
Abstract
Background
Electronic Health Record (EHR) implementation in low- and middle-income countries (LMICs) remains constrained by infrastructure limitations, dual documentation requirements, and limited local evidence on workflow impact—particularly in time-sensitive oncology settings. We evaluated the implementation of a modular, cloud-based EHR system in a tertiary surgical oncology unit in Sri Lanka operating in parallel with mandatory paper documentation.
Methods
A convergent mixed-methods study was conducted during the first six months of implementation. Quantitatively, paired comparisons were performed for 100 consecutive theatre lists and 100 consecutive biopsy-confirmed malignancy cases to assess changes in theatre-list preparation time and biopsy-to-diagnosis interval. Mean differences with 95% confidence intervals (CIs) and effect sizes (Cohen’s dz) were calculated. Concurrently, 26 healthcare professionals completed an investigator-designed usability survey; descriptive statistics were reported, and exploratory inferential analyses were performed. Open-text responses underwent reflexive thematic analysis.
Results
The EHR significantly reduced theatre-list preparation time from 4.10 minutes to 2.40 minutes (mean reduction 1.70 minutes; 95% (CI 1.44–1.96); Cohen’s dz = 1.29; p < 0.0001). The biopsy-to-diagnosis interval decreased from 14.95 days to 8.40 days (mean reduction 6.55 days; 95% (CI 4.52–8.58; Cohen’s dz = 0.64; p < 0.0001). Overall user satisfaction was high (mean 4.31/5, SD 0.55). Training adequacy was associated with higher satisfaction (mean difference 0.47; p = 0.035), and satisfaction correlated with ease of data entry (r = 0.60, p = 0.001). Qualitative analysis identified four themes: improved information retrieval, enhanced multidisciplinary coordination, hybrid documentation burden, and infrastructure-related optimisation needs. Survey inferential findings are exploratory due to use of a non-validated instrument.
Conclusions
In a resource-constrained oncology setting, implementation of a secure, cloud-based EHR was associated with substantial workflow efficiency gains and strong user acceptability, despite operating within a hybrid paper–electronic environment. Findings support the feasibility and measurable impact of context-sensitive digital transformation in LMIC tertiary services, while underscoring the importance of infrastructure reliability, structured training, and deliberate transition away from dual documentation for sustainable scale-up.
Keywords
• Electronic health records enhance workflow, data access, and team collaboration. • Electronic health records significantly reduced biopsy-to-diagnosis delays. • High user satisfaction is associated with intuitive design and adequate training. • Technical issues and system speed were the primary challenges for users. • Targeted training and robust infrastructure are vital for successful implementation.Highlights
Introduction
Electronic health records (EHRs) are central to contemporary digital health strategies, enabling longitudinal data capture, continuity across clinical encounters, and improved care coordination and secondary use of data for quality improvement and planning. 1 In hospital settings, EHR implementation has been associated with improvements in documentation quality, information accessibility, and selected workflow efficiency metrics; however, benefits are heterogeneous and depend strongly on local workflow redesign, training adequacy, governance alignment, and infrastructure reliability.2,3
Implementation challenges are particularly pronounced in low- and middle-income countries (LMICs) and other resource-constrained settings. Barriers commonly include unreliable connectivity, limited hardware availability, constrained technical support capacity, financial limitations, and resistance to workflow change.3–5 Hybrid transition states—where electronic documentation is introduced while paper records remain mandatory—may further increase documentation burden and attenuate perceived efficiency gains during early adoption. 4 These sociotechnical constraints mean that locally generated implementation evidence is critical to inform safe scale-up.
Sri Lanka is actively advancing its national digital health agenda. The National Digital Health Blueprint outlines an interoperable digital health architecture centred on a National Electronic Health Record (NEHR) system, 6 supported by the National Digital Health Guidelines and Standards (NDHGS), which provide implementation guidance on interoperability, privacy, security, and governance. 7 Despite these policy developments, EHR adoption in public-sector hospitals remains uneven, and comprehensive real-world evaluations of EHR implementation within time-sensitive clinical pathways are limited.
