
Abstract
Background
Digital health is growing rapidly, and older women in China who live at home, deeply influenced by traditional culture, often take on family care duties. Existing research rarely focuses on older Chinese women in home and community settings, or on the factors that affect gender equality in digital health. A comprehensive understanding of their challenges in accessing and using digital health resources is lacking.
Objective
To explore the factors influencing gender equality in digital health for community-dwelling older Chinese women.
Methods
Descriptive qualitative study; 19 participants were purposely sampled via collaboration with family doctors. Semi-structured interviews and mixed content analysis, guided by the Women and Health framework, were used.
Results
Of the 19 participants (aged 60–82 years, mean = 68.8), 16 (84%) were married, 9 (47%) had upper secondary education, and 14 (74%) lived with family. Analysis of factors influencing digital health gender equality among community-dwelling older Chinese women identified four core themes: cultural beliefs and gendered self-management behaviors; digital solutions bridging self-care and caregiving roles; preferences for person-centered digital tools and implementation processes; and a relationship-embedded digital ecology.
Conclusion
This study identifies the tension between self-care and caregiving among older Chinese women living at home and shows that digital technology can alleviate this tension. Effective digital health interventions were found to depend not only on the technological adaptability of tools but also on human-centered interaction design integrated within existing digital ecosystems. These findings have practical implications for digital health targeting community-dwelling older Chinese women, highlighting the need for tailored, age-inclusive tools that integrate self-care and caregiving needs. This advances gender equality in digital health and narrows access disparities.
Introduction
Digital health has expanded substantially amid technological innovation and accelerated healthcare digitization, offering considerable potential to improve access to care for marginalized and vulnerable populations.1,2 Notably, community-dwelling older Chinese women—an understudied group in this domain—represent a sizeable and policy-relevant cohort: adults aged 60 and above accounted for 23% of China’s total population in 2025, 3 and women constitute 51.7% of this elderly population. 4 Defined as individuals residing in their own homes (with potential access to home- and community-based services), this group is distinct from older adults in institutionalized settings (e.g., assisted living facilities, long-term care institutions). In China, where traditional gender roles remain influential, older women face unique challenges in accessing healthcare resources and securing economic stability—including socioeconomic disparities, provincial aging inequities, and the compounded burden of chronic conditions and mobility limitations. 5 These barriers not only restrict their access to tailored digital health services but also exacerbate existing health inequalities, thereby highlighting the pressing need for inclusive digital health design that explicitly addresses gender-based disparities in technology adoption and health outcomes.
Existing studies predominantly focus on the universal benefits of digital health for aging populations, overlooking how gender intersects with sociocultural norms and caregiving roles to shape access to and outcomes of these technologies. This gap highlights the urgent need for gender-responsive digital health solutions that explicitly advance equality by addressing the unique barriers faced by community-dwelling older Chinese women. Against this background, the present study addresses the following questions: (1) How do sociocultural norms and caregiving roles shape community-dwelling older Chinese women’s access to, use of, and experiences with digital health technologies? (2) What gender-responsive design principles and implementation strategies may help reduce these barriers and advance digital health equity for this group?
Digital health can be defined as “ the rational application of technology, leveraging intelligent data processing, to enhance people’s health and well-being, and optimize care for patients” 6 —a framework with multifaceted implications for older adults. A thematic synthesis of the existing literature identifies three core research streams. First, foundational enablers of digital health adoption emerge as dual-dimensional constructs encompassing individual competencies and environmental support. Existing studies suggest that older adults’ engagement with digital health technologies is shaped not only by individual digital literacy, but also by access to targeted health education and the availability of social support during adoption.7–9 In addition, prior research points to two major intervention domains with demonstrated benefits: exercise-oriented digital programs that support physical functioning, and home-based monitoring systems that facilitate chronic disease management and fall prevention.10,11 Third, technological innovation and engagement: Advanced tools such as augmented reality (AR) platforms enhance user motivation and intervention compliance, yielding measurable improvements in older adults’ physical function. 12 Collectively, these studies underscore digital health’s potential for older populations—but gaps remain in addressing gender-specific barriers faced by community-dwelling older Chinese women, particularly in tailoring interventions to their unique socioeconomic and cultural contexts.
Among these cultural influences, filial piety—a millennia-old Confucian core value in China that emphasizes intergenerational affection, respect for elders, and family obedience 13 — profoundly shapes their health behaviors and creates distinct barriers to digital health access. 14 In contemporary China, these norms frame them as primary family caregivers who often prioritize family health over their own. Aligning digital health interventions with filial piety’s family-centric care focus can address such barriers: municipal digital health initiatives reduce access disparities, 15 telemedicine mitigates care disruptions, 16 and patient-reported outcomes validate community digital health programs in managing geriatric diseases and easing their caregiving burden, 17 few explicitly integrate gender equality principles—failing to address how traditional roles amplify their technological marginalization.
Gender-specific challenges persist in digital health engagement: digital literacy directly influences older women’s ability to seek and benefit from health information, 18 yet research on community-dwelling older Chinese women remains sparse—particularly compared to high-income populations and male counterparts. Henson’s work on older Indigenous women in Australia19–21 highlights barriers to digital health uptake among marginalized female groups, but analogous research on community-dwelling older women in China is lacking.
Cultural expectations exacerbate caregiving burdens, limiting their capacity to prioritize self-care through digital tools, 22 and Sullivan 23 notes the dearth of systematic research on how digital health can advance gender equality in older women’s health. This “technological gender blindness” hinders the development of inclusive interventions. Recent scholarship underscores the imperative of embedding gender equality into digital health design and policy. 24 Frennert 25 advocates for feminist design frameworks to ensure technological advancements do not reinforce traditional gender roles.
This study adopts the Women and Health framework 22 as its theoretical lens. The framework is particularly relevant because it conceptualizes women as both users and providers of care, thereby drawing attention to their dual positioning as care recipients and caregivers. It also emphasizes how women’s health practices are embedded in broader social and cultural structures. In the context of community-dwelling older Chinese women, this framework helps explain how gendered caregiving expectations and Confucian familism may shape access to, engagement with, and benefit from digital health technologies. At the same time, the Women and Health model proposes adaptive solutions: caregiving burden visualization tools, flexible time-management features, and culturally congruent interfaces that center older women’s dual roles as caregivers and care recipients.
