 are typically at a disadvantage in utilizing online health information. Nevertheless, Existing evidence from America, 23 Saudi Arabia, 24 France, 25 China 26 and other countries has extensively indicated that chronic diseases were more common in these vulnerable groups.
Therefore, it remains a question that whether the OHISB has widened or narrowed the health disparities. Moreover, despite the ample evidence supporting its contribution to health literacy and chronic disease prevention, their specific relationship remains unclear. There is a pressing need not only to identify how online health information shape chronic disease literacy and outcomes, but also evaluate how OHISB influence health equity.
To address this gap, we conducted a questionnaire survey in Shanghai, China, and leveraged partial correlation analysis and restricted cubic spline (RCS) models to analyze the specific relationships among OHISB engagement, chronic disease literacy, and chronic disease prevalence. Furthermore, with a focus on sociodemographic-based disparities, we performed stratified interaction analyses to explore the heterogeneous effects of OHISB. The findings provide actionable evidence to design targeted online health information interventions, offering a feasible pathway to narrow health disparities, particularly in protecting vulnerable populations from chronic diseases.
Methods
Study design
From June to September 2024, a cross-sectional survey was conducted in Shanghai, China. The sample size was calculated using the following formula:
Geographically, Shanghai is divided into three regions: urban core, inner suburb, and outer suburb. Our survey adopted a 3-stage sampling method that first randomly selected 1 to 2 districts from each region and then randomly selected 3 to 5 communities from each district according to the population ratio to complete the survey. Researchers obtained approval from community administrators. Finally, local staff assisted in recruiting and training 2-5 research assistants per community for standardized data collection. They collected questionnaires through community residents’ WeChat groups and home visits. The survey’s cover page presented the study’s objectives and procedures, and participants were required to confirm their voluntary participation before accessing the survey questions. Online questionnaire was completed through an online survey platform (‘SurveyStar’, Changsha Ranxing Science and Technology, Shanghai, China). Our study finally included 1608 residents, and all questionnaire data were anonymized with strict confidentiality protocols. The questionnaires in English and original language (Chinese) were included in Multimedia Appendix 2.
Study population
This survey targeted adults aged 18 years and older who had resided in Shanghai, China, for more than six months. In recent years, China has been confronted with increasingly severe problems of declining birth rates and an aging population, 28 which has exacerbated the severity of the chronic disease challenge. Shanghai is a large city with the highest degree of aging in China, which lead to the epidemic of chronic diseases.29,30 The detection rate of chronic diseases among older adults (≥60 years old) in Shanghai has reached 70%. 31 Meanwhile, it has well-developed Internet infrastructure and healthcare system. Thus, Shanghai serves as an ideal empirical context for exploring the relationship between OHISB and chronic diseases, while offering actionable insights for regions undergoing similar socioeconomic and demographic transitions.
Measurements
OHISB engagement
OHISB engagement was measured through three self-reported items based on existing literature32,33: “I frequently seek health information online”, “When I have health problems, I will actively search for relevant health information online” and “I continuously follow the health information that interests me online”. The participants responded to these 3 items on a 5-point Likert scale ranging from “1 = totally disagree” to “5 = totally agree”. The total score of this scale varies between 3and 15, with higher scores indicating a more active and frequent seeking for online health information. The scale showed acceptable reliability and validity (Cronbach α=0.711, KMO=0.71).
Chronic disease literacy
Chronic disease literacy was assessed using the National Resident Health Literacy Questionnaire (2016 version). This is the officially certified health literacy assessment instrument established by China’s National Health Commission, which has been validated (Cronbach α=0.891) 34 and was used for annual health literacy surveys across China. This scale comprises six core aspects, and we selected the chronic disease dimension, which includes nutritional knowledge, mental health, hypertension prevention, tobacco control, tumor prevention, scientific exercise, weight management, and chronic disease treatment. The literacy scores ranged from 0 to 12, where a higher score signified better literacy.