Oncology services represent a particularly important context for evaluation. Delays in cancer diagnosis and treatment are associated with adverse clinical outcomes and increased patient distress. 8 Digital result-notification systems and structured multidisciplinary documentation platforms have demonstrated potential to improve timeliness and coordination in complex care pathways.9–11 However, evidence from LMIC tertiary oncology settings—where infrastructure constraints and hybrid documentation policies coexist—is sparse.4,12
The Surgical Oncology Unit and Cancer Multidisciplinary Team (MDT) at Teaching Hospital Anuradhapura implemented a modular, cloud-based EHR system while operating in parallel with mandatory paper documentation during the transition phase. This study evaluates that implementation using a convergent mixed-methods design. Quantitatively, we assessed changes in two predefined workflow efficiency indicators: theatre-list preparation time and biopsy-to-diagnosis interval. Qualitatively, we explored end-user experiences to identify perceived benefits, barriers, and optimisation priorities. The objective was to generate context-specific implementation evidence to inform sustainable EHR integration within resource-limited oncology services and to contribute to the broader digital transformation agenda in Sri Lanka and comparable LMIC health systems.
Methods
Study design and setting
This convergent parallel mixed-methods study combined quantitative and qualitative data to evaluate the implementation of a cloud-based Electronic Health Record (EHR). The evaluation was conducted over a six-month period (September 2022–February 2023) at the Surgical Oncology Unit, Teaching Hospital Anuradhapura, Sri Lanka—one of the country’s largest tertiary cancer centres transitioning from paper-based to digital documentation. The EHR was introduced in September 2022 following a structured pilot and internal testing phase, with full operational integration across outpatient clinics, inpatient wards, and theatre services during the study period. During this transition, documentation shifted from an entirely paper-based workflow to a hybrid EHR-supported environment while maintaining mandatory parallel paper records in accordance with national policy. The workflow transition process and system interface examples are illustrated in Figure 1 (paper-based theatre list workflow) and Figure 2 (EHR-generated theatre list workflow). Example of a handwritten surgical theatre list used before EHR implementation. Corresponding digital theatre list generated by the implemented EHR system.

EHR intervention and implementation context
Prior to implementation, clinical documentation relied entirely on patient-held clinic books, handwritten laboratory entries, and printed pathology and imaging reports physically carried by patients. This manual process frequently resulted in misplaced records, delays in retrieving past investigations, fragmented multidisciplinary communication, and unstructured follow-up after biopsy procedures, contributing to avoidable diagnostic delays.
To address these limitations, a modular, cloud-hosted EHR system was introduced. The system supported structured longitudinal documentation, digital theatre-list preparation, MDT case recording, real-time investigation tracking, and automated notification of key workflow events, including SMS alerts for biopsy report availability.
The EHR was developed in alignment with Sri Lanka’s National Digital Health Guidelines and Standards (NDHGS)
7
and incorporated: • Encrypted Secure Socket Layer (SSL) transmission • Role-based access control • Audit logging of user activity • Scheduled automated backups with disaster recovery support
Cloud hosting was selected to enhance data resilience, enable secure remote access, and reduce dependence on local hardware infrastructure in a resource-constrained setting. Access to the system was restricted to authorised hospital personnel through individual credential-based authentication, with periodic password renewal protocols enforced.
Before full deployment, the system underwent iterative testing in a controlled environment. Clinicians trialled the prototype in routine clinical scenarios, and refinements were made to optimise terminology, workflow alignment, and usability. Parallel paper documentation was maintained throughout the study period in accordance with national policy, ensuring continuity of care and providing redundancy during transition.
Study population and sampling
Patient cohort
One hundred consecutive adult patients with histologically confirmed malignancies entering the unit’s care during the six-month evaluation were enrolled.
