
Abstract
Background
The media play an important role in health promotion and disease prevention, while at the same time, a variety of mixed health messages in the media are beginning to pose new challenges to them. However, there is a lack of media health literacy (MHL) assessment tools in China. Therefore, the purpose of this study was to translate the Media Health Literacy (MeHLit) questionnaire into Chinese and to assess its psychometric properties.
Methods
This cross-sectional study was conducted from October to December 2022, and a methodological study of the translation and validation of the MeHLit questionnaire was conducted.
Results
As a result of an extensive translation and cultural adaptation process, the final MeHLit questionnaire was developed, which includes five dimensions and 21 items. Cronbach's α value of the questionnaire was 0.859, and Cronbach's α value of the dimensions ranged from 0.776 to 0.911, which is fairly good. As a result, the test–retest reliability coefficient and the split-half reliability coefficient of the questionnaire are both equal to 0.907. Its content validity index was 0.946, suggesting a reasonable level of content validity. Through exploratory factor analysis, a five-factor structure was identified based on the eigenvalues, total variance explained, and scree plot. As a result of the validation factor analysis, all recommended fit indicators were appropriate.
Conclusion
The Chinese version of the MeHLit questionnaire has been successfully introduced in China. It has shown good psychometric properties among the Chinese public and can be used as a tool to evaluate MHL in health screening.
Introduction
The media assumes a critical role in health promotion and disease prevention.1–3 In an increasingly media-saturated and digital environment, the media is increasingly used to disseminate important public health information efficiently.4–6 Researches show that the media influence public perceptions, attitudes, and behaviors on health issues by conveying information.7,8 The concept of media literacy originated in the 1930s as a means of thinking critically about media content and is typically defined as the ability to access, analyze, and generate media messages.9,10 The advent and growth of Internet media, particularly social media platforms such as WeChat, Weibo, QQ, and TikTok in China, have underscored the significance of media literacy. This is largely because the quality of information disseminated through these platforms is not guaranteed, there may be an overload of misinformation that lacks scientific basis and is oversimplified, and people with low levels of media literacy are easily misled by the “echo chamber effect.”11–13 The “echo chamber effect” is a sociopsychological phenomenon frequently encountered in the realm of media and communication studies. Inside this echo chamber, users are predominantly exposed to one-sided views that resonate with their own, while dissenting voices are filtered out. 14 This phenomenon of information homogenization can exacerbate confirmation bias, distort reality perception, and polarize viewpoints. 15 It also poses a potential threat to societal cohesion, given its association with the surge of misinformation and “fake news.”16,17 When an echo chamber is filled with false or misleading information, it tends to be propagated and accepted without critical scrutiny.18,19 This particularly poses a risk for individuals with low media literacy levels, as they are less equipped to distinguish between reliable and misleading information, making them prone to manipulation. Conversely, a good level of media literacy facilitates critical evaluation and accurate interpretation of media information, thereby fostering critical thinking and creativity.20–22 In the COVID-19 pandemic, media literacy can help respond to information epidemics for more reliable information, and public media literacy has become more important than ever at this time. 23
In 1998, the World Health Organization defined health literacy as “the cognitive and social skills that determine an individual's motivation and ability to acquire, understand, and use information in ways that promote and maintain health.” 24 With the emergence of the big data era, media literacy's relevance to health literacy has grown, particularly as media sources become primary resources for health information. 25 Media literacy education (MLE), focusing on helping people increase their ability to think critically, has been shown with positive effects on many health behaviors.21,26,27 Through MLE, citizens improve their cognitive ability to identify rumors in a social media environment,28,29 promote and develop the ability to correctly interpret and manage media messages,30,31 search for health promotion and disease prevention information,32,33 and identify symptom onset and disease progression efficiently. 34
Media literacy and health literacy have different conceptual assumptions. While health information typically originates from health systems, mass media content can be implicit and may promote or harm health.35–38 Thus, neither health literacy nor media literacy provides a comprehensive explanation of how individuals learn and utilize health information in a media-dominated environment. There are currently a variety of subcategories of health literacy definitions derived from the concept of health literacy, such as child health literacy and e-health literacy definitions.39,40 In 2011, Levin-Zamir et al. expanded upon the integration of health literacy and media literacy concepts to conceptualize media health literacy (MHL). 41 This concept diverges from the conventional health guidance model as it takes into account both explicit and implicit mass media content, usually generated by commercial entities or health systems, which could influence an individual's health either positively or negatively. 42
The global spread of COVID-19 led to an explosion of rumors, myths, false news, and health misinformation on social media platforms, spreading faster than the virus itself and significantly impacting national policies and social order in the fight against the pandemic.43–46 At the 2020 Munich Security Conference, WHO Director–General Tedros Adhanom Ghebreyesus asserted, “We’re not just fighting an epidemic; we’re fighting an infodemic.” 47 Studies have proven that mass media and online opinion leaders play an important role in crisis communication.48–51 It is anticipated that digital and media tools will increasingly be used at the global level to deliver health messages, provide health information, and navigate health systems.52–54 MHL plays an increasingly important role in this shift.