Methods
Study design
We adopted a descriptive qualitative design and conducted one-on-one semi-structured interviews with community-dwelling older Chinese women to explore factors influencing gender equality in their digital health.26,27 The study’s reporting is in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist 28 (Appendix B).
Participants and setting
Participants were recruited from Xianxia Community Health Service Center (CHSC), a primary healthcare facility situated in Changning District, Shanghai, China. This community-based center primarily serves the local mixed-income urban resident population, with an annual outpatient volume of approximately 45,000 visits; the socioeconomic characteristics of its catchment area are representative of Shanghai’s average urban level. Purposive sampling was used to select older women. 29 Social demographic factors, such as age, marital status, education level, and living arrangements, guided the purposeful sampling. The inclusion criteria for participants were as follows: 1) the age of the participants was above 60 years; 2) living at home; 3) the ability to communicate, give consent, and participate. The exclusion criteria were individuals: 1) suffering from serious diseases who may not complete the entire interview; or 2) without any experience of using digital technology. Participants were enrolled via a two-stage screening process to ensure study eligibility. First, family physicians at the community health service center preliminarily identified potential candidates during routine outpatient consultations by assessing age, residential status, and basic health status. Second, the research team conducted formal eligibility verification for these referred candidates—including confirming their digital health experience and completing a brief interview evaluation—before obtaining written informed consent.
Research team characteristics and reflexivity
The study team comprised six females, with two healthcare professionals (QC and WZ) and four researchers (YG, SY, NJ, and YL). The age range is from 20 to 54 years. The authors were all researchers trained in qualitative methods.
Reflexivity was discussed before interviews and during data collection and remained an ongoing consideration during analysis. Because some younger researchers could be perceived as more knowledgeable about digital technologies, we considered the possibility that this age and expertise-related power differential might shape participants’ responses. To mitigate this, interviewers began by emphasizing that participants were the experts in their own daily experiences, used non-technical and conversational language, relied on neutral prompts rather than corrective or leading responses, and allowed sufficient time for participants to describe challenges in their own terms. In addition, the research team maintained reflexive notes and discussed these in regular analytic meetings to examine how age, gender, and professional status might influence data generation and interpretation. These discussions also addressed the dual role of QC and WZ as both clinical staff and researchers, with explicit protocols in place to prevent participants from feeling pressured to participate or to provide socially desirable responses.
Interview guide
The semi-structured interview topic guide.
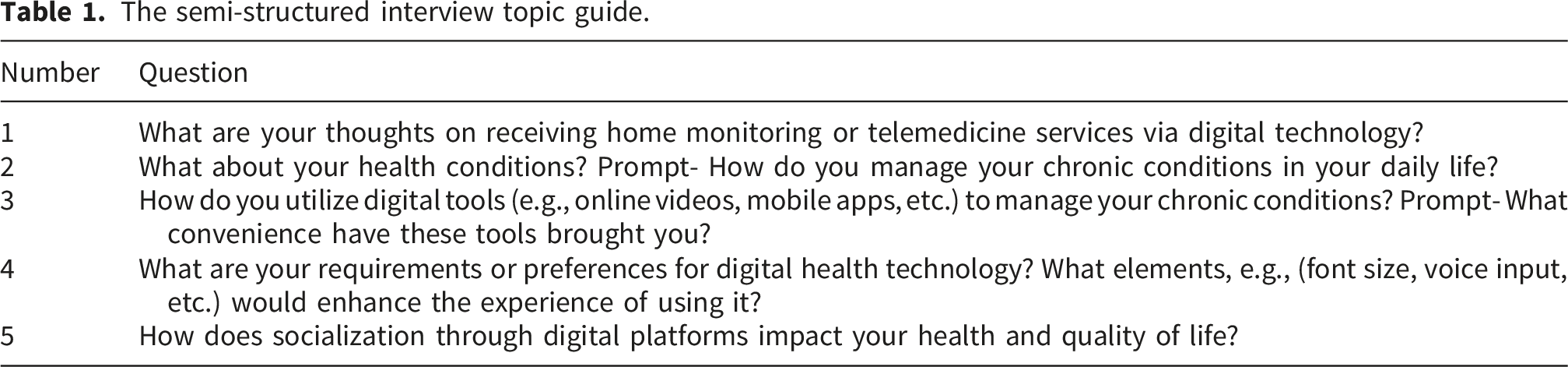
A pilot test was conducted with two community-dwelling older Chinese women to refine the interview guide; 27 key adjustments included simplifying overly technical digital health terminology and developing context-specific prompts tailored to the participants’ daily digital experiences. For example, the abstract term “digital health platforms” was replaced with the more familiar and accessible “digital tools”—a modification informed by WeChat being the most widely used digital platform in China and the primary digital tool for this cohort. 30 Additional refinements included rephrasing open-ended questions to be more conversational and concise, ensuring clarity and reducing response burden for older adult participants.
Table 1 shows the final semi-structured interview topic guide.
Data collection
Semi-structured interviews were conducted between December 2023 and January 2024 at the Xianxia Community Health Service Center in Shanghai, China. Before the interview, participants were asked to complete a paper questionnaire (Appendix A) to collect social demographic data (age, marital status, education level, 31 living arrangements) and self-rated health status (SRH). SRH was measured using a validated single-item scale: “How do you feel about your overall health, looking at the recent seven days?” with response options (very poor, poor, fair, good, very good) reverse-scored from 1 (very poor) to 5 (very good).32,33
All interviews were conducted individually in Mandarin by a single researcher, with each interviewer being one of four members of the research team (YG, SY, NJ, YL). Interviews ranged from 35 to 70 minutes, with a mean duration of 62 minutes. The 35-minute duration was limited to a pilot interview, which focused on testing the guide. The variation in interview duration was primarily due to participants’ willingness and ability to share their experiences: those with extensive digital health use were able to provide more elaborate narratives. Data collection and analysis were conducted iteratively, and sample adequacy was assessed throughout the study. While saturation is commonly used to guide sample size in qualitative research, its adequacy as a sole justification has been debated,34,35 particularly in small purposive samples. Accordingly, the final sample size was determined not only by the absence of substantially new themes in later interviews, but also by the focused study aim, the purposive recruitment of information-rich participants, and the depth of the interview data. 34 After the 15th interview, no substantially new themes relevant to the research question emerged. Four additional interviews were conducted to test the stability of the findings, and these did not materially alter the analysis. Thus, the final sample of 19 participants was considered adequate for this descriptive qualitative study. Audio-recorded interviews were transcribed verbatim by a professional transcription service provider and stored in a password-protected device.