Inclusion criteria
Patients newly admitted to the surgical oncology unit with confirmed cancer and complete documentation in both systems.
Exclusion criteria
Patients without histological confirmation, those transferred elsewhere before completion of care, or records missing in either system.
Sampling strategy
Consecutive sampling for patients and census sampling for staff.
Staff cohort
All healthcare workers with ≥1 month experience using the EHR (n = 26; 8 consultant surgeons, 10 medical officers, 6 nursing officers, 1 postgraduate trainee, and 1 ward clerk) were invited by email to complete an online survey; all consented to participate.
Data Collection and outcomes
Quantitative component
The quantitative evaluation focused on two predefined workflow efficiency outcomes: 1. Theatre-list preparation time 2. Biopsy-to-diagnosis interval
Theatre-list preparation time
The time required to prepare 100 consecutive theatre lists was measured under both the conventional paper-based workflow and the EHR-supported workflow.
Where possible, theatre-list preparation times were extracted directly from EHR system activity logs. When manual timing was required for paper-based lists, a standardised stopwatch protocol was applied (start: first list entry; stop: final verification). To enhance measurement validity, a second reviewer independently verified a random 10% sample of recorded timings.
Biopsy-to-diagnosis interval
The biopsy-to-diagnosis interval was defined as the number of days from biopsy date to pathology report availability and communication to the clinical team.
For the EHR-supported workflow, timing was calculated using biopsy dates and laboratory report release timestamps recorded in the system. For the legacy paper workflow, intervals were verified against pathology registers and clinic documentation procedures used to retrieve printed reports.
Clinician survey component
Healthcare worker perceptions of the EHR were assessed using an anonymous investigator-designed questionnaire distributed electronically six months after system introduction.
The instrument included: • Likert-scale items (1–5) assessing intuitiveness, interface usability, information accessibility, data entry experience, system speed, technical stability, training adequacy, technical support responsiveness, and overall satisfaction • Categorical items assessing training adequacy • Open-text prompts exploring workflow impact, barriers, resistance to change, dual documentation burden, and improvement suggestions
The questionnaire was informally piloted among five staff members across different roles and revised for clarity. No formal psychometric validation (content validity, construct validity, or reliability testing) was performed. Accordingly, inferential analyses were treated as exploratory and hypothesis-generating rather than confirmatory. 13
Descriptive statistics (mean, standard deviation, and 95% confidence intervals) were reported for Likert-scale items. Group comparisons were conducted using one-way ANOVA, and associations between overall satisfaction and usability domains were assessed using Pearson correlation coefficients with corresponding 95% confidence intervals. All survey findings were interpreted cautiously due to the non-validated instrument.
Qualitative analysis
Open-text survey responses were analysed using reflexive thematic analysis following Braun and Clarke’s methodological guidance. 14
The qualitative dataset comprised 381 substantive free-text comments across 21 open-ended prompts. Two researchers independently reviewed responses, generated initial codes, and collaboratively refined candidate themes through iterative discussion to ensure internal coherence and distinctiveness. Approximately 20% of responses were double-coded to enhance analytic rigor. An audit trail and analyst triangulation were used to strengthen credibility.
Consistent with a reflexive analytic approach, inter-rater reliability statistics were not calculated. The qualitative strand aimed to explain and contextualise quantitative findings rather than to generate inferential claims; therefore, thematic salience was described narratively rather than statistically.
Statistical Analysis
Continuous variables were assessed for approximate normality. Because distributions did not demonstrate substantial deviation from normality, paired t-tests were used to compare paper-based and EHR-supported workflows.
For each outcome, mean differences (paper minus EHR), 95% confidence intervals (CIs), and Cohen’s dz effect sizes were calculated.
For survey analyses: • One-way ANOVA examined differences in satisfaction between training adequacy groups • Pearson’s r assessed correlations between overall satisfaction and usability domains • 95% CIs and effect sizes (Cohen’s d, η2 where appropriate) were reported
A two-tailed p-value <0.05 was considered statistically significant.
