
Abstract
Objective
This study aims to map and visualize global research trends related to bipolar disorder (BD), with a focus on artificial intelligence (AI)-driven diagnosis and digital psychiatry from 2000 to 2025.
Methods
A bibliometric analysis was conducted using publications retrieved from Web of Science, Scopus, and PubMed, covering the period from January 1, 2000, to June 30, 2025. All data were extracted from databases at the time of search in mid-2025, and no future or projected data were included. After deduplication and data cleaning, 4,753 relevant articles were included. VOSviewer was utilized to perform co-authorship, keyword co-occurrence, and bibliographic coupling network analysis. Descriptive statistics, including annual publication trends, authorship patterns, and institutional contributions, were analyzed using Excel Pivot Tables.
Results
Scientific output in this field has grown significantly since 2015, with the United States (n=1850), United Kingdom (n=750), and China (n=620) leading in publications. Harvard University emerged as the most prolific institution. Author collaboration networks identified Eduard Vieta and Lars Vedel Kessing as key contributors. Keyword analysis revealed four dominant clusters: AI/machine learning, clinical diagnosis and biomarkers, cognitive function and quality of life, and digital interventions via smartphones and wearables. Journals such as Journal of Affective Disorders and JMIR Mental Health are central to recent literature. However, global collaboration remains limited, and the integration of digital phenotyping with biological data is still in early stages.
Conclusion
Research in BD is shifting toward AI-enabled and digital mental health approaches. Future studies should enhance interdisciplinary collaboration, focus on multimodal data integration, and promote equitable global access to digital psychiatric tools.
Keywords
Introduction
Bipolar disorder (BD) is a severe, chronic, and recurrent mental health condition characterized by alternating episodes of mania and depression, leading to substantial impairments in functioning and quality of life.1,2 Globally, BD imposes a significant burden on patients, families, and healthcare systems due to its high prevalence, frequent relapses, and associated comorbidities.3,4 The neurobiological underpinnings of BD are complex and involve genetic, neurochemical, and structural brain alterations, making its management challenging.5,6
In recent years, digital health technologies have emerged as promising tools in psychiatric care, offering novel ways to monitor, assess, and manage BD remotely and in real time.7–9 In this study, “digital psychiatry” refers to the integration of digital technologies such as mobile health applications, wearable devices, and telepsychiatry tools for the assessment, treatment, and management of psychiatric disorders, including bipolar disorder. “Artificial intelligence” (AI), on the other hand, refers to the use of machine learning algorithms and data-driven models to predict, diagnose, and optimize treatment strategies based on patient data. While these two fields overlap, they are distinct: not all digital psychiatry studies necessarily involve AI-driven approaches, and AI can be applied to a range of mental health disorders beyond those studied in digital psychiatry. Understanding this distinction is critical for interpreting the findings of this review, as it provides clarity on the scope and focus of the research covered. Digital phenotyping, defined as the moment-by-moment quantification of the individual-level human phenotype using data from personal digital devices, provides new insights into behavioral patterns relevant to BD.10–12 Wearable devices and smartphone-based applications can track physiological signals, sleep, circadian rhythms, social interaction, and mood states, contributing to more precise diagnosis and personalized treatment plans.3,13–16 For instance, web-based cognitive assessments 6 and acoustic or facial feature analysis using machine learning algorithms have shown potential in psychiatric evaluations.8,17
Artificial intelligence (AI) is revolutionizing the landscape of mental health care by enabling advanced data processing, pattern recognition, and predictive analytics.18–20 Machine learning (ML) techniques are increasingly applied to detect mood shifts, predict relapses, and assist in differential diagnoses, improving both accuracy and timeliness in BD management.21–23 Systems like MONARCA and MoodSensing exemplify AI-integrated mobile health interventions designed specifically for BD.19,23–26 These technologies support self-monitoring, reduce symptom fluctuations, and enhance patient engagement.3,11,27
Despite these advancements, several gaps and challenges remain. Issues such as user adherence to digital interventions,28–31 privacy concerns, 32 limited integration of AI with clinical endophenotypes, 3 and the need for tailored solutions across different illness stages 7 are critical barriers to full-scale implementation.33,34 Furthermore, while AI has been applied to related disorders such as depression and anxiety, 35 its specific role in BD requires further investigation.21,36 Current literature highlights the importance of real-time monitoring,37,38 social connectivity analysis, 39 and multimodal data integration using smartphones and wearable devices.10,40 However, there is a need for comprehensive mapping of how AI technologies have been adopted in BD care, particularly in diagnosis, treatment monitoring, and prediction of disease trajectories.41–45
Additionally, the potential of AI in managing comorbid conditions such as borderline personality disorder alongside BD is gaining attention, with ML models showing promising diagnostic capabilities.46,47 The integration of actigraphy for rest-activity cycle disruptions, 48 peer-supported interventions for older adults, 49 and telemedicine solutions for rural populations 50 further broaden the scope of digital health applications in BD. Nevertheless, concerns about ethical considerations, data security, and algorithmic biases continue to fuel ongoing debates.33,51
Given this evolving landscape, bibliometric analyses offer a powerful approach to systematically evaluate research trends, identify knowledge gaps, and inform future directions.35,51–53 Bibliometric studies in AI and mental health reveal exponential growth in publications, particularly in machine learning and digital health interventions.52,53 However, a focused analysis on AI applications in BD, encompassing diagnosis, monitoring, and treatment, is still lacking.
This study aims to conduct a comprehensive bibliometric and visualized analysis of the use of artificial intelligence and digital technologies in bipolar disorder, mapping global research trends, collaborations, and technological advances. By synthesizing existing knowledge and identifying research gaps, this work provides actionable insights for clinicians, researchers, and technology developers in the field of digital psychiatry and AI-based mental health care.