Data analysis
To better understand the challenges and opportunities that community-dwelling Chinese older women face in digital health, we employed a hybrid content analysis approach integrating directed (deductive) content analysis and conventional (inductive) content analysis,36,37 with the analytical process visualized in Figure 1. This sequential two-phase approach ensured both alignment with existing theory and responsiveness to participants’ emergent insights: Data analytical process.
Phase 1: Directed (Deductive) Content Analysis. Guided by the Women and Health conceptual framework 22 and prior literature, researchers (YG and YL) first constructed a predefined codebook reflecting gender-specific dimensions of digital health, including categories such as “lack of digital literacy,” “barriers to accessing health information,” and “role of family support”. This deductive step anchored our analysis to established theoretical constructs, ensuring we systematically captured gender-relevant patterns. To ensure coding consistency, both researchers independently analyzed three randomly selected transcripts (n=3/19), resolving interpretation discrepancies through iterative discussions to calibrate coding criteria.
Phase 2: Conventional (Inductive) Content Analysis. Following the deductive coding phase, YG and YL conducted line-by-line inductive coding on all remaining transcripts (n=16/19). Prioritizing participants’ verbatim expressions, the researchers maintained proximity to raw data while allowing insights beyond the pre-existing framework. A representative subset of interview transcripts (n=5/16) was first independently coded by two core researchers (YG and YL), with team discussions subsequently held to resolve coding discrepancies, refine coding definitions, and develop a standardized codebook. Following the finalization of this codebook, the two researchers then independently coded all remaining interview transcripts (n=11/16) in accordance with the unified coding framework; any emergent new themes identified during this formal coding phase were collectively discussed by the full research team and integrated into the codebook prior to continued coding. Besides, we emphasized the interactions between older women and their family members 38 and healthcare providers and how these interactions influenced their digital health behaviors.
Integration, Consensus Building, and Validation. Upon completing both coding phases, the research team integrated deductively predefined codes and inductively emergent insights: codes were either mapped to broader a priori themes or retained as new sub-themes when representing theory-distinct patterns (e.g., “WeChat app preference” was categorized under the sub-theme “age-friendly design needs”). Sub-themes were iteratively refined through repeated comparison with raw data and participant quotes, ultimately coalescing into four core themes aligned with study objectives. YG and YL presented preliminary themes to the whole team, and discussions continued until a consensus was reached on theme definitions and interpretations. To enhance credibility, summaries of the identified themes were sent to participants for member checking. All data management and coding were conducted using NVivo software.
Rigor
As two researchers (QC and WZ) are family doctors, interactions with participants were minimized during recruitment and interviews to reduce potential bias. Credibility was ensured by having two researchers (YG and YL) involved in the coding and analysis of data and keeping a track record of the data collection and analysis processes. In addition, audio-recording and adequate engagement with interview transcripts and reviewing the results against the interview data helped ensure data accuracy and representation. Furthermore, all team members were involved in the discussion and interpretation of the findings.
Ethical consideration
The study was approved by the Institutional Review Boards of Fudan University School of Nursing (IRB#2023-4-7). Ethical considerations were taken into account among community-dwelling Chinese older women. For example, during the in-depth interviews with older women, researchers reminded participants that their responses were anonymous and confidential and would not be disclosed to anyone other than the interviewer, including the doctor who assisted with recruitment. In addition, the research team would emphasize that participation in the study was voluntary and would not affect their ability to access services or participate in subsequent community interventions. Before interviews, each participant was given signed informed consent after the risks and benefits, confidentiality, and withdrawal options were explained to them. In recognition of participants’ time and travel costs associated with study participation, a small non-monetary token of appreciation (a set of daily necessities including tissues and wet wipes, with a total approximate value of CNY 20/30) was provided to each participant.
Results
The participants’ general information.

All participants confirmed that the transcript summaries were accurate and requested no changes. The final four themes and ten sub-themes were: 1) Cultural beliefs and gendered self-management behaviors. 2) Digital solutions bridging self-care and caregiving roles. 3) Prefer person-centered digital solution and implementation process. 4) Relationship-embedded digital ecology.
Theme 1: Cultural beliefs and gendered self-management behaviors
Sub-theme 1. Disease stigma and communication barriers
Cultural beliefs toward disease specificity, especially some gynecological diseases (such as pelvic floor dysfunction), influence older Chinese women’s attitudes and healthcare behaviors. When disease-related symptoms occur, they may be affected by a lack of knowledge or by embarrassment about speaking up and seeking medical attention. One participant shared: “(a long time ago)…… I had a case of vaginal bleeding that I didn’t care about at first, then I fainted and realized it was a fibroid……Now I feel good.” (Participant 15)
Older women in the study expressed a significant influence from the stigma associated with gynecological diseases. Participants often felt embarrassed to discuss their conditions with their families. Shame around disclosing symptoms was pervasive: “I haven’t told my family about my condition and feel embarrassed to tell them.” (Participant 11)
Another participant felt the same way: “I don’t know how to tell my family about my illness.” (Participant 14)
Another described how they were overwhelmed by the difference between their doctors’ and traditional societal perceptions of the problem of urine leakage in older adults: “They (the doctors and the participant’s peers) said leakage is common with old age, but I feel embarrassed.” (Participant 12) Cultural cognitive biases similarly exist in other chronic conditions, such as diabetes patients said: “I don’t want to use insulin; once you start injections, it means there's no cure left, doesn’t it?” (Participant 5)
This communication barrier is particularly pronounced amid generational differences. As one arthritis sufferer described: “My daughter-in-law says it’s an old person’s ailment that doesn’t need treating, but I want to use the physiotherapy device yet fear being told I'm wasting money.” (Participant 8).