Ethical approval
Ethical approval was obtained from the Ethics Review Committee, Faculty of Medicine, Rajarata University (ERC/2022/32). All staff participants provided informed consent. Patient data used for efficiency measurements were de-identified prior to analysis. No personally identifiable information was retained, and data handling complied with institutional privacy policies and Sri Lanka’s National Digital Health Guidelines.
Preprint acknowledgement
A preprint version of this work is available on medRxiv (DOI: 10.1101/2025.07.12.25331172). The current manuscript incorporates revisions following peer review.
Results
Participant characteristics
A total of 26 healthcare professionals completed the post-implementation survey (response rate: 100% of eligible staff). Participants included 8 consultant surgeons, 10 medical officers, 6 nursing officers, 1 postgraduate trainee, and 1 ward clerk. At the time of evaluation, 84.6% reported routine EHR use for the full six-month implementation period.
For workflow evaluation, 100 consecutive theatre lists and 100 consecutive biopsy-confirmed malignancy cases were analysed under both paper-based and EHR-supported processes.
Quantitative efficiency outcomes
Theatre list preparation time
The mean theatre-list preparation time decreased from 4.10 minutes (SD 0.80) using the paper-based process to 2.40 minutes (SD 0.42) using the EHR system, representing a mean paired reduction of 1.70 minutes (95% CI 1.44 - 1.96; Cohen’s dz = 1.29; p < 0.0001).
Biopsy-to-diagnosis interval
Paired comparisons of workflow efficiency outcomes between paper-based and EHR-supported processes. Values represent mean (SD) unless otherwise indicated.

Clinician survey (quantitative exploratory results)