Recognizing the importance of this issue and the urgency of improving public MHL, Nazarnia et al. developed and validated the MeHLit questionnaire, a tool designed to assess MHL. 55 The MeHLit questionnaire is divided into five dimensions, contains 21 items, explains 60.25% of the total variance, and has satisfactory reliability and validity. 55 To the best of our knowledge, the Chinese version of the MeHLit questionnaire has not been developed yet. Therefore, this study aims to introduce the MeHLit questionnaire into China and measure its psychometric properties through translation and cultural adaptation. We proposed the following hypothesis: the Chinese version of the MeHLit questionnaire has satisfactory psychometric properties.
Method
Participants
Using a cross-sectional study design, we assessed the validity and reliability of the Chinese version of the questionnaire to evaluate MHL, also known as MeHLit. The study employed a convenience sampling methodology, predominantly recruiting participants through online social networks. We developed an electronic questionnaire using Wenjuanxing (http://www.wjx.cn), a free online questionnaire platform in mainland China that provides the equivalent of Amazon Mechanical Turk. After unified training of survey staff, questionnaires were distributed through social platforms such as WeChat, QQ, and Weibo. Potential participants were provided with an explanation of the study's purpose and invited to complete the questionnaire. We set the permission to fill out the questionnaire so that each IP address could only be filled out and submitted once to prevent duplicate submissions. The data collection was conducted from October to December 2022. In order to conduct factor analysis, the sample size was determined based on general guidelines. These guidelines are at least 10 participants per item, with a 20% missing rate if the questionnaire is incomplete. 56 The translation questionnaire in our study consisted of 21 items, and it was necessary to have a minimum of 252 participants, but a large sample was necessary to gather accurate results. We finally recruited 514 adults (for item analysis) and 686 adults (for psychometric evaluation) based on the available conditions. Inclusion criteria were Chinese, age ≥18 years, access to smartphones and social networking sites, and willingness to participate in the survey. Participants who did not complete the participation survey were not included in the final sample. The study was voluntary, and all eligible participants had the option to withdraw at any time. The survey was conducted using a web-based anonymous questionnaire, and the personal details of participants were kept confidential. The study was approved by the Ethics Committee of Jinzhou Medical University.
Design
A methodological study with three phases: (a) translation and cross-cultural adaptation of the questionnaire; (b) item analysis of the questionnaire (n = 514); and (c) evaluation of psychometric properties of the questionnaire (n = 686). In addition, the samples involved in the third phase were randomly divided into two groups, one for exploratory factor analysis (EFA, n = 343) and the other for confirmatory factor analysis (CFA, n = 343). The flowchart is shown in Figure 1.

The development procedure of the Chinese version of the Media Health Literacy (MeHLit) questionnaire.
Translation and cross-cultural adaptation of the questionnaire
With the authorization of the developer, Dr Fatemeh Zarei, we translated the first draft of the English version of the MeHLit questionnaire into Chinese based on the adapted Brislin translation model, including translation, back translation, transcultural adaptation, and a pilot study.57,58
Step 1: Forward translation
By relying on the expertise of two Chinese native speakers who are fluent in English, the questionnaire was independently translated into Chinese.
Step 2: Integration
In addition to the “forward translation,” another graduate student, who speaks English fluently and is a native Chinese speaker, provided a comparison of the two translations. We developed a second Chinese version of the MeHLit questionnaire after discussions among the three researchers about discrepancy items.
Step 3: Back translation
The second Chinese version was back-translated by two native Chinese-speaking nursing PhDs. Both of them had never seen the original MeHLit questionnaire, avoiding information bias and helping to elicit unexpected meanings from the translated versions. The final step was to invite two bilingual nurse educators who were unaware of the original English version to compare and adjust for inconsistencies between the two translated versions. In order to ensure the translations matched the original English version, back-translators repeated the translation several times until the translations matched. The draft of the Chinese version of the MeHLit questionnaire was finally formed.
Step 4: Expert consultation
Several experts were invited to modify the questionnaire items to make them more consistent with the Chinese cultural context and expression, while ensuring that the original wording and meaning of the items remained unchanged to ensure that respondents could clearly understand the content of the items. An expert committee consists of two health education specialists, two psychologists, one communication specialist, one media specialist, and one nurse researcher with experience in acculturation and validation studies for quality life instruments. After reviewing and revising the first draft of the Chinese version, the third version was eventually produced, incorporating new semantics, language expression habits, and professional requirements.
Step 5: Pretest
Thirty participants who met the inclusion criteria were selected through convenience sampling. The researchers informed the participants of the study's purpose, methods, and significance before distributing the questionnaires. Afterward, an interview was conducted in which the interviewer asked if any of the items in the questionnaire were ambiguous, difficult to understand, or unpleasant. The final Chinese version of the MeHLit questionnaire was corrected and proofread following feedback from the interviews. Finally, the pretest Chinese version of the MeHLit questionnaire was developed.
Application of the COSMIN checklist methodology
Investigations concerning measurement properties must adhere to rigorous methodological standards. 59 The COnsensus based Standards for the selection of health status Measurement INstruments (COSMIN) checklist is a globally recognized tool for evaluating the methodological quality of health status measurement instruments. 60 We used the COSMIN checklist framework to examine the reliability (incorporating internal consistency and test–retest reliability) and validity (including construct and content validity) of the MeHLit questionnaire.