Sub-theme 2. Adaptive self-management as gendered practice
Participants’ health management practices reveal a gendered negotiation of care responsibilities. By embedding medical routines within domestic space, they transform caregiving roles into frameworks for sustaining personal health. These adaptive approaches demonstrate how women reinterpret self-management as a collective practice. One participant mentioned: “My hypertension is well controlled with medication, and has been stable for 20 years.” (Participant 3)
Rather than reflecting adherence alone, this account suggests a gendered strategy of preserving functional capacity over time so that health can be maintained without disrupting ongoing family responsibilities. Through the Women and Health lens, long-term self-management here is closely tied to women’s dual positioning as both care recipients and continuing caregivers. Another participant described integrating traditional practices like herbal foot soaks with daily exercise routines, emphasizing gradual physical activity to avoid overexertion: “I like to read Chinese medicine books and soak my feet. Then, slowly get up, do housework, and go exercise.” (Participant 7)
Some also explored alternative therapies, such as leech therapy for dizziness, while prioritizing regular movement: “I sometimes take leeches when I get dizzy... stick to walking and moving.” (Participant 14)
Participants balanced dual roles as patients and family caregivers, demonstrating exceptional adaptability. For instance, one respondent established post-dinner exercise habits to accommodate daytime caregiving responsibilities for a sick relative: “I’m used to walking and exercising after dinner... because I need to care for my sick brother during the day.” (Participant 13)
Another developed protective measure—preparing trachea medication and wearing high-necked clothing—while fulfilling daily obligations of childcare and household management: “I take care of grandchildren and cook every day. I prepare tracheal medicine and wear high-necked clothes to protect my throat.” (Participant 16)
It is particularly noteworthy that the participants transformed family caregiving responsibilities into motivation for self-care, confirming the prevailing logic. A participant said: “When I have to look after my grandchildren, I must first get my blood sugar under control.” (Participant 6).
Chronic disease management operates not through isolated medical adherence, but as a fluid integration of bodily care and social responsibility. By reframing caregiving as a motivation for self-regulation, participants transcend the self-or-other care dichotomy, positioning health maintenance as an act of relational resilience embedded in women’s daily lives.
Theme 2: Digital solutions bridging self-care and caregiving roles
Sub-theme 1. Increased time flexibility
Digital solutions bridging self-care and caregiving roles, enabling them to strike a delicate balance between meeting their health needs and fulfilling their duties as family caregivers. Some participants reported that they were required to complete a lot of housework, which created significant time constraints for self-health management. Therefore, the online video workout was popular among participants who were involved in chores because it offered ample time flexibility. For instance, one participant emphasized the convenience of online video workouts, stating: “Online video workouts are more convenient; I’m busy with household chores and need more flexibility.” (Participant 5)
Others described delayed viewing practices, with a respondent explaining and illustrating how digital content adaptability aligned with unpredictable caregiving rhythms: “It’s not realistic to do it daily. You put the video on my phone, and I’ll watch it later in the evening.” (Participant 6)
Multiple participants stressed efficiency gains from mobile-based programs, which allowed them to multitask or integrate exercise into domestic routines. One participant noted: “I have more chores, so I don’t want to continue after I have done rehabilitation twice; I want to use my phone to save time.” (Participant 9)
While another remarked: “I have a tight schedule at home, and my phone saves me time by allowing me to exercise” (Participant 14)
Digital solutions have emerged as a key buffer for older women, increasing time flexibility and enabling them to balance health needs with family responsibilities. However, such technologies are not universally effective. A participant mentioned: “I told the doctor on the phone about my chest pain, but they couldn’t check, so they just asked me to go to the hospital. It is wasting my time.” (Participant 17)
Digital solutions address the time scarcity problem and enable participants to regain control of their health narratives. This technological mediation effectively transforms structural barriers into manageable challenges, enabling participants to maintain healthy habits amid the demands of family caregiving. While these solutions enhance temporal autonomy, their limitations in acute medical scenarios highlight the need for complementary approaches in holistic health support.
Sub-theme 2. Reduced travel to healthcare
Additionally, the need to reduce travel to health-care facilities was repeatedly mentioned, especially by older women with limited mobility or who find the hospital environment stressful and inconvenient. These participants indicated that this digital solution greatly helped them access more convenient healthcare services and reduced their physical and mental burdens. For instance, one participant explicitly stated: “I prefer rehab at home; traveling to the hospital is too much of a hassle.” (Participant 3)
Another said: “I ask my doctor through my phone instead of going to the hospital.” (Participant 13)
These sentiments were echoed across demographics, with multiple respondents emphasizing that telehealth options reduced the logistical burdens of in-person care. The convenience factor emerged as particularly transformative for participants with limited mobility or those who found clinical environments distressing. As one elderly participant explained: “It’s too troublesome to go to the hospital and queue up; my phone is much easier.” (Participant 2)
Another participant with mobility impairments highlighted the accessibility advantage: “I’m old and have mobility problems; I prefer doctor visits by phone or at home.” (Participant 4)
This preference for home-based care was reinforced by existing mobile doctor services, as noted by a participant who mentioned: “There is a doctor visiting service to see the elderly; just contact them by phone.” (Participant 9)
Critically, the temporal and spatial efficiencies of digital platforms enabled participants to maintain caregiving continuity. A respondent captured this dual benefit succinctly: “I prefer using my phone for doctor visits; it’s very convenient, and I can finish my chores in the meantime.” (Participant 16).
However, digital solutions cannot replace all in-person medical visits. Sometimes participants have to go to the hospital in person, as one participant described: “My knee rehab needs the therapist to adjust my posture by hand. I might hurt myself if I do it wrong. I still have to go to the hospital for that.” (Participant 11)
Digital healthcare solutions significantly reduced travel burdens for older women, particularly those with mobility limitations, by enabling remote consultations and home-based rehabilitation. While telehealth improved accessibility and care continuity, its limitations in addressing hands-on clinical needs underscore the necessity of hybrid care models.