Overall satisfaction with the EHR system was high (mean 4.31, SD 0.55; 95% CI (4.09–4.53)). Domain-specific ratings were also favourable, with high scores for intuitiveness (mean 4.08, SD 0.60; 95% CI (3.85–4.31)), interface friendliness (mean 4.08, SD 0.58; 95% CI (3.86–4.30)), and information accessibility (mean 4.08, SD 0.57; 95% CI (3.87–4.29)). Ease of data entry was rated positively (mean 4.00, SD 0.62; 95% CI (3.76–4.24)), while system speed received slightly lower but still favourable ratings (mean 3.92, SD 0.69; 95% CI (3.64–4.20)). Technical stability showed greater variability (mean 3.65, SD 0.94; 95% CI (3.28–4.03)), whereas technical support was rated highest among all domains (mean 4.54, SD 0.65; 95% CI (4.28–4.80)).
Users rated the system highly for intuitiveness (mean 4.08), interface friendliness (mean 4.08), and information accessibility (mean 4.08). System speed was rated slightly lower (mean 3.92), reflecting occasional latency. The distribution of mean scores across usability domains is illustrated in Figure 3. Mean usability ratings (1–5 Likert scale) across key EHR domains. Error bars represent standard deviations.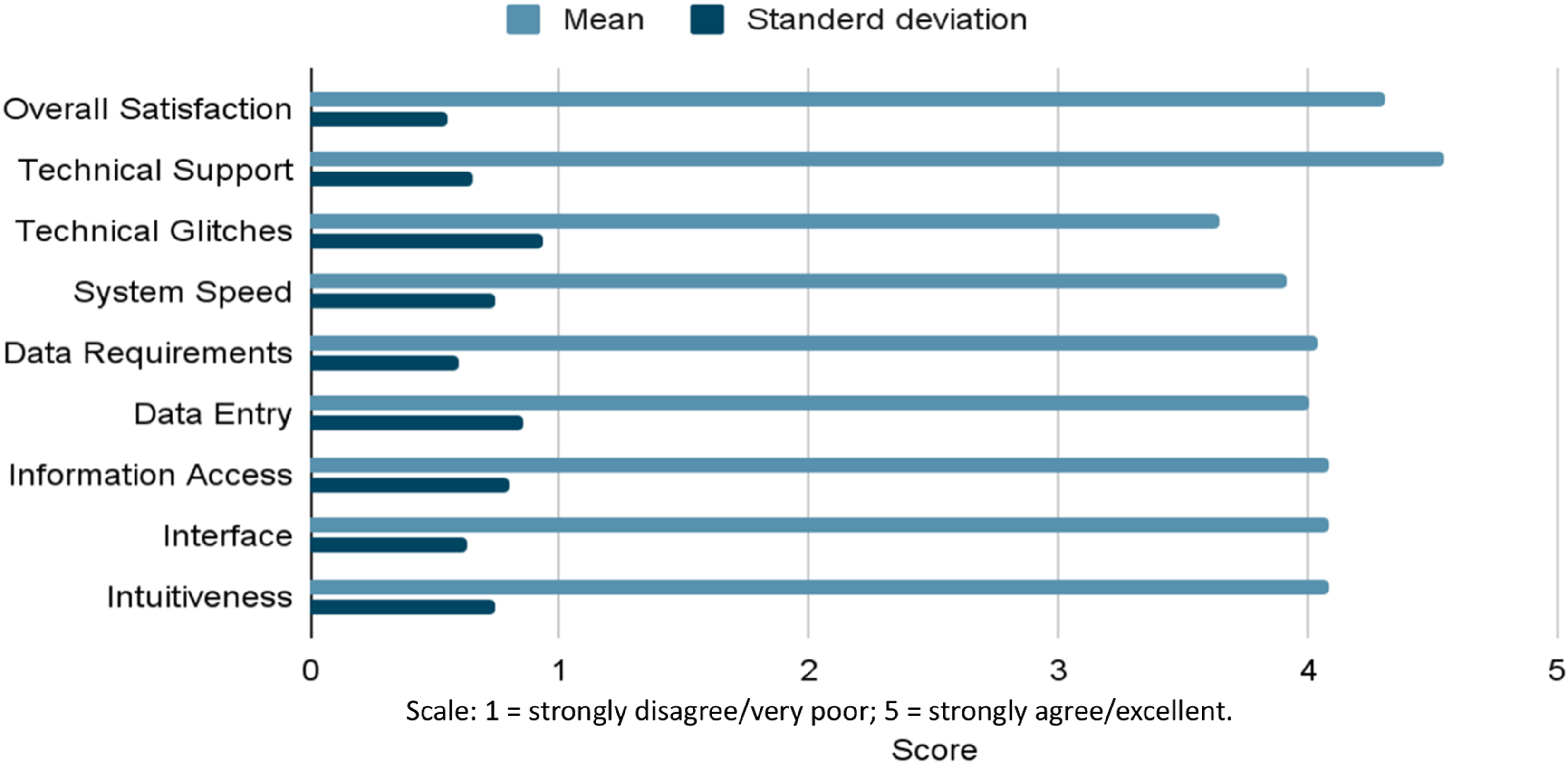
Exploratory group comparisons
Clinicians reporting training as “adequate” demonstrated higher overall satisfaction compared to those reporting “somewhat adequate” training (mean difference 0.47; 95% CI 0.04 to 0.90; Cohen’s d = 0.92; η2 = 0.17; F = 5.02; p = 0.035).
Exploratory correlations
Overall satisfaction was positively associated with: • Ease of data entry (r = 0.60; 95% CI 0.28 to 0.80; p = 0.001) • Intuitiveness (r = 0.43; 95% CI 0.05 to 0.70; p = 0.029) • Interface friendliness (r = 0.39; 95% CI 0.01 to 0.68; p = 0.047). These relationships are illustrated in Figure 4. Pearson correlation matrix illustrating associations between overall satisfaction and usability domains.

Qualitative findings
The survey generated 381 substantive free-text comments across 21 open-ended prompts. Reflexive thematic analysis identified four interconnected themes that contextualise the quantitative findings.