Item analysis of the questionnaire
In order to scientifically refine the items, we used the critical ratio method, correlation coefficient method, and internal consistency method. For determining whether the translation questionnaire had the ideal discrimination ability, first, we calculated the total translation questionnaire score and ranked it from high to low; then, we calculated the critical ratio by t-testing two independent samples from the top 27% (high-score group) and the bottom 27% (low-score group). 61 A high discrimination level is considered when the critical ratio of each item ≥ 3 (p < 0.05). 62 The item–total correlation coefficient and Cronbach's alpha values if the item was deleted were also used to assess discrimination. It indicated good homogeneity when item–total correlation coefficients ≥ 0.4. 63 Cronbach's alpha coefficient, a measure of internal consistency, was deemed good if it was >0.70. 64 Besides, McDonald's omega coefficient was used to estimate the reliability. 65 A preliminary EFA was conducted for factor loadings, and the factor loadings for each item were recommended to be higher than 0.4. 66 Items failing to meet these conditions were eliminated. 67
Evaluation of psychometric properties of the questionnaire
We invited a health education specialist, two psychologists, two communication specialists, and two media specialists to assess the content validity of the Chinese version of the questionnaire. The experts were selected based on (a) their extensive expertise in the fields of public health, science, and medicine; (b) their familiarity with the questionnaire's Chinese translation steps and psychological measures; (c) at least bachelor's degrees and ten years’ experience in their fields; and (d) their voluntary participation in this study. A Likert four-point scoring system was used to collect the experts’ responses, with responses including 1 = not relevant, 2 = slightly relevant, 3 = strongly relevant, and 4 = highly relevant. An item's content validity index (I-CVI) is the proportion of experts who rated the content as valid (relevance rating of 3 or 4). A questionnaire's content validity index (CVI) is calculated by averaging its item-by-item CVI, referred to as the S-CVI. We require the I-CVI ≥ 0.78 and the S-CVI ≥ 0.90, which indicates good overall content validity for the questionnaire. 68
The underlying factors of the translation questionnaire were investigated using EFA and CFA. Principal axis factor analysis of the EFA was completed to explore the underlying factor structure of the questionnaire. We considered the dataset suitable for EFA if Bartlett's test of sphericity was significant (p < 0.05) and Kaiser–Meyer–Olkin (KMO) > 0.60. 69 The principal components of the EFA were further estimated using principal component analysis (PCA) coupled with varimax rotation. Three principles of EFA were followed in this study: (a) the factor loadings of items should be ≥0.4, and there were no cross-loadings; (b) the cumulative explanatory variables of all common factors were ≥40%; and (c) each extracted common factor contains at least three items of measurement. If items did not meet the requirements of these statistical methodologies, the corresponding items would be excluded. 67
A number of “goodness-of-fit” statistics were used in the CFA to determine whether the hypothesized statistical model fits the actual dataset. The criteria for fitting indexes are as follows: (a) the chi-squared degree of freedom (χ2/DF) ≤ 3; (b) the root mean square error of approximation (RMSEA) ≤ 0.05; (c) the goodness-of-fit index (GFI), the adjusted GFI (AGFI), the Tucker Lewis index (TLI), the comparative fit index (CFI), and the incremental fit index (IFI) ≥ 0.9; and (d) the parsimonious GFI (PGFI) and the parsimonious normed-of-fit index (PNFI) ≥ 0.5.70,71
In addition, convergent and discriminant validity tests assessed the questionnaire's structural validity. We assessed convergent validity by measuring the average variance extracted (AVE) and composite reliability (CR). Ideally, the model should have CR > 0.7 as well as AVE > 0.45. 72 In order to determine the discriminant validity of the model, we calculated the square root of the AVE value and the correlation coefficient of each factor. It was a requirement that the square root of the AVE value was greater than the correlation coefficient between the corresponding factors in the model. 72
We conducted internal consistency analysis and test–retest reliability testing of the Chinese translation of the MeHLit questionnaire. For reliability analysis, we calculated overall and dimensional Cronbach's α coefficient and the split-half reliability coefficient of the questionnaire to assess internal consistency. To assess the test–retest reliability of the MeHLit questionnaire, 50 participants were remeasured 2 weeks later with the translated questionnaire, and correlation coefficients were calculated to assess the stability of the questionnaire. We required that Cronbach's α coefficient, the split-half reliability coefficient, and the test–retest reliability coefficient should all be 0.7 or higher.73,74
Instruments
The general demographic characteristics questionnaire
Based on a systematic literature review and team discussions, we designed a general demographic characteristics questionnaire. This questionnaire included five self-reported items: age, gender, educational status, marital status, and job status.