Theme 3: Prefer person-centered digital solution and implementation process
Preferences refer to the digital service designs desired by elderly women living at home based on their own digital literacy and usage habits. This study reveals their preferences for digital health tools.
Sub-theme 1. Simplified digital solution
Older women preferred person-centered, simplified, age-friendly digital solutions because of energy issues associated with old age. They were reluctant to learn complex technology and preferred simple, phone-based solutions. As one participant stated, reflecting a widespread reluctance to engage with complex technologies: “I don’t want to learn anything too complicated because I feel it is difficult.” (Participant 3)
This sentiment was echoed by multiple respondents who prioritized ease-of-use, with another participant noting: “I prefer simple, phone-based solutions; I don’t want trouble.” (Participant 5)
Memory constraints further reinforced this preference, as a participant remarked: “I hope it’s simpler; I can’t remember the complicated ones.” (Participant 6)
However, they expressed willingness to adopt technologies when accompanied by adequate support, as indicated by a participant who said: “Just make it simple for me on my phone... Install and show me how to use it; I’m willing to learn.” (Participant 11)
Notably, participants identified WeChat and its integrated apps as particularly effective platforms. One respondent stated: “WeChat and its apps are fine, simple, and easy for older people.” (Participant 16)
These findings suggest that leveraging familiar, widely adopted communication platforms could significantly enhance technology acceptance among older users, provided interfaces are streamlined and age-appropriate.
Sub-theme 2. Prefer an age-friendly design
Older women face various challenges when using digital services, including reading difficulties due to declining eyesight, frequent typing errors, and memory loss. In response, older people tend to prefer more age-friendly digital solutions, especially information access methods that are less taxing on the eyes, such as watching videos rather than reading articles; they also like to use voice input to avoid typing errors; and they need regular reminders to help them remember how to use digital services. One respondent noted: “Reading articles is hard; videos are easier to see.” (Participant 6)
Another mentioned: “I have bad eyes, and the small characters on my phone read uncomfortably.” (Participant 8)
Motor control issues lead to a preference for voice-activated functions. A participant explained: “I prefer voice because typing is easy to get wrong.” (Participant 11)
Additionally, memory constraints necessitated design interventions beyond interface adjustments. A respondent emphasized pointing to the critical role of proactive memory aids like notifications or tutorial refresher prompts: “I am old and have a bad memory, so I need regular reminders to use digital services.” (Participant 17)
Collectively, these insights advocate for a multi-faceted approach to age-friendly digital design that addresses sensory limitations, accommodates declining motor skills, and compensates for memory deficits.
Sub-theme 3. Self-directed use
Self-directed use refers to solutions that older women use only when necessary. Participants exhibited clear preferences for autonomous scheduling and content curation. One respondent asserted, illustrating their capacity to prioritize wellness activities independently: “I don’t need to be scheduled; I know when to exercise myself.” (Participant 5)
This autonomy extended to learning modalities, as another participant noted, emphasizing asynchronous access’s alignment with personal rhythms: “The videos are available, and I can follow them when I’m free.” (Participant 4)
Information consumption patterns revealed selective engagement strategies. A participant mentioned: “I watch videos to learn simple movements, and don't want long texts.” (Participant 1)
Digital literacy development was further evident in proactive information management, with a respondent declaring: “Too many messages bother me; I will delete them.” (Participant 11)
These findings emphasize the empowering nature of self-directed digital engagement, underscoring the importance of flexible, user-centric digital platforms.
Theme 4: Relationship-embedded digital ecology
This digital ecosystem facilitates older women’s healthcare access. While barriers persist in adopting health apps and online consultations, the study reveals how relational networks—including peer communities, family collaborations, and remote medical systems—shape their digital health experiences.
Sub-theme 1. Online peer support
The findings reveal that older women’s digital engagement is deeply embedded within their social networks, functioning as critical infrastructure for peer support and family connectivity. One participant explained: “My friends help me when I need it, and I contact them on WeChat.” (Participant 1)
This reflects the gendered value of social connection in self-management: older women rely on peer networks for support, and digital tools enable them to maintain these bonds while fulfilling caregiving roles. As one participant put it: “I often call and chat with my colleagues and friends...... I also organize gatherings to talk about what's in our hearts.” (Participant 3)
Organizing gatherings and maintaining communication reflects women’s gendered role, extending this role into the digital space. Digital tools do not replace offline relationships but strengthen them. A participant emphasized this social-digital synergy: “I have good relationships with the elderly in the community and often call and chat on WeChat.” (Participant 5)
This synergy is distinctly gendered: older women use digital tools to nurture relationships, mirroring their role as relationship maintainers.
Sub-theme 2. Enhanced remote family doctor support
Enhancing remote family doctor support is a viable solution to the issue of older women’s hesitancy to visit hospitals due to inconvenience of travel. Participants in recent discussions have overwhelmingly expressed a desire for more accessible healthcare services to be conducted via phone or digital platforms. One participant stating: “I wish I could get prescribed medication via my phone instead of going to the community clinic.” (Participant 16)
This preference reflects a gendered calculation: remote care eliminates the need to sacrifice family care for medical visits, aligning with women’s prioritization of their caregiving duties. This aligns with existing care models as noted by another participant: “My family doctor calls and visits to give care and provide medication monthly.” (Participant 1)
The demand for flexible service modalities extends to home visits or teleconsultations, particularly for those with severe mobility impairments: “We're too old to walk, so we want doctors to visit or consult via phone.” (Participant 4)
Monthly check-ins cater to gendered needs by providing consistent medical support without in-person visits, enabling women to maintain caregiving while managing their health. Digital platforms also expand access to medical information, as a participant described using TikTok: “There are doctors who explain on TikTok. I check it every day and compare different opinions.” (Participant 9)
Using social platforms to access medical information reflects a gendered approach to health-seeking: older women prioritize accessible, relatable content that can be consumed while multitasking. This complements remote doctor support, creating a more comprehensive digital health ecosystem.