Chronic disease prevalence
The participants self-reported whether they had ever been diagnosed with at least one chronic disease. It was recorded as a binary variable (Yes/No).
Sociodemographic characteristics
We collected participants’ sociodemographic characteristics, which included sex, age, residential area, education level, and monthly consumption.
Statistical analysis
In this study, we first conducted descriptive analyses, univariate analyses and partial correlations for chronic disease literacy and prevalence. Continuous data are shown using mean and SDs, whereas categorical variables were reported as frequencies and percentages. The differences in chronic disease literacy between sex (female, male) and residence types (urban, suburban which including inner suburb and outer suburb) were examined using the Student’s t-test, while the Analysis of Variance was used for comparisons across various age groups, educational levels, and category monthly consumption. Differences in chronic disease prevalence were examined using the Chi-squared test. Partial correlations were examined between OHISB engagement and chronic disease literacy, as well as between OHISB engagement and chronic disease prevalence, while controlling for age, sex, education, residence and monthly consumption.
We further explored the shape of the relationship between OHISB engagement and chronic disease literacy using the RCS regression with 3 knots based on the minimum Akaike Information Criterion (AIC). Two-stage least squares (2SLS) instrumental variable (IV) approach was used for endogeneity test.
In addition, we conducted stratified RCS analyses for sociodemographic characteristics, including age (categorized as 18-44years/≥45 years, on the basis of the median), residential area (urban/suburban), monthly consumption (≤¥3,000/¥3,001 or more), and education level was categorized into whether participants had received tertiary education; those who selected “college” or “postgraduate” were classified as “Yes,” while others were classified as “No”. Sensitivity analyses were performed to assess the robustness of the relationship between OHISB and chronic disease literacy.
The main statistical analyses were conducted with R v4.2.3 (R Foundation) using the rms package for RCS, and the endogeneity tests were conducted with Python v3.12.13. P values <0.05 (2-sided) were considered as statistically significant.
Results
Preliminary analysis
Sociodemographic characteristics, chronic disease literacy and the prevalence of chronic disease (N=1608).

There were marked differences in the chronic disease literacy and prevalence among the participants. The average chronic disease literacy score was 8.74±2.79. As detailed in Table 1, participants those aged 30-39 years (9.79±2.26), with urban residence (8.86±2.71), postgraduate education (10.59±1.52), and monthly consumption over ¥4001 (9.28±2.56) had higher literacy scores. Notably, the scores significantly decreased between the 40-49 age group and the 50-59 age group.
Nearly half of the participants reported at least one chronic disease diagnosis (46.70%). The prevalence of chronic disease was significantly higher among those aged over 80 years (93.5%), urban residents (49.10%), and with less than high school education (70.70%). Similarly, the prevalence in the 50-59 age group increased significantly and was 26.41% higher than that in the 40-49 age group. However, we did not observe significant differences in sex or monthly consumption (Table 1).
Association of OHISB engagement with chronic disease literacy
The average score of OHISB engagement was (10.02 ± 2.83) for all participants. Table S1 in the Multimedia Appendix 1 contains detailed descriptive statistics of OHISB across groups. A partial correlation revealed a significant association between OHISB and chronic disease literacy (r = 0.218, P < 0.001).
Moreover, the RCSs were fitted to evaluate the nonlinear patterns between OHISB engagement and chronic disease literacy. The nonlinear model was statistically significant (L.R.χ
2
= 218.28, P < 0.001, Pnonlinear <0.001). As presented in Figure 1, the plot indicated an initial significant increase followed by a plateau. Specifically, in the OHISB score ranged from 3 to 10, there was a remarkably increase in literacy (Effect =3.36, 95%CI: 2.74,3.97), but in the OHISB score ranged from 10 to 15, this growth had significantly slowed down (Effect = 0.55, 95%CI: -0.03, 1.13). RCS curves illustrating the nonlinear frequency–response between OHISB engagement and chronic disease literacy.
Endogeneity tests.