Theme 1: Improved information retrieval and administrative efficiency
Participants consistently described faster access to clinical data, reduced duplication, and more efficient theatre-list preparation.
“Has reduced the time to search for details in every document the patient brings.”
“Easy access to accurate patient data and interdisciplinary coordination.”
Clinicians noted that centralised digital records reduced reliance on patient-held documents and improved continuity during MDT discussions.
Theme 2: Enhanced multidisciplinary coordination
Respondents highlighted improved coordination across surgical, pathology, radiology, and MDT workflows.
“MDT discussions are smoother because all information is in one place.”
The digital documentation of MDT decisions was perceived as strengthening care continuity and reducing communication gaps.
Theme 3: Dual documentation burden during transition
Parallel maintenance of paper and electronic records was frequently cited as a source of temporary inefficiency.
“Need very smooth transition from paper-based to EHR.”
“Double work during the transition period.”
Although participants acknowledged the safety and redundancy benefits, many viewed dual documentation as the primary short-term barrier to maximising efficiency gains.
Theme 4: Infrastructure and technical optimisation needs
While overall system acceptance was high, intermittent network instability and occasional software glitches were reported.
“When there are network or system failures, unable to access the EHR.”
“Network issues and connectivity problems are delaying access.”
These challenges were generally framed as addressable through infrastructure strengthening rather than fundamental system design flaws.
Discussion
This convergent mixed-methods evaluation demonstrates that implementation of a secure, modular, cloud-based Electronic Health Record (EHR) in a high-volume tertiary surgical oncology unit in Sri Lanka was associated with significant improvements in workflow efficiency and high clinician acceptability. Quantitatively, theatre-list preparation time and biopsy-to-diagnosis intervals were significantly reduced, while qualitative findings attributed these gains to improved information visibility, reduced search burden, structured multidisciplinary documentation, and automated result notification. Together, these findings indicate that context-adapted EHR deployment can deliver measurable operational benefits even within resource-constrained and hybrid documentation environments.
Workflow efficiency in context
Systematic reviews of EHR implementation demonstrate heterogeneous impacts across healthcare settings, with the most consistent benefits observed in documentation efficiency, information retrieval, and coordination-dependent processes rather than direct clinical outcomes.2,3 More recent large-scale synthesis further highlights that these gains are strongly mediated by implementation quality—particularly workflow integration, stakeholder engagement, and training—rather than digitisation alone. 15
The observed reduction in theatre-list preparation time likely reflects decreased transcription burden, improved access to structured patient data, and elimination of delays associated with manual record retrieval. These findings align with evidence from low- and middle-income countries (LMICs), where efficiency gains are closely linked to infrastructure reliability, workforce training, and change management strategies.16–18 Similar mixed-methods evaluations from Ghana report high clinician satisfaction but persistent challenges related to system interruptions and usability, reinforcing the importance of implementation context. 18 Comparable Sri Lankan experience in outpatient services further supports the coexistence of efficiency gains with technical and workflow-related challenges during early adoption phases. 19
Impact on diagnostic timeliness and patient safety
The reduction in biopsy-to-diagnosis interval is particularly significant within oncology pathways, where delays in diagnosis can adversely affect treatment timelines and patient outcomes. 8 This improvement is likely attributable to structured investigation tracking and automated notification systems embedded within the EHR, reducing reliance on patients transporting results and enhancing clinician awareness of report availability.
Contemporary patient safety literature identifies diagnostic test-result workflows as high-risk processes prone to communication breakdowns without clear accountability and closed-loop systems. 20 Quality improvement studies demonstrate that EHR-enabled “closing the loop” mechanisms—supported by audit trails and notification systems—improve the timeliness and reliability of result follow-up. 20 The updated 2025 SAFER Guide on Test Results Reporting further emphasizes that diagnostic workflows require continuous monitoring, structured governance, and system-level safeguards to prevent missed or delayed follow-up. 21 These frameworks support interpreting our findings as indicative of improved diagnostic safety alongside operational efficiency.