Sub-theme 3. Empowered family monitoring
Family members actively participate in health monitoring for community-dwelling older Chinese women. This collaboration ensures their care, boosts their empowerment, as one participant noted: “My daughter reminds me to eat less salty and spicy food, and my partner cooks light meals.” (Participant 15)
This familial engagement embodies gendered care reciprocity, enabling lifelong caregivers to access reciprocal support through family-facilitated health adherence. Beyond care coordination, family involvement extends to environmental adaptations, as one participant mentioned: “My doctor told me not to squat more, so my daughter bought an automatic sweeper.” (Participant 19)
This adaptation translates medical advice into practical support, enabling older women to maintain caregiving roles while adhering to health guidelines. Family members also help bridge the digital divide, as one participant stated: “I can learn to use digital services, and my daughter helps when needed.” (Participant 6)
This reliance on female family members mirrors traditional mother-daughter caregiving dynamics, with support characterized by care and guidance. This familial support is key to enabling older women to access digital health tools, reinforcing their autonomy and alignment with their gendered roles.
These findings collectively depict a care ecosystem where digital tools gain meaning through social entanglement. Peer networks provide emotional scaffolding, telemedicine reconfigures institutional trust, and family collaborations translate medical advice into lived practices.
Figure 2 shows the themes and subthemes. The summary table of the correspondence between topics and participants’ quotations is provided in Appendix C. Themes and subthemes. Notes: The colored sections represent the emerging themes and subthemes, while the gray sections illustrate the simplified conceptual framework of Women and Health.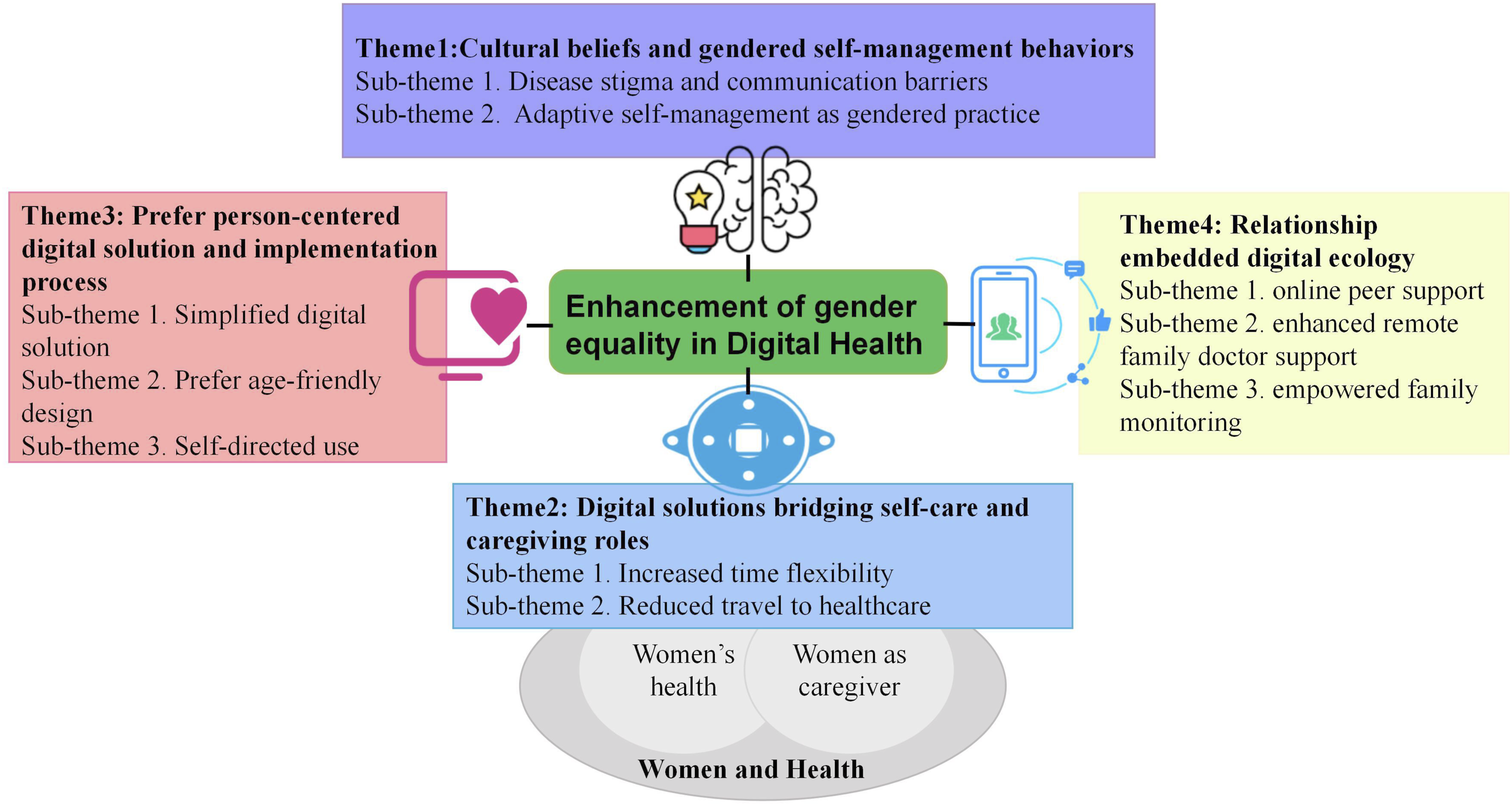
Discussion
This study conducted in-depth interviews with 19 community-dwelling older women aged 60–82 years (mean age = 68.8 years); 84% were married, 47% had upper secondary education, 74% lived with family, and 42% self-rated their health as average. Four core themes were identified: cultural beliefs and gendered self-management practices; digital health tools that bridge self-care and caregiving roles; preferences for person-centered digital health solutions and their implementation pathways; and a relationship-embedded digital health ecosystem. These findings elucidate the gendered digital health experiences of older women, characterized by dual-role conflicts, the adoption of adaptive technology, and the digital reconfiguration of social support networks.