The MeHLit questionnaire
The MHL regarding health information was measured through the MeHLit questionnaire developed by Nazarnia et al. 55 There are 21 items in the questionnaire, which are divided into five dimensions. Five dimensions can be categorized as goal appraisal skill, content appraisal skill, implicit meaning appraisal skill, audience appraisal skill, and visual comprehension skill. The Likert five-point rating system was used to collect participants’ responses. It ranged from never (0), rarely (1), sometimes (2), most of the time (3), and always (4). Scores range from 0 to 84. A high total score indicates more significant media literacy in understanding health information. Cronbach's α value was 0.91, with domains ranging from 0.70 to 0.82. 55
Data collection
After explaining the purpose and significance of the study, the researchers recruited participants primarily through online social networks. In the first phase, seven qualified experts received a survey package by email that included an informed consent form and expert consultation questionnaire and were advised to return it within 2 weeks. The questionnaires had a satisfactory recovery rate. In the second phase, 550 individuals were invited to participate in the survey, and 522 agreed to the invitation and signed the informed consent form. After removing invalid questionnaires with missing data, 514 valid questionnaires were retained for item analysis. In the third stage, we recruited 700 individuals, and after removing those who did not agree to participate in the study and those with missing data, we ultimately retained 686 questionnaires. It takes about 5–8 minutes to complete each questionnaire.
Data analysis
Statistical analysis was performed with a 95% confidence level, using SPSS 25.0 (IBM Corp., Armonk, NY, United States) and AMOS 23.0 (IBM Corp., Armonk, NY, United States). Participants’ general demographic characteristics were described using frequency and composition ratios. Item analysis was used to evaluate the quality of the items, and expert consultation was conducted to assess the content validity of the questionnaires. In order to investigate the underlying factor structure of translation questionnaires, EFA was conducted using the principal axis factoring method. Using AMOS 23.0, a CFA was conducted to assess the questionnaire's structural validity. The homogeneity and stability of the questionnaire were determined by an internal consistency analysis and a test–retest reliability analysis.
Before filling out any questionnaires, all participants in the study signed an informed consent form informing them of the purpose of the study and its significance and emphasizing the voluntary and anonymous nature of the participation. All methods and contents of this study were conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Ethics Review Committee of Jinzhou Medical University (no. JZMULL2022092).
Results
The general demographic characteristics
In the second phase, we finally recruited 514 individuals for the item analysis, with a sample including 321 males (62.5%) and 193 females (37.5%), with 30.9% of the participants married. In phase 3, there were 343 validated questionnaires for the EFA, consisting of 202 males (58.9%) and 141 females (41.1%), with 30.9% of participants being married. There is a total of 343 valid questionnaires for CFA, consisting of 188 males (54.8%) and 155 females (45.2%), with 37.0% of participants married. See Table 1 for more details.
Frequency distribution of demographic characteristics.

CFA: confirmatory factor analysis; EFA: exploratory factor analysis.
Translation and cross-cultural adaptation of the questionnaire
The original Chinese version of the MeHLit questionnaire was developed through translation, back translation, and cultural adaptation. To revise the MeHLit questionnaire, seven experts were invited. The questionnaire includes five dimensions (goal appraisal skill, content appraisal skill, implicit meaning appraisal skill, audience appraisal skill, and visual comprehension skill) and 21 items. The revised draft of the Chinese version of the MeHLit questionnaire was easy to understand and answer based on the opinions of all 30 participants who were initially surveyed. Ultimately, 21 items were developed as a pretest version of the Chinese version of the MeHLit questionnaire.
Item analysis of the questionnaire
The item's quality was estimated based on the critical ratio, the item–questionnaire correlation coefficient, and Cronbach's α coefficient. The critical ratio (CR) assesses the discriminability of the item, with >3.000 indicating that the item has a high discriminability. The results showed that CR values ranged from 11.243 to 27.170, with significant differences in scores between the high and low groups for all items (p < 0.001), indicating a high discriminatory ability for each item. This study's item–total correlation coefficients ranged from 0.419 to 0.646 (p < 0.001). Taking the translated questionnaire as an example, after deleting each item, we found that Cronbach's coefficient for the translated questionnaire was 0.902–0.908, which did not exceed Cronbach's coefficient of the questionnaire itself (0.909). Based on the above, it is recommended that all 21 items be retained. A preliminary EFA was completed to assess the preliminary factor structure and item loadings. The preliminary EFA showed that the recommended factor loadings ranged from 0.741 to 0.919, and none of the items had factor loadings below 0.40, so all items were recommended to be retained. The detailed information is shown in Table 2.
Item analysis of the Media Health Literacy (MeHLit) questionnaire.