***p < 0.01, ** p < 0.05, * p < 0.10. OLS uses HC1 robust standard errors. 2SLS standard errors corrected for two-stage procedure.
Furthermore, for those factors (age, residential area, education and monthly consumption) significantly associated with chronic disease literacy, we assessed effect modification by OHISB engagement using stratification and cross-product terms. Significant interaction effects were observed between OHISB and all sociodemographic factors (P
interaction
< 0.001). The interaction plots could be found in Figure 2. Interaction effects between age, residential area, education, monthly consumption and OHISB engagement on chronic disease literacy: stratified RCS curves.
As shown in Figure 2(a), the gap in literacy between the younger (18-44 years) and older (≥45 years) groups were substantial at low OHISB engagement levels but narrowed with increasing OHISB engagement. The absolute predicted difference was 2.78 at lowest OHISB level (score 3) but decreased to 0.42 at highest level (score 15). In terms of residential area, suburban residents presented greater literacy gains than urban residents, ultimately surpassing urban residents (2.08 to -0.71, Figure 2(b)). Similarly, participants without tertiary education showed greater responsiveness to OHISB, with diminishing literacy disparities as OHISB increased (2.98 to 0.80, Figure 2(c)). In line with the above findings, Figure 2(d) suggested the narrowing disparity between two monthly consumption group (1.23 to -0.30) as OHISB levels rising.
Association of OHISB with chronic diseases prevalence
Partial correlation revealed that the association between OHISB and chronic disease prevalence was not statistically significant (r = -0.005, P =0.855). And the association between chronic disease literacy and prevalence was also not statistically significant (r = -0.007, P =0.774).
Our study explored the interaction effects of OHISB and demographic characteristics (age, residential area, education and monthly consumption) on chronic diseases prevalence. The interaction RCS curve plots were presented in Figure 3. Conversely, we did not find evidence of interaction effects between age group, residential area, tertiary education and OHISB engagement in relation to chronic disease prevalence (P all > 0.05). Although the interaction effects did not reach statistical significance, a descriptive trend observed in Figure 3(a), (b) and (c) suggested that the absolute differences in predicted OR of chronic diseases prevalence narrowed slightly as OHISB levels increased. Notably, Figure 3(d) showed statistically significant interaction effects between monthly consumption and OHISB engagement on chronic disease prevalence (P