Digital health gender disparities: Older women’s dual role conflicts
This study reveals that community-dwelling older Chinese women navigate a fundamental tension between self-care needs and caregiving responsibilities, and digital health technologies offer a crucial, though incomplete, solution. The dual role of caregiver and care recipient inherent in this population is shaped by gendered social norms and aging-related health constraints, which directly influence their digital health experiences. Our findings show that older women are deeply entrenched in family caregiving roles. Many balance childcare, household management, and care for sick relatives, while simultaneously coping with chronic conditions such as hypertension, diabetes, and gynecological diseases. Chronic illnesses and mobility issues not only limit older women’s outdoor healthcare access but also worsen their self-care capacity, creating a vicious circle where age-related bodily decline increases the risk of severe conditions (e.g., arthritis, diabetes), making effective self-care under constraints an urgent need. This role conflict manifests primarily in time and energy allocation, as participants consistently prioritize family needs over their own health management, a pattern rooted in traditional gender expectations that place women as primary family caregivers. 39
Disease stigma further exacerbates this tension, particularly for gynecological conditions. Gynecological conditions trigger a series of physical and psychological problems, such as frequent urine loss and leakage, which can cause patients to feel a sense of shame, exacerbating their vulnerability. Participants reported embarrassment in disclosing symptoms to family members or seeking medical care, reflecting cultural cognitive biases that frame specific women-specific health issues as shameful or taboo. Research consistent with our findings indicates that women with more severe pelvic floor disorders often experience greater psychological distress, 40 which compounds the communication barriers they face. The participants avoided discussing urine leakage with family despite significant distress. This communication barrier not only hinders self-care but also limits the potential for family support in accessing digital health resources. Together, these findings illustrate how gendered social structures and cultural norms intersect with aging to create unique barriers to digital health engagement for older women.
Digital solutions: Enhancing healthcare access for older women
Findings show that digital solutions buffer older Chinese women’s health-caregiving conflicts and improve their access to healthcare. Smartphone-based digital health tools addressed two key barriers: time scarcity and travel burden. Participants valued the time flexibility of digital interventions. For instance, many used mobile devices to access rehabilitation guidance after completing household chores or caregiving tasks, eliminating the need to adhere to fixed clinic hours. Additionally, these digital solutions make accessing healthcare services more convenient, reducing the physical and mental stress of traveling to healthcare facilities. Remote consultations via phone or WeChat enabled participants to seek medical advice, renew prescriptions, and access health information. Besides, our findings identify that acute hands-on care needs cannot be replaced by digital tools, highlighting the universal need for hybrid care models that integrate digital convenience with in-person clinical support. This principle critical to equitable, person-centered care.
As all participants in this study were recruited from an urban setting, our data do not allow direct examination of rural–urban differences in digital health access or use. We therefore treat the rural–urban digital divide as a contextual limitation affecting the transferability of our findings rather than as an empirical theme arising from the interviews. Future research should include rural older women to examine how infrastructural constraints, digital access, and service availability may shape digital health engagement in different contexts. 41
Digital platforms: Bridging mental health gaps
This study highlights that digital platforms help bridge mental health gaps among community-dwelling older Chinese women, primarily by building relationship-embedded digital ecosystems that expand their social support networks. Older women experience psychological distress stemming from age-related health declines and role transitions.42,43 Traditional gender norms that prioritize their caregiving roles over personal mental health needs further reinforce gender inequities in health access. It is worth noting that the quality of family relationships can similarly affect the mental health of older people. 44 In particular, when living with their children, how they interact can significantly impact their psychological well-being. 45
Digital tools mitigate these disparities by strengthening relationship-embedded networks, empowering women to exercise health agency, and advancing gender equality in geriatric care. Centered on WeChat, these digital ecosystems enhance peer connections, remote clinician interactions, and family health monitoring. Older women have access to a vast array of information, including nutrition, mental health, and disease prevention. Online forums and support groups allow people experiencing similar health challenges to connect, providing mutual encouragement and advice. Furthermore, doctors, dietitians, and fitness trainers use digital platforms such as WeChat—China’s dominant multifunctional digital platform—to share knowledge, conduct consultations, and provide personalized guidance. Unlike many Western digital health tools that exist as standalone applications, WeChat’s integration of social, health, and daily life functions within a single interface drastically reduces barriers to access for digitally less literate older women. This culturally adapted design aligns with core gender equality goals by partially addressing the historical neglect of older women’s unique experiences and needs in digital health development.
In addition, this study highlights that participants living with family received greater digital health support, which alleviated the gendered care burden of prioritizing others’ health over their own self-care. In contrast, women living alone relied on digital peer groups for such mental health support, challenging the gendered stereotype that familial care alone suffices to meet older women’s comprehensive mental health needs. Digital platforms transform how women connect with their communities, enabling instant cross-regional communication to provide essential emotional support. 46
Educational background as a cross-cutting factor in digital health engagement
Educational background appeared to shape how participants engaged with digital health resources. Women with higher levels of formal education tended to describe more independent information-seeking practices and greater confidence in navigating digital platforms, whereas those with less educational experience more often relied on family members, community workers, or simplified modes of communication to access digital health support. In this sense, educational background functioned as a cross-cutting factor influencing digital self-efficacy, information appraisal, and preferences for how digital health content should be delivered. This suggests that digital health implementation should not assume a uniform user profile, but should instead provide differentiated support, including plain-language content, voice- or video-based guidance, and community-based assistance for users who may find text-heavy or multi-step digital systems difficult to navigate.
Implications
This study underscores the need to address the unique digital healthcare needs of older female caregivers—one that acknowledges both the transformative potential of digital tools and the well-documented risk of widening existing disparities. 47 While digital care can enhance healthcare accessibility for many community-dwelling older women, it cannot universally resolve their health challenges, particularly for underserved subgroups (e.g., rural residents, those with limited digital literacy) who continue to face structural barriers to digital health access as identified in our earlier analysis and corroborated by extant literature. 47 This nuance warrants tempering broader recommendations for integrating digital health into health policy with a commitment to mitigating disparities and ensuring that no subgroup is left behind.