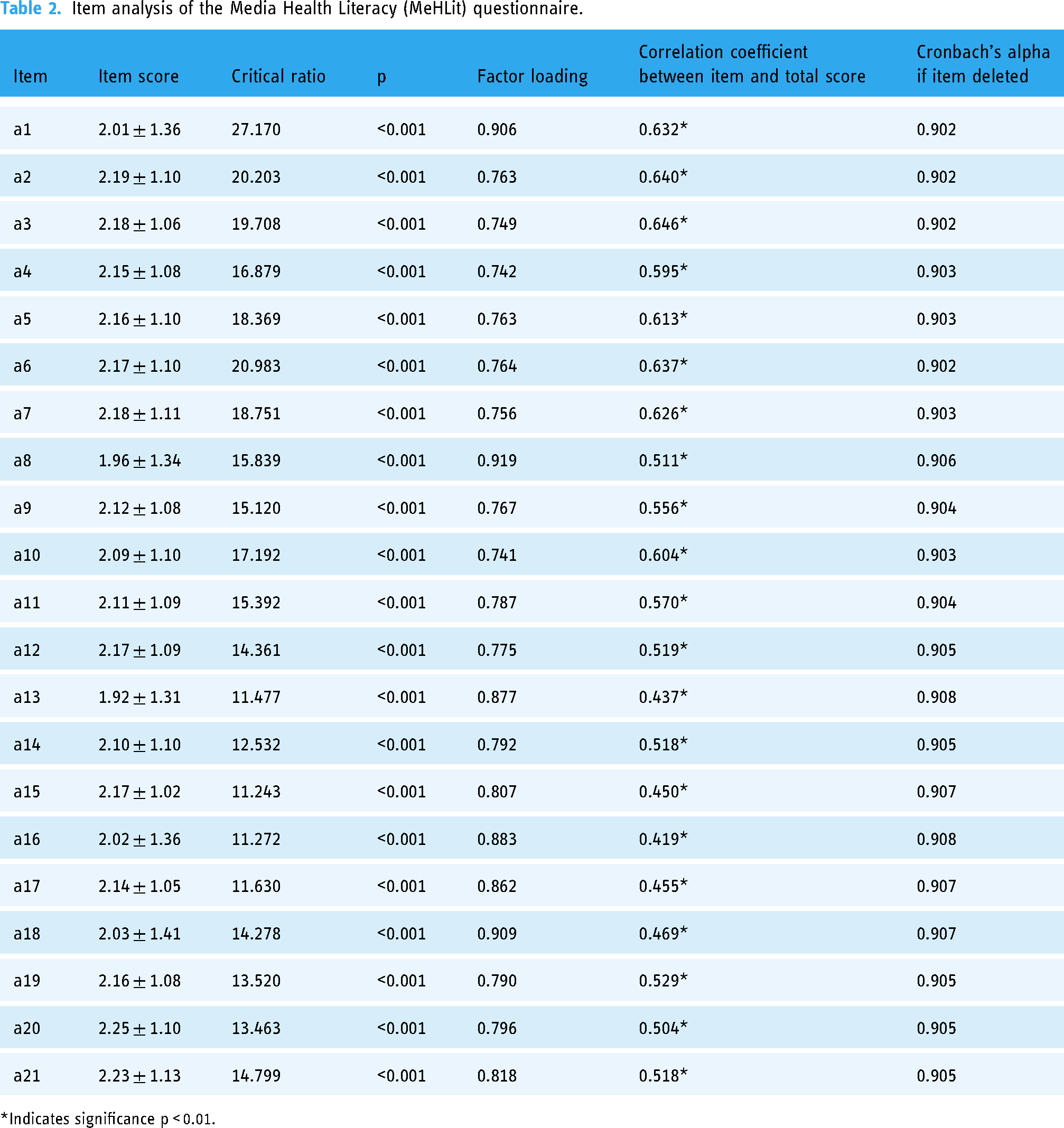
*Indicates significance p < 0.01.
Evaluation of psychometric properties of the questionnaire
Content validity
The results showed that the I-CVI ranged from 0.857 to 1.000 and the S-CVI was 0.946, both of which were higher than the reference value and had good content validity.
Construct validity
In the EFA, the Kaiser–Meyer–Olkin value was 0.773, and the Bartlett sphericity test was significant (χ2 = 2933.161; p < 0.001); therefore, it is suitable for factor analysis. Based on the graphical analysis of the scree plot, the Kaiser–Guttman rule (initial eigenvalues > 1), and the principle of explained total variance (at least >50%), this study confirmed the validity of the five-factor structure. The initial factor analysis resulted in five factors with eigenvalues of 19.112, 15.247, 12.995, 9.520, and 8.027, which explained 64.902% of the total variance of the items. In addition, the factor loadings for each factor were satisfactory, as shown in Table 3, and the graph of the scree plot is shown in Figure 2.