interaction
<0.001). High OHISB level neutralized the health risks associated with lower consumption levels. The absolute difference in predicted OR shifted from 2.80 (score 3) to -0.20 (score 5), indicating that the risk gap was effectively closed. Interaction effects between age, residential area, education, monthly consumption and OHISB engagement on chronic diseases prevalence: stratified RCS curves.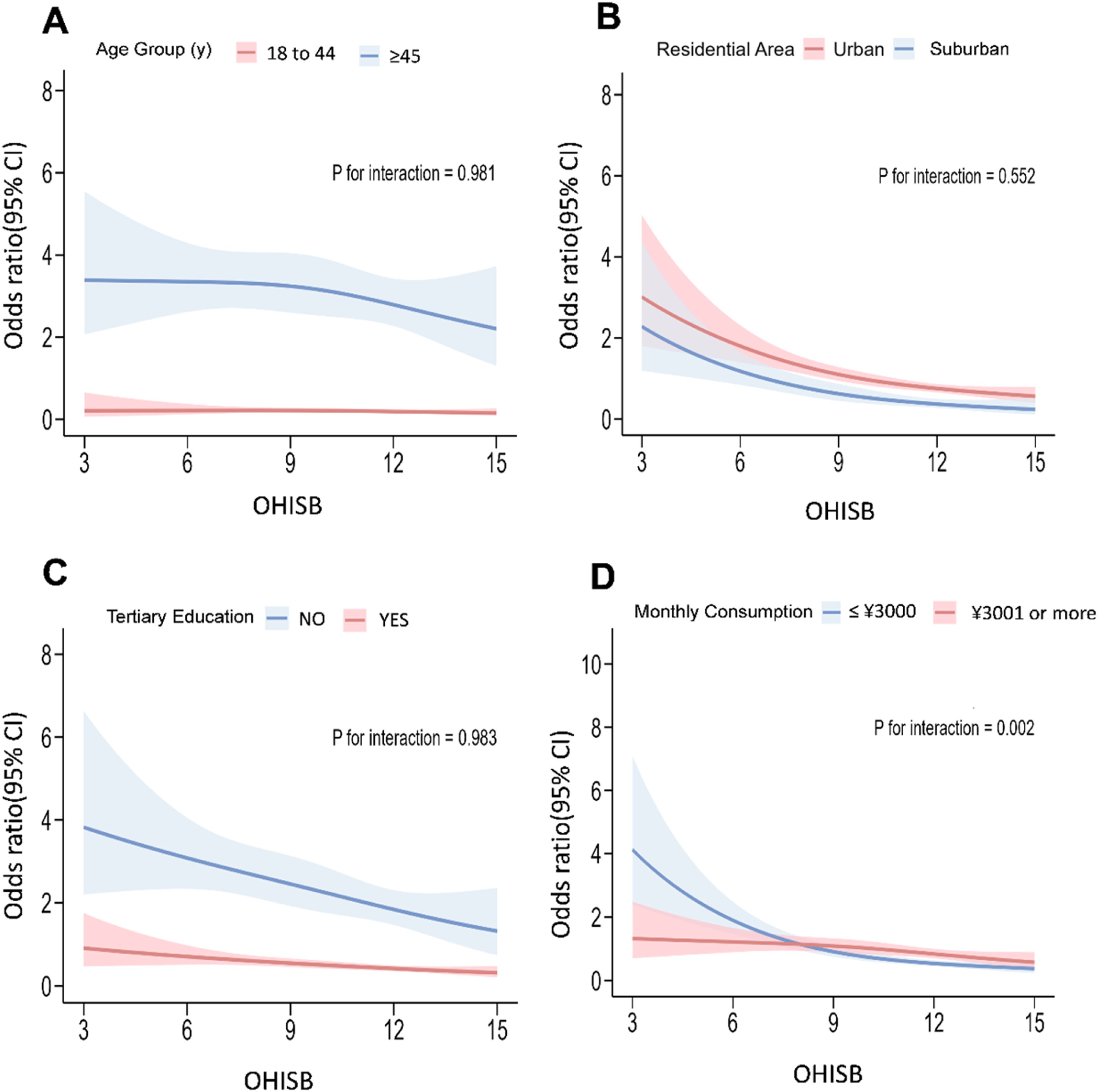
Sensitivity analyses
Our findings were also stable under sensitivity analyses and did not materially change our results (Figure S1, Multimedia Appendix 1). We defined low chronic disease literacy as a score of less than 80% of the total score and high health literacy as a score of more than 80% of the total score according to Chinese national criteria. Logistic regression analysis revealed a significant positive association between chronic disease literacy and OHISB. Furthermore, subgroup analysis revealed that the effect of OHISB engagement was stronger in participants aged ≥45 years, those living in suburban areas, without tertiary education, and monthly consumption ≤¥3,000.
Discussion
Principal findings
Although numerous studies have examined the factors influencing OHISB, chronic disease literacy, and chronic disease prevalence,3,5,23 the complex interrelationships among these variables remain poorly understood. Our study explored the effects of OHISB on chronic disease literacy and prevalence among Chinese adults. We found that (1) participants’ chronic disease literacy and prevalence varied across different demographic groups; (2) OHISB had a positive but limited effect on chronic disease literacy; and (3) age-based, residence-based, education-based and consumption-based literacy disparities significantly narrowed with increasing OHISB engagement. Conversely, we did not observe a significant overall association between OHISB engagement and the chronic disease prevalence, and the association between chronic disease literacy and prevalence was also not significant.