Guided by our findings, targeted strategies across key domains are proposed as follows: (a) Clinical Practice: Develop hybrid care protocols that integrate telehealth services with in-person hands-on therapy, particularly for mobility-dependent conditions (e.g., knee rehabilitation) where digital tools cannot replace clinical physical intervention. (b) Policy: Invest in targeted rural digital health literacy training programs while preserving and strengthening traditional in-person healthcare pathways, to prevent the exacerbation of rural-urban health equity gaps. Additionally, fund ongoing digital health support initiatives for older women to build sustained confidence in tool utilization, empowering them to balance their health and family caregiving roles. (c) Technology design should prioritize integration with dominant, familiar, multifunctional platforms already used in the daily lives of the target population, rather than relying solely on standalone digital health applications that may create additional adoption barriers. In the Chinese context, this may include platforms such as WeChat; more broadly, the principle is to build on familiar digital ecosystems that older women already trust and know how to use. (d) Future Research: Explore cross-cultural variations in family-mediated digital health use among older female caregivers, and further investigate how gendered caregiving norms shape digital health engagement across different socioeconomic and regional contexts.
Strengths and limitations
This study is among the few to specifically explore gender equality in digital health among community-dwelling older women. While prior research has examined gender equality in digital health for older adults more broadly, 48 most studies have not adopted a gendered lens that focuses on the distinct experiences of older women, particularly Chinese older women. Our study fills this gap by innovatively investigating this topic through a gender-responsive framework, shedding light on WeChat’s culturally specific integrated ecosystem (encompassing communication, payment, and health services) as a key platform shaping digital health engagement. By analyzing women’s dual roles as self-carers and caregivers, this research advances understanding of digital health equity within the structural determinants outlined in the Sustainable Development Goals. 49
There are also limitations to this study. First, its qualitative data may be susceptible to response bias: participants might modify their responses, as some family doctors were part of the research team. Although this bias was mitigated by informing participants that the doctors were not involved in data collection and by clarifying that responses would not affect participants’ access to healthcare, we acknowledge that healthcare professionals’ positional authority may still influence participants. Second, while purposive sampling is well-suited for qualitative exploration of targeted populations, it inherently carries limitations—including non-transferability of findings and potential selection bias, stemming from non-random participant selection. 50 A major limitation of this study is that women with no prior experience using digital technology were excluded from participation. As a result, the study does not capture the perspectives of the most digitally marginalized older women, whose barriers to digital health access may be more severe or qualitatively different from those represented here. The findings should therefore be interpreted as reflecting the experiences of community-dwelling older women with at least some level of digital exposure, rather than the full spectrum of digital exclusion. This sampling constraint may have led us to underestimate the depth of access barriers faced by absolute non-users. Third, this study serves as a starting point for understanding gender equality from the perspectives of older females. Given the pluralism of gender equality, we encourage future studies to triangulate data, such as by comparing male peers, intersectional factors, or provider viewpoints, to deepen understanding and support causal inferences. Fourth, we acknowledge that the COVID-19 pandemic had formally ended in China at the study’s onset (data collection: December 2023–January 2024), with no direct impact on our data collection. However, the widespread digitalization of healthcare services and the increased societal acceptance of digital health tools,, have likely increased our participants’ baseline willingness to engage with such tools. It should be taken into account when interpreting the study’s results and evidence.
Conclusions
This study extends the literature on aging and digital health by showing that, for community-dwelling older Chinese women, digital health engagement is shaped not only by age-related usability concerns but also by gendered caregiving responsibilities, family relationships, and socio-cultural expectations. By foregrounding women’s dual positioning as care recipients and caregivers, the study identifies context-sensitive principles for the design and implementation of digital health services that are more responsive to the lived realities of this population.
Supplemental material
Supplemental material - Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women
Supplemental material for Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women by Yuan Gao, Sai Yang, Ning Jiang, Weiwei Zhou, Qi Chu and Yan Liang in Digital Health.
Supplemental material
Supplemental material - Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women
Supplemental material for Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women by Yuan Gao, Sai Yang, Ning Jiang, Weiwei Zhou, Qi Chu and Yan Liang in Digital Health.
Supplemental material
Supplemental material - Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women
Supplemental material for Exploring gender equality in digital health: A qualitative study of community-dwelling older Chinese women by Yuan Gao, Sai Yang, Ning Jiang, Weiwei Zhou, Qi Chu and Yan Liang in Digital Health.
Footnotes
Acknowledgements
The authors wish to thank the study participants for their valuable contributions to this research. We also acknowledge the support of the teams at the Xianxia Community Health Service Center in Shanghai, China, for their assistance with data collection and study implementation. This work is independent research and does not represent the views of any affiliated organizations.
Ethical considerations
The study was approved by the Institutional Review Boards of Fudan University School of Nursing (IRB#2023-4-7).
Consent to participate
Written informed consent was obtained by each participant at the beginning of the interview.
Consent for publication
Informed consent for the publication of all study-related data, including de-identified participant information and study findings, was obtained from all participants before study commencement. No identifiable personal information of participants will be disclosed in this publication.
Author contributions
YG and YL contributed to the study design. QC and WZ contributed to conducting recruitment. YG, SY, NJ, and YL contributed to the interview. YG and YL contributed to data analysis and the original draft. All authors contributed to the critical revision of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant number 72304071), Fudan University School of Nursing Research Fund (grant number FNF202356), Shanghai Municipal Health Commission of Changning District (grant number 20234Y028), and the Xi Yuan Program of Fudan University (grant number 24663).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors declare that they have no competing interests.
Data Availability Statement
The datasets generated during and analyzed during the current study are not publicly available, as respondents were assured that the raw data would remain confidential and not be shared. The general information sheet and an excerpt from the codebook are provided in supporting files available for download along with the published manuscript.
Guarantor
Yan Liang (YL) is the Data Guarantor for this study and takes full public responsibility for the integrity, accuracy, and completeness of all study data, including data collection, curation, analysis, and reporting.
Supplemental material
Supplemental material for this article is available online.