Multidisciplinary coordination as a sociotechnical intervention
Digital support for multidisciplinary team (MDT) coordination represents an increasingly important focus of oncology digital transformation. Recent studies evaluating tumour board platforms and MDT digital tools demonstrate improved efficiency, reduced administrative workload, and enhanced completeness of case discussions when structured digital data are available.22,23 Our findings are consistent with this emerging evidence, suggesting that integrated EHR modules supporting theatre workflow, MDT documentation, and investigation tracking can provide measurable benefits even during early implementation.
However, qualitative findings also highlight that technological functionality alone is insufficient. Variability in clinician engagement and persistence of paper-based processes limited perceived benefit in some contexts. This aligns with sociotechnical models of EHR implementation, which emphasise that successful adoption depends on alignment between technology, workflow, organisational culture, and governance structures.3,4,17
Usability, training, and the hybrid documentation burden
High usability ratings in this study reflect the importance of intuitive system design and accessibility in driving clinician acceptance. Previous literature consistently identifies usability and perceived ease of use as major determinants of sustained EHR adoption.2,3 The observed association between training adequacy and satisfaction further reinforces the importance of structured onboarding and continuous user support. 16
A central finding was the burden associated with hybrid paper–electronic documentation. Transitional states, where electronic systems are implemented alongside mandatory paper records, are known to increase workload and reduce perceived efficiency. 4 24 In this study, national policy requirements necessitated continued paper documentation, potentially attenuating observed efficiency gains. This suggests that the measured improvements may underestimate the full impact achievable following complete digital transition. Implementation literature similarly emphasises that benefits of digitisation are often diluted until redundant processes are eliminated and workflows fully normalised.15,16
Infrastructure reliability and cloud deployment
Infrastructure limitations, including intermittent connectivity and system instability, were identified as key barriers despite overall positive usability. These challenges are well documented in LMIC EHR implementations, where technical reliability and support capacity are critical determinants of success.16–18
Cloud-based deployment was selected to improve system resilience, scalability, and accessibility while reducing dependence on local hardware infrastructure. Recent evidence indicates that cloud-based health information systems can provide robust data security when supported by encryption, role-based access control, audit logging, and governance frameworks. 25
However, security and privacy are not solely technical issues; they require strong institutional policies, credential management, and accountability mechanisms. 26 These considerations are particularly relevant in resource-limited settings where local infrastructure may be less reliable.
Alignment with LMIC evidence
The challenges observed in this study—connectivity instability, training variability, resistance to change, and hybrid documentation burden—mirror those described in LMIC EHR literature.3–5 Implementation studies in Kenya and other resource-constrained settings emphasise contextual adaptation, stakeholder engagement, and sustained technical support as essential components of success. 5 Our findings extend this literature by focusing specifically on time-sensitive oncology workflows and by integrating quantitative efficiency metrics with qualitative explanation of adoption dynamics.
Implications for LMIC implementation and national policy
The findings of this study align with broader LMIC evidence demonstrating that successful EHR implementation requires context-sensitive adaptation, sustained stakeholder engagement, and alignment with national digital health strategies.16–18 Sri Lanka’s Digital Health Blueprint outlines a vision for interoperable national EHR systems, but large-scale implementation requires locally generated evidence to inform policy and practice. 6
This study provides implementation-level evidence that modular, standards-aligned EHR systems can deliver measurable benefits in real-world clinical settings. Institution-led pilots may therefore serve as practical platforms for innovation, enabling iterative refinement and capacity building prior to national scale-up. Key implementation priorities include: • Ensuring infrastructure reliability • Providing continuous training and technical support • Transitioning away from hybrid documentation models • Strengthening governance and interoperability frameworks
Limitations and future directions
This study has several limitations. It was conducted in a single tertiary centre and evaluated early implementation outcomes over a six-month period, which may limit generalisability. The persistence of hybrid documentation may have influenced efficiency measurements, and behavioural adaptation during observation may have introduced Hawthorne effects. 27 The clinician survey was investigator-designed and not psychometrically validated; therefore, inferential findings should be interpreted as exploratory. 13
Future research should focus on multi-centre and longitudinal evaluations, including assessment of cost-effectiveness, interoperability, documentation burden, and patient-level clinical outcomes. Such studies are essential to determine whether observed efficiency gains translate into sustained system-level improvements and improved patient care.