Method
This bibliometric analysis was conducted using three major academic databases: ISI Web of Science, Scopus, and PubMed. The search period covered publications from January 2000 to June 2025, ensuring the inclusion of relevant scientific literature over the past two and a half decades.
The search strategy was developed based on predefined keywords related to bipolar disorder, digital psychiatry, and artificial intelligence. The full search strings used in each database were as follows:
These refined search strings were designed to maximize both sensitivity and specificity across databases and ensure reproducibility.
In VOSviewer, the following parameters were used: • Minimum occurrences of keywords: 5 • Threshold for co-authorship links: 2 • Minimum citation count for bibliographic coupling: 20.
To reduce potential bias and increase the accuracy of data collection, the search strategy was iteratively refined. Two independent researchers reviewed and validated the search process to confirm the consistency and reproducibility of the methodology.
During data extraction, an evidence hierarchy was applied to contextualize the strength of the mapped literature. Studies were categorized into randomized controlled trials, prospective or well-designed observational studies, and exploratory or methodological contributions. This hierarchy served as a pragmatic indicator of evidence maturity rather than a formal quality appraisal, as risk-of-bias assessment is not typically feasible within large-scale bibliometric analyses. The approach allowed differentiation between publication growth and methodological advancement across the field.
Inclusion and exclusion criteria
Publications were included if they explicitly addressed bipolar disorder within the broader domains of digital psychiatry, artificial intelligence, or technology-enhanced mental health research. Eligible studies encompassed research on telepsychiatry, mobile health applications, digital biomarkers, digital phenotyping, passive sensing technologies, AI-based diagnostic or predictive models, machine-learning–driven analytics, and digital platforms designed for clinical management, monitoring, or relapse prediction in bipolar disorder.
To strengthen the methodological rigor of the review, each publication was screened not only for topical relevance but also for extractable study design information.
Studies were therefore included only when metadata allowed classification into a recognizable design category (e.g., randomized controlled trials, non-randomized interventions, observational studies, cross-sectional studies, case–control studies, methodological/algorithmic papers, systematic reviews/meta-analyses, or case reports). Publications lacking sufficient information to determine study design were retained for bibliometric mapping but flagged for limited interpretability in the level-of-evidence assessment.
To enable differentiation between publication volume and evidence robustness, an evidence hierarchy framework was applied based on study design classification. Randomized controlled trials were considered high-level evidence, prospective and well-designed observational studies were categorized as moderate-level evidence, while retrospective analyses, methodological or algorithm-development studies, bibliometric investigations, narrative reviews, and case reports were classified as low-level evidence. This hierarchy was used as a pragmatic proxy for methodological maturity across the literature rather than as a formal risk-of-bias or quality appraisal. Although this hierarchy does not replace formal risk-of-bias assessment or guideline-based evidence grading (e.g., GRADE), it provides a structured approximation of methodological maturity within large-scale bibliometric datasets where individual study appraisal is not feasible.
Studies were excluded if they did not relate to the core research themes, represented duplicate entries, or consisted of non-research material such as conference abstracts, editorial pieces, letters, commentaries, or general news items. Records with incomplete bibliographic metadata, such as missing author information, institutional affiliation, reference lists, or journal identifiers, were removed when these gaps prevented reliable integration into citation, co-authorship, or co-occurrence networks.
Hyper-authorship publications (i.e.,records with more than 100 authors) were excluded to avoid artificial inflation of collaboration metrics and distortion of co-authorship network structures.
(i.e.,records with more than 100 authors) were excluded. These records typically originate from large scientific consortia, particularly in genetics, neuroimaging, or multi-site clinical trials, and their inclusion can artificially inflate collaboration metrics and distort co-authorship network structures. Their exclusion reduces the risk of inflated degree centrality and improves the interpretability of typical collaboration patterns within the field. Nevertheless, we acknowledge that removing such records may underrepresent the contribution of large international consortia to the development of digital mental health research.
All retrieved records underwent a rigorous deduplication and data-cleaning procedure
Finally, Because early-period records (2000–2010) often contained sparse metadata, additional filtering was applied to minimize temporal noise and reduce statistical volatility in early-year trend analyses.
Data analysis and bibliometric tools
The bibliometric analysis was conducted using VOSviewer (version 1.6.20), a specialized software for constructing and visualizing scientific networks. Multiple mapping approaches were applied to examine the structure of the research field. Keyword co-occurrence analysis was performed to identify the frequency and co-occurrence of terms, revealing conceptual linkages and emerging research themes. Density visualization maps were generated to highlight thematic concentrations, illustrating areas with high levels of scientific output in bipolar disorder and digital psychiatry.
Co-authorship networks were constructed at both the author and country levels to assess collaborative patterns and international research partnerships. Additionally, organizational collaboration maps were generated to evaluate institutional affiliations and partnerships within the field.
Bibliographic coupling analysis was conducted at two levels. At the article level, this method assessed shared references among individual publications to identify clusters of closely related studies. At the journal level, bibliographic coupling was used to map connections between academic journals based on common citations, providing insights into interdisciplinary linkages and journal influence within the research ecosystem.
Descriptive statistical analysis
In addition to network analysis, descriptive statistical analyses were carried out using Pivot Tables in Microsoft Excel. These analyses included the evaluation of publication distributions by author, country, journal, and year of publication. The annual trend of scientific production was also assessed to capture the temporal dynamics and growth trajectory of research related to bipolar disorder, digital psychiatry, and AI integration.
Content analysis
To complement the quantitative findings, a manual content analysis of key publications within the identified clusters was conducted. This qualitative step provided a deeper understanding of the research landscape, allowing for a nuanced interpretation of the bibliometric patterns. The manual review of core articles helped contextualize the thematic developments and emerging trends revealed through the bibliometric mapping.