Social divides influencing chronic disease literacy and prevalence
Above all, our results revealed how Chinese residents’ sociodemographic backgrounds were manifested in individuals’ varying levels of chronic disease literacy and prevalence. Consistent with previous research,35,36 significant disparities in health literacy and chronic disease prevalence were closely tied to sociodemographic factors, including age, residential area, education, and economic status. 226,37
Our results revealed that urban residents, younger and well-educated individuals tend to have higher chronic disease literacy and a lower prevalence of chronic diseases. This chronic disease-related social divide is prevalent worldwide, 38 and a primary explanation is that vulnerable groups tend to face inferior healthcare services, living environments, and the ability to distinguish information, as well as greater psychological stress.39,40 Notably, we observed a significant decline in chronic disease literacy among the 50–59 age group, concurrent with a substantial increase in the prevalence of chronic diseases. Chinese residents generally retire between the ages of 50 and 60, 41 and retirement may lead to various challenges, such as decreases in social interaction 42 and cognitive function, 43 which may ultimately affect their health status. 44
OHISB positively related to chronic disease literacy with a ceiling effect
Our study also highlighted that OHISB positively related to chronic disease literacy, in line with previous studies.10,11 Nevertheless, this relationship exhibited a nonlinear pattern, while initial engagement in OHISB leads to rapid improvements in chronic disease literacy, continued searching eventually yields diminishing returns, and literacy scores begin to plateau. With regard to similar phenomena, Ettema and Kline 45 reported the existence of the so-called ceiling effect: an individual’s pursuit of specific knowledge is not endless, after reaching a certain upper limit, the increase in the amount of knowledge gradually decelerates or even stops, reaching a ceiling. While prior studies have not explicitly explored the ceiling effect from a health literacy perspective, our findings confirmed the ceiling effect in the Chinese context and health communication filed. Despite appropriate amounts of health information prove beneficial, overload health information might lead to health misperceptions 46 and health anxiety. 47 This has been characterized as a U-shaped relationship between informational provision and health anxiety. 48 Additionally, neurocognitive studies have shown that brain activation levels decrease significantly under information overload. 49
The ceiling effect of OHISB engagement calls for recalibrating digital health campaigns. Public health agencies could adopt a tiered engagement framework, prioritizing foundational health information for low-engagement users, while reducing low-quality, duplicative health information to avoid information overload for high-engagement users.50,51
OHISB narrowing the social divides in chronic disease literacy
Another important finding of our study was that the OHISB may linked to the narrowing of existing social divides in chronic disease literacy. Existing studies have noted that health literacy is consistently lower among vulnerable populations.52,53 Notably, we identified significant interaction effects, showing that the positive association between OHISB and chronic disease literacy is particularly pronounced for vulnerable groups, such as older adults, suburban residents, and individuals with low consumption and education level.
This finding make a significant contribution to the literature on the digital divide. There have been debates about whether the Internet use could reduce health inequalities based on socioeconomic status. Previous research has shown that vulnerable groups derive relatively fewer benefits from the Internet due to the digital divide. 54 These groups typically exhibit lower levels of e-health literacy,55,56 which limits their capacity to understand and apply health information, increasing their susceptibility to misleading or inaccurate health content. 57
Nevertheless, our observations emphasize that OHISB demonstrated increased benefits among socioeconomically vulnerable groups. One potential explanation is the expansion of internet infrastructure in recent years, particularly in rural and underserved regions, which has enhanced OHISB among vulnerable groups. 58 Another potential explanation may be ceiling effect, 11 while vulnerable groups have greater room for growth in health literacy.