Conclusion
This mixed-methods evaluation demonstrates that implementation of a secure, modular, cloud-based Electronic Health Record (EHR) within a high-volume surgical oncology unit in Sri Lanka was associated with significant reductions in theatre-list preparation time and biopsy-to-diagnosis interval, alongside high clinician acceptability. These efficiency gains were achieved despite operation within a hybrid paper–electronic documentation phase, suggesting that the observed improvements may represent conservative estimates of potential impact following full digital transition.
Qualitative findings underscore that technological functionality alone is insufficient to guarantee sustained benefit. Infrastructure reliability, structured and role-specific training, multidisciplinary engagement, and deliberate decommissioning of parallel paper workflows emerged as critical determinants of long-term usability and perceived value. Without coordinated attention to these sociotechnical factors, additive documentation burden and connectivity limitations may attenuate efficiency gains.
Although survey-based inferential findings are exploratory and the study was conducted in a single tertiary centre, the results provide pragmatic, implementation-level evidence that standards-aligned, context-sensitive digital transformation is feasible and operationally impactful in resource-limited oncology settings. In the absence of a fully operational nationwide EHR, interoperable institutional systems aligned with national digital health standards may serve as practical bridge solutions, generating local evidence and capacity to inform broader scale-up.
Future multi-centre and longitudinal studies should evaluate sustainability, health-economic implications, documentation burden, and downstream patient outcomes to determine whether workflow improvements translate into durable system-level and clinical benefit. These findings contribute to the growing body of LMIC digital health implementation evidence and offer actionable lessons for national digital health strategy in Sri Lanka and comparable settings.
Supplemental material
Supplemental Material - Implementing an electronic health record system in a tertiary care surgical oncology setup – A mixed method analysis
Supplemental Material for Implementing an electronic health record system in a tertiary care surgical oncology setup – A mixed method analysis by Amila Prathibha Nellihela, Shamika Kavindi Gunaratne, Vathsal Chinathaka Bandaranayake, Ruchika Nirmalie Senevirathne Jayalathge, Theekshana Pathirana, Malinga Gallala, Jayanjana Asanthi, Karunanithy Pirahanthan, Sulakshi Nikeshala Karunanayake, Abheetha Abegunasekara, Tharindu Saranga Jayasinghe, and Mahesh Senarathne in Digital Health
Footnotes
Acknowledgement
We would like to sincerely acknowledge M. Rathnayake, R.M.M. Rathnayake, A.P.G.A. Indrajith, R.P.R.V. Pathirana, Y.A.S.D. Ranaweera, R.M.N.D. Rathnayake and K.N.O. Hettige for their invaluable contributions to the development of the Electronic Health Record system used in this study.
ORCID iDs
Ethical considerations
Ethical approval was obtained from the Ethics Review Committee, Faculty of Medicine, Rajarata University (ERC/2022/32). Written informed consent was obtained from all staff participants, and de-identified patient data were analysed under institutional approval. No personally identifiable information was retained.
Author Contributions
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors and was personally funded by the principal author.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Data Availability Statement
De-identified data supporting this article are available from the corresponding author upon reasonable request.
Preprint statement
A preprint version of this manuscript was previously posted on medRxiv (DOI: 10.1101/2025.07.12.25331172); this peer-reviewed article supersedes that version.
Guarantor
Amila Prathibha Nellihela acts as the guarantor, accepting full responsibility for the conduct of the study, access to the data, and the decision to publish.
Supplemental material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.