Results
A total of 4,753 articles related to bipolar disorder, digital psychiatry, and artificial intelligence were retrieved from Web of Science, Scopus, and PubMed for the period 2000 to 2025. The collected data were analyzed using VOSviewer (version 1.6.20). This software enabled a comprehensive analysis of the scientific structure, including keyword co-occurrence mapping, author and country collaboration networks, and bibliographic coupling.
Scientific collaboration analysis
Country collaboration network
Top 10 countries in scientific output on bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

As shown in Figure 1, the annual number of publications increased steadily from 2000 onward, with a marked acceleration after 2015. To complement these descriptive trends, Table 2 provides a breakdown of study design types across the full dataset. Methodological and AI/ML model development studies represent the largest proportion, followed by observational and review articles, while RCTs account for a comparatively small share of the evidence base. To illustrate how these study designs evolved over time, Figure 1 presents their temporal distribution using a three-year centered moving average. The figure shows rapid growth in methodological and observational studies after 2015, whereas RCTs increased more gradually and remained limited throughout the period. These patterns indicate that the expansion of the field has been driven primarily by technology-focused and data-driven research, with slower development of high-level clinical trial evidence. When interpreted using the applied evidence hierarchy, the majority of publications correspond to low- and moderate-level evidence categories, whereas high-level evidence remains comparatively limited. Based on the applied evidence hierarchy, 50.3% of publications were categorized as low-level evidence, primarily including methodological studies, review articles, and case reports. Moderate-level evidence, mainly observational studies, accounted for 37.8% of the literature, whereas randomized controlled trials representing high-level evidence constituted only 11.9% of the included publications. These findings indicate that although publication volume has expanded substantially, the growth of higher-level clinical evidence has progressed more slowly. This imbalance has important methodological implications. The predominance of exploratory and technology-development studies suggests that bibliometric growth should be interpreted as an indicator of innovation activity rather than evidence consolidation. Consequently, the field may be advancing conceptually faster than it is progressing in clinically validated implementation, highlighting the need for longitudinal trials, real-world validation studies, and stronger translational research pathways. Consequently, bibliometric growth in this field should be interpreted primarily as an expansion of exploratory innovation capacity rather than definitive evidence consolidation. Temporal trend of study designs (2000–2025). Study design distribution (2000–2025).

As shown in Figure 2, the scientific collaboration network among countries. In this network, the United States is positioned at the center and forms the largest node, reflecting both the highest level of scientific output and the broadest scope of international collaborations. Following the United States, countries such as the United Kingdom, Germany, China, Canada, Australia, Spain, Italy, France, and Denmark play prominent roles in international scientific collaboration within this field. Country collaboration network based on article co-authorship.
The growth trend in countries’ contributions indicates that during the period from 2000 to 2009, the primary focus of scientific production and collaboration was concentrated in North America and Western Europe. From 2010 to 2019, the share of Asian countries, particularly China and South Korea, increased significantly. In the period from 2020 to 2025, the collaboration network expanded further; however, developed countries, especially the United States and European nations, still account for the majority of scientific production and collaboration.
On the other hand, the scientific gap between different regions of the world remains evident. Countries in the Middle East, Africa, and parts of Latin America are positioned at the margins of this network and exhibit limited levels of international collaboration. This underscores the need for policy development and strategic planning to enhance global scientific collaboration and reduce inequalities in knowledge production.
Organizational collaboration network
Top 10 institutions and universities in scientific output on bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

As shown in Figure 3, the organizational and institutional collaboration network in the field of bipolar disorder, digital psychiatry, and artificial intelligence. In this network, Harvard University and Stanford University are positioned at the center of the red cluster, indicating their pivotal role in scientific collaboration. The University of California campuses and the National Institute of Mental Health (NIMH) are also key institutions within this cluster. Organizational collaboration network based on article co-authorship.
The green cluster includes Canadian universities and selected European centers such as the University of Toronto, the University of British Columbia, and McMaster University, reflecting a concentration of regional collaborations in North America.
The blue cluster is composed of European universities, including King’s College London, the University of Oxford, the University of Edinburgh, the University of Barcelona, and the Karolinska Institute, which actively collaborate with each other.
The yellow cluster highlights the roles of the University of Copenhagen, the Technical University of Denmark, and Rigshospitalet, all of which serve as key centers with a significant focus on Europe.
A comprehensive review of the network reveals that although scientific collaboration in this field is partly international, the main focus remains on a few well-established institutions. The majority of scientific output and collaborative networks are concentrated among leading academic institutions in the United States, Canada, Europe, and Australia. This pattern indicates that the global research landscape in this domain is still heavily influenced by the activities of a limited number of major centers and has not yet achieved full geographical dispersion.
Author collaboration network
Top 10 authors by number of publications in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

As shown in Figure 4, the collaboration network among authors. This map is based on article co-authorship and reveals multiple scientific collaboration clusters. The largest cluster belongs to the research group led by Eduard Vieta and Diego Hidalgo-Mazzei, who are located at the center of the network and have established extensive collaborations with other researchers. Author collaboration network.
The large blue cluster includes Lars Vedel Kessing and Maj Vinberg, reflecting a tightly knit collaboration group focused primarily on research activities in Northern Europe and Scandinavia.
The green cluster primarily consists of John Torous and his collaborators, who are actively engaged in the field of digital health and integrative psychiatry and maintain broad collaborations with other authors.
Additional clusters include those led by Michael Bauer, Mauricio Tohen, and Michael Berk, who mainly focus on the treatment and management of bipolar disorder.