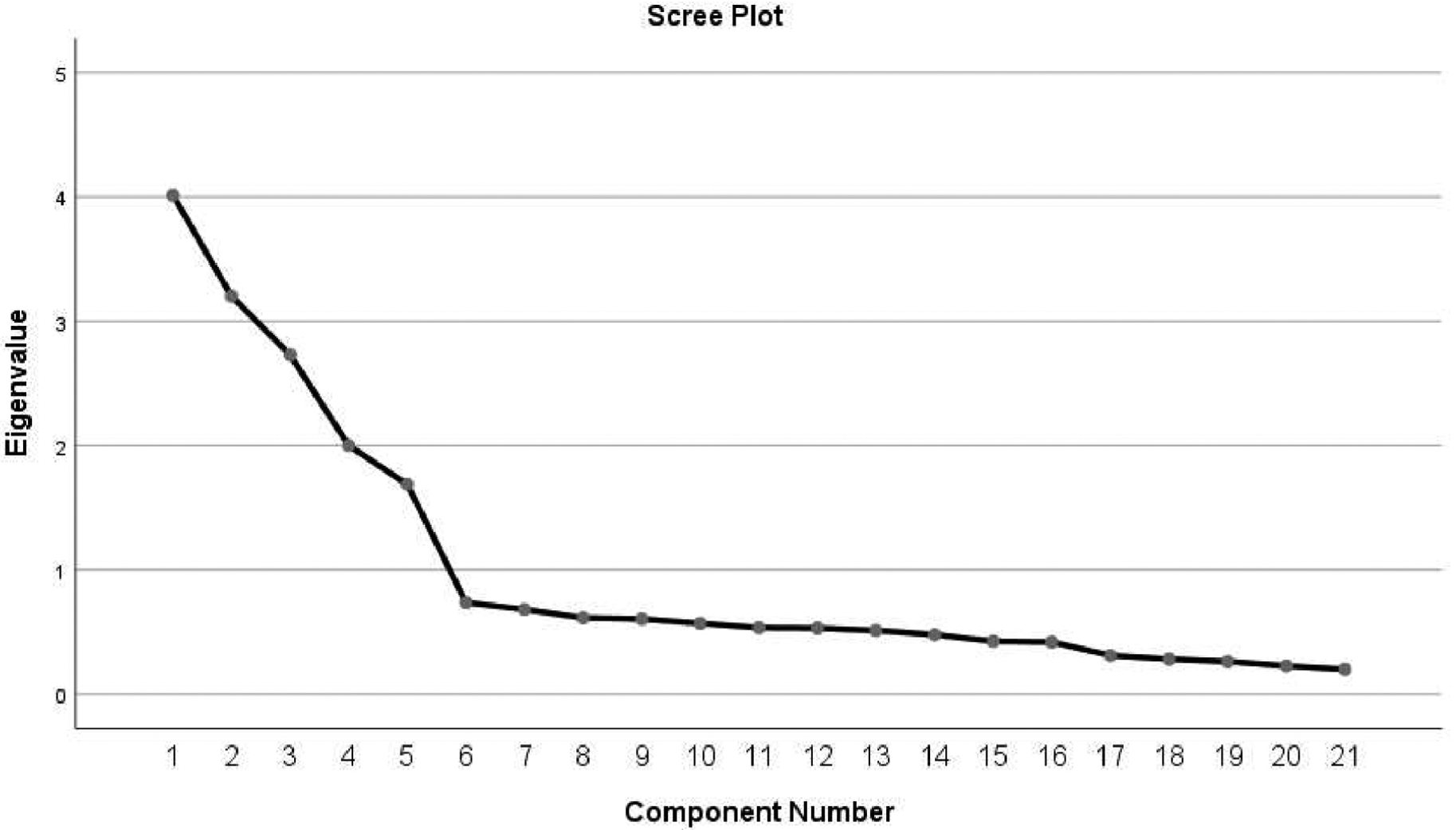
Scree plot of exploratory factor analysis for the Chinese version of Media Health Literacy (MeHLit) questionnaire.
Factor loadings of exploratory factor analysis for the Chinese version of the Media Health Literacy (MeHLit) questionnaire.

Note: Major loadings for each item are bolded.
To test the construct validity of the MeHLit questionnaire, we first used maximum likelihood structural equation model (SEM) for CFA to assess the degree of fit of the five-factor model to the observed data (Figure 3). As the results of model fitting, χ2/DF = 1.433, GFI = 0.936, AGFI = 0.917, RMSEA = 0.036, TLI = 0.978, CFI = 0.981, IFI = 0.981, PGFI = 0.725, and PNFI = 0.802. All fit indices are good, which indicates that the five-factor model is a good representation of the underlying structure of the MeHLit questionnaire in the data. The results of the analysis showed that the AVE values ranged from 0.521 to 0.705 and the CR values ranged from 0.706 to 0.944, both of which exceeded the recommended thresholds, indicating that the questionnaire was excellent in the convergent validity. The discriminant validity analysis of this study showed that the square root values of AVE ranged from 0.722 to 0.840, both of which were greater than the maximum correlation coefficient values, indicating that the questionnaire had good discriminant validity (Table 4).

Standardized five-factor model of the Chinese version of the Media Health Literacy (MeHLit) questionnaire.
Convergent validity and discriminant validity of the Media Health Literacy (MeHLit) questionnaire.

AVE: average variance extracted; CR: composite reliability.