Challenges in translating OHISB-related gains to health outcomes
Despite the association between OHISB and improvements in chronic disease literacy, our study revealed no direct association between OHISB engagement and chronic disease prevalence, nor was a direct association found between literacy and prevalence. The knowledge‒behavior gap may explain the result, 59 which posits that individuals’ health practices are influenced not only by their knowledge but also by their attitudes, so having health knowledge does not always translate into health behaviors and health outcomes. 60
Previous studies have noted that vulnerable groups face more objective barriers to behavioral change, such as limited access to healthcare services, financial constraints, and inadequate social support, 61 which in turn impedes the role of health literacy in improving health outcomes. Research on South and Southeast Asian refugee women indicated that while health education programs could positively influence health outcomes, the group continued to face severe health challenges due to limited healthcare access and unmet clinical needs. 62 OHISB may not overcome the complex socioeconomic and environmental factors that are strong determinants of chronic disease prevalence. Moreover, chronic diseases often develop over decades, 63 making it difficult to detect short-term effects of health information interventions.
When it comes to the impact of OHISB on social disparities in chronic disease prevalence, although only monthly consumption exhibited a significant interaction with OHISB, the RCS plot revealed a risk convergence trend. It indicates that promoting digital health engagement could be a potential intervention for health equity. 64 However, to fully bridge the knowledge-behavior gap, digital interventions must be integrated with policy efforts that address the objective barriers, such as financial constraints and healthcare accessibility. 65
Limitations
This study has several limitations. First, the cross-sectional design inhibits causal inference, and failed to reflect how the gradual accumulation of OHISB into health outcome over time. Second, data obtained from participants rely on self-reported responses that could be biased. Third, this study employed chronic disease prevalence as the primary health outcome, without incidence or control, thereby failing to evaluate whether OHISB could improve clinical indicators among chronic disease patient. Future research can adopt longitudinal approaches to explore the dynamic indicators, such as incidence rates and standardized control metrics to provide a more comprehensive evaluation of OHISB’s impacts on chronic disease.
Conclusions
This study provided a critical perspective on the role of online health information seeking in promoting chronic disease literacy in a major Chinese metropolis. We found that OHISB was strongly associated with chronic disease literacy, while the benefits it confers are subject to a ceiling effect. Furthermore, the benefits of OHISB are particularly pronounced among socioeconomically vulnerable groups, but this increased knowledge does not lead to a lower prevalence of chronic disease directly. Our results suggested that online health information should be tailored to the vulnerable populations, as they stand to derive the greater benefits from OHISB. In addition, this study highlighted the knowledge‒behavior gap in chronic disease prevention. While the internet showed significant associations with indicators of health equity, its full potential may be unlocked if we bridge this gap.
Supplemental material
Supplemental material - Associations of Online Health Information Seeking Behavior (OHISB) with chronic disease literacy and prevalence among adults in Shanghai, China
Supplemental material for Associations of Online Health Information Seeking Behavior (OHISB) with chronic disease literacy and prevalence among adults in Shanghai, China by Yanli Shen, Zhuojun Ye, Shulei Fan, Xiao Jiang, Huiyun Yuan in Digital Health.
Supplemental material
Supplemental material - Associations of Online Health Information Seeking Behavior (OHISB) with chronic disease literacy and prevalence among adults in Shanghai, China
Supplemental material for Associations of Online Health Information Seeking Behavior (OHISB) with chronic disease literacy and prevalence among adults in Shanghai, China by Yanli Shen, Zhuojun Ye, Shulei Fan, Xiao Jiang, Huiyun Yuan in Digital Health.
Footnotes
Ethical considerations
The study protocol received ethical clearance from the Ethics Committee of Renji Hospital, Shanghai Jiao Tong University School of Medicine (Approval No.: KY2024-072-C). The survey data were anonymous, and the answers were protected by privacy laws.
Consent to participate
All participants provided informed consent and participated in the study voluntarily.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Shanghai Municipal Government Decision-making Consultation Project (Grant ID: 2022-S-08).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available for data protection reasons. However, materials and instruments are available from the corresponding author upon reasonable request.
Declaration of AI
AI tools were used solely for language polishing and translation to improve readability, and the final manuscript were reviewed and revised by the authors. Authors maintain ultimate accountability for the scientific integrity of the work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.