The collaboration pattern indicates that localized, cohesive research clusters are predominant, although some international collaborations have also emerged. For instance, there are visible collaborative links between European and American researchers in certain clusters; however, most connections remain intra-cluster and regional. This pattern highlights the specialized convergence within specific research teams and the continuity of long-term collaborations over time.
Citation analysis
Citation mapping of articles
Citation analysis is one of the principal methods in bibliometric studies and plays a critical role in identifying influential articles, exploring scientific trajectories, and mapping knowledge networks. In this study, articles published in the fields of bipolar disorder, digital psychiatry, and artificial intelligence from 2000 to 2025 were analyzed from a citation perspective. The focus of this analysis was to identify key articles and the dominant thematic clusters within the scientific literature.
Top 10 most cited articles in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

The study by Price (2011) is regarded as a foundational article in the area of neuroimaging for mood disorders, focusing on brain structures associated with mood fluctuations. The paper by Faurholt-Jepsen (2015b) is one of the first studies to implement daily monitoring of patients using smart applications, providing a model for digital interventions in the management of bipolar disorder. The work of Orrù (2012), focusing on machine learning models for psychiatric disorder classification, has become one of the most frequently cited references in this domain and has been widely referenced in subsequent research.
As shown in Figure 5, the provides a visual representation of the citation network of the analyzed articles. In this network, each node represents an article, and the size of the node corresponds to the number of citations it has received. Articles with higher citation counts are depicted with larger nodes. The lines between nodes represent citation relationships, and clusters are distinguished by different colors, indicating various thematic areas within this field of study. Citation network map of articles related to bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).
The red cluster in this map primarily includes studies related to digital interventions, self-monitoring, and mobile health. Articles by Torous (2016) and Naslund (2015) are at the center of this cluster, focusing on the use of digital tools for monitoring and treating patients with bipolar disorder. These works are foundational in integrating mobile technologies into psychiatric care.
The blue cluster consists of articles focused on neurophysiology and brain imaging. At the center of this cluster is Phillips (2013), regarded as one of the most significant studies in biomarker identification through neuroimaging.
The green cluster is dedicated to articles that emphasize the use of artificial intelligence and machine learning in the diagnosis of mood disorders. The works of Anticevic (2013) and Orrù (2012) are central to this cluster, playing a key role in introducing machine learning algorithms into psychiatric research.
In addition to these main clusters, several smaller clusters are also observable, primarily consisting of earlier studies on traditional psychiatric treatments. These smaller groups account for a lesser share of total citations and are mainly focused on classical topics in psychiatry.
A temporal citation analysis reveals that prior to 2015, research primarily focused on neurophysiology and brain imaging, with articles such as Phillips (2013) and Price (2011) receiving the highest number of citations during this period. However, from 2015 onwards, coinciding with advances in smart technologies, the research focus shifted toward digital interventions and intelligent health solutions. Articles like Torous (2016) and Low (2015), which concentrate on digital monitoring and AI-based diagnosis, have received the most citations in the 2020s. This shift reflects a transition in the field from traditional models toward novel technological approaches in diagnosis and treatment.
Overall, the findings of the citation analysis indicate that the research trajectory in bipolar disorder and mental health has shifted from classical clinical interventions and biomarker imaging toward the use of digital technologies, mobile-based interventions, and artificial intelligence algorithms. This trend reflects a conceptual transformation in the field of digital psychiatry, aligning with the evolving needs of modern healthcare systems, which are increasingly moving toward data-driven and personalized care models.
Thematic and conceptual structure analysis
Keyword co-occurrence mapping
Keyword co-occurrence analysis is one of the core approaches in bibliometric studies, enabling the identification of a field’s conceptual structure, thematic trends, and scientific orientations. In this study, the keywords of articles related to bipolar disorder, digital psychiatry, and artificial intelligence published between 2000 and 2025 were extracted and analyzed. This process led to the construction of a conceptual map based on keyword co-occurrence, effectively illustrating the evolution of concepts in this field.
Most frequent keywords in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).
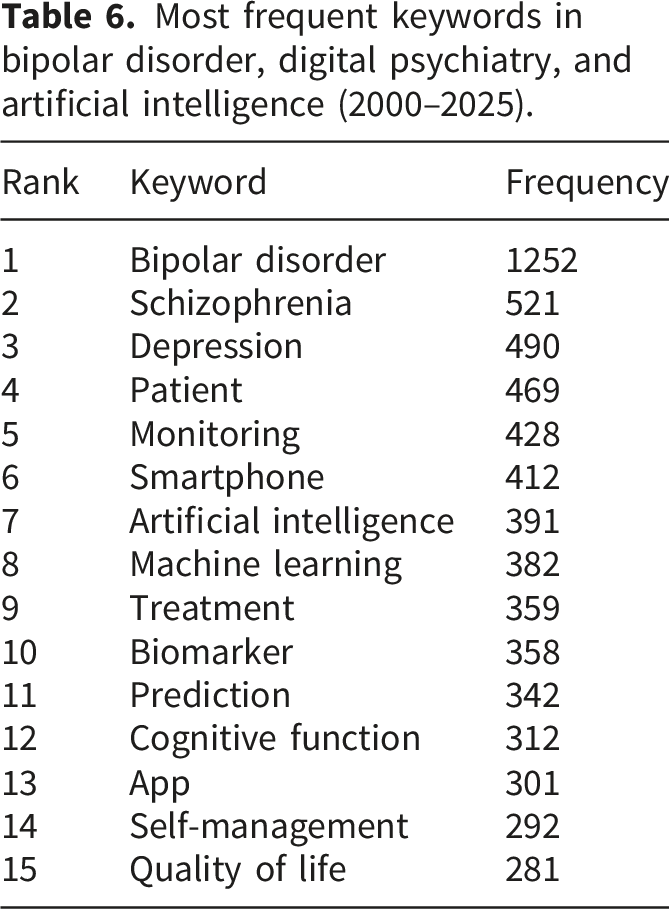
Figure 6 presents the conceptual structure of the field based on keyword co-occurrence analysis. The network illustrates relationships between frequently used terms and the formation of thematic clusters within the literature. Node size reflects keyword frequency, while link thickness indicates the strength of co-occurrence between terms. Colors represent algorithmically generated thematic clusters produced by VOSviewer and indicate conceptual proximity rather than chronological progression or evidence hierarchy. In these network visualizations, colors do not reflect temporal progression or evidence hierarchy but instead indicate groups of keywords that frequently co-occur within the same publications. Therefore, cluster colors represent conceptual proximity rather than chronological development. Keyword co-occurrence map in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).