Internal consistency, split-half reliability, and test–retest reliability
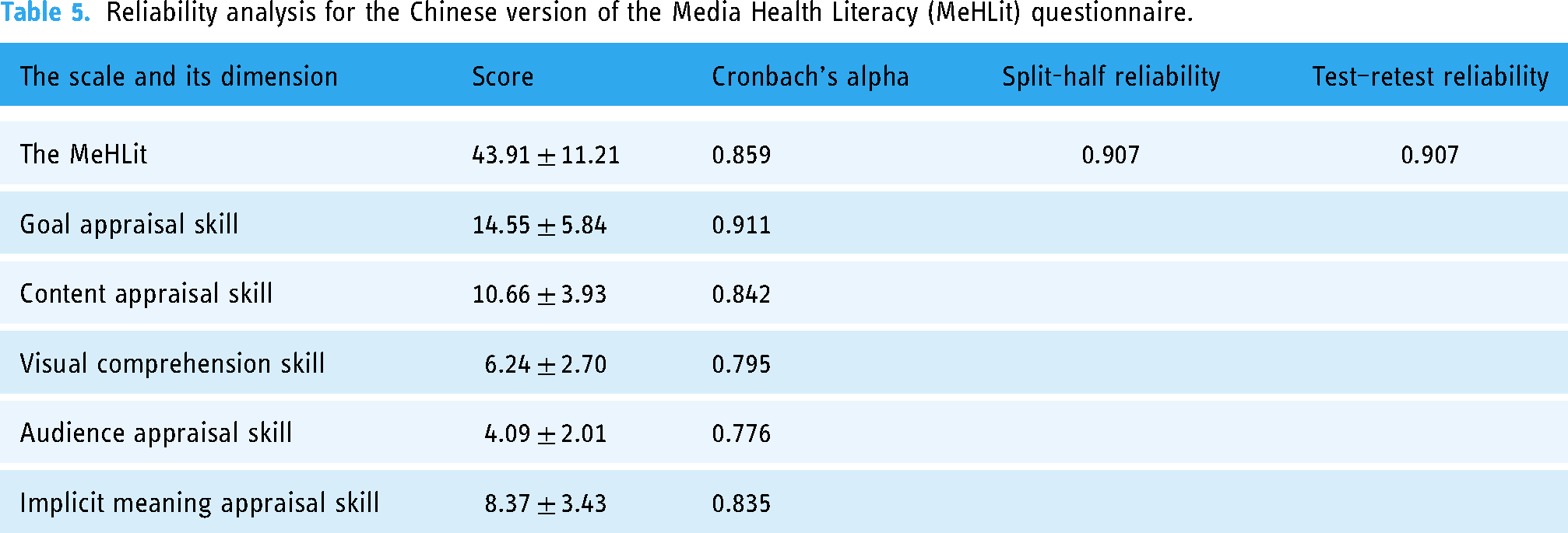
In this study, the reliability of the Chinese version of the MeHLit questionnaire was evaluated in terms of internal consistency, split-half reliability, and test–retest reliability. The translated questionnaire has high internal consistency with Cronbach's α value of 0.859, while Cronbach's α value of dimensions is 0.776–0.911, the split-half reliability is 0.907, and test–retest reliability is 0.907 (Table 5). McDonald’s omega coefficient was 0.833, which indicates adequate reliability for scores on the Chinese version of the MeHLit questionnaire.
Reliability analysis for the Chinese version of the Media Health Literacy (MeHLit) questionnaire.
Discussion
Both health literacy 75 and media literacy76–79 have different tools to assess the two concepts. MHL, as a hybrid and unique concept, currently lacks an instrument to assess adult MHL in China. In this study, the MeHLit questionnaire was translated into Chinese for the first time, 57 and its psychometric properties were validated by factor analysis. 80 The Chinese version of the MeHLit questionnaire has good reliability and validity and can be considered a valid tool for assessing MHL among Chinese adults. In addition, during the COVID-19 pandemic, the public mainly obtained health-related information through various media (e.g. news apps, radio, and TV news), and MHL played an important role in identifying the truth and falsity of health-related information from different sources. 81 Improving public MHL will benefit individuals to acquire health knowledge purposefully and apply it effectively for self-protection, disease prevention, and health screening, thus improving and enhancing personal health behaviors.
The Chinese version of the MeHLit questionnaire has suitable distinction
In this study, the MeHLit questionnaire was translated into Chinese and cross-culturally adapted according to the Brislin translation principle. 57 A group of seven experts was invited to review and revise the content validity of the translated questionnaire, and we developed the Chinese version of the MeHLit questionnaire through their review and revision. Through a preliminary survey, 30 participants indicated that the semantic expression of the questionnaire was clear and the content was easy to understand. The final Chinese version of the MeHLit questionnaire contains 21 items divided into five dimensions, with a structure comparable to the English version. Item analysis showed that the CR values of all items were higher than the standard value of 3 and statistically significant, further verifying that the reliability of the questionnaire was guaranteed and did not require deletion. In addition, the scores of each item were moderately to highly correlated with the total score of the questionnaire. 82 Cronbach's α values did not exceed the original values of the translated scale after each item was removed. All of these indicate that the Chinese version of the MeHLit questionnaire has good applicability and discrimination.
The Chinese version of the MeHLit questionnaire has adequate reliability
Reliability analysis is a measure of the reliability and validity of an instrument or questionnaire and is used to reflect the authenticity of the instrument being measured. 83 In this study, we assessed the reliability of the Chinese version of the MeHLit questionnaire by measuring internal consistency reliability, split-half reliability, and test–retest reliability. Cronbach's α coefficient assesses the internal consistency and reliability of the questionnaire, with >0.7 indicating good reliability.84,85 The study confirmed that the Chinese version of the MeHLit questionnaire had high internal consistency, as indicated by Cronbach's α coefficient for the total scale of 0.859 and Cronbach's α coefficient for the dimensions ranging from 0.776 to 0.911, slightly higher than the results of the original scale, 55 indicating that the scale measurement results are reliable. Despite the good internal consistency of this study, we further performed additional assessments, such as split-half reliability or test–retest reliability. The split-half reliability coefficient was 0.907, further demonstrating reliability. Test–retest reliability is an evaluation of whether repeated measures with a research instrument produce consistent results for the same group of subjects, assessing the stability of observed scores over time. According to the results, the test–retest reliability of the Chinese version of the questionnaire was 0.907, indicating that the Chinese version of the MeHLit questionnaire has good stability and can be used for assessing adults’ MHL to assess an individual's ability to critically evaluate and apply complex media health information. In this way, they can navigate the healthcare system to get health-related information to solve health problems and make relevant decisions. Overall, the Chinese version of the MeHLit questionnaire has good reliability and validity, and it is suitable for Chinese subjects.