The network reveals
The
The
The
The
The
Highly connected terms such as bipolar disorder and patient appear near the center of the network, acting as bridging concepts linking multiple thematic domains rather than belonging to a single cluster.
Temporal patterns were examined separately using overlay visualization, in which color gradients represent the average publication year of keywords and are independent of the cluster coloring displayed in Figure 6.
As shown in Figure 7, the temporal evolution of normalized keyword occurrences in bipolar disorder research between 2000 and 2025 is presented using an overlay visualization generated in VOSviewer. In this visualization, node colors represent the average publication year of each keyword rather than cluster membership or evidence hierarchy. Cooler colors (blue–green) indicate earlier prominence in the literature, whereas warmer colors (yellow–red) reflect more recent thematic emergence. Trend of scientific keyword occurrences in bipolar disorder research (2000–2025).
The visualization demonstrates heterogeneous growth trajectories across research themes. Core clinical terminology shows sustained presence across the study period, while technology-oriented keywords — including artificial intelligence, machine learning, and smartphone-based monitoring — appear with warmer overlay colors, indicating more recent integration into the literature. These patterns suggest a gradual thematic expansion toward digital psychiatry and data-driven approaches, reflecting increasing research attention to technology-assisted diagnosis, monitoring, and treatment strategies.
Keyword density map
Keyword density analysis is a key visual method in bibliometric studies that allows for the identification of the concentration and frequency of concepts within the research body. This tool enables researchers to graphically detect both high-frequency topics and underexplored areas, providing a clearer understanding of the conceptual focus and gaps in the existing literature.
As shown in Figure 8, the keyword density map, which illustrates the frequency and conceptual concentration of keywords in studies related to bipolar disorder, digital psychiatry, and artificial intelligence. In this map, high-density keywords appear in yellow and red regions, indicating their frequent usage in the scientific literature. As the color shifts toward green and blue, it represents lower density areas, signifying less frequent mentions and lower scientific focus. Keyword density map in bipolar disorder, digital psychiatry, and artificial intelligence research (2000–2025).
At the center of the map, the term Bipolar Disorder appears with the highest density, reflecting its central role in the field’s research landscape. Other keywords, such as Schizophrenia, Depression, Patient, Monitoring, Smartphone, Artificial Intelligence, and Machine Learning, are positioned in high-density layers surrounding the central core. These terms reflect the field’s expansion toward emerging technologies and digital tools for the diagnosis and management of psychiatric disorders.
The analysis of the map also reveals that emerging keywords, such as Digital Psychiatry, Self-management, Serious Mental Illness, and Feasibility, appear in lower-density and more peripheral regions. This indicates that, although smart technologies are increasingly entering the mental health domain, certain new concepts have not yet been extensively explored in the scientific literature. The presence of these terms in less populated areas of the map highlights research gaps and potential opportunities for future studies.
The findings suggest that, so far, the majority of research has focused on more traditional aspects, such as clinical diagnosis, disease modeling, and comorbidity analysis. In contrast, novel topics related to digital psychiatry and AI-based interventions for patient self-management have received less attention. This situation underscores the need for future research strategies and exploration pathways to increasingly concentrate on emerging and underrepresented keywords, thereby helping to advance the field of digital mental health care.
Bibliographic coupling analysis
Bibliographic coupling map – journals
Bibliographic coupling analysis is an effective method in bibliometric studies that assesses the degree of overlap in referenced sources between articles or journals. This analysis reveals which journals share the highest proportion of references, indicating thematic or methodological proximity. In this study, the journal-level bibliographic coupling network was analyzed for publications related to bipolar disorder, digital psychiatry, and artificial intelligence during the period 2000–2025.
Top 10 journals by bibliographic coupling strength in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

Furthermore, journals such as JMIR Mental Health and JMIR Preprints, which specifically focus on digital health and smart technologies in psychiatry, have shown a considerable degree of bibliographic coupling. This highlights the substantial growth of digital psychiatry journals in recent years. Additionally, Frontiers in Psychiatry holds an important position in this analysis as an interdisciplinary journal with a focus on innovative technologies in mental health.
As shown in Figure 9, the bibliographic coupling network of journals. In this map, each node represents a journal, and the size of the node corresponds to its coupling strength. The lines between the nodes represent the extent of shared references; the more numerous and prominent the links, the greater the overlap in cited sources. Bibliographic coupling map of journals.
In this map, two main clusters are identified. The red cluster predominantly consists of classic psychiatry journals, such as the Journal of Affective Disorders, Bipolar Disorders, Schizophrenia Bulletin, and Molecular Psychiatry. These journals frequently use similar reference materials in the fields of neuroscience and traditional psychiatric disorders.
The green cluster represents digital health and technology-driven psychiatry journals, including JMIR Mental Health, JMIR Preprints, and BMC Psychiatry. This cluster reflects these journals’ focus on digital technologies, mental health applications, and smart monitoring systems.