The Chinese version of the MeHLit questionnaire has ideal validity
Validity refers to the degree to which a tool can adequately reflect the content to be measured, including content validity and structural validity. Content validity refers to the extent to which the items in a scale adequately respond to the measured content and is mostly assessed by a committee of experts. Seven experts were invited to assess the content validity of the translated questionnaire, and their comments were incorporated into the final version of the questionnaire. After the experts evaluated the Chinese version of the MeHLit questionnaire, the I-CVI ranged from 0.857 to 1.000 and the S-CVI was 0.946, both of which were higher than the reference values, 86 indicating excellent content validity. Construct validity reflects the extent to which the scale is consistent with its conceptual framework. To assess the construct validity of the questionnaire, the items were evaluated by factor analysis (EFA and CFA). Prior to the CFA assessment of construct validity, the EFA explored the factor structure. When EFA was used to evaluate the construct validity of the questionnaire, if the cumulative variance contribution of the common factors extracted from the scale was >60% and each factor loading was >0.4, it indicated good construct validity.87,88 EFA showed that the Chinese version of the MeHLit questionnaire maintained the same factor structure as the original English version, with all items loaded on the same factors as the original version. The five-factor structure extracted by EFA in this study was consistent with the original questionnaire, 55 which accounted for 64.902% of the total variance, and the factor loadings of each item in the questionnaire were >0.4, which had high construct validity. The results suggest that the 21-item MeHLit questionnaire for assessing MHL has high validity and is an encouraging tool for assessing the MHL of the public. Meanwhile, the CFA showed that the fit index was good and stronger than the original questionnaire, 55 indicating that our actual survey data fit the structural equation model very well and that the tool was able to measure the important concept of MeHLit well and the items were easy to understand. Both EFA and CFA show that the English and Chinese versions have the same statistical structure, indicating the cross-cultural validity of the tool.
Limitations
This study has some limitations that need to be noted and discussed. First, most of our data were collected through social platforms, and the non-use of these social software by the public who did not participate in this study may have biased the results. Second, bias from the nature of convenience sampling is inevitable; based on this, we considered a rigorous data collection procedure to reduce selection bias and considered a 20% sample loss rate. In addition, due to the self-reported nature of this survey, bias is unavoidable. Finally, although we have fully validated the psychometric characteristics of the Chinese version of the MeHLit questionnaire among the public, we did not explore the factors that influence public MHL. In addition, as there are currently no clearly defined criteria for MeHLit scores to determine whether individuals have MHL, they need to be further explored in future studies. Therefore, these will be the focus of our future work, which will be important for our next step.
Conclusion
The Chinese version of the MeHLit questionnaire was successfully introduced in China. It has shown good psychometric properties among the Chinese public and has high potential applicability as a standard assessment tool to measure the level of MHL among the public. The questionnaire can also help healthcare providers and researchers develop educational strategies for populations with low MHL, improve their MHL skills, and regulate misleading and low-quality health-related information on media platforms to reduce the public health threat of misinformation, thereby improving their overall health status. During the COVID-19 epidemic, improving MHL will enable the general public to better prevent COVID-19, resulting in better health outcomes.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076231203801 - Supplemental material for Psychometric evaluation of the Chinese version of the media Health Literacy Questionnaire: A validation study
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076231203801 for Psychometric evaluation of the Chinese version of the media Health Literacy Questionnaire: A validation study by Wenbo Li, Yanli Zhang, Jiaqing Liang and Hongyu Yu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231203801 - Supplemental material for Psychometric evaluation of the Chinese version of the media Health Literacy Questionnaire: A validation study
Supplemental material, sj-docx-2-dhj-10.1177_20552076231203801 for Psychometric evaluation of the Chinese version of the media Health Literacy Questionnaire: A validation study by Wenbo Li, Yanli Zhang, Jiaqing Liang and Hongyu Yu in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank the study participants for their contributions to this research. In addition, Prof. Fatemeh Zarei, one of the developers of the MeHLit questionnaire, provided helpful feedback and valuable editorial suggestions.
Contributorship
WL performed the study design, data collection, and analysis and interpretation of the results and drafted the manuscript. HY made the necessary revisions to the manuscript. YZ performed the data collection and analysis and interpretation of the results. JL assisted with data collection. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were approved with the ethical standards of the Ethics Committee of the Jinzhou Medical University. In addition to this, we confirmed that the experimental protocol was approved by the Ethics Committee of the Jinzhou Medical University (No. JZMULL2022092) and in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Hongyu Yu
Informed Consent
Written informed consent was obtained from all participants included in the study.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.