Journals such as Frontiers in Psychiatry and European Psychiatry act as bridges between the traditional psychiatry field and modern technologies, positioning themselves at the center of the network. Through their interdisciplinary approach, these journals play a key role in converging classical and innovative domains.
The findings of this section indicate that the scientific publication structure in the field of bipolar disorder and digital psychiatry is evolving toward the integration of emerging technologies with clinical and neuroscience studies. The growth of digital health journals and their significant role in the bibliographic coupling network reflect a shift in publication patterns toward technological topics in recent years. This trend may signal the future direction of research, moving toward digitalization in diagnosis and treatment.
Bibliographic coupling of documents
In the document-level bibliographic coupling analysis, the scientific structure of articles in the field of bipolar disorder, digital psychiatry, and artificial intelligence was investigated. This analysis aimed to identify the degree of thematic convergence and shared references among various articles. The results demonstrate that certain core publications in this field exhibit stronger connections due to their focus on similar topics and shared reference materials.
The data were extracted and analyzed using VOSviewer software, and the bibliographic coupling structure is depicted in Figure 10. Bibliographic coupling map of documents (2000–2025).
Top 10 articles by bibliographic coupling strength in bipolar disorder, digital psychiatry, and artificial intelligence (2000–2025).

As shown in Figure 10, the bibliographic coupling structure of documents. Larger nodes represent articles with higher coupling strength, while the connecting lines indicate shared references between publications.
Several distinct clusters can be identified in this network:
The green cluster mainly comprises articles related to the digitalization of mental health services and the application of artificial intelligence in psychiatric interventions. Central works in this cluster include Torous (2016), Naslund (2015), and Low (2015). This cluster reflects the recent focus on digital psychiatry and innovative technologies in mental health. The growth of specialized journals such as JMIR Mental Health is also prominent in this cluster, signifying a shift in scientific publishing toward technological topics in mental health.
The purple cluster focuses on brain imaging, biomarkers, and neural networks, with Orrù (2012) and Anticevic (2013) positioned at its center.
The red cluster mainly involves classic clinical studies on the epidemiology and traditional treatments of bipolar disorder. Within this cluster, Oquendo (2004) serves as one of the most frequently cited references.
According to the results, some articles, such as Vandana (2023) and Abi-Dargham (2023), are located at the periphery of the network and exhibit lower bibliographic coupling with other studies. These works often address emerging or novel interdisciplinary fields that have not yet been fully integrated into the mainstream scientific literature. For example, studies that combine artificial intelligence with biological and epidemiological data currently show limited coupling with other publications due to the innovative and nascent nature of their topics. This situation highlights conceptual gaps that may pave the way for future research opportunities.
The document-level bibliographic coupling analysis reveals that, particularly since 2015, the field of bipolar disorder and digital psychiatry has progressively shifted toward the extensive use of digital technologies, mental health apps, and machine learning algorithms. Specialized digital-focused journals such as JMIR Mental Health have emerged as key publication platforms, reflecting structural changes in scientific publishing.
However, peripheral articles with lower coupling strength point to opportunities for research development in cutting-edge areas, such as hybrid artificial intelligence, environmental data analysis, and digital mental health for underserved populations. Addressing these gaps may help pave the way for future studies and foster greater convergence in the scientific literature of this field.
Identification of research trends, gaps, and future directions
The findings of this bibliometric study indicate a substantial transformation in digital psychiatry and bipolar disorder research over the past two decades, with a pronounced thematic shift emerging after 2015. Keyword co-occurrence analysis revealed that digital monitoring–related terms formed a coherent thematic cluster in the network visualization, particularly within the cluster characterized by smartphone-related terms together with sleep, stress, and cognitive function (Figure 6). Although specific terms such as digital phenotyping and passive sensing may not appear explicitly in the visualization because low-frequency terms are filtered during network construction, this cluster conceptually reflects the growing emphasis on continuous behavioral monitoring and data-driven assessment approaches.
Temporal trend visualization further demonstrated that keywords related to artificial intelligence, machine learning, smartphone applications, and self-management experienced marked growth beginning around 2015 (Figure 7). This temporal acceleration suggests the growing prominence of AI-assisted digital phenotyping and mobile monitoring approaches as a major research direction in the field. Complementary evidence from bibliographic coupling analyses also identified a prominent research stream focused on technology-assisted monitoring and predictive modeling, reinforcing the interpretation that digital psychiatry has become one of the dominant thematic areas in recent years.
Beyond the increase in keyword frequency, the structural evolution of research networks highlights a broader conceptual transition away from episodic diagnostic frameworks toward continuous, ecological, and data-driven monitoring paradigms. Researchers have increasingly incorporated smart health applications, passive behavioral data, and machine-learning–based analytic strategies into bipolar disorder assessment. These developments reflect the movement toward individualized prediction models and multimodal data integration derived from smartphones, wearable technologies, and digital biomarkers. Such advances hold promise for improving diagnostic precision, enabling earlier relapse detection, and supporting more responsive clinical management. However, they also introduce important methodological and ethical challenges, including algorithmic bias, limited cultural generalizability, under-representation of non-Western populations, and privacy concerns associated with passive sensing data. Addressing these challenges requires rigorous validation procedures, transparent model auditing, and standardized data-governance frameworks.
Alongside technological developments, collaboration network analyses indicate persistent gaps in global scientific cooperation. Differences in research funding, disparities in digital infrastructure, and heterogeneous national priorities limit participation in multinational research projects. Structural barriers, such as language differences, lack of interoperable data systems, and inconsistent ethical regulations for AI-based mental health research, further restrict cross-border collaboration. As a result, the United States, the United Kingdom, Germany, and Australia maintain central positions within global networks, while emerging contributors like India and Brazil remain largely regionally oriented. These patterns risk perpetuating global inequalities in scientific output and may reduce the representativeness of AI models applied to diverse clinical populations.
Analysis of reference structures and bibliographic coupling also revealed a notable conceptual divide between emerging digital psychiatry research and classical biological or neuroscience-based approaches. While journals such as the Journal of Affective Disorders and JMIR Mental Health have become central outlets for research on digital interventions, leading journals in biological psychiatry, including Molecular Psychiatry and Translational Psychiatry, remain primarily associated with biomarker and neuroimaging-based studies. This persistent separation results in fragmented research clusters and highlights the lack of integration between biological, behavioral, and digital frameworks. Without intentional interdisciplinary efforts, this gap may slow progress toward developing comprehensive diagnostic, predictive, and therapeutic models for bipolar disorder.
Another important finding is related to patient acceptance and adherence. Concerns about privacy, low digital literacy, limited familiarity with technology, and cultural differences remain major barriers to the widespread adoption of digital mental health tools.29,31,32 Evidence from other psychiatric fields such as eating disorders has demonstrated that health-related quality-of-life (HRQoL) assessments must be tailored to disorder-specific functional impacts to ensure accuracy and patient relevance. 50 Similar efforts are needed in bipolar disorder, where specialized digital HRQoL instruments and cognitive-function assessment tools could significantly enhance clinical usability. Broader neurocognitive research also underscores the relevance of cognition-oriented evaluation frameworks, suggesting that digital phenotyping in bipolar disorder should more systematically incorporate cognitive performance markers. 52
Additionally, a significant conceptual gap persists in data integration. Most current studies focus predominantly on behavioral digital data, with limited attempts to combine these streams with biological markers such as genetics and neuroimaging. 3 This narrow focus may result in incomplete models whose generalizability across diverse clinical environments is limited. Developing integrative frameworks that incorporate behavioral, biological, clinical, and environmental data would substantially strengthen the predictive and clinical value of digital psychiatry.
The practical implications of these findings emphasize the need for a comprehensive, interdisciplinary approach to AI-driven digital mental health. Joint research workshops involving developed and developing countries, multinational research consortia, and harmonized ethical frameworks could promote broader scientific cooperation and knowledge exchange. Strengthening digital infrastructure in countries with limited participation is essential for reducing global disparities. Likewise, user-centered design, robust data governance, and culturally sensitive digital interventions must be prioritized to enhance patient acceptance and clinical applicability.29,31,32
Overall, the evidence indicates that the field is undergoing a fundamental shift from traditional episodic care toward continuous, data-driven, and personalized digital mental health strategies. This transformation aligns with global healthcare trends and has the potential to significantly improve patient outcomes and quality of life. Future progress will depend on expanding international collaboration, integrating biological and digital knowledge bases, and advancing precision-oriented interventions in mental health.
Future research should prioritize longitudinal clinical validation of digital phenotyping tools and the integration of multimodal datasets combining behavioral, biological, and environmental information. In particular, large-scale randomized clinical trials and real-world implementation studies are needed to determine the clinical effectiveness, safety, and scalability of AI-enabled digital interventions. Additionally, future investigations should focus on explainable artificial intelligence approaches, cross-cultural validation of predictive models, and the development of standardized ethical and regulatory frameworks to support responsible deployment in routine psychiatric care.
Discussion
This study explored the growth trajectory of research on artificial intelligence (AI) and digital technologies in the context of bipolar disorder over the last two decades. The findings demonstrate a significant expansion in digital psychiatry research, with AI-based digital phenotyping emerging as a major thematic area after 2015.3,17,18 As the number of publications in early years (2000–2005) was very small, part of this observed exponential increase reflects a low baseline rather than a true surge in research activity. The increasing use of mobile health applications, wearable sensors, and passive behavioral data has introduced innovative approaches for detecting mood fluctuations and predicting relapse risk.8,13,18 These developments support more personalized treatment strategies, enabling clinicians to tailor interventions to patient-specific patterns and trajectories.14,15,54
Importantly, increased publication volume should not be interpreted as equivalent to methodological advancement. The evidence-level distribution observed in this study indicates that much of the field’s growth has been driven by exploratory, observational, and technology-development studies, while high-level randomized clinical evidence remains relatively scarce. This imbalance highlights the need for future research to prioritize rigorous longitudinal designs and controlled clinical trials to support the clinical translation of digital psychiatry innovations.
Importantly, bibliometric indicators capture productivity and structural evolution of a field rather than methodological rigor at the individual study level. Therefore, while the observed evidence distribution provides insight into the relative maturity of research designs, it should not be interpreted as a substitute for systematic quality appraisal. Future meta-analyses and risk-of-bias–focused reviews are required to determine the true clinical reliability of emerging AI-driven digital psychiatry interventions.
The proliferation of machine-learning models for analyzing multimodal data, including voice, text, physiological signals, and smartphone-based behavioral indicators, represents another major trend in the literature.8,45,46 These technologies have enhanced the early identification of mood episodes and facilitated timely interventions, ultimately improving clinical outcomes and reducing hospitalization rates.
Geographically, the United States, the United Kingdom, Germany, and Australia contribute the largest share of global research output (Table 1; Figure 1). Yet, international collaboration remains limited, particularly among countries with rapidly increasing publication counts, such as India and Brazil. Structural inequalities, including disparities in digital health infrastructure, inconsistent national mental health priorities, and heterogeneous regulatory environments, continue to restrict global research integration. Additionally, language barriers and limited access to secure computational platforms further hinder scientific cooperation.
The analysis of source structures revealed a dual scientific landscape: journals focused on digital mental health (e.g., JMIR Mental Health) have become central for publishing AI-related research, while classical biological psychiatry journals (e.g., Molecular Psychiatry, Translational Psychiatry) retain prominence for biomarker and neuroimaging studies.4,5 This divide highlights limited integration between digital methodologies and biological mechanisms, underscoring the need for interdisciplinary research linking behavioral digital data with neurobiological processes.
Patient acceptance and adherence remain major challenges to the real-world implementation of digital interventions. Concerns about privacy, limited digital literacy, and cultural differences play a substantial role in adoption barriers.29,31,32 Lessons from related fields such as eating disorders demonstrate the importance of disorder-specific HRQoL assessments in improving patient-centered evaluation. 50 Incorporating similar tools into digital bipolar disorder research may enhance relevance and accuracy. Furthermore, emerging evidence from cognitive research highlights the importance of evaluating cognitive function in psychiatric and aging populations, suggesting an opportunity to integrate cognition-related metrics into digital phenotyping frameworks. 52
A key conceptual gap also exists in multimodal data integration. Most studies rely heavily on behavioral digital signals without pairing them with biological markers such as neuroimaging findings or genetic data. 3 This limitation restricts the development of comprehensive predictive models. Interdisciplinary efforts that merge biological and digital data streams are essential for advancing precision psychiatry in bipolar disorder.
The practical implications of this study are clear. A holistic approach is required, one that integrates technological advances with biological insights and patient-centered design principles. Joint international workshops, cross-country research consortia, and investment in digital infrastructure, particularly in low-resource settings, are critical for reducing global disparities. Ethical principles, transparency in AI models, and robust privacy-protecting mechanisms must be prioritized to ensure equitable adoption across populations.29,31,32
Overall, the findings suggest that bipolar disorder management within digital psychiatry is transitioning from traditional care models toward continuous, data-driven, and personalized interventions. This evolution aligns with global healthcare trends and holds significant potential for improving patient quality of life. Continued progress will require expansion of international collaboration, integration of biological and digital knowledge, and the development of culturally sensitive and ethically robust digital mental health tools.
These findings emphasize the importance of distinguishing bibliometric expansion from genuine evidence maturation when evaluating progress within rapidly evolving interdisciplinary research domains.
Beyond academic contributions, the findings offer practical implications for healthcare decision-makers, digital health developers, and policy stakeholders. The identified research clusters highlight areas where implementation efforts may be accelerated, particularly in patient engagement, remote monitoring, and data-driven clinical support. Furthermore, collaboration patterns suggest opportunities for strengthening interdisciplinary and cross-sector partnerships to enhance real-world impact.
This study has several limitations. Excluding hyper-authorship records may have reduced the visibility of large multi-institutional collaborations. Additionally, restricting the analysis to Web of Science, Scopus, and PubMed may have led to the omission of relevant studies indexed elsewhere, introducing potential database coverage bias. Furthermore, bibliometric indicators primarily reflect publication productivity and citation relationships rather than methodological rigor or strength of evidence, limiting conclusions about the actual quality and clinical maturity of the literature. The use of VOSviewer also introduces methodological constraints, as clustering and network visualizations depend heavily on the accuracy and completeness of bibliographic metadata. Inconsistencies in author names, affiliations, or reference formatting may influence co-occurrence patterns, network density, and cluster formation, potentially affecting map interpretation. Moreover, the absence of qualitative content analysis restricts deeper contextual understanding of thematic evolution and research impact. These limitations should be considered when interpreting the findings, particularly regarding generalizability and the inferred maturity of emerging research themes. Future studies should incorporate broader data sources, qualitative assessments, and formal evidence-level evaluations to obtain a more comprehensive understanding of the field. Finally, future research should assess the real-world clinical impact of AI-enabled technologies through randomized clinical trials and longitudinal studies to better establish safety, feasibility, and clinical utility in routine psychiatric care.
Conclusion
This bibliometric analysis underscores the substantial progress made in integrating technology into psychiatry, particularly in the context of bipolar disorder. The rapid rise of artificial intelligence (AI), machine learning (ML), and digital phenotyping since 2015 has transformed diagnostic and monitoring practices, paving the way for personalized, real-time mental health care solutions. However, despite these advancements, the findings highlight an uneven distribution of scientific contributions, with developed countries leading research output while emerging economies remain significantly underrepresented. Strengthening international collaborations and fostering interdisciplinary partnerships are essential steps in addressing this imbalance.
Moreover, future research should prioritize the validation of digital tools through large-scale clinical trials, ensuring that real-world data is incorporated into the evaluation process to verify both clinical efficacy and ethical implementation. Bibliometric analyses, such as the one presented in this study, can play a crucial role in informing the design of these trials by identifying promising technologies, emerging research clusters, and thematic gaps that warrant deeper investigation. By addressing these challenges, the field can move toward a globally inclusive, technology-driven psychiatric care model that enhances outcomes for individuals living with bipolar disorder. The collective effort to bridge gaps in research, clinical application, and international collaboration will ensure that innovative mental health solutions reach diverse populations, ultimately improving the quality of care worldwide.
Footnotes
Acknowledgements
The authors would like to thank the scientific community whose publications formed the basis of this bibliometric analysis.
Ethical considerations
Not applicable. This study is a bibliometric analysis based on previously published data. No human participants, personal data, or identifiable information were involved.
Consent for publication
Not applicable. This study does not involve any individual participants or identifiable personal data.
Author contributions
Mohammad Narimani contributed to the conceptualization, study design, methodology development, supervision, and critical revision of the manuscript. Mahdi Naeim was responsible for data collection, data analysis, visualization, and drafting the original manuscript. Both authors read and approved the final version of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to database licensing restrictions but are available from the corresponding author upon reasonable request.